
Abstract
Background and Aims:
To evaluate the efficacy and safety of a modified laparoscopic ureterolithotomy for the treatment of upper ureteral stones; this method involved the use of a Carter–Thomason fascial closure device, a broken 15th blade.
Material and Methods:
From February 2009 to December 2012, 38 patients with unilateral upper ureteral stones were examined and classified into 2 groups: one group underwent conventional laparoscopic ureterolithotomy (n = 21) and the other group underwent modified laparoscopic ureterolithotomy (n = 17). The modified laparoscopic ureterolithotomy consisted of the use of a Carter–Thomason fascial closure to extract the black silk along with the nylon tape. The ureter incision was made with a modified instrument consisting of a needle holder with a broken 15th blade tip.
Results and Conclusions:
Patient demographics were similar in both groups. No significant differences were detected between the conventional laparoscopic ureterolithotomy and modified laparoscopic ureterolithotomy groups with respect to operating time, estimated blood loss, and stone clearance rates. Drain-indwelling times were significantly shorter in modified laparoscopic ureterolithotomy patients than in conventional laparoscopic ureterolithotomy patients (3.2 ± 1.3 vs 4.7 ± 1.5 days). Hospital stay was significantly lesser in modified laparoscopic ureterolithotomy patients than in conventional laparoscopic ureterolithotomy patients (4.3 ± 1.2 vs 5.2 ± 1.2 days). No differences were detected in the ureteral stent indwelling time for the two groups. The use of the Carter–Thomason fascial closure facilitated ureter handling, and the use of a needle holder with a broken 15th blade tip enabled a sharp and precise ureteral incision. Our method allows early removal of the drain and thus earlier patient discharge.
Introduction
Upper and middle ureteral stones are controlled by using extracorporeal shock-wave lithotripsy, transureteral lithotripsy, or percutaneous lithotripsy. In patients presenting with impacted large stones, particularly those located in the proximal ureter, open surgery provides the benefit of removing the stone in one procedure (1, 2).
The use of laparoscopy in the field of urology has progressed significantly in recent years. Laparoscopic surgery is superior to open surgery with regard to the cosmetic outcomes, which leads to greater patient satisfaction. It is also effective in reducing postoperative pain, problems related to large open wounds, blood loss, and the length of hospital stay. Laparoscopic ureterolithotomy as a minimally invasive treatment has been continuously gaining importance in the treatment of urinary stones, mainly replacing open surgery (3).
Laparoscopic ureterolithotomy can effectively suppress the superior shift of stones to the renal pelvis and prevent residual stones due to the large burden of primary stones. To maximize the therapeutic benefit of laparoscopic ureterolithotomy, we developed a modified method based on the use of the Carter–Thomason fascial closure and a needle holder with a broken 15th blade tip.
This study describes a modified laparoscopic ureterolithotomy (MLU) method and compares it with conventional laparoscopic ureterolithotomy (CLU). In this retrospective study, we evaluated the efficacy and safety of MLU for the management of large proximal ureteral stones.
Materials and Methods
We retrospectively reviewed the medical records of 38 patients who underwent laparoscopic transperitoneal ureterolithotomy for large proximal ureteral stones during the period between February 2009 and December 2012. Patients with stones less than 1.5 cm in size, previous transperitoneal surgical procedures, acute urinary tract infection (preoperative fever and elevated white blood cell count), abnormal coagulation test results, distal ureteral stricture, or absolute contraindication for laparoscopic surgery were excluded from the study.
The initial indications were large (more than 1.5 cm) middle to upper ureteral stones (above the upper margin of the sacroiliac joint), impacted stones, concomitant laparoscopic surgery for a different indication, and need for stone removal in a single management session. Demographic data of patients who underwent laparoscopic ureterolithotomy were recorded, including age, body mass index (BMI), and stone side, location, and size. Stone size (maximal diameter) and location were assessed by abdominopelvic computed tomography or intravenous pyelography.
Operative outcomes, including stone clearance rate in a single session, operation time, and estimated blood loss, were assessed. Stone clearance was defined as the absence of residual stone fragments, as evaluated by plain radiography after surgery. The presence of a residual stone in a postoperative image was designated as a failure.
