
Abstract
Background and Aims:
Breast reconstruction has been shown to improve quality of life. However, factors involved in long-term patient satisfaction are largely unknown. Our aim was to evaluate patient satisfaction and donor-site morbidity in five types of breast reconstruction.
Material and Methods:
A prospectively collected database of all breast surgery patients at Hospital Rudolfstiftung, Vienna, Austria, was searched for five types of breast reconstruction (2000–2006): implant, latissimus dorsi-flap, latissimus dorsi-flap with implant, free transverse rectus abdominis musculocutaneous-flap, and deep inferior epigastric perforator-flap. Patients were sent a study-specific questionnaire to assess satisfaction. Short-form 36-item health survey was used to analyze (quality of life), and complication data were retrieved from the database and assessed during a follow-up visit.
Results:
There were 257 patients identified, of whom, 126 responded to the survey (17 implant, 5 latissimus dorsi + implant, 64 latissimus dorsi, 22 transverse rectus abdominis musculocutaneous, and 18 deep inferior epigastric perforator reconstructions). No statistical differences were found in complication or reoperation rates. Deep inferior epigastric perforator–flap patients were significantly more satisfied compared to patients from the implant group (p = 0.007). However, there was no significant difference regarding quality of life scores among the groups. After logistic regression analysis, only “impairment on daily life” showed to be independently correlated with patient satisfaction. This contrary to both operation type and complication rate which did not correlate with patient satisfaction.
Conclusions:
Our results indicate that operation type, complication rate, and revision rate did not independently correlate with patient satisfaction. Therefore, to further improve patient satisfaction, future research should be focused on other pro-operative factors, for example, patient education, expectations, and personality characteristics.
Introduction
One in eight women in the United States will be faced with the diagnosis of breast cancer at some point in her life (1). Roughly one-third of these women will elect to undergo mastectomy (2). And while mortality of breast cancer is decreasing due to advances in treatment strategies, incidence is steadily rising, resulting in exponential increase of breast cancer survivors (1). A large percentage of these women are unhappy with the cosmetic outcome (3), of whom, many are faced with the decision whether to undergo breast reconstruction.
Mastectomy defects can leave deep scars both physically and mentally, and there is a large body of evidence indicating improvement of self-esteem and mental health following breast reconstruction (4). However, decision making is complicated by a multitude of options and a wide range from implant to different autologous reconstruction alternatives. As information from health-care professionals is most valued for decision making (5), outcomes research is essential to provide patients with concrete and reliable information to assist in their decision making.
Although patient satisfaction is important in all surgical disciplines, it is of pivotal importance in postmastectomy reconstruction as its over-riding goal is to satisfy patients with respect to improvement in quality of life (QoL). As many factors besides clinical outcomes can influence patient satisfaction, both clinical outcomes and patient-reported outcomes should be rigorously assessed in studies that attempt to evaluate surgical success.
There is clear evidence showing that unrecognized or unfulfilled expectations regarding surgical outcomes are directly related with poor patient satisfaction and greatly influences patient’s perception of the surgical result (6, 7). On the contrary, it is difficult to come by clear data regarding impact of various breast reconstruction alternatives on patient satisfaction and QoL. And these data are of grave importance to communicate to the patient in order to create realistic expectations regarding surgical outcomes (8–11). Therefore, the objective of the study herein was to evaluate patient satisfaction and donor-site morbidity in a large sample population in five common types of breast reconstruction: expander/implant, latissimus dorsi myocutaneous (LD)-flap, LD-flap in combination with an implant, free transverse rectus abdominis musculocutaneous (TRAM)-flap, and deep inferior epigastric perforator (DIEP)-flap.
Material and Methods
Study Design and Population
Patients who underwent either immediate or delayed breast reconstruction between May 2000 and October 2006 were identified from a prospective database for breast surgery patients at Hospital Rudolfstiftung, Vienna, Austria. Five different types of breast reconstruction were included in the study, that is, expander/implant, LD-flap, LD-flap in combination with an implant, TRAM-flap, and DIEP-flap. Both unilateral and bilateral breast reconstructions were included. All surgeries were performed at the Department of Plastic and Reconstructive Surgery, Hospital Rudolfstiftung, Vienna, Austria. Patients with reconstruction for other reasons than cancer and severe comorbidities (American Society of Anesthesiologists (ASA) III) were excluded from the study.
