
Abstract
Background and Aims:
Surgery cancelations cause inappropriate use of hospital resources and additional financial and psychological stress to patients. Cancelation rates have been described to be even more than 10% of scheduled cases. Preoperative anesthesia evaluation clinics have been initialized to decrease cancelation rates. At Hyvinkää hospital, 95% of elective surgical patients are admitted on the morning of operation, and only 25% of these patients visit preoperative anesthesia evaluation clinic prior to surgery. Cancelation rate in Finnish hospitals has not been described.
Material and Methods:
We studied retrospectively 12,205 scheduled elective same-day admission surgical cases at Helsinki and Uusimaa Hospital District, Hyvinkää hospital for a period of 2 years. Obstetric cases, emergency cases, and a few inpatient cases were excluded. A case was considered as canceled if surgery was canceled after the finalization of operation room schedule for the next day. Cancelation rates among different specialties and reasons for cancelation were analyzed.
Results:
A total of 12,205 surgeries were scheduled during the study period, and 551 (4.5%) of these were canceled. The highest cancelation rate was in hand surgery, with 8.2% of scheduled cases, followed by orthopedic surgery with 5.4%, and pediatric surgery with 5.1% cancelation rate. Endocrinology had no cancelations, and breast, urology, and vein surgery also had less than 2% of canceled cases. Patient-related issues caused 72.4% of cancelations, and operation no longer being necessary caused 26% of all cancelations.
Conclusions:
Day of surgery cancelation rate was low in same-day admission, although it varied between specialties. Specialties having explicit surgery indications had fewer cancelations than specialties having surgery indications based on more subjective diagnostic. Process improvements need to be considered continuously to further decrease cancelation rate.
Keywords
Introduction
Cancelation of scheduled surgery is very expensive and inconvenient for both hospital and patient (1, 2). Traditionally, patients are admitted to hospital a day before the operation for preoperative assessment and preparation. Cancelation on the day of surgery among these patients may lead to prolonged hospital stay and additional costs (1). Day surgery and same-day admission have become more popular because they decrease hospitalization time and costs and increase both hospital productivity (3, 4) and patient satisfaction (5, 6). To sustain anesthesia safety and prevent excessive day-of-surgery cancelations, outpatient anesthesia preoperative evaluation clinics (APEC) have become more common while same-day admission has become more widely used (7, 8). They increase hospital productivity and reduce surgical cancelations and costs (2–4, 9, 10).
Cancelation rates and reasons for cancelation vary widely in published studies (2, 11–13). Cancelation rates for the total study populations range from 4.6% to 13.2%, and most common reasons range from lack of operation room (OR) time to patient no-show. Recent multicenter study in Germany described cancelation rate variation from 12.4% in university hospitals to 5.0% in community hospitals (14). Hospitals in published studies have different proportions of same-day admission in elective surgery, and a large proportion of patients is still admitted a day before surgery (2, 10). In addition, preoperative anesthesia evaluation usage varies from 33% to 100% of patients (14, 15).
In Finland, in the Hospital District of Helsinki and Uusimaa at Hyvinkää hospital, 95% of elective surgical patients are admitted on the day of surgery in a From Home to Operation (FHTO) process. In this process, patients are admitted to surgery through FHTO unit on the day of surgery regardless of the type of surgery and previous health status. Only one-fourth of patients have anesthesia evaluation at FHTO APEC 1–4 weeks prior to surgery. The process is cost-effective (16), and no differences in postoperative outcome after initialization of the process have been found (17). Nevertheless, cancelation rate in Finnish hospital has not been described.
The aim was to determine total cancelation rate and rate per different surgical specialty in same-day admission in a Finnish large-size community hospital. Furthermore, we wanted to identify cancelation reasons and detect possible weak points in our system.