Drain indwelling, ureteral stent indwelling, and hospital stay were also recorded. Postoperative complications, including open conversion, prolonged ileus, gonadal vessel injury, and intestinal injury, were analyzed in the two groups. General anesthesia was used for all patients. After placing the patient in a semilateral position, a skin and fascial incision (1.2 cm) was made lateral to the rectus muscle at the level of the umbilicus, and a 10-mm balloon trocar was introduced to guide the surgical scope. The abdomen was insufflated with CO2 gas through the initial trocar. In CLU, the other two trocars (10 and 5 mm) were inserted under laparoscopic vision, parallel to the first trocar in an equilateral triangle pattern. In MLU, two 5-mm trocars were inserted consecutively for the working channels. A fourth 5-mm trocar was occasionally used for liver retraction in right-sided cases. The descending colon was reflected from its retroperitoneal attachment to move the colon medially, and the ureter was identified on the major psoas muscle. The ureter segment containing a stone was identified by a prominent bulge on a suspicious lesion. To avoid upward movement of the calculi, efforts were made to avoid touching the ureter directly, and cranial dissection was performed. In CLU, the upper segment of the ureter above the stones was isolated and clamped with a laparoscopic becop clamp to prevent the superior shift of stones. In MLU, the proximal ureter with the stone was pulled with nylon tape and black silk. The nylon tape was used to surround the ureter, and a small clip was applied. The clipped tape was pulled with black silk 1-0, and the direction of the traction was adjusted to facilitate handling of the ureter. A Carter–Thomason closure device was used to guide the black silk outside the body, and the traction and angle were adjusted (Fig. 1). The black silk was clamped using mosquito forceps, which enabled modification of the traction without loosening.
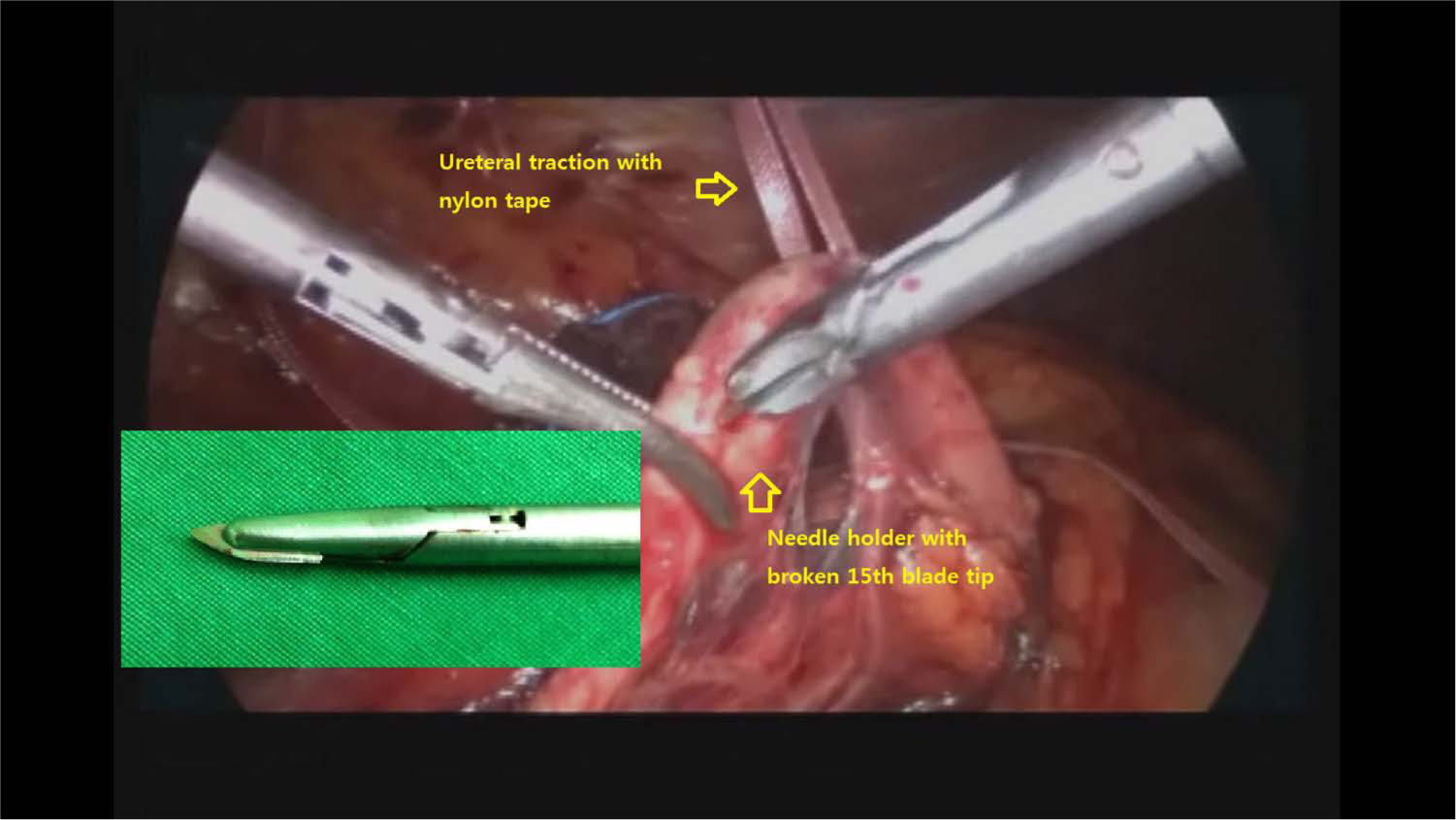
Operative field before ureteral incision: traction with nylon tape, enabled by the use of Carter–Thomason fascial closure and black silk outside the body. Modified instrument for incision: needle holder with a broken 15th blade tip at the stone level.