The study followed the Helsinki Declaration and was approved by the Local Ethics Committee of the Medical University of Vienna. All patients gave their informed consent to participate under the guidelines of the local ethics committee. The following data were obtained: patient satisfaction using a self-designed questionnaire, short-form 36-item health survey (SF-36), and complication rate.
Assessment of Patient Satisfaction
The women were sent a study-specific questionnaire and invited for a follow-up visit. Questionnaires were mailed along with self-addressed postage-paid return envelopes. To maximize response rates, nonresponders were mailed a reminder after 2 months. Only survey results from patients who had completed their reconstruction were included, and only patients who completed QoL questionnaires were selected in the analysis.
Patients were asked to score postoperative pain on a 5-point scale from “absent” to “very severe.” Also, self-reported recovery time to preoperative status was scored. In addition, patients were asked to rate their impairment on daily life and their impairment during physical exercise on a 5-point scale ranging from “no impairment” to “severe impairment.” Furthermore, patients were asked whether they were satisfied with the overall result. In response to this question, patients could choose from three different answers: “not satisfied,” “satisfied,” and “fully satisfied.” Patients who were not fully satisfied were asked to explain the reason for their incomplete satisfaction. Finally, patients were asked whether they would undergo the same procedure again. This study-specific questionnaire was developed based on questionnaires previously used to assess surgical procedures of the breast, including European Organization for Research and Treatment of Cancer Breast Cancer-Specific Quality of Life (EORTC QLQ BR-23) (12) and Functional Assessment of Cancer Therapy-Breast (FACT-B) (13).
General QoL was assessed using the validated questionnaire, SF-36 (14). This questionnaire consists of eight scaled scores, which are weighted sums of the items in their sections. These eight scales can be divided into two clusters. First, Physical Health in which physical functioning, physical role functioning, bodily pain, and general health are scored. Second, Mental Health in which vitality, social functioning, emotional role functioning, and mental health are being assessed.
Additional data regarding complications were extracted from the database and clinical evaluation during the follow-up visit. Complications were categorized as being minor or major. Minor complication included clinical signs of infection, abdominal bulging/hernia, limited necrosis of the breast, and delayed wound healing which was defined as prolonged healing time requiring dressing changes assisted by health personnel. Major complications comprised necrosis of most of the flap, total flap failure, and capsular contracture.
Statistical Analysis
Statistical analysis was performed using GraphPad Prism version 5.0 (GraphPad Software, Inc., La Jolla, CA, USA). For continuous variables, p-values were derived from analysis of variance (ANOVA) for comparing mean values between groups. When comparing two groups, Student’s t-test was used. For categorical variables, p-values were derived from chi-square test for independence. The p-values for variables that were calculated from a score are computed by a Kruskal–Wallis test. Values are given as mean (standard error of the mean (SEM)). Statistical significance was considered for values of p < 0.05.
To calculate the odds ratio of independent risk factors for patient satisfaction, a stepwise logistic regression analysis was done. Following variables were used for the model: type of surgery, postsurgical complications, revisions, quality of daily life, and SF-36 score. Independent variables were included into the model at a level of p < 0.05 and excluded at p > 0.1.
Results
A total of 257 patients underwent breast reconstruction between May 2000 and October 2006. Of these women, 13 underwent a bilateral reconstruction summing up to a total of 270 breasts. Of these 257 patients, 126 returned the questionnaire and attended the follow-up visit, resulting in an overall response rate of 49.0%. Among the responders were 17 implant-based reconstructions (9 implant reconstructions and 8 with expanders), 69 LD-flaps (5 with and 64 without implants), 22 free TRAM-flaps, and 18 DIEP-flaps (Table 1). The response rate was highest in the LD + implant group and the DIEP group, whereas patients reconstructed with implants had the lowest response rate. However, these differences were not statistically significant (p = 0.14, Table 2). A minimal response rate of 43.6% was obtained in all categories. Both responders and nonresponders showed similar baseline characteristics regarding age and time since surgery. Average (range) age of the group that responded the survey was 51.6 years (33–82 years). The average follow-up was 38.4 months (6–77 months). All women had been Caucasian, well educated, and employed. Among responders, when baseline characteristics were specified per reconstruction type, it showed that all groups were of a similar average age and were on average assessed the same time after their surgery (Table 2). Immediate reconstructions were more frequently performed among implant and LD patients (p = 0.04). Furthermore, implant-based and DIEP-flap reconstructions were more frequently performed in a bilateral fashion as compared to other groups (p = 0.05). The follow-up time was similar in all groups.