Material and Methods
The study population consists of 12,205 patients scheduled for elective surgery in FHTO process at HUS Hyvinkää hospital. Patients were operated between July 2009 and June 2011. Hyvinkää hospital is a large-size community hospital providing secondary health care for a population of 180,000. The hospital provides emergency health care in surgical, internal, pediatric, and obstetric fields. Surgery specialties include orthopedic and traumatology, gastroenterology, plastic, endocrinology, pediatric, and vein surgery, as well as gynecology and otorhinolaryngology (ORL). Arterial, cardiac, neurosurgery, or ophthalmology patients are treated in university hospital in the same hospital district.
Since 2006, 95% of elective patients have been admitted to surgery through FHTO unit regardless of patients’ previous health, extent of surgery, or need for postoperative care. Only 5% of the patients are admitted to ward prior to surgery, and these include for example patients in need of blood transfusion prior to surgery. Patients are referred to an APEC according to predefined criteria, and only patients with high surgical risk visit APEC. This includes 25% of all elective patients.
In FHTO process, a surgeon confirms surgery indications at surgery polyclinic. A specialized nurse examines patient records, allocates patients to APEC, and maintains and organizes surgical waiting list. Patients receive general information about preoperative preparations and specific information about surgery, in both spoken and written formats. This includes information regarding what do to if patients’ health status changes. Patients receive their invitations to operation approximately 3 weeks prior to surgery, and a nurse contacts all patients arriving to surgery a day before operation to verify the admission and operation time. On the morning of operation, patients arrive to FHTO unit, which is located next to the ORs. Patients meet a nurse and the operating surgeon, who may be different from the surgeon who they met during polyclinic visit. Patients walk to the OR when the OR is ready. After the operation, patients are either discharged or admitted for postoperative care to intensive care unit or surgical ward.
All elective surgical patients scheduled for operation in FHTO process were included in this study. The study population included both day-only surgical patients and patients requiring postoperative hospitalization. Patients admitted to hospital as inpatients a day before surgery and for emergency operations were excluded. In addition, elective cesarean sections and procedures performed outside OR (i.e. endoscopy, radiology) were excluded.
A case is considered as canceled after the OR schedule has been verified at 1 p.m. the day before and the surgery has not been performed on the intended day. Surgery can be canceled by patient, operating surgeon, or anesthesiologist. Cancelation and categorized reason for cancelation are always recorded in real time into OR management software Opera (Opera 4.0 SP4, GE Healthcare). Data were collected retrospectively from the software. Main outcomes were total cancelation rate, rates per specialty, and reasons for cancelation.
Statistical analyses were made by SPSS (IBM SPSS Statistics, Version 19, IBM Corp.) statistical software. Categorical data were analyzed using the Pearson’s chi-square test, and the whole data were analyzed before subgroup analyses. The p-values less than 0.05 were considered statistically significant. Results are presented as means ± standard deviations, as medians (ranges), or as frequencies.
Results
From 1 July 2009 to 30 June 2011, a total of 12,205 patients were scheduled for surgery, and 551 (4.5%) cases were canceled. The most common surgical specialty was orthopedic (31.8%), followed by gastroenterology (15.2%), ORL (13.6%), and gynecology (11.1%) (Table 1).
Cancelation by specialty (frequencies, percentages).
