
Abstract
Background and Aims:
Loss of femoral bone stock in elective revision total hip arthroplasty poses unique and substantial challenges. Structural onlay allografts may provide mechanical stability for the cementless revision prosthesis and increase bone stock.
Material and methods:
At least one cortical onlay allograft was used in 40 elective total hip arthroplasty revisions (40 patients) to reconstruct femoral bone defects. The operations were performed between January 1999 and August 2010 in the Turku University Hospital, Finland. The mean follow-up time was 52 months (range: 12–125 months).
Results:
The allografts were incorporated into the bone tissue in 37 of 40 (92.5%) patients. Cementless revision stems healed in 36 of 40 (90.0%) patients, but these patients were not exactly the same patients whose allografts were successfully incorporated. One or more surgical complications were experienced by 14 of 40 (35.0%) patients during follow-up. In all, 4 of 40 (10.0%) patients (all women) had hip infections during follow-up. Of the 7 patients with rheumatoid arthritis, 4 (57.1%) had at least one complication.
Conclusions:
The use of the cortical onlay allografts provides a feasible option for restoring the integrity of the proximal femur in revision total hip arthroplasty, but the complication rate is high, particularly in female patients with rheumatoid arthritis.
Keywords
Introduction
As a consequence of the growing number of old people in Finland, the incidence of primary total hip arthroplasties (THAs) (1) and of revision THAs is increasing. Bone deficiency around the femoral implant after revision THA is not rare and poses a risk for loosening of the prosthesis over time. Femoral bone stock deficiency is usually caused by osteolysis, which follows wear of implants, stress shielding from an excessively stiff implant, loosening of the implant, or infection. Iatrogenic causes of femoral bone stock deficiency include perforation during removal of bone cement during elective THA revisions. There may also be perioperative periprosthetic fractures.
Various techniques for dealing with bone loss are available, including impaction grafting (2, 3), structural cortical onlay allografting (4–6), proximal femoral allograft-prosthesis construction (7), modular metal augmentation, and application of reconstruction prostheses.
Femoral bone deficiency may be reconstructed in connection with revision THAs with the use of cortical onlay strut allografts, and the results have been satisfactory (8–11). Strut grafts become revascularized and incorporated into the surrounding bone tissue if the fit is stable (12). This is, however, a slow process and may not reach complete incorporation in adults (12).
In our clinic, we have, during recent decades, gained extensive experience of onlay allograft struts for the reconstruction of bone stock in association with cementless femoral revisions. The indications for strut allografts are segmental defects of the femoral diaphysis, ectatic femurs, iatrogenic perforations in connection with bone cement removal, perioperative periprosthetic fractures, and strengthening of extended femoral osteotomies. We have previously published a study on onlay allografts for treating periprosthetic fractures (13), and in this report, we analyze retrospectively our results of using onlay allografts for replacing femoral bone deficiencies in revision THAs.
Patients, Materials and Methods
A tissue database has been developed by BCB Medical (Turku, Finland) for managing bone banks. The database also provides a variety of statistical tools for the generation of reports on the information stored in the database. Our institution has used the program for 8 years, and data from 1990 are available. The Turku University Hospital is a central hospital with a population base of 460,000 people covering the southwest part of Finland.
Register data were compared to patient notes. At least one cortical onlay allograft was used in 40 elective THA revisions (40 patients) between January 1999 and August 2010 to reconstruct femoral bone defects at our institution. The initial diagnosis (cause for the primary THA) was recorded. The exact date for the primary THA was not always known. The mean follow-up time after the revision operation was 52 months (range: 12–125 months). If the revised hip was reoperated, the status of the stem and the strut graft were recorded. The follow-up time of the strut graft was considered to have ended when, in a reoperation, the graft was loose. The follow-up time of the stem was considered to have ended if, in a reoperation, the stem was removed or replaced. Otherwise, the follow-up of a patient was considered to have ended at the time of the last orthopedic note in the medical records. None of the patients died during follow-up.
Surgical complications were classified as infection, fracture, dislocation, nonunion of the graft, and nonunion of the stem. Nonunion of the graft and/or of the stem was verified either at reoperation or by radiography.
The tibial or femoral allografts were freeze-dried and prepared by the University of Turku Tissue Bank. Before use, the grafts were excised and prepared under strict aseptic conditions. The allografts were not subjected to treatment with alcohol or other chemical agents, nor were they subjected to irradiation.
