
Abstract
Background and Aims:
The mastery of manual skills that are indispensable for the performance of surgical tasks is a competence specific to surgery. One way of facilitating this acquisition is to move the training out of the operating room and all of its restrictions. Surgical training out of the operating room, also called simulation, has spread widely in the past decade, especially in laparoscopic and endoscopic surgery.
Material and Methods:
This review assesses the role of virtual reality (VR) simulators in laparoscopic surgery and their actual impact on technical skills.
Results and Conclusions:
There is a wealth of simulators, ranging from low- to high-fidelity simulators incorporating haptic feedback. They comprise basic tasks, procedural modules, and full procedures. Virtual reality simulators have shown acceptable fidelity and validity evidence. Moreover, training out of the operating room on virtual reality simulators has demonstrated its positive impact on basic skills during real laparoscopic procedures in patients. The benefit of virtual reality over simple video trainers remains unclear for teaching basic skills. However, virtual reality simulators provide automatic feedback that permitted to design structured competency-based curricula and allow deliberate practice. Finally, advanced procedures and patient-specific models have been designed on virtual reality simulators, and further investigations are still awaited to appraise their educational value.
Introduction
The mastery of manual skills that are indispensable for the performance of surgical tasks, which we call “surgical technical skill” (STS), is a competence specific to surgery (as there are technical skills specific to anesthesia, interventional radiology, or cardiology). According to Epstein (1), it represents one of the essential dimensions of professional competence. William Halsted introduced in 1889 the notion of surgical apprenticeship, based on the gradual transfer of tasks and responsibility. This system remains the cornerstone of surgical training more than a century later. However, its limitations are now growing due to both the evolution of surgical practice and the management of teaching hospitals (2). We can cite the following: the ethical question of surgery performed by a novice; the reduction of time residents spend in the operating room (OR) due to the compensatory rest; the economic pressure to optimize the use of OR; and the increasing medicolegal pressure. Furthermore, the acceleration of technical innovation increases the number of skills to be acquired and mobilizes teaching surgeons to their own acquisitions: this evolution is paramount in the field of laparoscopic and robotic surgery. One way of facilitating the acquisition of STS is to move the training out of the OR and all of its restrictions. The inspiration for this approach came from the aeronautics sector within which simulation has been used for over 50 years.
Surgical training out of the OR, also called simulation, has spread widely in the past decade, especially in laparoscopic and endoscopic surgery (2, 3). Furthermore, regulatory bodies such as the Society of American Gastrointestinal and Endoscopic Surgeons (SAGES) and the European Association of Endoscopic Surgeons (EAES) have promoted training both inside and outside the OR for laparoscopic surgery (4). Training tools may be inanimate models such as virtual reality (VR) simulators and video trainers (VT), as well as live animals or cadavers. Although expensive (at least 60,000 €), VR simulators allow more advanced training than VT without presenting the ethical issue of live animals and cadavers. Moreover, traditional training is not without its cost. Bridges and Diamond (5) estimated this cost to be approximately 40,775 € per graduating resident, based on the time “lost” by primary operator residents in the OR. In addition, the application of faculty costs leads to approximately 62,810 € to 172,682 € per resident (6). VR simulators are therefore an increasingly attractive option: once bought, they require little running cost, are easily available for use, and allow iterative skills training.
VR Simulators: Principles and Models
VR simulators consist of laparoscopic instruments that are connected to a desktop computer: trainees have to select the tip of the instrument they need, and then they are able to follow the instrument’s path on the computer screen as they move it, in real time. Furthermore, VR simulators have the ability to provide automatic and instantaneous measures of performance, also called metrics, such as time, number of movements, path length, or accuracy (7). These metrics can be used as an assessment tool: they can serve to monitor progress while learning a technical skill, aid in the provision of structured feedback, and ultimately ensure that proficiency criteria have been reached. Furthermore, it is possible to record the trainees’ performance in a database from which it can be recovered for analysis.
