
Abstract
Background and Aims:
Stiffness after a rotator cuff tear is common. So is stiffness after an arthroscopic rotator cuff repair. In the literature, however, postoperative restriction of passive range of motion after open rotator cuff repair in shoulders with free passive range of motion at surgery has seldom been recognized. We hypothesize that this postoperative stiffness is more frequent than recognized and slows the primary postoperative healing after a rotator cuff reconstruction. We wondered how common is postoperative restriction of both active and passive range of motion after open rotator cuff repair in shoulders with free passive preoperative range of motion, how it recovers, and whether this condition influences short- and long-term results of surgery. We also explored factors predicting postoperative shoulder stiffness.
Material and Methods:
We retrospectively identified 103 postoperative stiff shoulders among 416 consecutive open rotator cuff repairs, evaluating incidence and duration of stiffness, short-term clinical results and long-term range of motion, pain relief, shoulder strength, and functional results 3–20 (mean 8.7) years after surgery in 56 patients.
Results:
The incidence of postoperative shoulder stiffness was 20%. It delayed primary postoperative healing by 3–6 months and resolved during a mean 6.3 months postoperatively. External rotation resolved first, corresponding to that of the controls at 3 months; flexion and abduction took less than 1 year after surgery. The mean summarized range of motion (flexion + abduction + external rotation) increased as high as 93% of the controls’ range of motion by 6 months and 100% by 1 year. Flexion, abduction, and internal rotation improved to the level of the contralateral shoulders as did pain, strength, and function. Age at surgery and condition of the biceps tendon were related to postoperative stiffness.
Conclusions:
Postoperative stiff shoulder after open rotator cuff repair is a common complication resolving in 6–12 months with good long-term results.
Introduction
Shoulder stiffness concomitant with a rotator cuff tear is common (1, 2). So is stiffness after an arthroscopic rotator cuff repair (RCR) (3–9). Even today, however, many hospitals and surgeons have not chosen arthroscopic techniques, or in rotator cuff surgery, they use arthroscopy less than open techniques. Postoperative restriction of both the active and passive range of motion (ROM) after an open RCR has even less often received recognition (10–13). Some studies fail to exclude patients already experiencing preoperative stiffness, or they fail to quantitatively compare preoperative ROM to postoperative ROM. They thus lack data on the postoperative restriction of shoulders that show clearly free passive ROM preoperatively (12–14).
“Frozen shoulder” is a term used by Mansat et al. (11), who considered frozen shoulder after RCR a major complication. Holloway et al. (15) used the term “postoperative frozen shoulder”. Some studies report an incidence rate of 3% to 25%, but the exact prevalence of postoperative stiffness after an open RCR is unknown and perhaps even impossible to define due to many confounding factors (7, 11–14).
During his long clinical career, the senior author (M.V.) assumed that after open RCR, poor short-term clinical outcome with passive restriction of ROM might correlate more closely with a postoperative frozen shoulder–type phenomenon than with such issues as inadequate rehabilitation. Mansat et al. (11) reported frozen shoulder as a surgical complication and considered an intense inflammatory response as causing stiffness unresponsive to intense rehabilitation efforts. Idiopathic frozen shoulder has an inflammatory phase, but during its 1–1.5-year natural course it does heal well (16).
Assuming that this entity, postoperative stiff shoulder, extends primary postoperative healing but soon recovers by itself without permanent stiffness or other sequelae, we evaluated the following phenomena: incidence and duration of postoperative stiffness after an open RCR, long-term ROM, pain relief, and shoulder strength, as well as functional outcome of an open RCR in postoperative stiff shoulders 3–20 years after surgery. We also explored short-term clinical results, comparing them with results in controls. None of the study or control patients had passive shoulder stiffness before or at surgery. Several risk factors for postoperative stiffness after arthroscopic RCR have been described, such as single-tendon cuff repair, age, and workers’ compensation insurance (6, 8, 9). We therefore also tried to identify any factors predisposing to postoperative shoulder stiffness after open RCR.