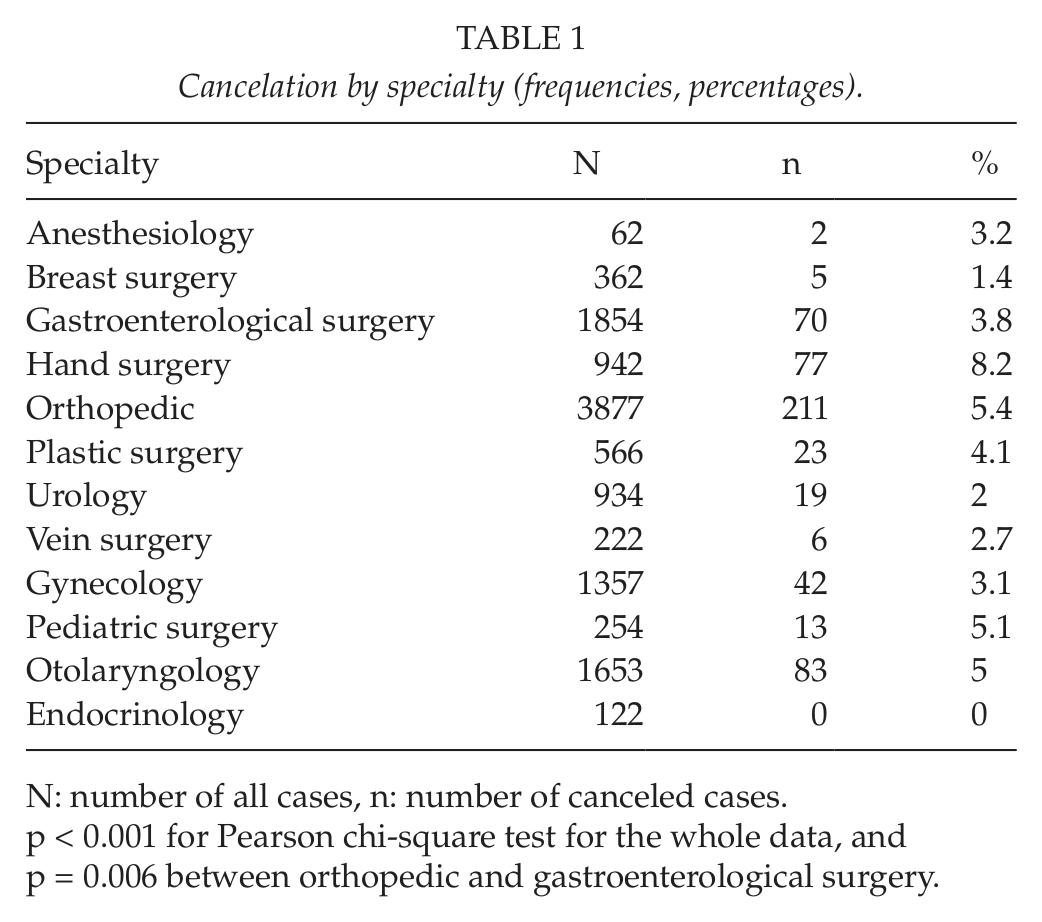
N: number of all cases, n: number of canceled cases.
p < 0.001 for Pearson chi-square test for the whole data, and p = 0.006 between orthopedic and gastroenterological surgery.
The type of surgical specialty had significant effect on the frequency of cancelations (p < 0.001) (Table 1). Cancelations were most common in hand surgery (8.2% of all hand surgery patients), followed by orthopedic (5.4%), pediatric (5.1%), and ORL surgery (5.0%). On the contrary, of 122 scheduled operations for endocrinological surgery, none were canceled. Between the two most common types of surgery, orthopedic surgery had more cancelations (5.4%) than gastroenterological surgery (3.8%), (p = 0.006).
Reasons for cancelation were divided into three categories: patient-, hospital-, and staff-related issues. Most of the cancelations were due to patient-related issues (399 cases, 72.4% of all cancelations). Hospital-related issues were the reason in 109 cases (19.8%) and staff-related issues in 43 cases (7.8%) (Table 2).
Detailed cancelation reasons, n = 551 (frequencies, percentages).