Bone loss was classified radiologically as described by Della Valle and Paprosky (14). In Type I bone loss, there is minimal loss of metaphyseal cancellous bone with an intact diaphysis. In Type II bone loss, there is extensive loss of metaphyseal bone with an intact diaphysis. In Type IIIA, the metaphysis is damaged severely and provides no support, but there is a minimum of 4 cm of intact cortical bone in the femoral isthmus. In Type IIIB, the metaphysis is damaged severely with some intact cortical bone present distal to the isthmus (<4 cm). In Type IV, there is extensive metadiaphyseal damage and a widened femoral canal. The assessment of the available radiographs was performed systematically by two members of the research team (H.K. and K.M.).
A cementless long revision stem was used in all cases. There were 31 of 40 (77.5%) extendedly porous-coated revision stems (14 Integral, 14 Reach, 2 Biomet 300 revision stem, 1 Mallory-Head™ stem, all manufactured by Biomet, Warsaw, IN, USA) and 9 of 40 (22.5%) fluted distal fixation stems (8 Link MP, Waldemar Link GmbH, Hamburg, Germany and 1 Zimmer revision stem, Zimmer, Warsaw, IN, USA).
Statistical Methods
Continuous variables were characterized by means and ranges and categorical variables by frequencies and percentages. Differences between treatment groups for the normally distributed continuous variable age were tested by the t-test for independent samples and for the nonnormally distributed variable follow-up time by the Mann–Whitney U test. Categorical variables were analyzed with the χ2 test or Fisher’s exact test.
Results
The mean age of the patients was 76 years (range: 47–93 years). The proportion of women was 33 of 40 (82.5%). The reason for the revision was aseptic loosening in 33 of 40 (82.5% of all revisions), dislocation in 2 of 40 (5.0%), pseudoarthrosis in 3 of 40 (7.5%), and infection in 2 of 40 (5.0%) patients. A strut allograft was needed to treat a perioperative perforation, which occurred when bone cement was removed in 7 of 40 (17.5%) cases, to treat a perioperative periprosthetic fracture in 14 of 40 (35.0%) cases, to treat bone deficiency in 11 of 40 (27.5%) cases, and to strengthen an extended trochanter osteotomy in 8 of 40 (20.0%) cases. The initial diagnoses were osteoarthritis (OA) in 27 of 40 (67.5%) cases, rheumatoid arthritis (RA) in 7 of 40 (17.5%) cases, fracture in 3 of 40 (7.5%) cases, avascular necrosis in 2 of 40 (5.0%) cases, and Legg–Perthes–Calve’s disease in 1 of 40 (2.5%) cases. A cemented stem had been used in 31 of 40 cases (77.5%) and a cementless stem in 9 of 40 cases (22.5%).
The index revision was the first revision of the hip in 24 of 40 (60.0%) cases, the second revision in 10 of 40 (25.0%) cases, the third revision in 3 of 40 (7.5%) cases, the fourth revision in 2 of 40 (5.0%) cases, and the fifth revision in 1 of 40 (2.5%) cases.
In all, 36 of 40 (90.0%) revision stems eventually healed with bony union. The strut allograft was incorporated into the bone tissue of 37 of 40 (92.5%) patients (Fig. 1). There was one patient with RA whose revision stem and strut allograft did not ossify. Overall, 14 of 40 (35.0%) patients had at least one surgical complication during follow-up. The mean age of the patients without any complications was 76 years (range: 55–93 years) and with at least one complication was 76 years (range: 47–88 years). The mean follow-up time of the patients without complications was 51 months (range: 12–122 months) and of those with at least one complication was 54 months (range: 12–125 months). In all, 12 of 33 female patients (36.4%) and 2 of 7 male patients (28.6%) had at least one complication. The number of the study patients was too small to allow statistical comparison between gender and the occurrence of complications.