Characteristics responders versus nonresponders.
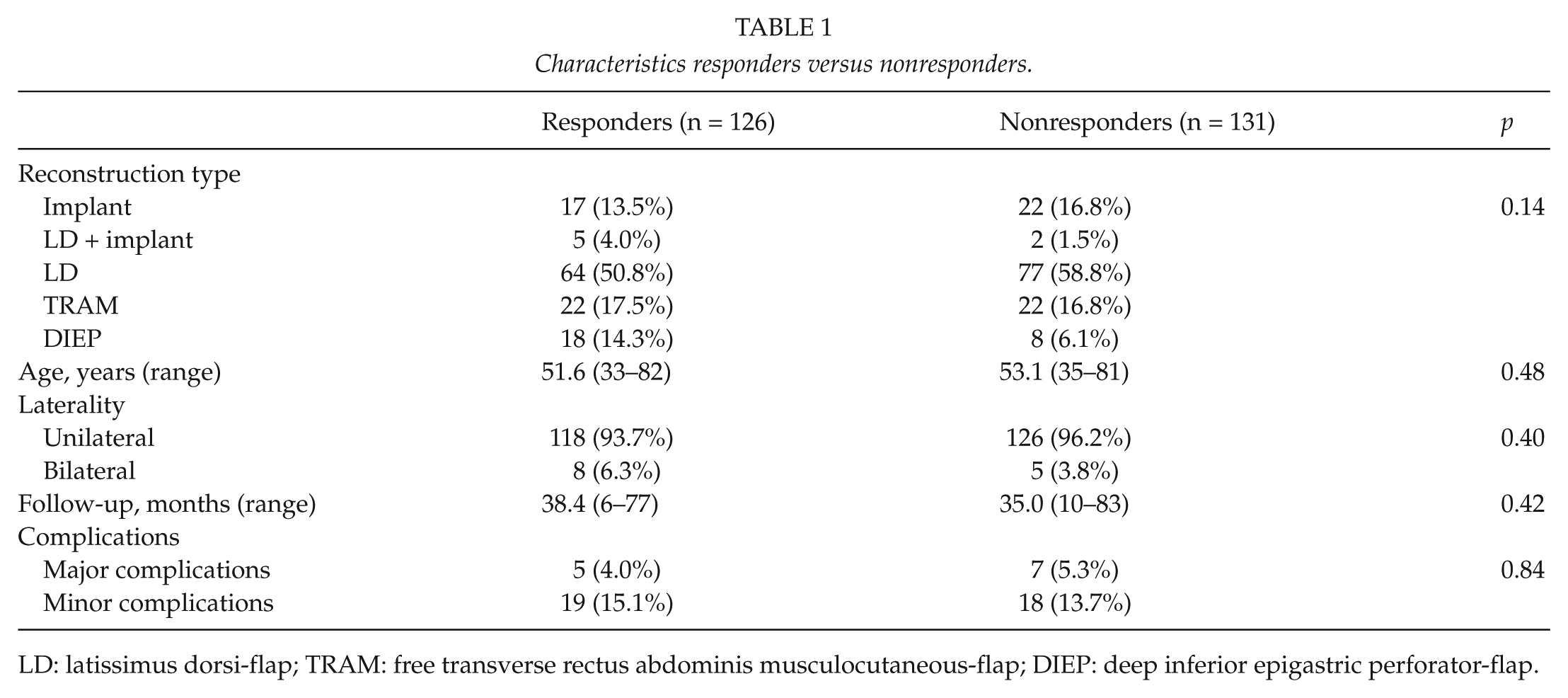
LD: latissimus dorsi-flap; TRAM: free transverse rectus abdominis musculocutaneous-flap; DIEP: deep inferior epigastric perforator-flap.
Baseline characteristics per reconstruction type of survey responders.