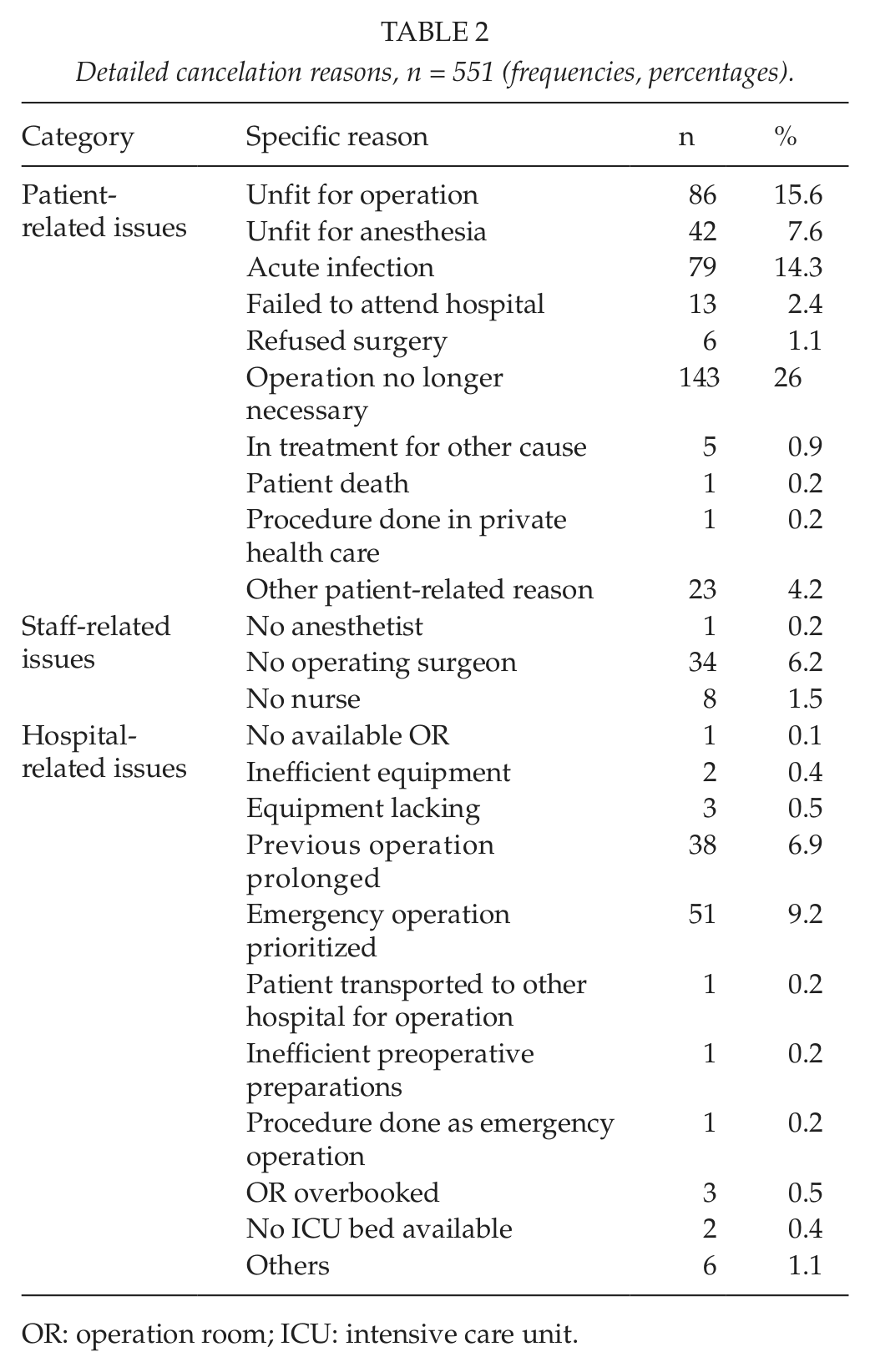
OR: operation room; ICU: intensive care unit.
Three most common reasons for cancelation covered 60.3% of all cancelations (308/511 cases). The most common reason was operation no longer being necessary (143 cases, 26% of all cancelations, 1.2% of all patients). The second most common reason was patient being unfit for operation (86 cases, 15.6% of all cancelations, 0.7% of all patients). The third most common reason was acute infection (79 cases, 14.3% of all cancelations, 0.6% of all patients). After acute infection, the other reasons were emergency operation prioritized (9.2%, 51 cases), patient unfit for anesthesia (7.6%, 42 cases), prolonged previous operation (6.9%, 38 cases), and lack of surgeon (6.2%, 34 cases) (Table 2).
