
Abstract
Background and Aims:
Aging with comorbidities, obesity, and rapid recovery from operation may increase the need for laparoscopic cholecystectomy, but long-term use of statins may be associated with a decreased risk of gallstones. This population-based cohort study presents the changing rate and causative factors of laparoscopic cholecystectomy in Finland during the era of statin use.
Materials and Methods:
Age structure of the population, changes in body mass index and diabetes, and the number of all cholecystectomies in 1995–2009 were retrieved from the registers of National Institute for Health and Welfare. Additionally, these results were supplemented by a population-based retrospective cohort (1581 laparoscopic cholecystectomy) in one community-based hospital area. The risk factors for laparoscopic cholecystectomy, use of statins, and surgical outcome were analyzed.
Results:
During the 15 years, 123,794 cholecystectomies were performed in Finland, of which 94,740 (76.5%) were performed using laparoscopic technique. The median rate of laparoscopic cholecystectomy varied between 110 and 140 operations per 100,000 inhabitants. In 1995–2009, the annual number of cholecystectomies decreased from 8600 to 7500, the number of laparoscopic cholecystectomies increased by 10%, and the number of open cholecystectomies declined by 60%. In a cohort of 1581 laparoscopic cholecystectomies, the proportion of elderly (>65 years of age), obese (body mass index > 30 kg/m2), and diabetic patients increased from 17% to 28%, 9% to 34%, and 4% to 8%, respectively. Use of statins increased more than fourfold during the 15 years.
Conclusions:
The rates of all cholecystectomies decreased despite marked increase in laparoscopic cholecystectomies performed. The increase in risk factors for gallstones in Finland implied more marked increase in laparoscopic cholecystectomies. The possible role of statins on gallstone disease is discussed.
Introduction
Since its introduction in 1980s, laparoscopic cholecystectomy (LC) has become the golden standard for the treatment of symptomatic gallstones. LC has also been shown to be safe and efficient in the treatment of acute cholecystitis (1, 2). Compared to the traditional open cholecystectomy (OC), LC is associated with less postoperative pain, shorter hospital stay, earlier return to normal activities, and improved cosmetic results (2). Thus, the threshold for surgery may be lowered, which may contribute to the increased rate of cholecystectomies and especially LCs (3). Around 70%–80% of all cholecystectomies in the Western world are now performed using laparoscopic technique (4–6).
A worldwide increase in aging of general population, metabolic syndrome, obesity, and diabetes mellitus is likely to cause an elevated risk of symptomatic biliary stone disease and subsequent requirement for the LC (7–9). As in other Western countries, obesity and closely associated type 2 diabetes are rapidly increasing in Finland (10, 11). About 25% of diabetic patients have gallstone disease, and every fifth of the patients come into cholecystectomy (12). Long-term use of statins may be associated with decreased rate of cholelithiasis (13). The cardiac, pulmonary, and metabolic comorbidities commonly observed in morbidly obese patients may affect the outcome of gallbladder surgery. No studies have assessed the impact of aging, obesity, and related comorbidities on the rate of overall cholecystectomies and LCs in a population-based level during the era of statin use. In Finland, the use of statins and other lipid-lowering drugs has increased 11-fold between 1995 and 2005 (14).Therefore, we analyzed the effect of obesity and aging on the rate of cholecystectomies nationwide and in one well-defined community-based hospital district between the years 1995 and 2009.
Materials and Methods
A population-based register study was performed to assess the rate of both OC and LC in Finland between the years 1995 and 2009. The numbers of discharge diagnoses and surgical procedures were obtained from the National Institute for Health and Welfare (NIHW) registry (15). Age and weight changes of population, the number of diabetic patients, and use of statins were also recorded from earlier studies and from the official statistics of Finland (14–16). Diabetic patients included all those who received drug reimbursement for any glucose-lowering drugs, and the vast majority of them had type 2 diabetes. Drug reimbursement register has nearly 100% coverage, but the undiagnosed and diet-only treated are not included in this register. Nationwide population data from 1995 to 2009 were retrieved from the Official Statistics of Finland (15). Reimbursed prescriptions for lipid-lowering drugs between 1995 and 2009 in Finland were retrieved from the nationwide Prescription Register (14).