There is a wealth of simulators, ranging from low-fidelity trainers such as the Minimally Invasive Surgical Trainer in Virtual Reality (MIST-VR®; Mentice, Gothenburg, Sweden), which only comprises basic skills and has no haptic feedback, to high-fidelity simulators such as the LAP Mentor™ (Simbionix, Cleveland, OH, USA) that allows to practice on full procedures and has force feedback (Fig. 1). The MIST-VR comprises abstract basic tasks, enabling the acquisition of psychomotor skills rather than cognitive knowledge. The LapSim® (Surgical Science, Gothenburg, Sweden) has more realistic tasks than the MIST-VR, involving structures that are deformable and may bleed (Fig. 2), and comprises 3 levels of difficulty. It also has more advanced tasks such as laparoscopic suturing and running the small bowel, as well as full procedures such as laparoscopic cholecystectomy, appendectomy, and hysterectomy. It does not have haptic feedback. The Xitact LS500® (Xitact, Morges, Switzerland) comprises basic tasks in a virtual abdomen with force feedback. Finally, the LAP Mentor is the latest generation VR simulator, incorporating haptic feedback. It comprises basic tasks, suturing tasks, procedural modules, and full procedures that range from basic (cholecystectomy, hernia repair) to advanced laparoscopic surgery (gastric bypass, hysterectomy, and sigmoid colectomy). The VR images are based on magnetic resonance imaging (MRI) and in vivo laparoscopy for procedural modules and full procedures (3).
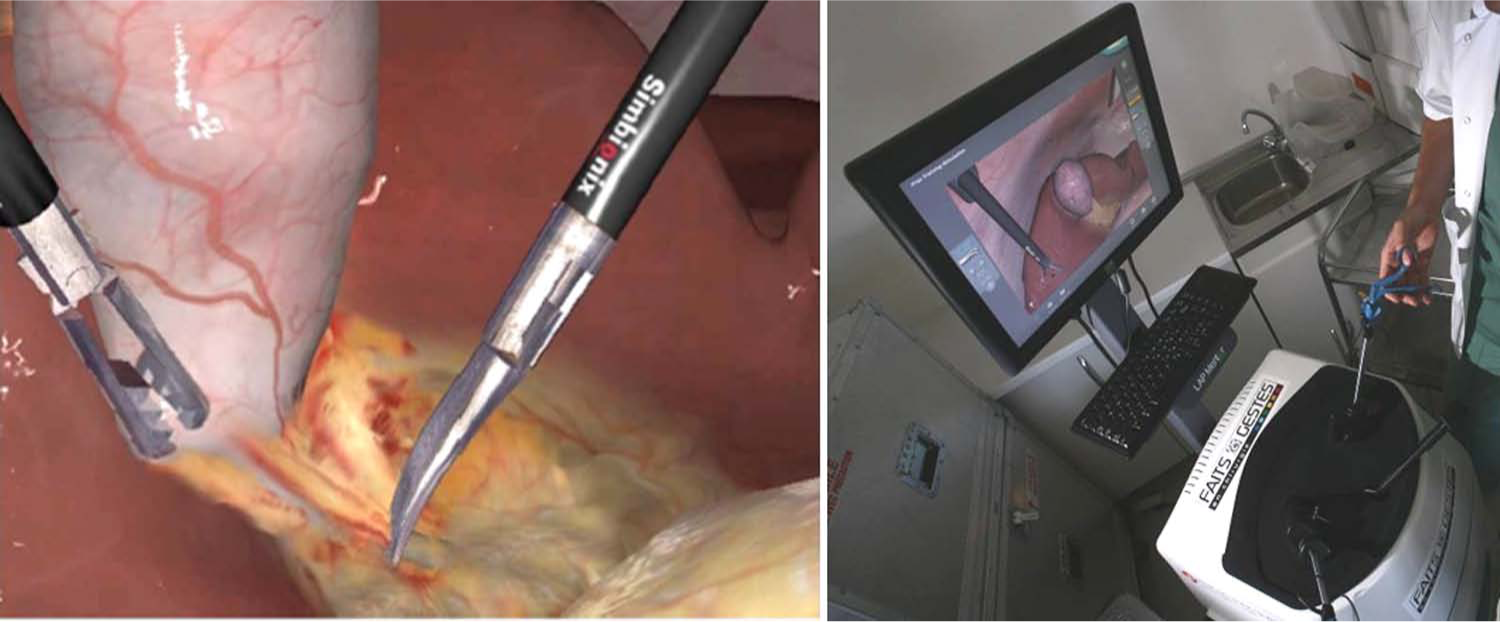
Virtual laparoscopic cholecystectomy on the LAP Mentor™.