Surgery specialties had different cancelation reason proportions (Fig. 1). Largest proportion was patient-related issues in most specialties. Pediatric surgery and anesthesiology had 100% and orthopedic, gynecology, hand, and plastic surgery had over 70% of cancelations due to patient-related reasons. Urology, on the contrary, had only 47% of patient-related reasons. Gastroenterology, breast, and vein surgery had less than 70% but over 50% of patient-related reasons. Second largest reason was hospital-related in other specialties; however, in vein and ORL surgery, staff-related reasons were more common than hospital-related reasons.
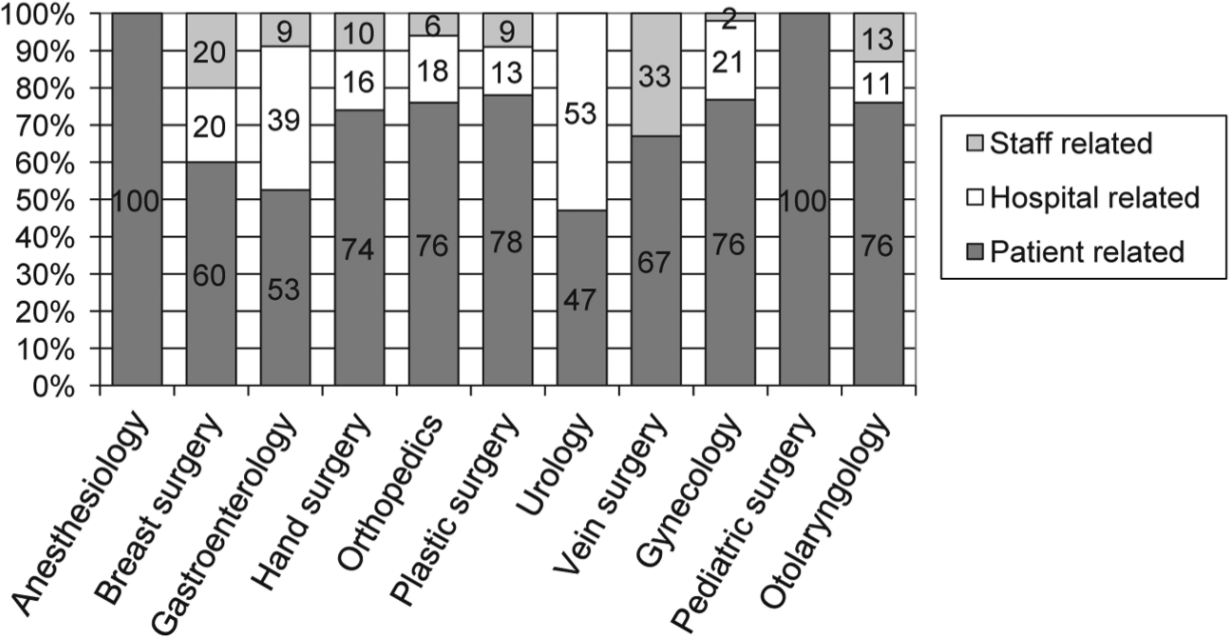
Cancelation reason proportions by specialty.
Discussion
This study investigated surgery cancelations in same-day admission in a Finnish large-size community hospital. Total cancelation rate was 4.5%. Yet, it varied between surgery specialties from 0% in endocrinology to 8.2% in hand surgery. Three most common reasons were all patient-related, and the most common reason was operation no longer being necessary, which accounted for 26% of cancelations.
The FHTO process and the OR management software Opera were introduced at the same time in 2006. Before Opera, cancelation rates were not recorded. Therefore, estimating the effect of FHTO on cancelation rates is limited. Nevertheless, cancelation rate of 4.5% in FHTO process with 95% of same-day admission is low. Only 25% of FHTO patients are evaluated at preoperative anesthesia clinic prior to surgery. Whereas in Germany all patients are evaluated by anesthesiologist prior to surgery, yet cancelation rate is more than 8% in large community hospitals (14). In other studies, cancelation rates were 6.6% (18) and 13.5% (19), both after initialization of a preoperative evaluation clinic.