To analyze in more detail, the causative risk factors for LC, a cohort retrospective study including 1581 LCs in one well-defined community-based hospital district serving 110,000 inhabitants was performed. Data of all cholecystectomies between January 1995 (first LC in the study hospital) and December 2008 were collected into the surgical audit database. During the same period, 984 OCs were also performed in the study hospital (17). Results of statin use and other medication, the American Society of Anesthesiologists (ASA) classification, and body mass index (BMI, kg/m2) of the patients were recorded. Audit of perioperative data (elective vs emergency operation, complications, and conversion rate) was also recorded. Elective operation means that the operation time was scheduled beforehand. Emergency operations were mainly performed because of acute cholecystitis. Patients’ comorbidities were recorded as none, diabetes, coronary heart disease, hypertension, pulmonary or renal diseases, as well as those with multiple comorbidities (more than two) (18). The effect of obesity (BMI > 30 kg/m2) on the rate of LC was evaluated. The laparoscopic surgery was performed using a standard four-port technique as described earlier (17). Amsterdam classification of the severity of bile duct injuries was used (19). Amsterdam criteria type A indicates leakage from cystic duct or peripheral radicals, type B indicates major bile duct injury with leakage, type C indicates a bile duct stricture without leakage, and type D indicates complete transection or excision of common bile duct. Type A and type C lesions were considered mild, and type B and type D lesions severe.
Data were analyzed using SPSS Statistics 17.0 (SPSS, USA, 2008). Statistical analysis was performed using Student’s t-test or χ2 test. P-values less than 0.05 were considered significant. The study protocol was approved by the local ethical committee.
Results
Nationwide Analysis
A total of 123,794 cholecystectomies were performed in Finland between 1995 and 2009, of which 94,740 (76.5%) were performed using laparoscopic technique. The annual rate of all cholecystectomies decreased from 8600 to 7500 (13%) during the study period.
In 1995–2009, the number of LCs increased by 10% and the number of OCs declined by 60% (Fig. 1). The median rate of LC varied between 110 and 140 operations per 100,000 inhabitants. During the study period, the elderly population (>65 years of age) increased from 732,417 to 910,441 (24%) according to the figures of the official statistics of Finland. The number of elderly patients operated by using LC technique increased from 1248 procedures to 1473 (18%) in Finland. Between 1995 and 2009, the nationwide mean BMI increased from 26.7 to 27.2 kg/m2 (16). The proportion of obese inhabitants (BMI > 30 kg/m2) increased from 10.6% to 16% between 1995 and 2008. The number of diabetic drug-treated patients increased from 134,400 to 190,000 (41%).

Incidence of cholecystectomies in Finland in 1995–2009.
A nationwide register study in Finland revealed that the 1-year prevalence of statin use increased 11-fold (95% confidence interval = 11.2, 11.5), that is, from 7.8 per 1000 inhabitants in 1995 to 88.9 per 1000 in 2005 (14).The overall incidence of statin use increased from 355 per 100,000 inhabitants in 1995 to 1772 per 100,000 in 2005. Among females, the incidence increased from 312 per 100,000 female inhabitants to 1732 per 100,000, and among males, it increased from 399 per 100,000 male inhabitants to 1815 per 100,000 (14).
Community Cohort Analyses
A total of 1581 LCs (including 119 conversions) were performed between 1995 and 2008 in the study hospital. Fig. 2 presents the total number of LCs and LCs performed in elderly (>65 years of age), obese (BMI > 30 kg/m2), and diabetic patients in the study hospital. The rates of LC increased initially over twofold from 48 per 100,000 inhabitants to 102 per 100,000, but during the later years of the follow-up, this initial increase leveled off. The proportion of obese, elderly, and diabetic patients in all LCs almost doubled during the study period (Fig. 2).

Number of all laparoscopic cholecystectomies (LCs) and LCs performed in patients aged >65 years, obese (BMI > 30 kg/m2) patients, and diabetic patients in the study hospital between 1995 and 2008.
Demographic data and operative outcome of the LC patients are described in Table 1. Most of the operated patients were females with nonemergency LC. Conversion rate was 7.5%. The overall morbidity rate was 12%. Most complications were minor, such as superficial wound infections, minor bleeding, urinary retention, or port hernias. The overall incidence of mild bile duct injuries was 0.7% (n = 11), but no severe transection of common bile duct was observed. There were 10 Amsterdam criteria type A and one type B bile duct injuries: 8 cystic duct leaks, 2 leaks from duct of Luschka and 1 major bile duct injury with leakage. The bile duct injuries were treated either by endoscopic retrograde cholangiopancreatography (ERCP) stents or operatively by using t-tube and drainage. Two LC patients died because of cardiac complications.
Demographic and operative data of 1581 patients who underwent laparoscopic cholecystectomy in 1995–2008 in the study hospital.

SD: standard deviation; ASA: American Society of Anesthesiologists; BMI: body mass index.