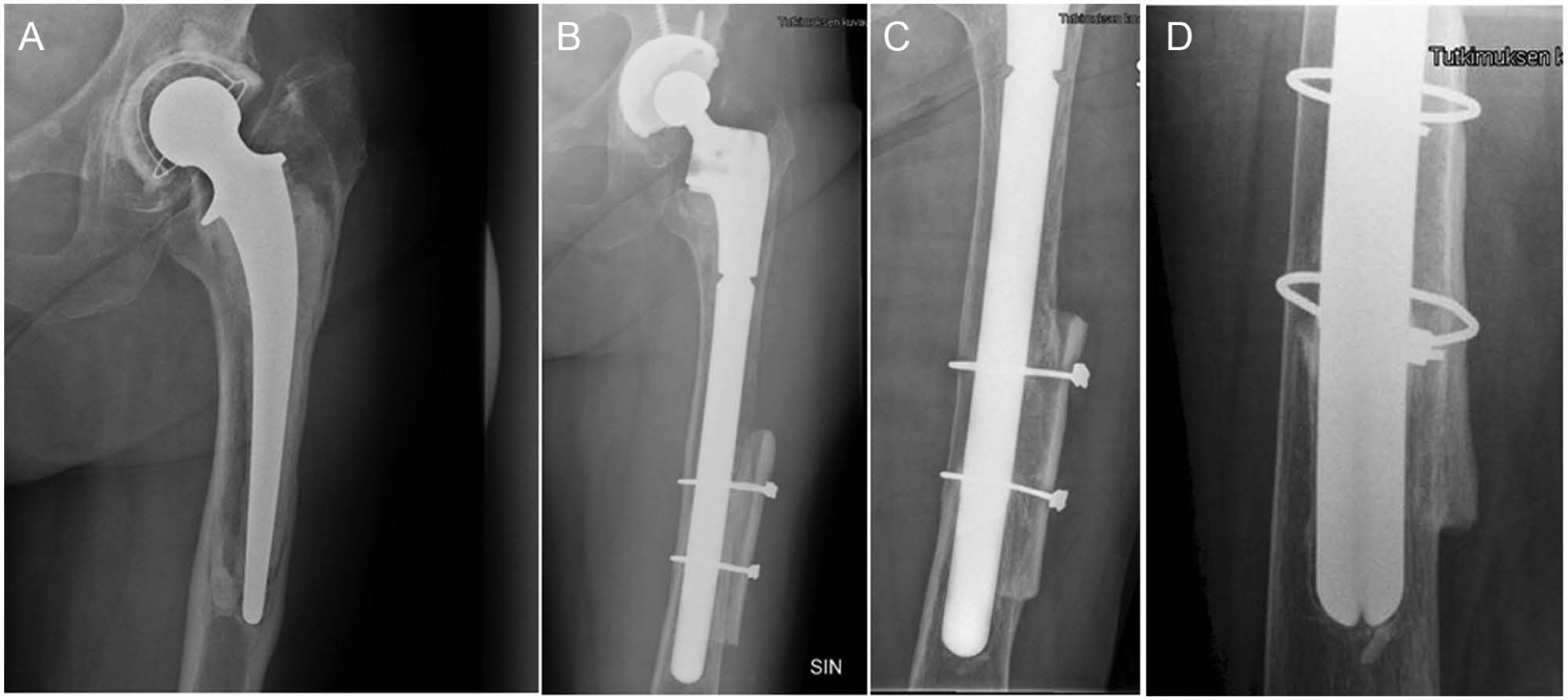
A) Preoperative radiograph of the left hip of a patient with a loose implant. B) Postoperative radiograph after revision with a Mallory-Head stem and a strut graft, which was used because of a perioperative fracture. Radiograph of the strut graft 3 years after the revision, C) anteroposterior-projection and D) lateral projection. The stem and the strut graft have healed.
Femoral bone deficiency grading (according to Paprosky) was successful in 30 patients. There were 5 Type I, 8 Type II, 8 Type IIIA, 6 Type IIIB, and 3 Type IV deficiencies. The number of the study patients was too small to allow statistical comparison between Paprosky grading and the occurrence of complications or osteointegration of the strut. When bone loss was further analyzed divided into two (mild bone loss, including Paprosky I and II, and severe bone loss, including Paprosky IIIA, IIIB, and IV), there were 3 of 13 (23.1%) complications in the mild bone loss group and 9 of 17 (52.9%) complications in the severe bone loss group. The association between the severity of bone loss (two-class) and the occurrence of complications was not statistically significant (p = 0.14). The mild bone loss was not associated with the occurrence of osteointegration of the strut either (p = 0.24).
