
Abstract
Background and Aims:
Treatment of occlusive femoro-popliteal artery disease has changed during the last decade because of intensive development of endovascular technology. The aim of this study was to evaluate patient treated endovascularly or surgically for femoro-popliteal atherosclerotic lesions and to assess perioperative and mid-term outcome.
Material and Methods:
This is a retrospective analysis of consecutive patients who had undergone prosthetic above-the-knee femoro-popliteal bypass or percutaneous transluminal angioplasty and stenting of superficial femoral artery stenosis or occlusion at Tampere University Hospital, Finland, between January 2007 and December 2009. Patients who were alive were re-evaluated in 2010. Primary and secondary patency and outcomes were assessed.
Results:
A total of 131 patients were treated; surgically 63 patients (69 procedures) and endovascularly 68 patients (74 procedures). The mean follow-up time was 17 months (SD ± 13 months). In the late follow-up visit, 8 (18%) patients in the bypass group suffered from claudication and 9 (20%) from critical limb ischemia. The corresponding figures for the endovascular group were 20 (36%) and 8 (20%), respectively. The primary patency was 60% at 2 years in the bypass group and 73% in the endovascular group (p = 0.092); the primary assisted patency was 62% versus 76%, respectively (p = 0.068). The secondary patency was 74% in the bypass group versus 79% in the endovascular group (p = 0.487).
Conclusions:
According to current results following TASC II guideline, satisfied overall mid-term results can be achieved in the treatment of superficial femoral artery atherosclerotic disease.
Keywords
Introduction
Peripheral arterial disease (PAD) often results in narrowing or occlusion of superficial femoral artery (SFA), which can lead to typical symptoms of PAD, for example, intermittent claudication (IC) or critical limb ischemia (CLI) (1). However, it has been estimated that roughly only one-third of PAD patients exhibit these typical symptoms (2). The overall prevalence of PAD steadily increases from the age of 50 years onward and is in the range of 3%−18%, increasing to 25%−30% in persons above 75 years. The prevalence of IC is around 7% in persons over 70 years, while the prevalence of CLI is approximately 1% (2).
PAD, regardless of the symptoms, has been associated with increased cardiovascular morbidity and mortality (3). The risk for cardiovascular mortality is estimated to be two- to four-fold among those with IC compared to those with normal ankle brachial index (ABI). The prognosis is even worse for CLI patients as their mortality rate is approximately 20% during the first year after presentation (1). The fate regarding lower extremities in IC patients is rather good, as in only 5%−10% of the patients, the disease progresses to CLI during the 5 years following the diagnosis, with 1%−3% eventually requiring major amputation. At the same time, up to 30% of the CLI patients require major amputation within 1 year after the diagnosis (1).
With the development of endovascular techniques, the number of patients receiving endovascular treatment for symptomatic PAD has increased steadily during the past decades (4). The major advantage of endovascular treatment is its noninvasive nature resulting in the decrease of treatment-related complications. However, among patients with CLI, surgical reconstruction is still often mandatory due to extensive arterial changes (1). Today, Transatlantic InterSociety Consensus document II (TASC II) provides a useful tool to identify arterial lesions most probably suitable for endovascular or surgical treatment. Atherosclerotic lesions are classified into four categories (TASC II A-D) depending on their extent and severity of stenosis (1). Category TASC II A-B SFA lesions are recommended to be treated endovascularly, and TASC II C-D lesions surgically. Patients with TASC II C lesions together with major comorbidities are, however, recommended to be treated by intraluminal means.
The purpose of this study was to evaluate patient characteristics, including TASC II SFA lesion classification, among individuals treated surgically or endovascularly for femoro-popliteal (SFA) atherosclerotic disease and to assess perioperative and mid-term outcome after different treatment modalities.
Material and Methods
Study Population
This is a retrospective analysis of consecutive patients treated for SFA stenosis or occlusion due to PAD at Tampere University Hospital (TAUH), Finland, between January 2007 and December 2009. Patients who had undergone above-the-knee femoro-popliteal bypass or percutaneous transluminal angioplasty (PTA) and stenting of SFA for the first time were included in the study. Patients with PTA only or patients presenting with acute lower extremity ischemia were excluded. Patients were followed until the end of September 2010.