Material and Methods
We identified a total of 103 patients with severe postoperative restriction of ROM among 416 consecutive open RCRs performed between 1988 and 2004 in ORTON Orthopaedic Hospital of the Invalid Foundation. Of these, we excluded preoperative posttraumatic stiff shoulders manipulated before surgery (9 patients), evident posttraumatic adhesive capsulitis diagnosed and manipulated at surgery (3), and shoulders treated only by partial repair, due to severe retraction and poor tendon quality (2), as well as one patient with manipulation under anesthesia 8 weeks after surgery. This left 88 patients with postoperative stiff shoulder. One patient had an evident re-tear with poor shoulder strength, and in four instances, clinical follow-up data were insufficient, leaving 83. Of those, four had died. Of the remaining 79, 56 patients (71%, 59 shoulders) participated in the follow-up study. The study group comprised 39 men (70%) and 17 women, and 45 (76%) were traumatic tears. Preoperatively, X-rays were taken, and the rotator cuff tears were verified by either ultrasound or arthrography. At the final follow-up, no radiological imaging was performed. Age at surgery averaged 56 years (range, 40–83). Time from onset of symptoms to surgery ranged from 2 weeks to 84 months (mean, 8.4 months, median, 4.0 months). Operative delay was <6 months in 38 cases, 6–12 months in 12 cases, and >12 months in 9. Operative delay was less than 1 year in 78%. The mean size of the tear was 3 cm × 4 cm (12.6 cm2). The size of the tear was measured in two directions at surgery. The tear in square centimeters was stated as rectangular, although tears were more or less triangular. The supraspinatus tendon was involved in all cases, the subscapular in seven patients (12%). The size of the tear was massive (≥4 cm × 4 cm) in 29% in the study group and 26% in the control group, the tear including at least the supra- and infraspinatus tendons. A respective 22% and 37% tears were small (≤1–2 cm × 3 cm), including only the supraspinatus tendon. The biceps tendon was intact in 90% in the study group and in 60% within control shoulders, and was absent from 2% and 10%, respectively. Pre- and postoperative data came from patients’ medical records collected by H.V. Minimum follow-up was 3 years (average, 8.7 years; range, 3–20) (Table 1). All patients gave their informed consent. We obtained permission to perform this study from the ethics committee of the hospital district where the study was conducted (296/E6/07, 19 September 2007).
Demographics of patients with postoperative stiff shoulder and controls at surgery.
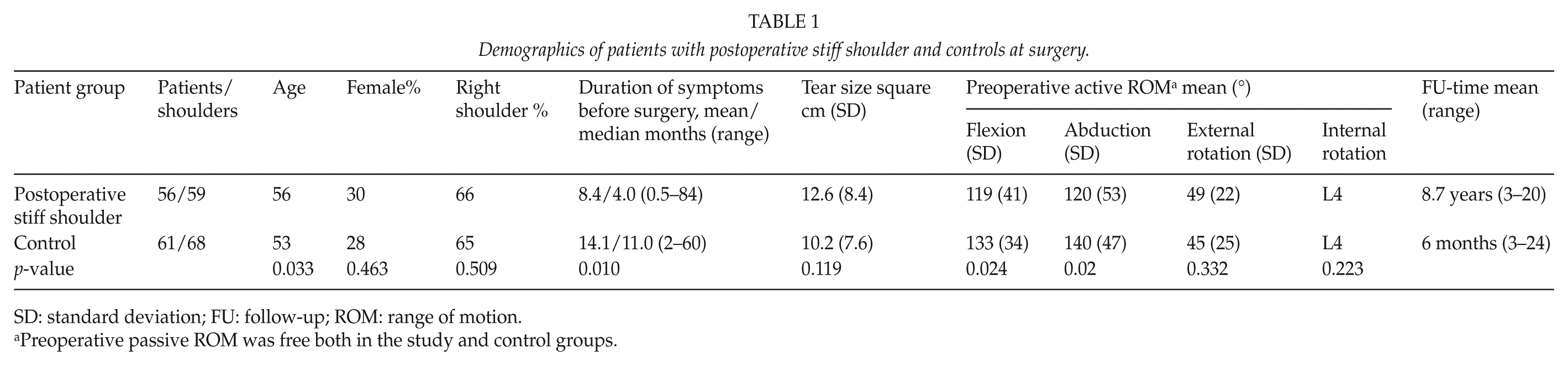
SD: standard deviation; FU: follow-up; ROM: range of motion.
Preoperative passive ROM was free both in the study and control groups.