In CLU, the ureteral incision was made using laparoscopic scissors. In MLU, a modified instrument consisting of a needle holder with a broken 15th blade tip was used, which enabled a sharp and precise ureteral incision at the level of the stone (Fig. 1). The stone was removed by a grasper.
Next, the ureter was catheterized using a standard 6F double-J stent. In CLU, the guide wire was inserted through the single side hole of the double-J stent placed into the bladder through the ureteral incision site. After removal of the guide wire, the proximal end of the double-J stent was placed in the renal pelvis through the incision site.
In MLU, the traction on the ureter and the level were readjusted to facilitate the insertion of the ureteral catheter. Long and short guide wires were inserted through the two separate side holes of the stent that were closed at both ends. The stent was then inserted in a bidirectional manner through the ureteral incision site, and the two guide wires were removed.
The incision was closed with 4-0 vicryl interrupted sutures. In MLU, the traction on the ureter was adjusted to optimize the space and angle for suturing. A drain was inserted and the stone was extracted in a sac through the 10-mm camera port site. Routine antibiotic therapy was used to avoid infection. On postoperative day 1, a simple abdominal image was obtained to confirm the absence of remnant stones and check the position of the double-J stent. The entire MLU procedure was made available for review by a video journal (4).
The drainage tube was removed after a drainage volume < 30 mL/day was achieved, and the ureteral stent was removed by cytoscopy under local anesthesia in the two groups. To compare the 2 groups, a match-paired analysis was performed considering all variables. All the data analyses were performed by univariate analysis using the Mann–Whitney U-test or Pearson’s chi-square test. The statistics program SPSS version 12.0 (SPSS Inc., Chicago, IL) was used, and p values below 0.05 were considered statistically significant.
Results
Demographic and clinical characteristics of the patients in each group are shown in Table 1. Of the 38 patients included in the study, 9 (23.6%) were women and 29 (76.3%) were men. Upper ureter stones were present in 27 (71.0%) patients, and middle ureter stones were detected in 11 (29.0%) patients. Patient demographics were similar in both groups.
Patient demographic data.