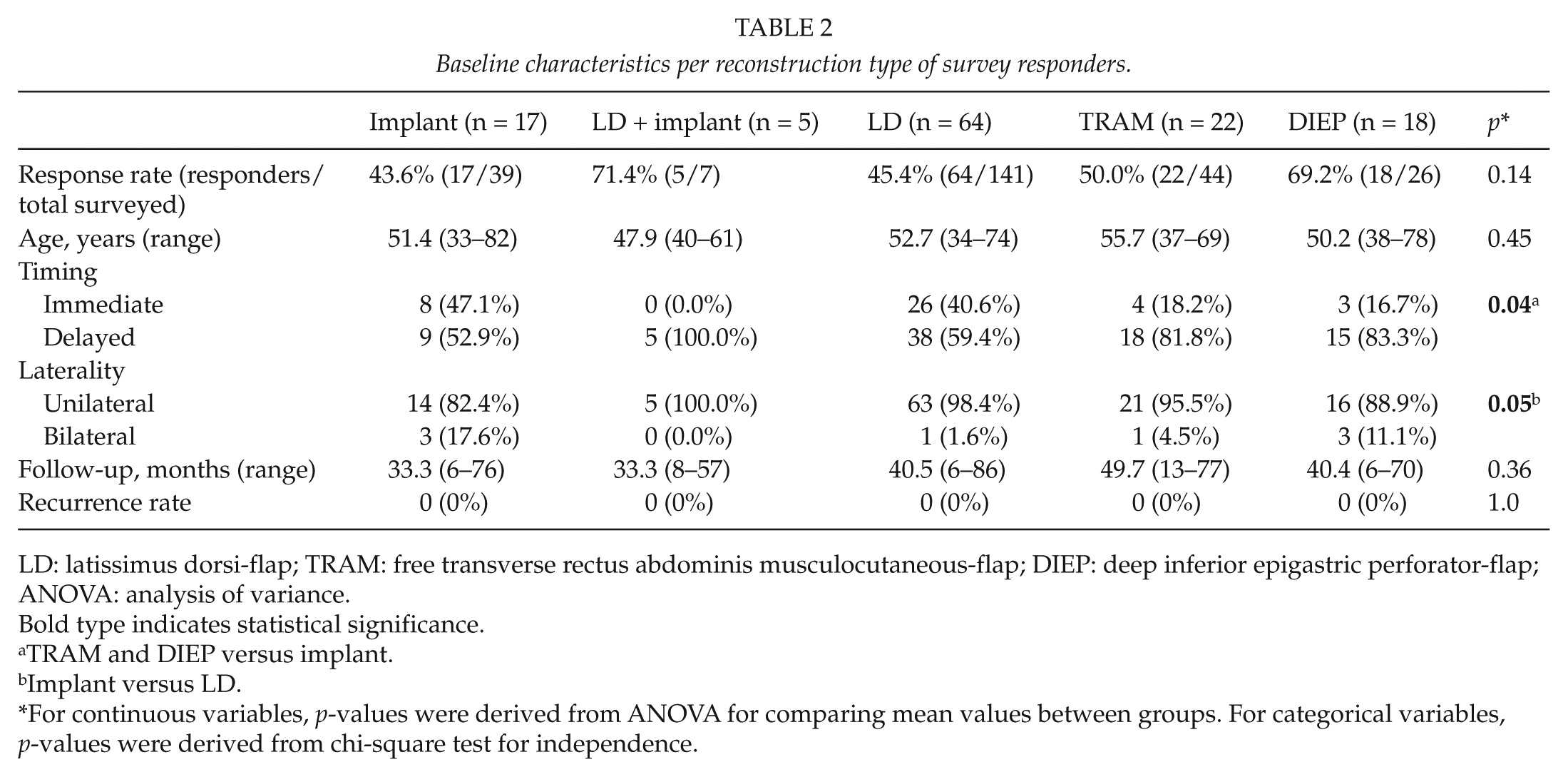
LD: latissimus dorsi-flap; TRAM: free transverse rectus abdominis musculocutaneous-flap; DIEP: deep inferior epigastric perforator-flap; ANOVA: analysis of variance.
Bold type indicates statistical significance.
TRAM and DIEP versus implant.
Implant versus LD.
For continuous variables, p-values were derived from ANOVA for comparing mean values between groups. For categorical variables, p-values were derived from chi-square test for independence.
Complications
The overall complication rate of all 257 women in the study was 19.1%, of which, 14.4% was categorized as minor and 4.7% as major complications. When comparing responders to nonresponders, both minor and major complications occurred at a similar rate (p = 0.84) (Table 1).