Our inclusion criteria for postoperative stiff shoulder after open RCR were free preoperative passive ROM and severely restricted active and passive shoulder ROM after a 2- to 5-day inpatient mobilization period, meaning 5–6 weeks after surgery. Their mean passive flexion was 77°, abduction 76°, and external rotation 19°, both flexion and abduction being <110° in 92% of the shoulders and external rotation ≤35° in 88% (Tables 3 and 4). Preoperative ROM was measured either 1 day before or on the same day of surgery. Both preoperative and postoperative ROM was measured by the same surgeon who performed the surgery (90% by M.V.). Concerning short-term follow-up, we also used summarized ROM (flexion + abduction + external rotation). Pain was seldom severe at the time of diagnosis of postoperative stiffness. The study group’s shoulder pain on a visual analog scale (VAS) was measured at final follow-up. Because our intention was to investigate purely postoperative stiffness after open RCR, we excluded shoulders with preoperative stiffness. Exclusion criteria were preoperative passive restricted ROM of the shoulder, shoulders manipulated before surgery, and evident frozen shoulder diagnosed at surgery requiring manipulation. In addition, to reduce confounding factors, we excluded shoulders treated only by partial repair, due to the resultant severe retraction of the ruptured tendon and poor tendon quality.
We randomly selected as controls 61 patients (68 shoulders, 44 males, 65% traumatic tears) with free preoperative passive ROM (every fifth patient picked from a random pile of patient files) from among those remaining 313 surgical patients. We excluded those control patients who had not attended the routine follow-up visits in our hospital. The control patients underwent the surgery by the same surgeons by the same methods as did the study-group patients, and their postoperative treatment was the same. Their mean age at surgery was 53 years (range, 34–68), and operative delay 2–60 months (mean 14.2 months, median 11.0 months) being less than 1 year in 64%. Tear size averaged 10.2 cm2. The supraspinatus tendon was involved in all cases, the subscapular in two patients (3%) (Table 1).
M.V. performed 53 (90%) of the 59 repairs; for 54 tears, the repair was direct tendon to bone, done with nonabsorbable sutures (Mersilene®; Ethicon Inc, Somerville, NJ, USA). For five patients (8%) with old, retracted tears, repair involved a free-tendon graft (17–19). Postoperatively, the arm was mostly immobilized in an abduction splint for an average of 5.5 weeks. In the study group, 81% and in the control group, 94% used a splint. The elbow joint was mobilized on the first postoperative day, with passive mobilization of the arm started at 2 weeks in the splint. After immobilization, all patients visited the hospital for 2–5 days of intensive supervised physiotherapy including assisted and active ROM exercises as well as pool exercises. Normally, physiotherapy continued for 1–3 months as outpatients, but in those patients with shoulders showing postoperative passive stiffness, it continued even longer. The patients routinely came to their follow-up visits 1 and 2 months after the mobilization period. Normally, most of them returned or had already returned to work by the 2-month visit (3.5 months after surgery, 8 weeks after the mobilization period). The next visit was scheduled after 3 months, but if the patient was unable to work, after 1 month. At every visit, active and passive ROM and shoulder strength by manual testing without a spring balance were recorded. Their strength was tested with a spring balance preoperatively and at final follow-up. The surgical technique, surgeons, and short-term controls were the same as for the control patients.
Questionnaires (Appendix 1) were sent by mail to the patients before the final follow-up, along with the invitation to the study. The questionnaire comprised questions concerning demographics, subjective satisfaction, and symptoms of the operated shoulder including pain evaluation on a VAS (range, 0–10; 0 = no pain and 10 = maximal, intensive pain). In addition, patients received the Simple Shoulder Test questionnaire (20). They completed these questionnaires at home and returned them at the follow-up visit.
All 56 patients underwent a physical examination preoperatively, postoperatively, and at the final follow-up. ROM of both shoulder joints was measured with a goniometer, and muscle strength in abduction was measured at final follow-up with the same Salter spring balance used preoperatively (18, 19). The last postoperative routine clinical follow-up examination took place 6 months–1 year after surgery. The final follow-up took place 3–20 (mean 8.7) years after surgery. At the final follow-up visit, the physical examination was performed by an independent observer (H.V.). Presence of a painful arc sign was indicated by yes or no. Shoulder function was assessed by Constant–Murley score (21).