Hand, orthopedic, pediatric, and ORL surgeries had the highest cancelation rates, and the most common reason was patient-related issues in all of them. On the contrary, endocrinology had no cancelations, and breast, urology, and vein surgery had each less than 3% of canceled cases. Urology was the only specialty in which patient-related issues were not the most common reason. Endocrinological operations were mainly thyroidal operations, which have explicit surgery indications. Whereas indications for hand and orthopedic surgeries may be debatable and result in higher cancelation rate. Hand surgery was separated from orthopedic because it has been noted to have highest cancelation rate monthly and special reasons for cancelation. For example, cat scratches caused cancelations before patients were given a written instruction to avoid them.
Overall, patient-related issues covered over 70% of cancelations, and operation no longer being necessary was the most common single reason. In Finland, waiting time for surgery has traditionally been quite long, and it has been aimed to be less than 6 months. However, the goal is still not fully achieved. Longer waiting time may lead to recovery by conservative treatment or worsening of health status, whereby surgery is considered either unnecessary or too risky. Hand and orthopedic surgery often have longer waiting time, which may be another explanation for high cancelation rate. Endoprosthesis patients meet operating surgeon 2 weeks prior to surgery, and other patients do not meet a surgeon between making the surgery decision and the morning of surgery. Currently, it is not possible to increase extra policlinic visits to all patients. Alternatives to these visits need to be considered. A nurse verifies the operation and admission time via phone on the day before operation, which may reduce cancelations due to patient no-show (11, 20). However, health status changes should be acknowledged earlier to allow hospital time to organize other surgery instead. Patient information on this issue needs to be emphasized.
Patient unfit for operation and acute infection were the next common reasons for cancelation. Patient unfit for anesthesia caused only 7.6% of cancelations. Chronic diseases should be balanced before operation and should not cause cancelations. A trained nurse screens patients to identify those with high surgical risk, and one-fourth of elective surgical patients visit APEC. These clinics have shown to decrease cancelation rate and operation delays (2, 19). Fischer described cancelation rate of 0.21% due to medical reasons (i.e. hypertension) after implementation of APEC (4). However, patient unfit for anesthesia and unfit for surgery caused 23% of cancelations altogether. Criteria for APEC visit and benefit of increasing these visits need to be examined.
The most common hospital-related reasons for cancelation were prioritized emergency operation and prolonged previous operation. A traumatology OR was recently initialized, which may reduce cancelations due to prioritized emergency operations. Prolonged previous operations should be minimized if possible. Schofield et al. (21) described that if surgeons estimates the time needed for operation themselves, it may lead to underestimation and further delay or cancelation of the following operation. This has been resolved by the software Opera, which estimates time needed for the operation according to duration means of the surgeon’s previous similar surgeries. A block time system that prevents cancelation due to overrun OR time has been described (22), but currently, it is not considered to be implemented in Finland. Missing surgeon was the reason in 6.2% of canceled cases. At Hyvinkää hospital, only few specialists perform certain type of operation, that is, certain hand or vein surgeries, and the specialist cannot be replaced if needed.
We have a large and miscellaneous patient population that demonstrates a Finnish hospital material. Further studies to investigate surgery cancelation in certain patient populations and in other hospitals are essential. Weaknesses of our study include also its retrospective nature. However, the cases were identified and the categorized reasons were registered in real time. Interpretation of categorization instructions may vary between individuals, which is a limitation of our study, even if estimated as being minimal. Cancelation rate is monitored monthly, and improvements to lower the rate are considered continuously. We had a long study period to minimize possible short-time variation of the cancelation rate.
In conclusion, low cancelation rate of 4.5% in same-day admission was recorded. Still, majority of cancelations were due to patient-related issues, particularly, unnecessary operation was highlighted. Patient information and surgery indications need to be emphasized in the future.