Among survey responders, 24 complications were scored, resulting in a complication rate of 19.0%. There are no statistical differences regarding complication rate between the groups (p = 0.66, Table 3). For obvious reasons, capsular contracture did not occur in the autologous reconstruction groups. Flap failure and partial necrosis of the flap did not occur in implant-based groups. Revisions rates were similar in all groups (p = 0.53). When comparing TRAM to DIEP, total flap loss occurred at a similar rate; however, there was a higher need for reoperation in the TRAM group (18.2% vs 11.2%), although this difference did not reach significance (p > 0.05). Only in the TRAM group, one patient suffered from bulging. When comparing implant-based reconstruction types to autologous reconstruction types, the postoperative infection rate is similar; however, the need for reoperation is relatively higher in implant-based reconstruction types (13.6% vs 9.6%), although not significantly different (p > 0.05).
Complications.
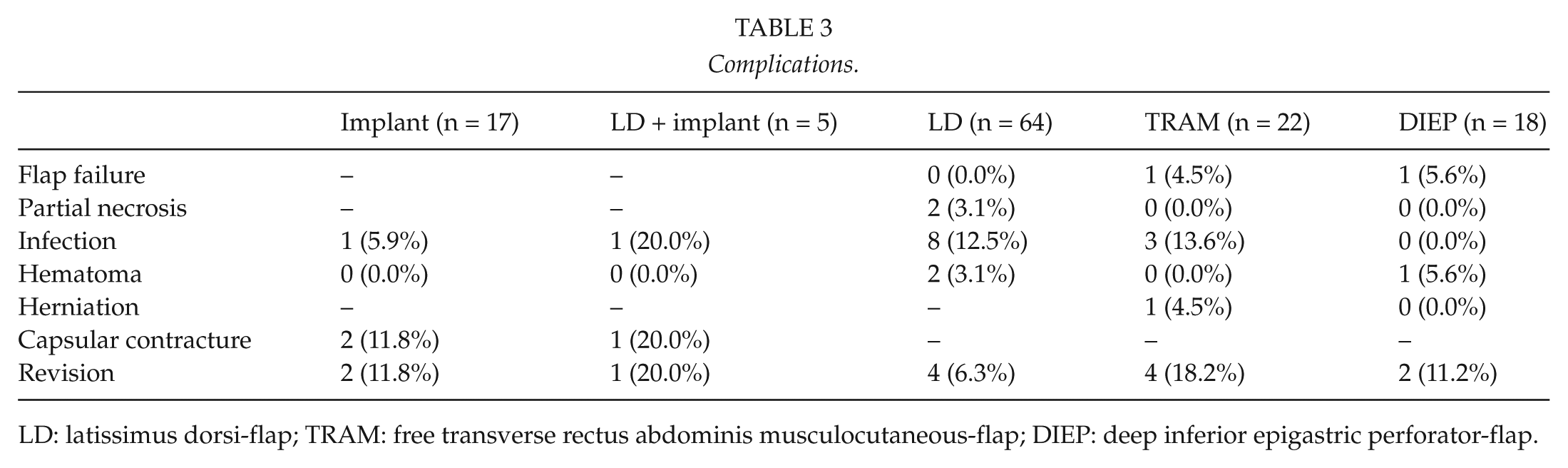
LD: latissimus dorsi-flap; TRAM: free transverse rectus abdominis musculocutaneous-flap; DIEP: deep inferior epigastric perforator-flap.
Patient Satisfaction
The questionnaire revealed that there were no statistical differences between the different reconstruction types regarding postoperative pain score and the recovery time to preoperative status (p = 0.07 and p = 0.06, respectively, Table 4). Also the answers regarding impairment on daily life and physical activity revealed no differences between the groups. In contrast, responses to the question regarding general satisfaction revealed that women who underwent a reconstruction with a DIEP-flap were significantly more satisfied with the overall result as compared to patients from the implant group (p = 0.007). Also, TRAM and DIEP patients answered more frequently that they were “fully satisfied” as compared to patients from implant-based groups (p = 0.004). Finally, the results of the questionnaire showed that the majority of the patients from all groups would recommend the same type of reconstruction to a close relative or family member. This result was irrespective of the undergone reconstruction type.
Survey results per reconstruction type.