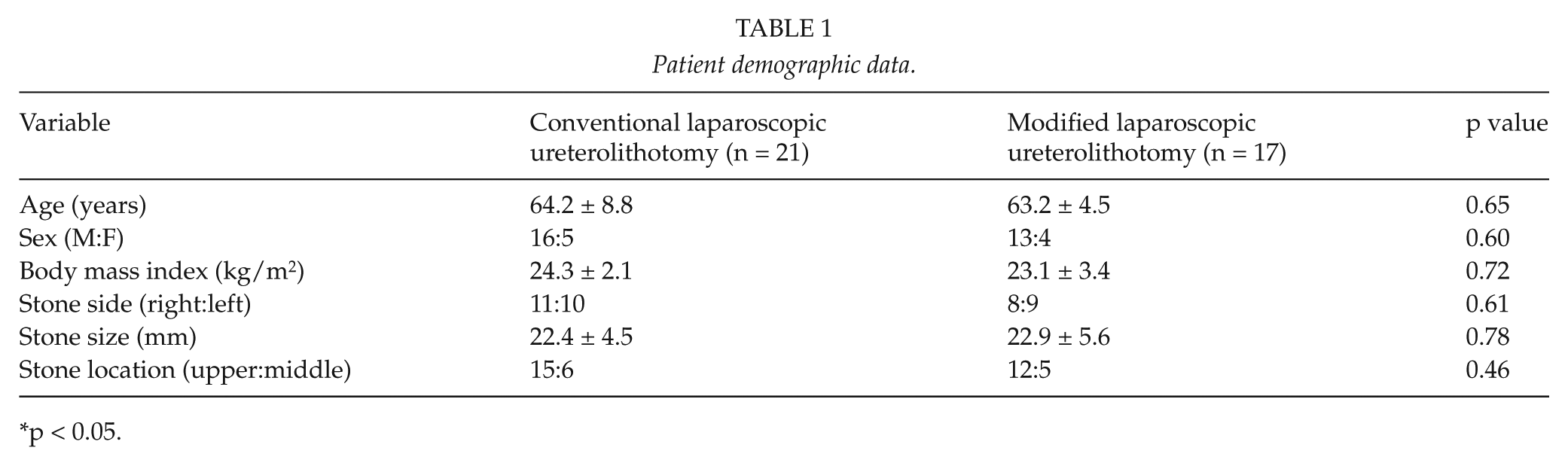
p < 0.05.
A comparison of intraoperative and postoperative parameters is shown in Table 2. Surgery was successful in all but two cases where small remnant stones were detected. In one patient in the CLU group, the remnant stone was pushed upward into the renal pelvis. The patient was treated with shock-wave lithotripsy, and he became stone-free after treatment. One patient in the MLU group had a very small stone that did not require treatment.
Intraoperative and postoperative characteristics.
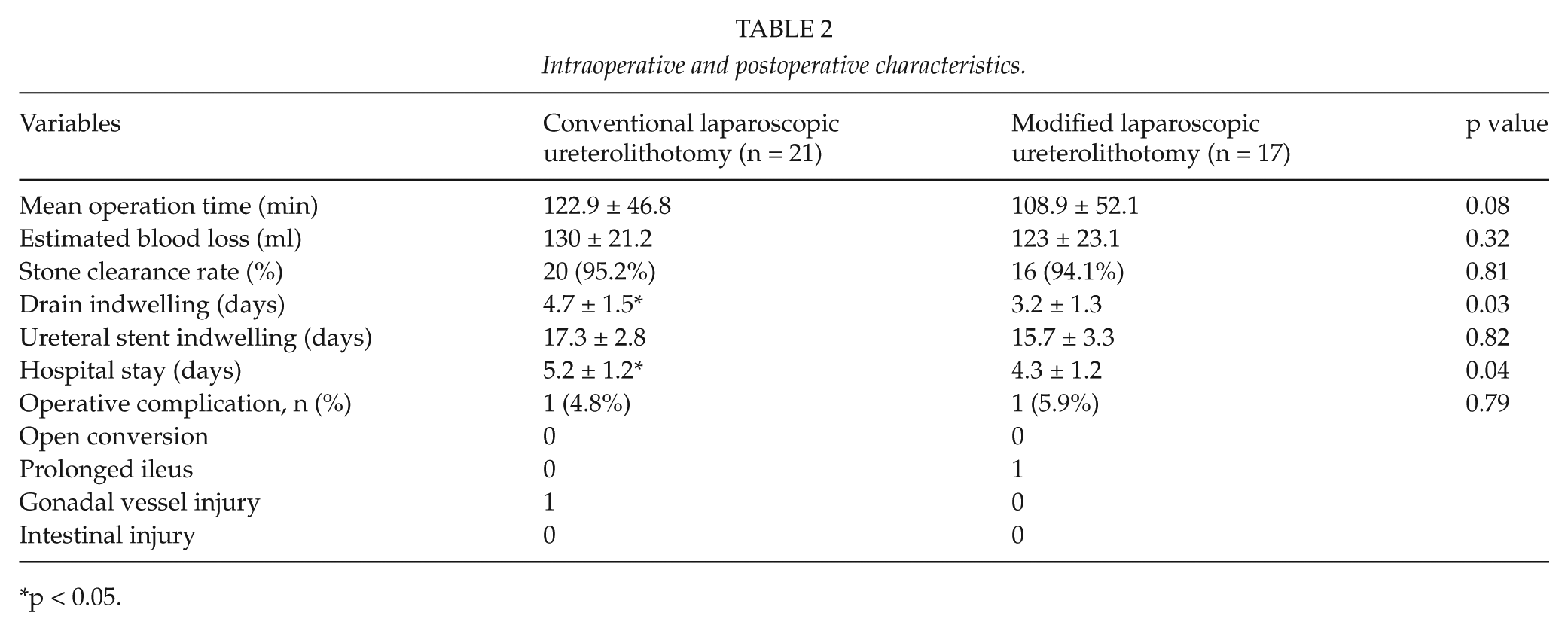
p < 0.05.