Risk Factors for Pad and Other Comorbid Conditions
Data from the patients’ files were collected systematically by one investigator (H.L.). Review of the patients’ case records provided information on age, gender, diabetes mellitus, hyperlipidemia, hypertension, smoking within 5 years, coronary heart disease (CHD), cerebrovascular disease, respiratory disease, and chronic renal failure. The diagnosis for each disease was considered positive if it had been previously established at TAUH or mentioned in the referral, or if the patient was on appropriate medication. In addition, for chronic renal failure, creatinine level >150 µmol/L at presentation was considered as positive. Special attention was paid to preoperative antiplatelet and anticoagulant therapy as well as statin medication. Preoperative ABI was also recorded.
Preoperative Imaging and Indications for Procedures
All preoperative digital subtraction angiograms (DSA) were available for evaluation. The evaluation was performed by one investigator (H.L.). All lesions were classified retrospectively according to the TASC II classification (1). Indications for procedures were classified according to the Rutherford classification of PAD with an exception of mild and moderate claudication, which were grouped as one entity (5).
Procedures
The decision of treatment modality was always made together with both vascular surgeon and interventional radiologist, and it was based on patients’ overall status, symptoms, and angiogram findings. The use of particular vascular prosthesis or stent was chosen according to the surgeon’s or radiologist’s preference. The indications for using stent included significant residual stenosis (50%) and/or flow-limiting dissection after PTA. The length of stay, inhospital complications, and information on discharge (home and rehabilitation center) were also searched from the patients’ files and local vascular registry.
Follow-Up
Patients visited the vascular outpatient clinic 4 weeks after discharge from the hospital. In addition to ABI measurement, the patency of treated segment or vascular prosthesis was evaluated by clinical examination and duplex scanning. Possible postoperative complications were noted and registered in the local vascular register.
Patients were followed until death or major amputation of the treated lower extremity. Deaths were ascertained by means of record linkage of the study data with the National Causes of Death Register on the basis of the personal identification code unique to every resident in Finland. Additionally, follow-up ended if surgically treated patients had undergone distal secondary bypass, if the graft had occluded during the study period, if endovascularly treated patients had undergone surgical bypass, or if the stented segment had occluded (information from the patients’ files).
Patients who were alive, had not undergone major amputation, and had no information about secondary procedure or occlusions were invited to an additional follow-up visit in July–September 2010. Current lower extremity symptoms were noted, and thorough vascular surgical evaluation was performed (ABI measurement, clinical examination, and duplex scanning). Vessel or bypass graft patency (patent/occluded) was recorded. Altogether, 80% of all living patients (35 patients/45 extremities in the bypass group and 47 patients/56 extremities in the endovascular group) agreed to arrive for additional evaluation, 10% (5 bypass and 5 endovascular group patients) were interviewed over phone (subjective symptoms), and 10% (8 bypass and 3 endovascular group patients) denied their participation.
Patency
Primary patency was defined as a patent vessel or bypass graft without any additional procedures. PTA performed for graft or in-stent stenosis to ensure patency was regarded as primary assisted patency, whereas more extensive endovascular or surgical procedure (thrombolysis, stenting, and embolectomy) for occlusion/thrombosis was considered as secondary patency.
Statistical Analysis
SPSS 19.0 for Windows was used for statistical analysis (SPSS, Chicago, IL, USA). For discrete variables, analyses were made with the aid of cross-tabulations combined with χ2 tests, and comparisons of means between the two groups were carried out with the t-test for independent samples. Survival analysis with the log-rank test was used to examine primary, primary assisted, and secondary patency according to treatment modality. A p-value <0.05 was considered statistically significant.