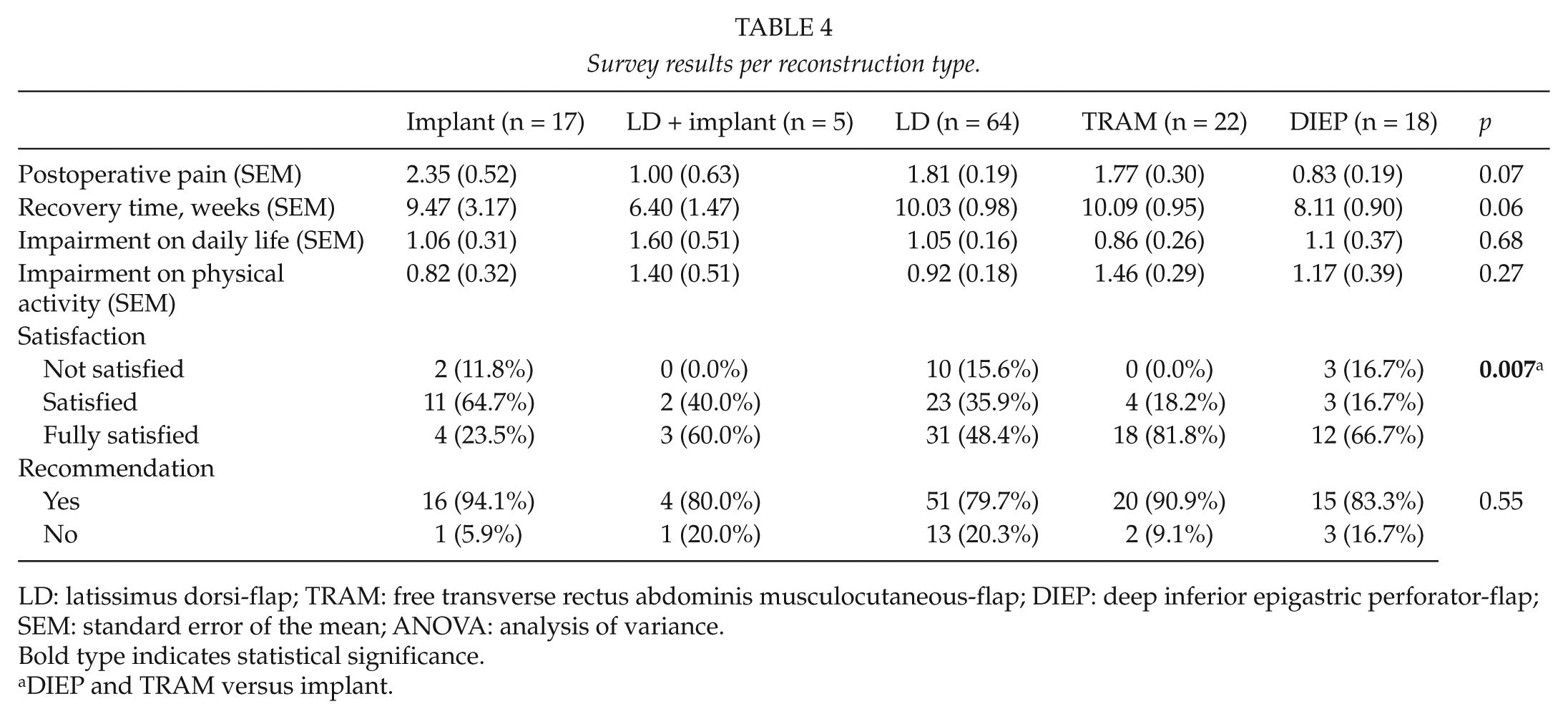
LD: latissimus dorsi-flap; TRAM: free transverse rectus abdominis musculocutaneous-flap; DIEP: deep inferior epigastric perforator-flap; SEM: standard error of the mean; ANOVA: analysis of variance.
Bold type indicates statistical significance.
DIEP and TRAM versus implant.
In addition, general QoL as assessed by SF-36 was similar among the groups (Table 5). Accordingly, when analyzed per section, no differences between the groups were found in the section describing physical health (i.e. physical functioning, physical role functioning, bodily pain, and general health). Also, when assessing mental health–related items (i.e. vitality, social functioning, emotional role functioning, and mental health), no differences were found between the different reconstruction types.
Quality of life as surveyed by SF-36 per reconstruction type.