The stone clearance rates and estimated blood loss were similar in the CLU and MLU groups. The mean operating time was shorter in the MLU than the CLU group, but the difference did not reach statistical significance (108.9 ± 52.1 vs 122.9 ± 46.8). Drain-indwelling time was significantly shorter in patients who received MLU than in those treated with CLU (3.2 ± 1.3 vs 4.7 ± 1.5 days). Hospital stay was significantly lesser in MLU patients than in CLU patients (4.3 ± 1.2 vs 5.2 ± 1.2 days). The ureteral stent indwelling time did not differ between the two groups. Hydronephrosis significantly decreased and its clinical symptoms improved and eventually disappeared in all patients.
The rate of complications was similar in the two groups, and conversion to open surgery was not required in any of the cases analyzed. One MLU male patient required reinsertion of the nasogastric tube because of symptoms of nausea with ileus on postoperative plain radiographs. He recovered with conservative management after 3 days. Gonadal vessel injury occurred in one CLU patient and was immediately controlled by using a hemolock clip. Blood transfusion was not necessary in any of the cases analyzed.
Discussion
Urolithiasis is the third most common disease of the urinary tract and has high recurrence and morbidity (5). The treatment of urinary stones has advanced significantly in the last few decades. The development of endoscopic lithotripsy devices has allowed the widespread use of ureteroscopic lithotripsy for the treatment of small ureteral stones. However, the treatment of choice for large proximal ureteral stones remains controversial (6). Minimally invasive therapies in the form of endoscopic surgery in conjunction with the advent of shock-wave lithotripsy have diminished the role of open stone surgery. Currently, a preferred noninvasive alternative to open surgery is laparoscopic ureterolithotomy (7).
Since the introduction of laparoscopic ureterolithotomy, the laparoscopic approach has increasingly begun to replace open surgery for the management of ureteral stones. In general, laparoscopy has certain obvious advantages over open surgery, such as a shorter hospital stay, a better cosmetic outcome, and faster recovery (8, 9). On the other hand, laparoscopy often involves longer operative times and greater blood loss than ureteroscopy. Moreover, laparoscopy is associated with a risk of abdominal organ injury and conversion to open surgery (10).
We developed a MLU method aimed at maximizing the advantages and minimizing the disadvantages of the laparoscopic approach. All patients underwent transperitoneal laparoscopic ureterolithotomy, which is more common than the retroperitoneal approach and therefore more familiar to the urologic surgeon, in addition to providing a wider working space and a clearer view of familiar anatomical landmarks (7, 11).
For CLU patients, two working trocars (10 and 5 mm) were used together with a 10-mm balloon trocar to guide the surgical scope. For two CLU right-sided patients, a fourth 5-mm trocar was used for liver retraction. On the other hand, the MLU was performed with 5-mm working trocars in all patients. The use of the Carter–Thomason fascial closure device and black silk to pull the ureter provided adequate access to the operating field, making the use of an additional port unnecessary. This traction system was also effective for preventing the upward migration of the stone.
During CLU, the upper segment of the ureter was clamped with a 10-mm laparoscopic becop clamp to prevent the superior shift of stones. A 10-mm working port was used for stone retrieval and for insertion of the suture needle and gauze. Therefore, a 10-mm working port was required. On the other hand, in the MLU method, a laparoscopic sac was used for stone retrieval and gauze removal, and a 10-mm scope trocar was used for insertion of the suture needle and gauze. Consequently, patients undergoing MLU had better cosmetic outcomes and lesser trocar placement–related pain than the CLU patients.
No significant differences were detected between the CLU and MLU groups with respect to the mean operating time, estimated blood loss, and stone clearance rate. In the modified method, the mean operating time was slightly shorter than in the conventional method (108.9 vs 122.9 min), but the procedure was not technically superior to that used in previous reports (12, 13). Al-Sayyad (12) reported a mean operative time of 107 min with a range of 70–250 min, and Huri et al. (13) reported a mean operative time of 124 min. Although the differences in operative time in this study were not statistically significant, the modified procedure based on pulling the ureter provided a superior operative field for ureter incision and suturing, and the modified stenting method contributed to the shorter operative times. These improvements in the surgical technique may result in more significant differences in operative time in the future.