Results
Study Population and Risk Factors
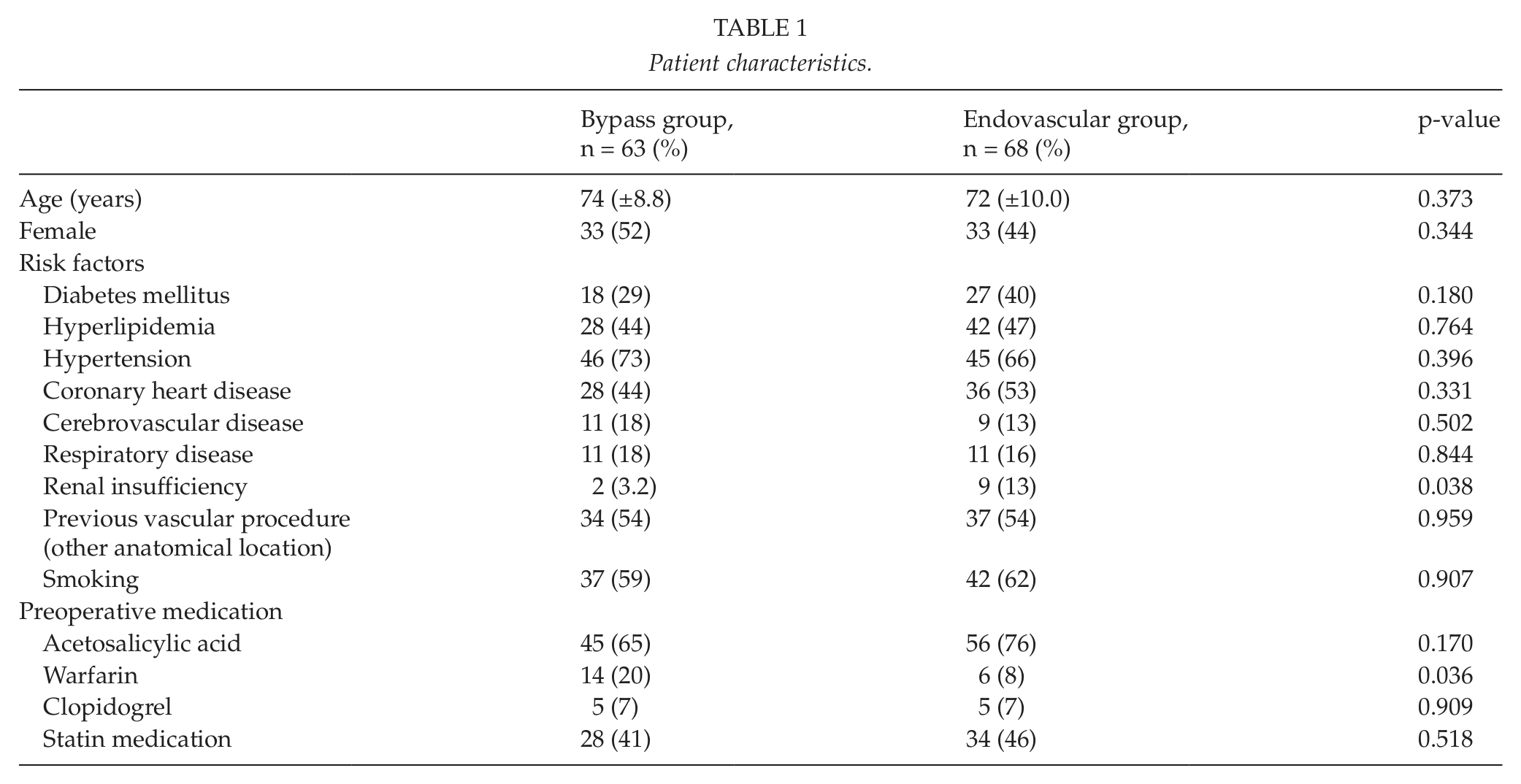
Altogether, 131 patients were treated for SFA lesions with above-the-knee femoro-popliteal bypass (63 patients and 69 procedures) or with PTA and stenting (68 patients and 74 procedures) during the study period. The mean age of the cohort was 73 (±9.1) years without significant difference between the treatment groups. PAD risk factors, other comorbid conditions, and preoperative medication are presented in Table 1. Renal insufficiency was found to be significantly more common in the endovascular group compared to the bypass group (p = 0.038). Additionally, patients who were treated surgically were significantly more often receiving warfarin therapy.
Patient characteristics.
Preoperative Imaging and Indications for Procedures
Table 2 characterizes the distribution of TASC II categories between the treatment groups. Although SFA lesions were classified retrospectively, the distribution seems to follow TASC II guidelines consistently, as 80% of the patients in TASC II groups A and B were treated endovascularly, while all patients in TASC II D group received surgical treatment.
TASC II and Rutherford classifications.