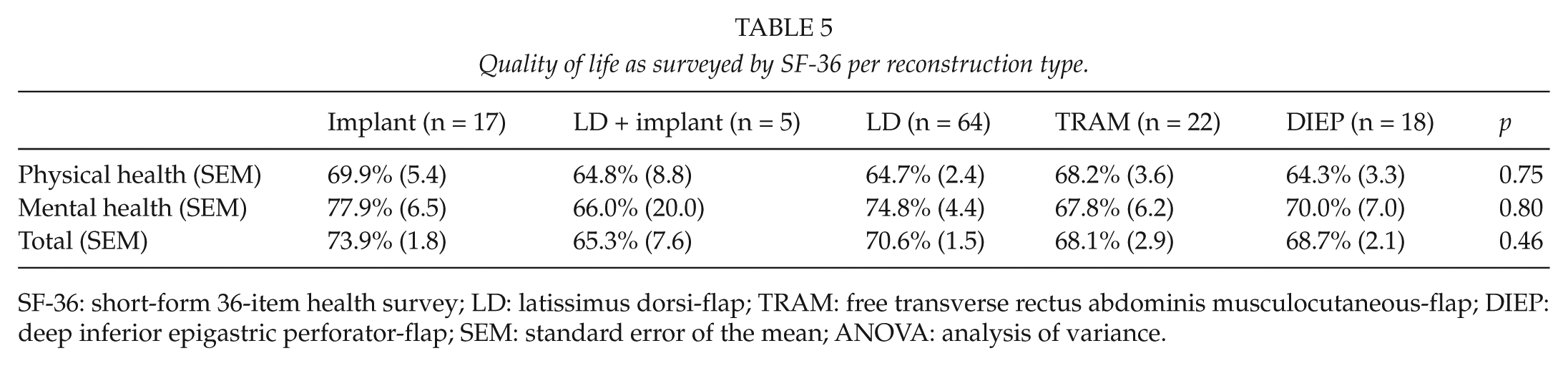
SF-36: short-form 36-item health survey; LD: latissimus dorsi-flap; TRAM: free transverse rectus abdominis musculocutaneous-flap; DIEP: deep inferior epigastric perforator-flap; SEM: standard error of the mean; ANOVA: analysis of variance.
Factors in Satisfaction
Multivariate analyses were used to assess the effects of different variables on patient satisfaction. To find variables that may affect satisfaction, we performed univariate analysis using the study population as a whole. Variables included in the satisfaction analysis were overall complication rate, revision rate, reconstruction type, “impairment on daily life,” and QoL as measured by total SF-36 scores. This combined multivariate model showed significance regarding effects on general satisfaction (p = 0.029). However, when excluding “impairment on daily life” from this model, no statistical significant effect was found regarding satisfaction. On the contrary, when including “impairment on daily life,” but excluding SF-36 scores, levels of correlation with satisfaction increased. We then performed stepwise logistic regression to ensure that only those variables significantly influencing general satisfaction were included in the final logistic regression analysis. After multiple eliminations, the only factor that continued to play a significant role in general satisfaction was “impairment on daily life.” Patients who reported a greater impairment on daily life had decreased odds of being satisfied (odds ratio (OR): 0.6, 95% confidence interval (CI): 0.40–0.91, p = 0.017). Both reconstruction type and complication and revision rates failed to show a statistically significant correlation with general satisfaction levels.
Discussion
This study assessed long-term patient satisfaction in 126 postmastectomy patients with five different types of breast reconstruction. Our results indicate that contrary to operation type, complication rate, and revision rate, only “impairment on daily life” was independently correlated with patient satisfaction.
As body image and physical integrity is of pivotal importance in QoL, it is of no surprise that there is a vast body of evidence showing the devastating effects of breast cancer and cancer-related mastectomy on QoL (15–17). Breast reconstruction has been shown to significantly ameliorate this burden on mental well-being and body image (18, 19). However, there is still controversy over factors being involved in patient satisfaction after breast reconstruction.
In our study, the overall major complication rate of 4.0% is within range of what is reported in the literature (20–22). Several studies that assessed correlations between patient satisfaction and complications have shown a lack of correlation between the two (21, 22). In line with these previous studies, when analyzing our data by logistic regression, complication rate did not show to be an independent factor in patient satisfaction. On the contrary, recent work by Colakoglu et al. (19) shows that patients having a complication from breast reconstruction were about 60% more likely to be aesthetically dissatisfied than those without a complication. This discrepancy could be explained by the difference in follow-up, which was on average 23.3 months in Colakoglu et al.’s study versus 38.4 months in our study. It has been well documented that postreconstruction satisfaction rates decline over time (23). Therefore, when analyzing long-term patient satisfaction, it might be increasingly more difficult to show differences in satisfaction.