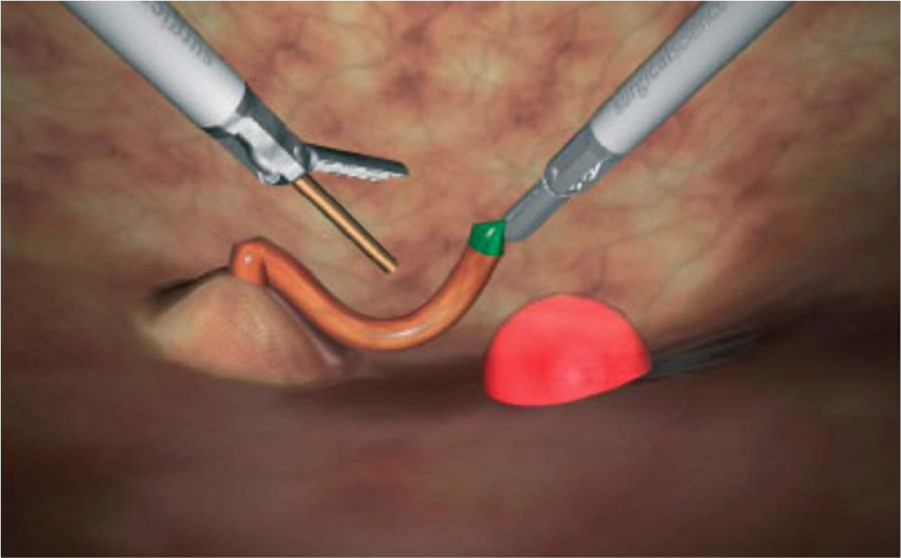
Basic laparoscopic task on the LapSim® (cutting exercise).
Validated Tools for Surgical Training and Assessment
VR simulators have shown acceptable fidelity, or face validity (i.e. the extent to which the tasks or procedures resemble real-life situations), content validity (i.e. if the domain that is being measured is actually measured by the tool: for example, while trying to assess technical skills we may actually be testing knowledge), and predictive and concurrent validity (i.e. respectively, the ability of the tool to predict future performance, and the extent to which the results of the assessment tool correlate with the gold standard for that domain) (8). Furthermore, a variety of VR simulators have demonstrated construct validity, that is, their metrics can discriminate between expert and novice performance. The MIST-VR has demonstrated construct validity (9), as well as the LapSim® for lifting and grasping task, clipping task, and cholecystectomy (10, 11). More sophisticated simulators such as the LAP Mentor or the Olympus ENDO-TS1 (Olympus Keymed, Southend, UK) colonoscopy simulator model have also demonstrated construct validity (12, 13). However, regarding the literature, not all metrics are construct-valid measures. The parameters that have the most evidence to support their use are time taken, number of movements, path length (i.e. the distance covered by the instrument’s tip), and, to a certain extent, error scores for particular tasks. These assessment parameters are consistent across various types of simulators. However, they are not necessarily meaningful for trainees and may not provide them with insight into the level of their own performance. Structured training programs and mentoring (including supervision and oral feedback) are therefore still paramount in the field of surgical education.
Learning Curves and Curricular Approach
Based on these construct-valid metrics, learning curves have been shown on a variety of VR simulators. In most studies, novices reached expert proficiency after approximately 10 trials, but learning curves presented with individual variations: trainees with similar baseline level may indeed take different amounts of time to reach expert level (14). Furthermore, Ahlberg et al. (15) showed that training without proficiency goals was not optimal. Indeed, they compared the STS of medical students trained on the MIST-VR to a control group during a laparoscopic appendectomy on a porcine model. The intervention group was trained only for a certain amount of time but with no proficiency goal. There was no difference between the two groups.
A major advance in basic technical skills training is therefore the implementation of structured competency-based curricula, using proficiency goals on construct-valid measures (Fig. 3) (10, 12). Proficiency measures are based on the performance of experienced surgeons. The aim is to acquire a basic level of proficiency prior to entering the OR and to reduce the learning curve on real patients: predefined benchmark criteria can ensure that skills acquisition is successful. Training sessions are short and iterative (a maximum of 3 sessions are allowed per day, performed at least 1 hour apart) in order to ensure a distributed rather than massed approach to skills training. Indeed, the distributed training has demonstrated higher impact on STS in VR (17). Such curricular approach has also been implemented in endoscopy (13) and may as well be used in the future for advanced laparoscopic surgery. Finally, retention of STS has been shown up to 7 months after training to proficiency on VR simulators (18).