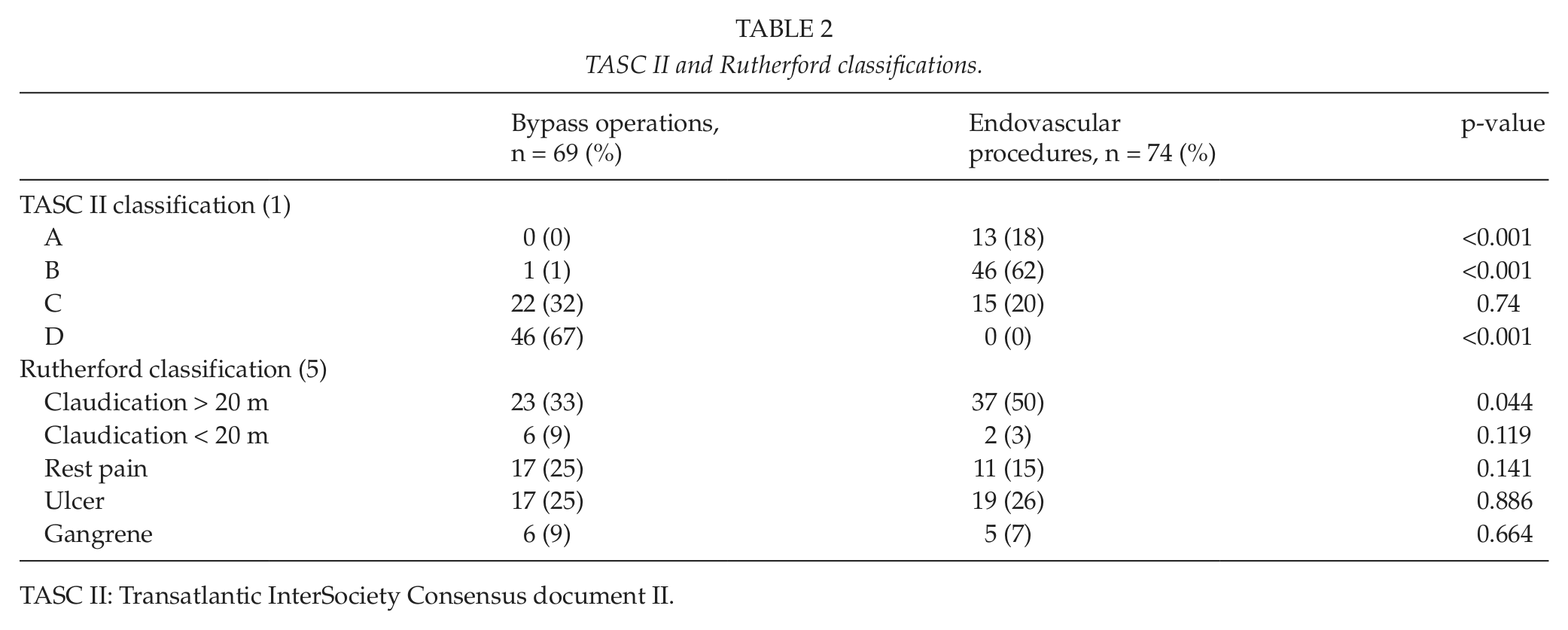
TASC II: Transatlantic InterSociety Consensus document II.
The primary indication for the procedure was claudication in 29 (42%) cases in the surgical group and 39 (53%) cases in the endovascular group, without statistically significant difference between the groups. However, mild/moderate claudication (Rutherford category I–II) was significantly more common in the endovascular group compared to the bypass group (50% vs 33%, p = 0.044). Other procedure indications (ischemic pain, ulcer, gangrene caused by CLI) were similar between the study groups (Table 2).
Procedures and Perioperative Characteristics
Polytetrafluoroethylene (PTFE) grafts were used in 66 (96%) cases and autogenous vein grafts in 3 (4%) cases in the bypass group. In the endovascular group, a total of 90 stents were used. Stent material was nitinol in 91% of the cases and stainless steel in 6% of the cases, while in 3% of the cases, the stent material was not specified. No covered stents were used.
Perioperative (30-day) complications are listed in Table 3. One (1.5%) cardiovascular death occurred in the endovascular group resulting in 0.7% overall perioperative mortality (p = 0.514 between the groups). Furthermore, one (1%) major amputation was required in the bypass group and two (3%) in the endovascular group (p = 0.532). As expected, wound infections and seromas were significantly more common in the surgical group. The initiation of clopidogrel medication after endovascular treatment (usually for 3 months) consequently resulted in a significant difference in its use between the groups (83% in endovascular vs 12% in surgical group, p < 0.001).