Even though reconstruction type and its effect on patient satisfaction had been an extensively studied topic (24), there is no general consensus on how the type of reconstruction being performed correlates with patient satisfaction. However, an increasing body of evidence is elucidating certain aspects of this topic. There is a general consensus suggesting that autologous reconstructions result in significantly increased patient satisfaction when compared to implant-based reconstructions (11, 25). This is in line with our findings showing that women who underwent an autologous reconstruction were significantly more “fully satisfied” as compared to women undergoing a reconstruction solely using an implant. However, this did not show in QoL scores nor did this reflect whether women would recommend their chosen procedure to other women. Moreover, there was no significant correlation between patient satisfaction and type of reconstruction.
When comparing patient satisfaction of LD patients to patients who underwent an abdominal-based reconstruction, our data failed to show significant differences regarding general satisfaction and QoL scores. This is similar to data reported by Spear et al. (10), showing no difference in patient satisfaction in a population of 79 breast reconstruction patients of which 13 LD-based reconstructions. Also, Brandberg et al. (25) showed in a prospective randomized trial no correlation between satisfaction and type of reconstruction in 75 patients (pedicled TRAM vs LD-flap vs lateral thoracodorsal flap). Conversely, there are data indicating a significant difference in patient satisfaction between LD and abdominal-based reconstructions (20). However, in this study, the majority of LD patients were reconstructed also utilizing an implant (90 with vs 26 without). As patients who underwent an LD + implant–based reconstruction can have complications from the autologous tissue as well as from the implant, these satisfaction levels might resemble implant-based satisfaction levels. This possibly explains the found difference in patient satisfaction in their study.
Previous studies examining outcomes of abdominal flap reconstruction have analyzed differences in abdominal wall function, donor-site morbidity, hospital stay, and complication rate (26). Few data, however, can be found on patient satisfaction comparing abdominal-based reconstructions. In a recent study by Momoh et al. (27), 120 DIEP patients were compared to 114 pedicled TRAM patients. The authors were able to show a significant difference in general satisfaction in favor of DIEP. However, when assessing aesthetical satisfaction in the aforementioned study, no significant differences were found. Conversely, our data show no differences between free TRAM and DIEP reconstructions regarding general satisfaction or QoL. Although free and pedicled TRAM-flaps showed similar satisfaction scores in a previous study (25), differences might rely on the fact that our study was a head-to-head comparison of free TRAM versus DIEP instead of pedicled TRAM versus DIEP. On the contrary, greater impairment in abdominal wall function in TRAM as compared to DIEP patients has been described in previous literature (26). Therefore, a questionnaire with more specific questions addressing abdominal donor-site morbidity might have resulted in a difference in patient satisfaction between TRAM and DIEP reconstructions.
A number of limitations to the study herein ought to be addressed. First, for obvious ethical reasons, patients cannot be randomized for reconstruction type. Therefore, one unavoidable limitation is selection bias. Another inherent limitation in questionnaire-based studies is responder bias. Although, in baseline, responders were in all characteristics and complication rates comparable to nonresponders, it is still possible that highly satisfied or highly dissatisfied patients were more willing to respond to the questionnaire. Also, our data need to be replicated by a valid and reliable, surgery-specific patient-reported outcome measure, such as BREAST-Q (28). Unfortunately, as the BREAST-Q was only available in English at the start of the study, this questionnaire could not be employed in this German-speaking patient population.
In conclusion, the study herein indicates that neither complication rate nor operation type is an independent predictor of patient satisfaction. The fact that only “impairment on daily life” correlated with satisfaction reflects that patient satisfaction is very much determined by subjective patient experiences of everyday living. However, in order to be able to improve outcome and specifically satisfaction, future studies focusing on elucidating preoperative factors affecting those postoperative daily experiences are needed. Perhaps research fields such as patient education (29), patient expectations, and personality characteristics deserve thorough attention in the context of breast reconstruction. In the end, it is our responsibility to guide patients through the decision-making process regarding their individual needs.
Footnotes
Acknowledgements
The authors are most grateful to Nina Gösseringer for her help in data collection.
Declaration of Conflicting Interests
None of the authors have any commercial associations or financial interests to disclose.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.