The results of conversions to OC are presented in Table 2. Conversions were performed significantly more often on males than females (11% vs 6.2%) and on elderly patients, obese patients, and patients having an emergency operation or diabetes. Conversions were associated with higher postoperative morbidity. The risk factors for symptomatic gallstones and subsequent LC were also analyzed in the study hospital (Table 3). Although the number of LCs doubled during the study period, the rate of elderly patients undergoing LC was not significantly increased. More patients with obesity, males, and patients with higher classification of ASA were operated by LC during 2008 than in 1995 (Table 3). The number of patients using statins or other lipid-lowering drugs increased markedly (from 4.2% to 17%) during the study period. The effect of learning curve in terms of conversions or postoperative complications of LC was not statistically significant in 1995–1996 and 2007–2008 (data not shown).
Comparison of laparoscopically completed cholecystectomies and conversions to open surgery in the study hospital.
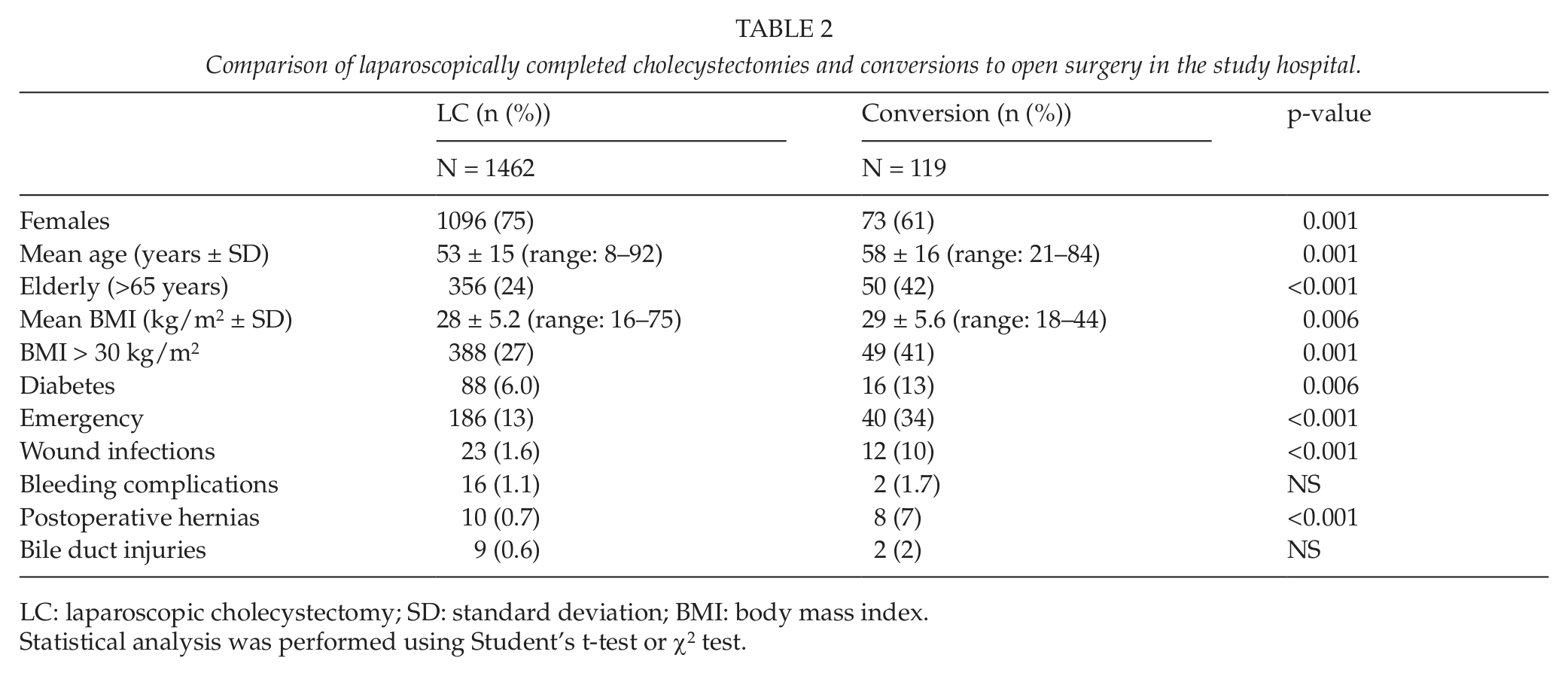
LC: laparoscopic cholecystectomy; SD: standard deviation; BMI: body mass index.
Statistical analysis was performed using Student’s t-test or χ2 test.
Changing incidence of risk factors for laparoscopic cholecystectomy in 1995 and 2008 in the study hospital.

LC: laparoscopic cholecystectomy; BMI: body mass index; ASA: American Society of Anesthesiologists.
Statistical analysis was performed using Student’s t-test or χ2 test.
Includes diabetes, hypertension, cardiac disease, pulmonary disease, renal disease, and liver disease.