Perioperative patient characteristics and postoperative complications.
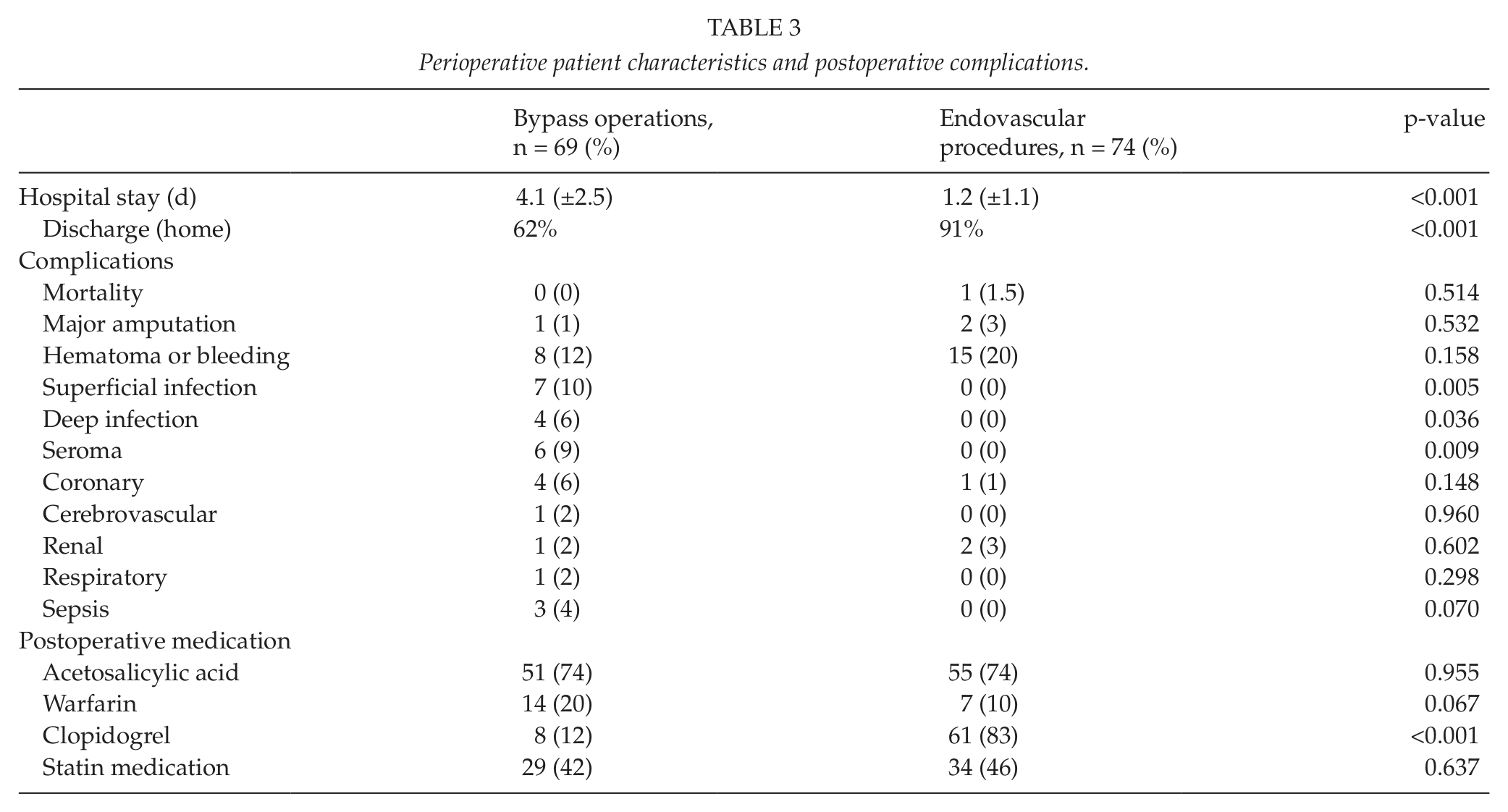
Hospital stay was significantly longer in the bypass group compared to the endovascular group (4.1 days, standard deviation (SD) ± 2.5 and 1.2 days, SD ± 1.1, respectively, p < 0.001) (Table 3). Moreover, surgically treated patients needed postoperative rehabilitation in a regional hospital or municipal health center ward significantly more often (38% vs 9%, p < 0.001).