The χ2 test served for analysis of incidence of postoperative frozen shoulder, Student’s t-test for length of postoperative frozen shoulder. Analysis of variance (ANOVA) served for long-term ROM, pain relief, shoulder strength, and functional outcome of RCR. Differences in categorical variables were tested with Pearson’s χ2 or with Fisher’s exact test. Based on univariate analysis, age at surgery, sex, operative delay, preoperative flexion and abduction, tear size, subscapular tear, biceps tendon condition, free-tendon graft, abduction splint, and immobilization period after open RCR were included in logistic regression analysis of the factors predisposing to postoperative stiffness. A logistic regression model revealed relative risk estimates (adjusted odds ratios (ORs) with 95% confidence intervals (CIs)) for factors predisposing to postoperative stiffness after open RCR. Significance was set at 0.05. We performed all statistical analyses with SPSS (Version 18.0; SPSS Inc., Chicago, IL, USA).
Results
The incidence of postoperative stiffness was 20%. The primary postoperative recovery of ROM was 3–6 months longer in the study group and ROM recovered during a mean period of 6.3 (2–18) months postoperatively. External rotation resolved first with no significant difference from that of controls (mean 36° vs 41°) 3 months after surgery. Flexion and abduction still were inferior at 6 months, but no differences appeared at 1 year (Table 3).
ROM of the index shoulders improved exactly to the contralateral level in flexion, abduction, and internal rotation. Even though external rotation resolved first, it was inferior to the contralateral shoulder’s rotation by 11% in a mean 8.7 years afterwards (Table 2). Concerning short-term follow-up, index-point summarized ROM (flexion + abduction + external rotation) 6 weeks after RCR was 68% of ROM in the control group, at 3 months 82%, at 6 months 93%, and at 1 year it reached almost 100% (Table 3). The painful arc sign was positive in six shoulders.
ROM, strength, pain, and function of postoperative stiff shoulder patients at final follow-up 3-20 years after surgery.
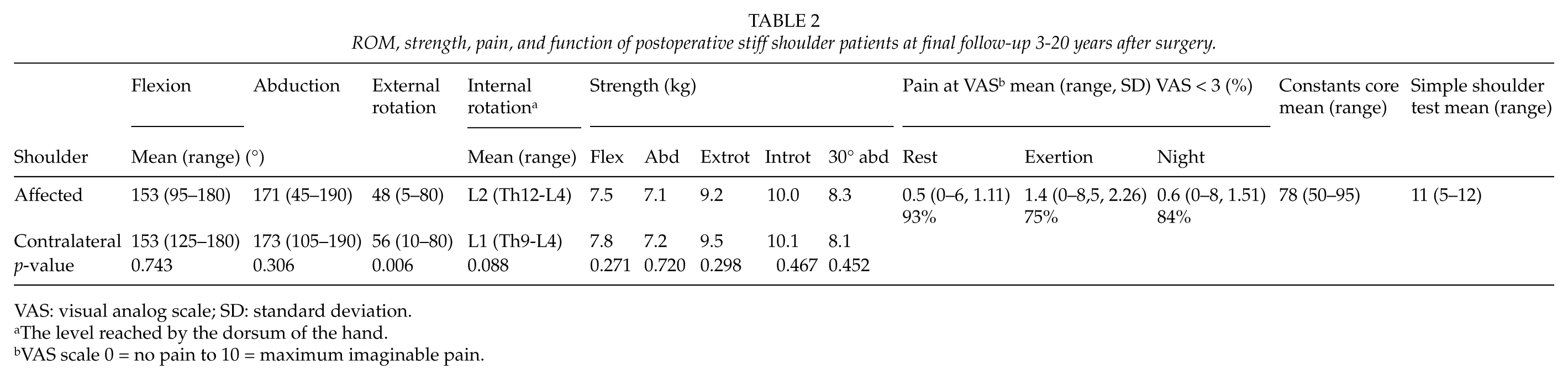
VAS: visual analog scale; SD: standard deviation.
The level reached by the dorsum of the hand.
VAS scale 0 = no pain to 10 = maximum imaginable pain.
Mean ROM of postoperative stiff shoulders and control shoulders after open rotator cuff repair.