Discussion
The main result of our population-based analysis was that the incidence of LC increased in Finland and the rate of OC decreased dramatically during the last 15 years. However, the number of all cholecystectomies declined. One reason for increased LC rate may be a reduction in the threshold for surgery in the laparoscopic era (3). The other reason may be an increased incidence of mild symptomatic gallstones leading to LC. The increasing trend of LCs would also be the expected finding for the diffusion of technology over time as experience has grown and the safety and efficacy have become proven. To our knowledge, the operative treatment protocol or indications to surgery have not been changed much during the last 15 years in Finland, although the increased use of ERCP particularly in elderly patients may explain part of the reduction of cholecystectomies.
Total amount of cholecystectomies declined by about 10% in the whole country. There are very few recent analyses of the incidences of LC and OC at the population level. Between 1988 and 1993 in North Carolina, the percentage of OC dropped from 100 to 32, and LCs progressed from nonexistent to the dominant approach for managing patients with cholelithiasis (6). Contrary to our country, the overall rate of cholecystectomy in North Carolina remained stable. There are, however, reasonable large variations between hospitals, regions, and even countries in the type of cholecystectomy used (20–22).
In our cohort study, the proportion of elderly, obese, and diabetic patients undergoing LC seemed to be increasing during study period. Gallstones are common with prevalence as high as 10%–15% in adults of developed countries. The known risk factors for gallstones are female gender, increasing age, obesity, the metabolic syndrome, rapid weight loss, and gallbladder stasis (9, 23). During follow-up, about 80% of gallstones remain asymptomatic, 10% develop mild symptoms, and 10% develop severe symptoms leading to cholecystectomy (24). The etiology of symptomatic gallstones is associated with obesity and alcohol use, possibly in part through their effects on serum lipids (23, 25). In Finland as in other Western societies, obesity, alcohol use, and comorbidities are increasing, which may also affect LC rate. Although other causative risk factors for gallstones are increasing, one explanation to the lack of increase in overall cholecystectomies may be the markedly increased use of statins. The use of statins and other lipid-lowering drugs has increased tremendously in Finland in recent years (14). This has occurred particularly among the elderly patients with hypercholesteremia.
Long-term use of statins may be associated with a decreased risk of gallstones (13, 26). The advent of LC has moved the interest away from the pharmacological treatment of gallstones. In the Western world, 80%–90% of gallstones originate from cholesterol-supersaturated bile, with the remainder formed as pigment stones, primarily from bilirubin and calcium (27). Statins inhibit hepatic cholesterol biosynthesis, and therefore may reduce the risk of gallstone disease some 30% (28). Recent studies have raised the possibility that cholesterol-lowering agents that inhibit hepatic cholesterol synthesis (statins) or intestinal cholesterol absorption (ezetimibe), or drugs acting on specific nuclear receptors involved in cholesterol and bile acid homeostasis may offer, alone or in combination, additional medical therapeutic tools for treating cholesterol gallstones (27). Evidence of the association between statins and gallstone disease is conflicting, and further case-control studies are needed to find out the causal role of statins in symptomatic gallstones and number of cholecystectomies.
In the US population, persons with gallstone disease have increased mortality overall and mortalities from cardiovascular diseases and cancer (29). Although LC is a relatively safe procedure, patients who die as a result of gallstone disease tend to be elderly patients, to have been admitted as emergency cases, and to have had multiple comorbidities (30). Deaths following cholecystectomy usually followed emergency admission (76%) and were more likely to have been associated with postoperative medical complications than surgical complications (30). Our results from the study hospital indicated that fatal outcome of LC was rare, and also postoperative complications remained at acceptable level. In Finland, a large number of LCs is performed by general surgeons without special expertise in hepatobiliary surgery. Iatrogenic bile duct injury is one of the most frightening complications associated with biliary surgery. Another main result of this study was very low percentage of severe bile duct injuries associated with LC. Over 1500 LCs were performed in the study cohort with only one severe type B injury of common bile duct. The quality of LC is currently quite high in many Scandinavian countries, with a low conversion rate and a high frequency of short admission without readmission (22). Our results confirmed those from earlier studies that acute cholecystitis, diabetes, male gender, aging, and obesity were all important risk factors for conversion and poorer outcome of LC (31, 32).
In conclusion, our population-based study found that the number of LCs is increasing in Finland, but total rate of cholecystectomies remained stable or decreased slightly, although the number of patients with increased risk for symptomatic gallstones is increasing. LC is a safe procedure to remove the gallbladder with minimal serious complications. The impact of enormous increase in statin use on the frequency of symptomatic gallstones warrants further studies.
Footnotes
Acknowledgements
We would like to thank nurses Jaana Väisänen, Marjo Hämäläinen and Riitta Varjo and Dr Anu Koski for their help in collecting the data.