Follow-Up
The mean follow-up time was 16 months (SD ± 13 months) in the bypass group and 18 months (SD ± 13 months) in the endovascular group. Altogether, 28 (21%) patients died during the follow-up (15 (24%) in bypass group and 13 (19%) in endovascular group, p = 0.28). The majority of the deaths were cardiovascular (16 (6%)).
At the 30-day follow-up visit, 81% of patients in the bypass group felt that their lower extremity symptoms were less than before the procedure. The respective figure for the endovascular group was 70%. At the same time, 1% of the patients in the surgical group and 3% in the endovascular group were complaining about worsened symptoms. ABI measurements showed marked increase in both treatment groups: the preoperative ABI was 0.45 (SD ± 0.25) in the surgical group and 0.59 (SD ± 0.18) in the endovascular group, while the figures at the follow-up visit were 0.88 (SD ± 0.23) and 0.85 (SD ± 0.23), respectively.
The late follow-up (including those who were interviewed over phone) revealed that 84% of the surgically treated patients regarded themselves less symptomatic compared to the situation prior to the initial procedure, while the corresponding proportion in the endovascular group was 91%. The symptoms per treated extremity according to the Rutherford classification during the evaluation at the outpatient clinic were 28 (62%) in Rutherford class 0, 8 (18%) in Rutherford class 1 or 2, and 9 (20%) in Rutherford class 4 or more in the surgical group, and 28 (50%), 20 (36%) and 8 (14%), respectively, in the endovascular group. These results were without statistically significant difference. The mid-term follow-up ABI was 0.71 (SD ± 0.41) for the surgical group and 0.82 (SD ± 0.28) for the endovascular group. The number of secondary procedures to maintain patency was significantly higher in the surgical group compared to the endovascular group (12 (17%) vs 5 (7%), respectively), thrombolysis being the most common procedure. Additional 6 (9%) major amputations were needed in the surgical group and 3 (4%) in the endovascular group during the follow-up (p = 0.244). The primary patency was 60% at 2 years in the bypass group and 73% at 2 years in the endovascular group (p = 0.092) (Fig. 1); the primary assisted patency was 62% in the bypass group versus 76% in the endovascular group (p = 0.068), and secondary patency was 74% in the bypass group versus 79% in the endovascular group (p = 0.487) (Fig. 2).
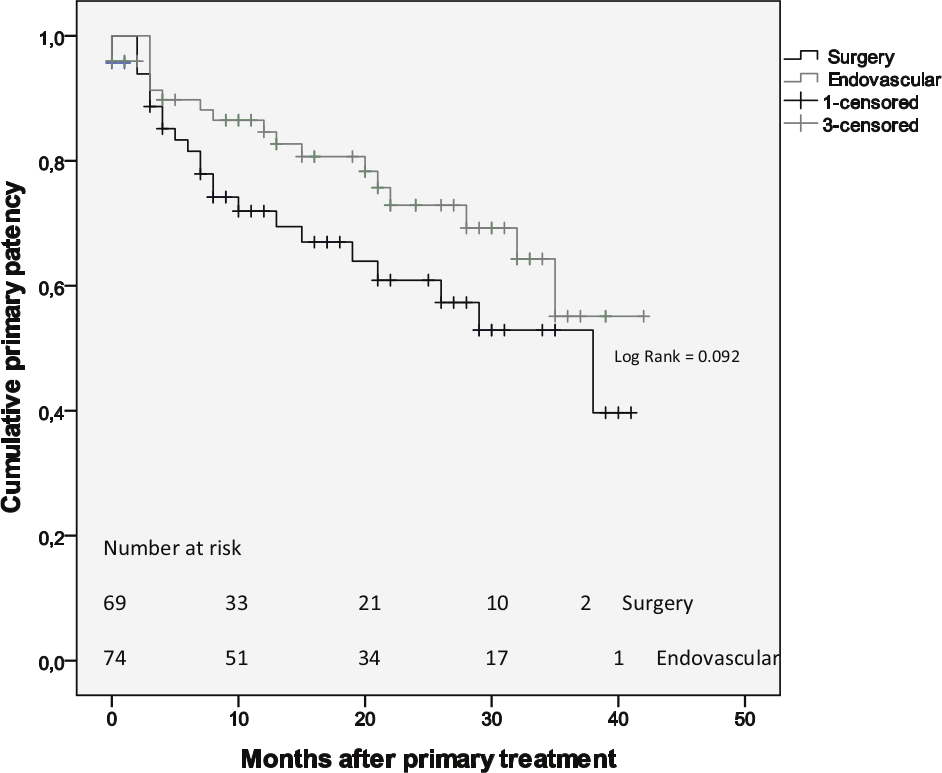
Cumulative primary patency: Kaplan–Meier survival analysis.