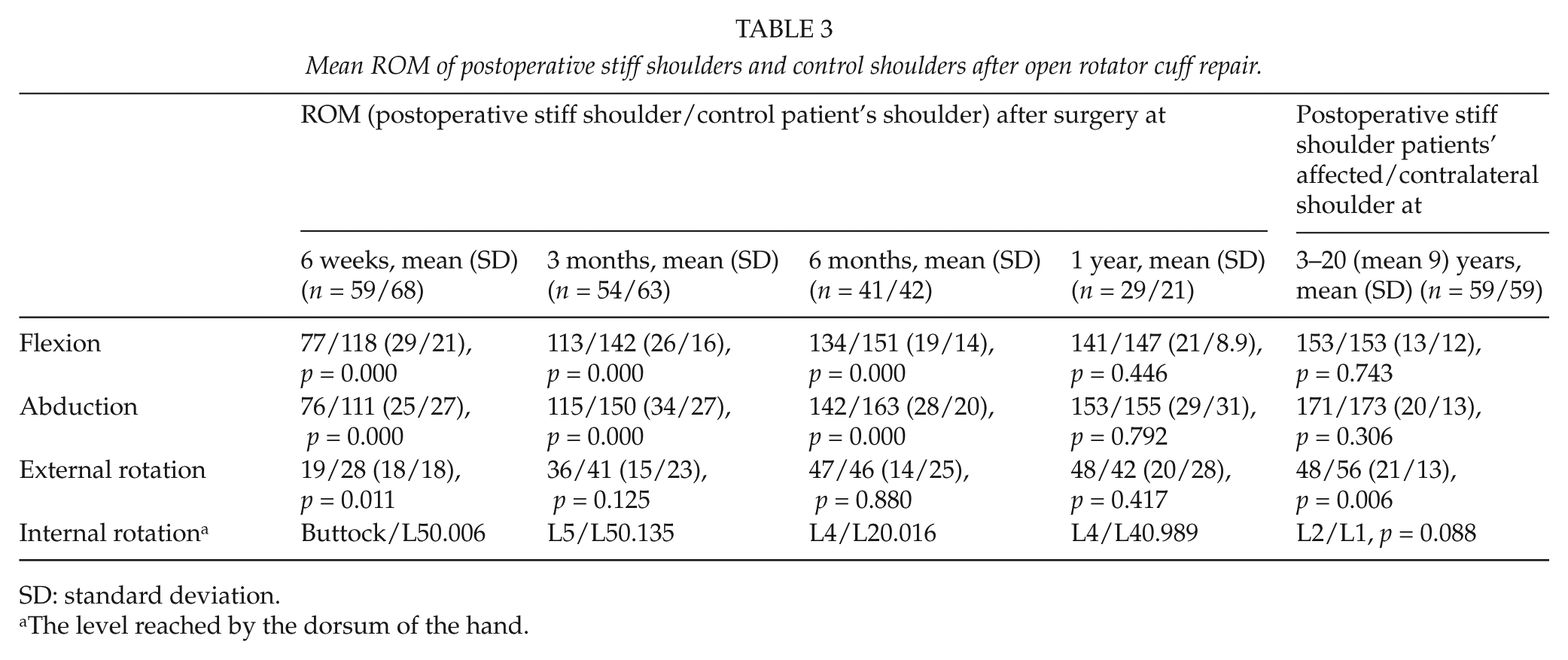
SD: standard deviation.
The level reached by the dorsum of the hand.
Pain at rest on the VAS scale at final follow-up was <3/10 for 93% (Table 2).
The strength of the postoperative stiff shoulder matched that of the contralateral shoulder well (Table 2). Concerning function, the Constant–Murley score averaged 78 and was ≥80 in 56%. The Simple Shoulder Test had a mean value of 11 of 12 (Table 2).
Of the variables tested for any association with postoperative stiffness, some showed an association that reached significance. In logistic regression analysis of the factors predisposing to postoperative stiffness, we included the following variables: age at surgery (p = 0.033), operative delay (p = 0.010), preoperative flexion (p = 0.024) and abduction (p = 0.020), condition of the biceps tendon (p = 0.001), and free tendon graft (p = 0.008). Our logistic regression analysis showed that higher age at surgery (OR 1.11, 95% CI 1.01–1.20) and sound biceps tendon (OR 19.38, 95% CI 1.78–211.18) proved to predispose to postoperative stiff shoulder. No correlation appeared between incidence of postoperative stiff shoulder and use of the abduction splint.