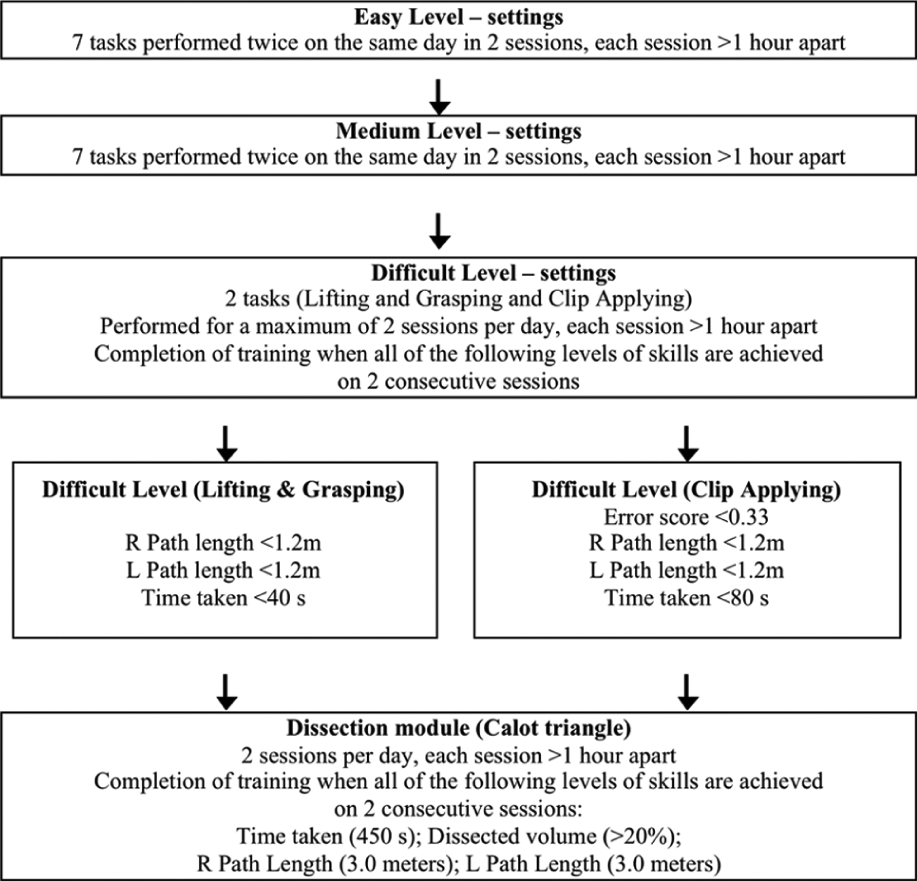
Example of an evidence-based virtual reality curriculum, designed on the LapSim by Aggarwal et al. (10).
Transfer of Technical Skills
There is a wealth of data on VR simulation, but many studies have major flaws: small sample sizes, multiple VR models, varying rating scales, and lack of objective tools to assess the transfer of STS (3, 19). There is therefore a great amount of data in the literature that has prompted Champion and Gallagher to state that “poor scientific reflection in medical simulation has become too common” (16). However, some studies have assessed the transfer of STS after training on VR simulators. Several randomized controlled trials have shown that training to expert levels of proficiency on VR simulators results in improved performance in a porcine model compared to conventional apprenticeship (20–22). Four randomized controlled trials assessed the impact of VR training during a real procedure in man (23–26). Grantcharov et al. (23) appraised the impact of MIST-VR simulator training in a multicenter study, comparing their intervention group to controls. Evaluation criteria were the time required to perform a laparoscopic cholecystectomy, an error score, and a score for economy of movements (analog scale). There was a significant difference between the two groups for all three criteria. Seymour et al. (24) also studied the impact of MIST-VR training versus controls on STS in the OR: a significantly positive effect was again demonstrated. However, there was no baseline evaluation in the OR, and the time between training and assessment was not stated. Similarly, Scott et al. (25) reported an improvement in STS after VR training. In gynecology, Larsen et al. (26) demonstrated that training on the LapSim® resulted in improved STS during a laparoscopic salpingectomy with respect to time and to a validated score. Moreover, both Xitact LS500® and LAP Mentor demonstrated a significantly positive impact on STS in the OR in nonrandomized comparative studies (27, 28). Finally, beyond training to acquire STS, VR simulators have also demonstrated a positive impact as a warm-up tool for surgeons before doing a laparoscopic cholecystectomy (29).