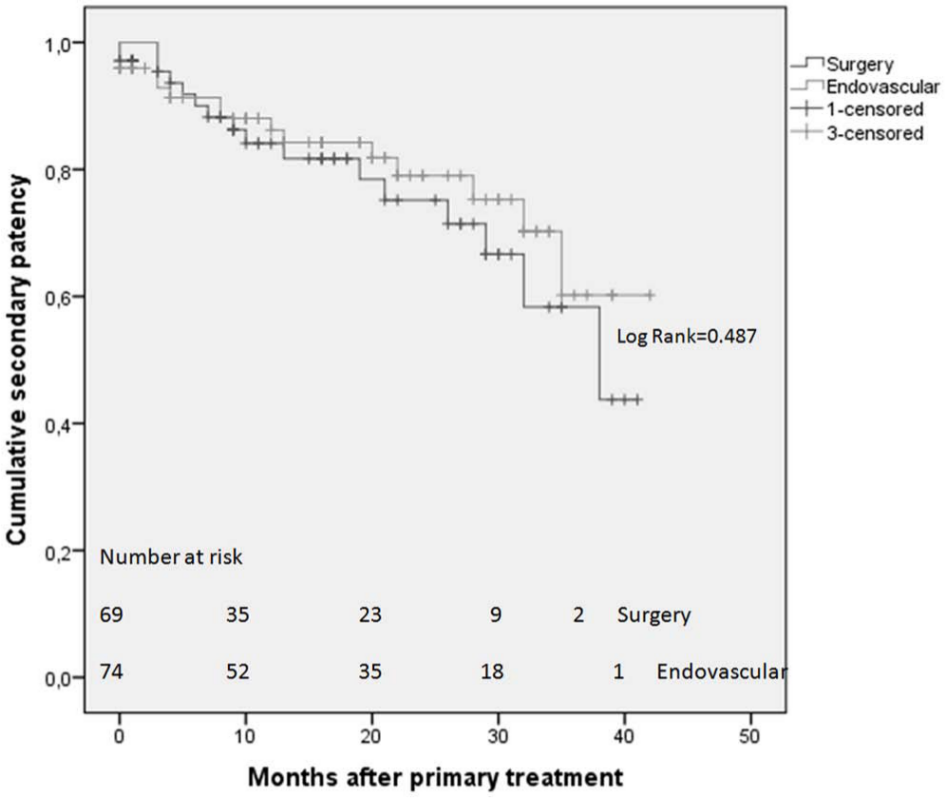
Cumulative secondary patency: Kaplan–Meier survival analysis.
Discussion
Our study shows that patient selection for the treatment of SFA atherosclerotic lesions followed almost invariably TASC II recommendations. Additionally, periprocedural morbidity was mainly due to surgical wound infections and seromas, and surgical patients required longer hospital stay and postoperative rehabilitation significantly more often. At the same time, mid-term results were similar in both surgical and endovascular groups with regard to symptom recurrence, patency, major amputations, and mortality.
The purpose of this study was to evaluate treatment strategy among individuals treated surgically or endovascularly for femoro-popliteal (SFA) atherosclerotic disease in an academic institution. The study setup does not allow us to make direct comparisons between treatment modalities as the patient groups are not similar with regard to the severity of atherosclerotic lesions or PAD risk factors. It has actually been shown in a randomized setting that roughly, only 10% of patients with CLI are suitable for both treatment methods, thus making the comparison of treatment modalities itself troublesome (6).