Discussion
Clinical and functional early, mid-term, and long-term results of open RCR are well documented (2, 5, 13, 17, 18, 22–29). Surgical intervention is a significant cause of shoulder stiffness (4, 7), and stiffness is the most common complication after RCR (3), but postoperative restriction of active and passive ROM after open RCR rarely receives any mention (11, 13), and mention usually regards prolonged immobilization, inability to comply with physical therapy (10), or a too tight repair (12). Risk factors are also age under 50 and having workers’ compensation insurance (15), but tear size (3) or sling immobilization for 6 weeks have not been among the risk factors (5). On the other hand, a small cuff tear may also be a risk factor (11). As regards arthroscopic RCR, on the contrary, advanced age is an important risk factor (9). We believe that poor short-term clinical outcome with passive restriction of ROM after open RCR may often be correlated more with postoperative stiff shoulder than, for instance, with inadequate rehabilitation. Franceschi et al. (4) also considered postoperative stiffness to be related to adhesions and capsular contracture, perhaps similar to the mechanism involved in idiopathic adhesive capsulitis with cytokines, inflammatory cell products, and platelet-derived growth factors. Further studies are needed with biopsies compared to histopathology findings in idiopathic frozen shoulder.
We acknowledge limitations. First, the study is retrospective. Second, the study population is heterogeneous, including patients with very different follow-up times. However, short-term follow-up time was about the same in every patient and in both the groups. Third is a possible selection bias because our hospital is a third-level referral hospital, meaning perhaps more difficult cases, but we also have many private patients coming directly to our hospital.
Fourth, the arm was immobilized in an abduction splint for an average of 5 weeks in most cases. Today, most shoulder surgeons do not use a splint, and even using a sling, they mobilize the arm early. We found, however, no correlation between incidence of postoperative stiff shoulder and use of the abduction splint. As a matter of fact, abduction splints were used more often and longer for our control patients (80% vs. 93%, mean 4 vs. 5 weeks). Neither did Mansat et al. (11) find any correlation after RCR between immobilization style and complications such as postoperative frozen shoulder. We still use the splint in chronic, very large retracted tears to avoid postoperative disruption.
Fifth, we did not use imaging methods to determine the integrity of the rotator cuff at follow-up. Sixth, concerning tear size, we used square centimeters counted side by side, although often tears were not rectangular. Seventh, duration of symptoms or operative delay was significantly longer for controls. In logistic regression analysis, this failed to reach significance, however.
Eighth, we had no follow-up exam at 9 months after surgery that might have revealed even faster improvement. Ninth, some patients did not come to the 6-month or 1-year follow-up. These patients already had significantly better ROM at the 3-month follow-up, so we may assume that they had no need to come. Their postoperative stiffness had already resolved in 3 months to such an extent that their ROM no longer differed from the control patients’ ROM at 3 months (flexion or abduction already mean 143°).
Tenth, we would like to use the clinical term “postoperative frozen shoulder,” although we have performed neither arthroscopic nor microscopic examinations. Although it greatly resembles it, we do not yet precisely know whether the basic disorder in these shoulders is really biologically the same as in a spontaneous frozen shoulder, in which clinically the course is similar except for more pain and longer duration.
As regards the incidence of postoperative stiffness, Simon Bell from Australia stated in the ninth International Conference for Shoulder and Elbow Surgery in Washington, DC, in 2004 that it was 25% after open RCR, but he has never published his results. In other studies, incidence was 3% after open RCR (11), and 16% after open revision surgery (10), whereas we had 20%. Perhaps our incidence differs because we diagnosed stiffness just 6 weeks after surgery and after 2–5 days of physiotherapy. In a similar population of 209 patients after open RCR (13), when the inclusion criterion fell into the lower quartile of passive ROM, stiffness incidence at 6 weeks after surgery was 17%. Some of their patients had, however, already experienced preoperative stiffness. Postoperative stiff shoulder has a tendency to recover within 6 months. Evaluating postoperative stiffness at 3 or 6 months after RCR should produce an incidence even lower. In a review of 500 RCRs, when evaluated at 9 months, 4% had significant arthrofibrosis after RCR (14) and 5% after arthroscopic RCR (6) (Table 4). Mansat et al. (11) reported frozen shoulder as a complication of RCR with an incidence of 0.5% in a series of 40 studies of RCR between 1982 and 1995.