Are VR Simulators Better Than VT?
Training out of the OR has proven its positive impact on basic skills during real laparoscopic procedures in patients on both VT and VR. However, few studies have yet compared VT with VR. Considering the staggering difference in cost, it seems pertinent to determine whether the higher cost of VR simulators is associated with an increased efficiency or whether in contrast a VT, around 20 times less expensive, is just as valuable a learning tool.
Studies comparing VT and VR showed mixed results, and only two studies have compared the impact of VT against VR on STS in the OR (27, 30). One systematic review (31) concluded a superiority of VR simulators in terms of scores of performance established outside of the OR but also mentioned that “the advantages of VR over VT training are not evident.” Munz et al. (32) compared the performance of 3 groups out of the OR before and after training. The first group received training sessions on the LapSim® and the second on a VT; a third control group received only conventional apprenticeship. They concluded that there existed a significant progression of the two groups trained on the simulators compared to the control group and that there was no significant difference between the two simulators, with however a tendency in favor of the VT. However, the transfer of skills to the OR was not assessed in this study. In 2005, Youngblood et al. (33) compared the impact of the Tower Trainer® (Simulab Corporation Seattle, WA, USA), VT, and the LapSim® on STS in live pigs. They found a superiority of the LapSim®. However, this study had several limitations. First, no baseline testing was performed, which would have ensured that the two groups were comparable. Second, the assessment tool was not a validated score. Two studies have compared the impact of VR versus VT on STS in the OR. Hamilton et al. (30) compared the MIST-VR with a VT, the SCMIS GEM® (Karl Storz Endoscopy, Culver City, CA, USA). The performance of 19 residents in the OR during a laparoscopic cholecystectomy procedure was assessed before and after a training session. The assessment tool used was a validated global score. The authors demonstrated a significant progression outside of the OR in both groups, but a transfer of skills to the OR was only demonstrated in the VR group. One explanation is that training sessions were not supervised, and while feedback is given to trainees on VR simulators by the metrics, trainees had no feedback on VT apart from time taken (although a rapid hand movement may not necessarily be a correct one). However, a limitation to that study is that all trainees were not assessed by the same observer, and one candidate was not always assessed by the same observer before and after the training. The last study compared two groups training on simulators, the LAP Mentor or a VT, the Mac Gill Inanimate System for Training and Evaluation of Laparoscopic Skills (MISTELS), to a control group during a laparoscopic cholecystectomy in the OR. Both intervention groups demonstrated a significant improvement compared to the control group, but there were no differences between the VT and VR groups (27).
In total, there may not be a superiority of VR simulators over VT for teaching laparoscopic basic skills. However, VR systems present two advantages over VT. First, they provide automatic feedback at the completion of each task, allowing deliberate practice. This deliberate practice has recently demonstrated a positive impact on STS in the porcine model (34). However, such computer-generated feedback is useful but usually insufficient to improve the skills without supervision and verbal feedback. Second, VR provides more diversity than VT: indeed it comprises not only training for basic skills but also more advanced training, including multiple scenarios for one given procedure.
Beyond Training for Basic Laparoscopic Skills
Until now, training out of the OR involved mostly basic laparoscopic skills. However, VR simulators of the latest generation provide advanced procedures such as gastric bypass, sigmoid colectomy, hysterectomy, or carotid artery stenting, and forthcoming research in VR should focus on this field. Furthermore, patient-specific models have been designed in VR simulation to answer the “ceiling effect associated with the fixed nature of the anatomy model” described by Essani et al. (35). Patient-specific models have been designed on various medical fields such as vascular, craniofacial, rectal surgery, neurosurgery, or percutaneous interventions (36). Finally, VR simulators have also been developed and validated in the field of robotic surgery (37).
Conclusion
Training out of the OR on VR simulators has proven its positive impact on basic skills during real laparoscopic procedures in patients. It also offers an ethical way of assessing the competency of a surgeon in performing a procedure, without risk to a patient. The benefit of VR over VT remains unclear for teaching basic skills. However, VR simulators provide automatic feedback at the completion of each task, unlike VT. This feedback permitted to design structured competency-based curricula and allow deliberate practice. Finally, advanced procedures and patient-specific models have been designed on VR simulators, and further investigations are still awaited to appraise their educational value.