The initial purpose of TASC II classification was to give clinicians a useful tool to identify atherosclerotic lesions in the lower extremities most probably suitable for endovascular or surgical treatment (1). However, the document has raised criticism, and its reliability has been challenged. Recently, Kukkonen et al. (7) showed that when two independent reviewers analyze angiographic pictures and evaluate TASC II categories, the interobserver agreement was only 49%. They rightly conclude that the use of the classification as a basis for decision making should be questioned. Furthermore, according to Scali et al. (8), good long-term results in the treatment of SFA lesions can be achieved through profound consideration of not only anatomic but also patient-specific characteristics. In our cohort, the decision of treatment modality was always made together with vascular surgeons and radiologists, taking into consideration patients’ comorbidities. All TASC II type A and B lesions, except for one case, were treated endovascularly. Those 15 patients in the TASC II C group who were treated by endovascular means had significantly more comorbidities than their surgically treated counterparts. Patients with TASC II D lesions are traditionally treated surgically in our unit, and we have not adopted endovascular treatment for these patients contrary to some other centers (9, 10).
Length of hospital stay is an important economical issue today. In this study, patients treated with endovascular method had significantly shorter hospital stay and needed rehabilitation at regional hospital or municipal health center ward more rarely. This is probably explained by lesser procedural stress and fewer complications in the endovascular group. Postoperative complications after surgical procedures, such as superficial wound infections and seromas, can hardly be totally avoided and will most probably always cause somewhat prolonged hospital stay. Our results concerning the length of hospital stay and the prevalence of postoperative complications are in line with previous publications (4, 11). As the indications for procedures were similar in both groups, we cannot provide answer to why surgically treated patients required rehabilitation significantly more often. Had we been able to evaluate the functional status prior to the initial procedure, we would probably have found some data explaining the difference between the groups.
There was some discrepancy between patients’ subjective symptoms and satisfaction compared to recorded patency at the late follow-up. The underlying explanations can be various. It could reflect the overall activity level of the cohort with a limited need to walk outdoors or climb stairs, thus the current activity level not producing life restricting symptoms of CLI. Another explanation could be higher mortality among CLI patients, while among the surviving participants, with relatively short follow-up, the progression of PAD had not yet been realized. Interestingly, in our cohort, particularly in the endovascular group, patients regarded themselves less symptomatic during the late follow-up (70% at 1 month vs 91% at late follow-up), while the figure for the surgical group remained almost unchanged (81% vs 84%). The number of secondary interventions does not explain the difference as they were significantly less in the endovascular group. Our results are somewhat contradictory to previous results showing less symptom recurrence in the surgical group (11).
The literature on the treatment of SFA lesions is mounting (6, 11–17). However, the assessment of patency and overall results of different treatment modalities is somewhat problematic as study designs vary considerably. The Basil trial was the first randomized controlled trial (RCT) assessing treatment of SFA pathology in CLI patients (6). The results between bypass surgery and endovascular treatment were similar when the end point was major amputation. Furthermore, it has been shown that bypass surgery is associated with significantly better long-term leg salvage (18). Another RCT showed that bypass surgery is better when treating longer (5–15 cm) lesions (19). This is the conclusion of recent non-randomized studies as well (11, 16). Controversial opinions have also been published (16, 20, 21). According to Dosluoglu et al. (16), patients with TASC II type C lesions treated endovascularly had better patency than those treated surgically. Our results are quite similar to that of Dosluoglu et al. (16). Had we used autologous vein instead of PTFE grafts, we would probably have achieved better patency in the surgical group as it has been shown in the literature (22).
This study is affected by several limitations. First, this is a retrospective, non-randomized study, which causes unequal comparison between the groups. The retrospective nature also involves possible data issues associated with the use of hospital discharge histories and patient case records. However, the multiple admissions of the subjects to our hospital due to comorbidities prior to the initiation of this study made data collection easier and, we believe, more accurate. Furthermore, possible data errors and miscoding will be similar for both groups. The second limitation is the relatively small number of patients, which may limit the statistical validity of our findings and which prevented us from making further subgroup analysis. Another potential issue is the relatively short duration of the follow-up, which could have an impact on the results.
Conclusion
First-line treatment for patients with SFA atherosclerotic occlusive disease is yet to be determined. According to the current results, patient selection followed almost invariably TASC II recommendations. Furthermore, by following these guidelines, satisfied overall mid-term results can be achieved in the treatment of SFA atherosclerotic lesions. It should be emphasized, however, that such guidelines should always be used together with patient-specific factors when making final treatment decisions for an individual patient.
Footnotes
Declaration of Conflicting Interests
There is no potential or actual personal, political, or financial interest in the material, information, or techniques described in the article.