Literature on postoperative stiffness after rotator cuff repair.
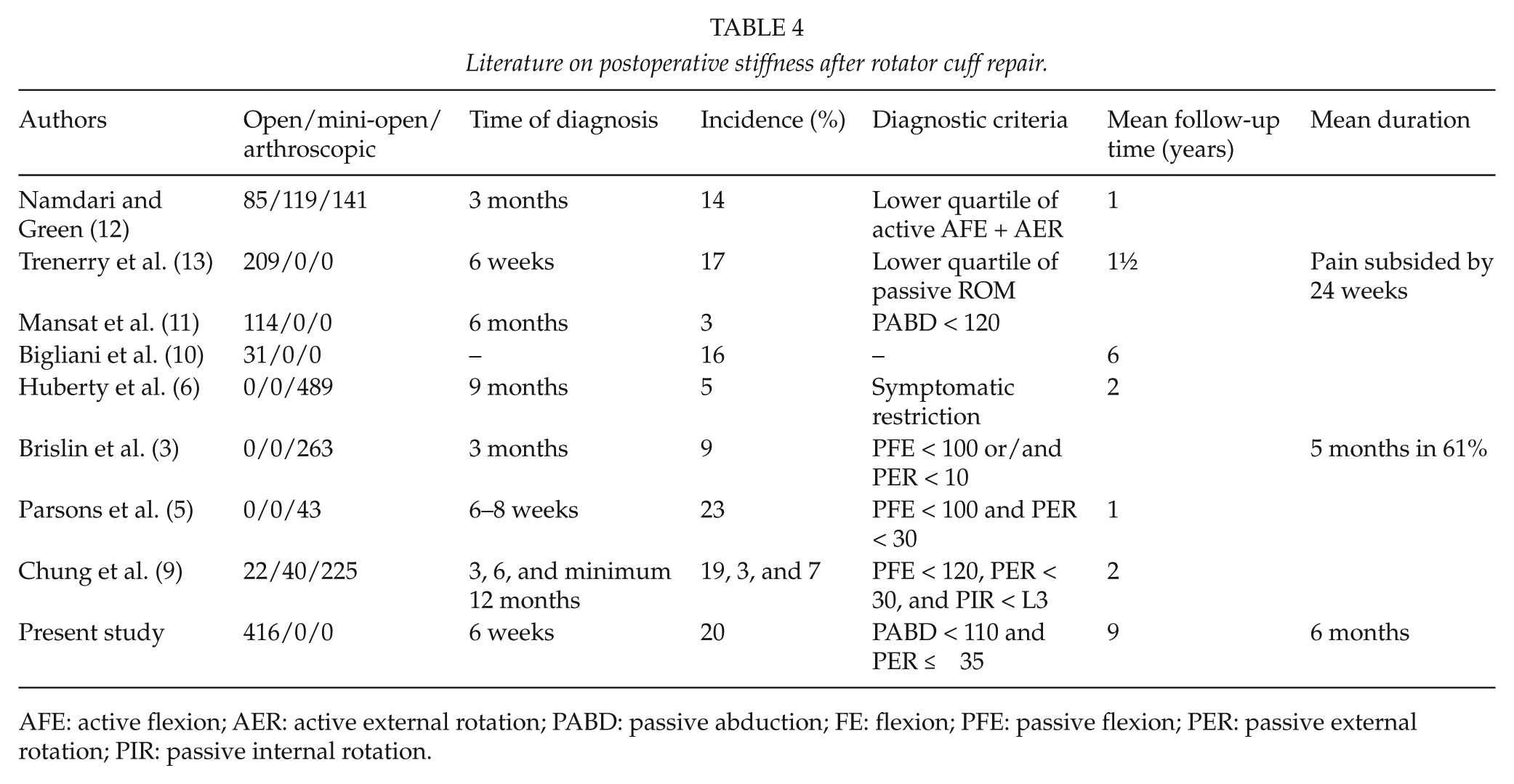
AFE: active flexion; AER: active external rotation; PABD: passive abduction; FE: flexion; PFE: passive flexion; PER: passive external rotation; PIR: passive internal rotation.