The MLU procedure was associated with significant improvements over CLU, such as drain-indwelling time (3.2 ± 1.3 vs 4.7 ± 1.5 days) and hospital stay (4.3 ± 1.2 vs 5.2 ± 1.2 days), which could be due to several factors. The use of a needle holder with a broken 15th blade tip enabled a sharp and precise ureteral incision at the level of the stone. Compared with the use of laparoscopic scissors, our modified method resulted in a clean incision surface. Furthermore, the traction on the ureter provided a wider working space and improved the incision angle. The optimal direction of the traction and the best angles for incision of the ureter and suturing were defined before the insertion of the Carter–Thomason closure device. Actually, this fascial closure system is designed to prevent port-site herniation, a potential complication of minimally invasive surgeries. This device enables surgeons to close trocar sites efficiently and reliably. We used this device to extract the silk to pull the nylon tape encircling the ureter, extracorporeally. This method provided good access for suction or additional dissection during ureteral incision, and ambidextrous handling of the suture was possible without the risk of destroying surrounding structures. Watertight suturing was possible because of the improved suturing angle and superior surgical field. The ureter traction tension and level were readjusted to facilitate the insertion of the ureteral catheter. The insertion of a both-end-closed ureteral catheter in a bidirectional manner via the use of two guide wires was technically feasible. The narrow space of the ureteral incision site made it difficult to operate when the double-J stent was twisted in the operating field. Better exposure of the incision site achieved by traction and bidirectional stenting led to a clear improvement in operative efficiency.
One case of gonadal vessel injury occurred during ureteral manipulation in CLU due to a poor operative view, underscoring the advantages of the modified method with regard to the safety of the surgical procedure. In the Korean Health Care System, which is nationwide and mandatory, the hospital admission cost is maintained at a minimum compared with that of other systems. Therefore, the hospitalization period in this study was not superior to that in previous reports. The overall hospital stay ranges between 3 and 4 days according to previous studies (14, 15). However, the modified method should result in less urine leakage and therefore an earlier discharge.
Our study has several limitations. Because a large amount of comparative data were not available, we could not reach a firm conclusion regarding the operative superiority of our modified method. Although we emphasized that these methods are effective, evidences are weak to support our hypothesis. The differences between the CLU and MLU are complex. In addition, this was a retrospective study and a comparative randomized controlled trial design was not possible. As for patient selection, we used laparoscopic ureterolithotomy as a primary procedure, but it is more likely that for some clinicians, laparoscopic ureterolithotomy will be reserved for those patients who require a salvage procedure after failed ureteroscopy or shock-wave lithotomy as a primary procedure. Concepts that include use of a broken knife could be dangerous in case of inattentive instrument handling. And passing of the Carter–Thomason to the abdomen not only needs another hole over the abdomen but may need cautious measures to prevent any visceral injury. Moreover, generally more activities and tissue manipulation are accomplished in MLU: insertion and adjusting the anchoring sutures and more dissection of the ureter to allow it to be pulled up. Nevertheless, the results of this study show that MLU allows the early removal of the drain after surgery and, therefore, a faster patient discharge. Furthermore, the modified method provided better cosmetic outcomes related to trocar placement and an improved surgical procedure with a cleaner incision and a wider surgical field for ureter suturing and stenting.
Conclusion
In conclusion, this study analyzed the outcomes of laparoscopic ureterolithotomy using a modified method and showed that compared to the CLU method, the modified method enabled the early removal of the drain after surgery and therefore a faster discharge of patients. The Carter–Thomason closure device facilitates ureter handling, and the use of a needle holder with a broken 15th blade tip enables a sharp and precise ureteral incision. Our results suggest that the MLU method is feasible for application in clinical practice.
Footnotes
Acknowledgements
The authors would like to acknowledge the work of J. G. Lee, D. G. Moon and M. M. Oh of the Department of Urology, Korea University College of Medicine in data collection and analysis for this article.
Declaration of Conflicting Interests
None.
Funding
This work was supported by a National Research Foundation of Korea (NRF) grant funded by the Korea government (MSIP) (No. 2011-0020128) and by the Soonchunhyang University Research Fund.