Concerning duration of symptoms, the figure for duration of postoperative stiff shoulder is not reported precisely. Brislin et al. (3) did state that his patients’ postoperative stiffness after arthroscopic RCR resolved with minimal motion deficit (<10% passive loss in any plane) at a mean 5 months after surgery. Of those 23 cases, 14 (61%) resolved, the other 39% still having significant lack of passive ROM at 5 months. Here, postoperative stiffness lasted approximately 6 months and had resolved before 1 year, a duration of symptoms thus shorter than for idiopathic frozen shoulder (16).
Concerning ROM, Trenerry et al. (13) found motion to steadily improve between 6 weeks and 76 weeks postoperatively, reaching nearly complete recovery. In our patients, ROM began to improve on average at 3 months and had improved to almost normal (93% of ROM in the control group) on average by 6 months without any treatment except physiotherapy. External rotation resolved in 3 months, as occurred in Cho and Ree’s (30) study of 15 patients with arthroscopic RCR of preoperatively stiff shoulders. Concerning pain, only a few short notes mention pain caused by postoperative stiffness after RCR. Pain scores improved from 5.6 to 2.0 among patients with stiff shoulders (p = 0.590) and from 5.1 to 1.7 among the non-stiffness patients (p = 0.820) (24), and pain subsided by 24 weeks (13). Here, pain resolved well (Table 3).
As regards function after postoperative stiff shoulder, Parsons et al. (5) reported a mean 1-year American Shoulder and Elbow Surgeons (ASES)score of 83 among the stiffness patients and 79 for the non-stiffness patients, as well as a Constant–Murley score of 77 and 74, respectively, without any statistical significant difference between these groups. For the present population, the Constant–Murley score for postoperative stiff shoulders averaged 78, being ≥80 for 56%. Thus, postoperative stiff shoulder seems not to affect shoulder function in the long term.
As factors predisposing to postoperative stiffness after RCR, Namdari and Green (12) listed the following: preoperative limitation of active ROM, open repair, size of tear, dominant extremity, diabetes mellitus, and workers’ compensation claim. Mansat et al. (11) stated that among open RCR patients, those who developed postoperative stiffness after RCR had smaller tears involving fewer tendons. Brislin et al. (3) did not find tear size to be a predisposing factor. In our study, higher age and sound biceps tendon led to elevated risk for postoperative stiffness. The risk for developing postoperative stiff shoulder increased by 10% per year of age. Chung et al. (9) also stated that old age is an important factor for postoperative stiffness after arthroscopic RCR. Risk increased considerably if the biceps tendon was intact. That was surprising, and perhaps reflects the fact that the biceps tendon may also, in spontaneous frozen shoulder, be severely affected. Mansat et al. (11) found that the larger the amount of tissue in the area, the more available it is for participation in the inflammatory response.
Causes of stiffness after RCR are also postulated to include prolonged immobilization, inability to comply with physical therapy, or constraint of shoulder motion owing to a tight repair (10). We, however, were unable to find any of these factors as significant. We have seen postoperative stiff shoulders following repair of small rotator cuff tears also without any immobilization, implying that immobilization in the splint is not the cause of postoperative stiffness. Neither did we show any significant correlation between the splint and the incidence of postoperative stiffness. Parsons et al. (5) also concluded that slower rehabilitation does not lead to long-term stiffness. Their patients under age 50 were at higher risk for stiffness, but our results showed just the opposite.
Conclusion
Postoperative stiff shoulder after open RCR is a common complication resolving normally in 6 months. We believe that postoperative stiffness after open RCR should receive more recognition as one of the most important complications. This is essential, especially for those patients and physiotherapists who worry about any unexpected and unexplained delay not only in active but also in passive ROM recovery. We should be able to tell them that a probable reason for such tardy improvement is postoperative stiffness, which resolves without any surgery within 6–12 months quite well.
Footnotes
Acknowledgements
We thank Jyrki A. Kettunen PT, PhD, for statistical aid and Carol Norris, PhD, for language revision.
Declaration of Conflicting Interests
The authors have no conflict of interest.
Ethical Approval
Each author certifies that his or her institution approved the human protocol for his or her investigation, that all investigations were concluded in conformity with ethical principles of research, and that informed consent for participation in the study was obtained.
Funding
The institution of the authors has received, during the study period, funding from EVO, HUS = government grant from Helsinki University Hospital District.