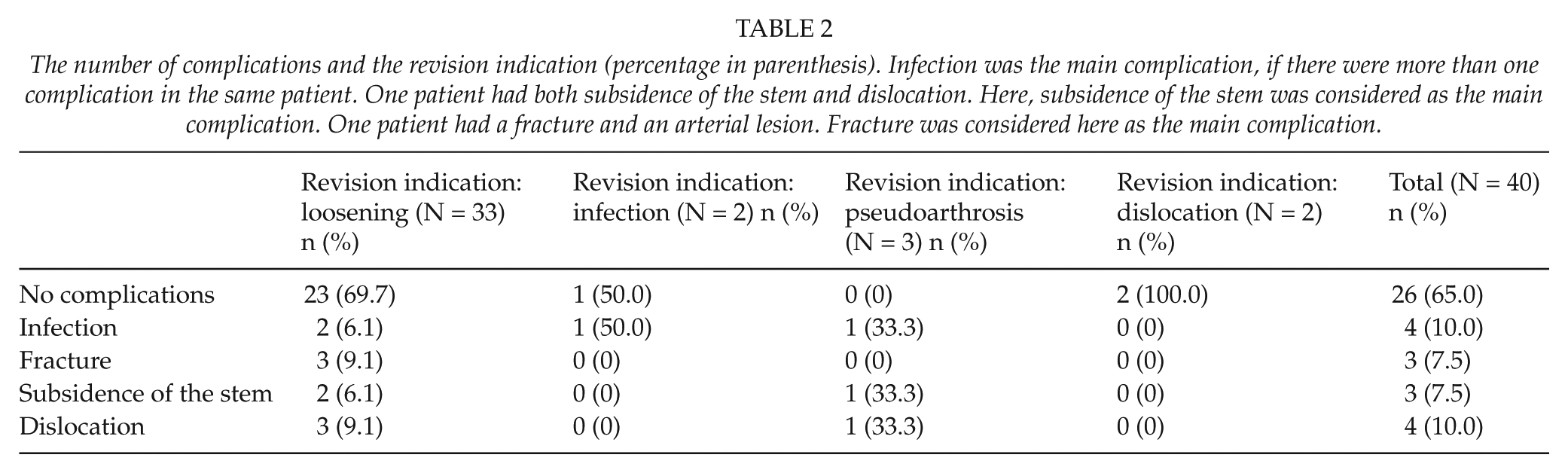
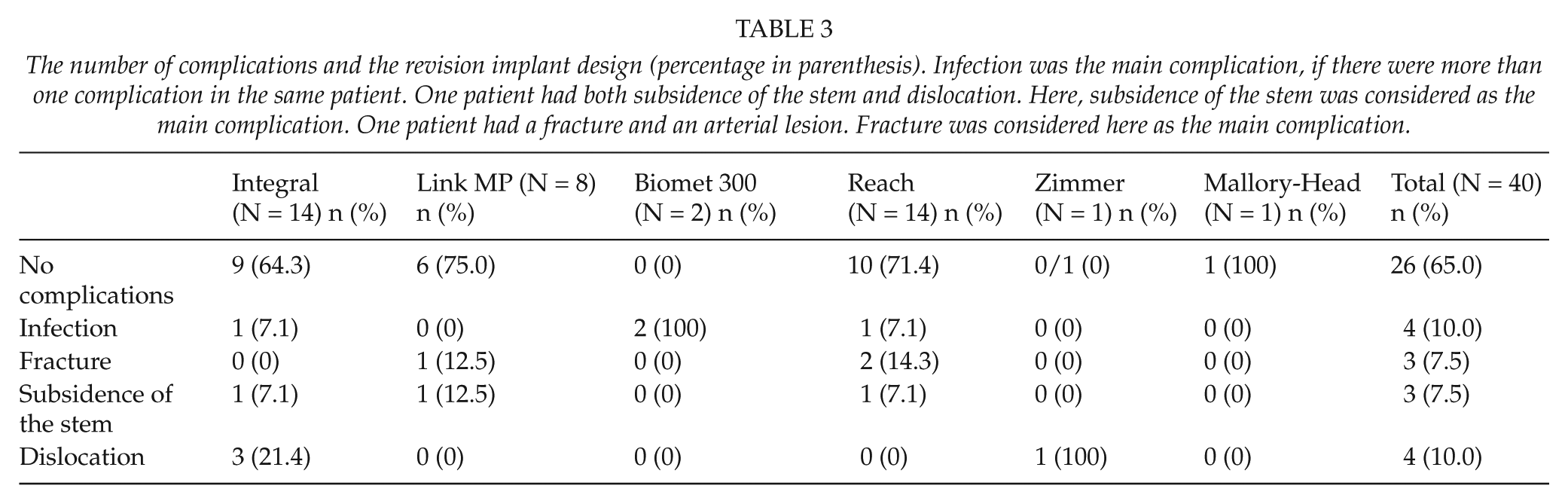
Both the strut graft and the cementless revision stem osteointegrated in 26 of 31 (83.9%) patients after a revision of a cemented stem and in 8 of 9 (88.9%) patients after a revision of a cementless stem. The number of complications by diagnosis is presented in Table 1, the number of complications by cause for revision is presented in Table 2, and the number of complications by stem design is presented in Table 3.
The number of complications in the revision operation and the diagnosis of the primary operation (percentage in parenthesis). Infection was the main complication, if there were more than one complication in the same patient. One patient had both subsidence of the stem and dislocation. Here, subsidence of the stem was considered as the main complication. One patient had a fracture and an arterial lesion. Fracture was considered here as the main complication.
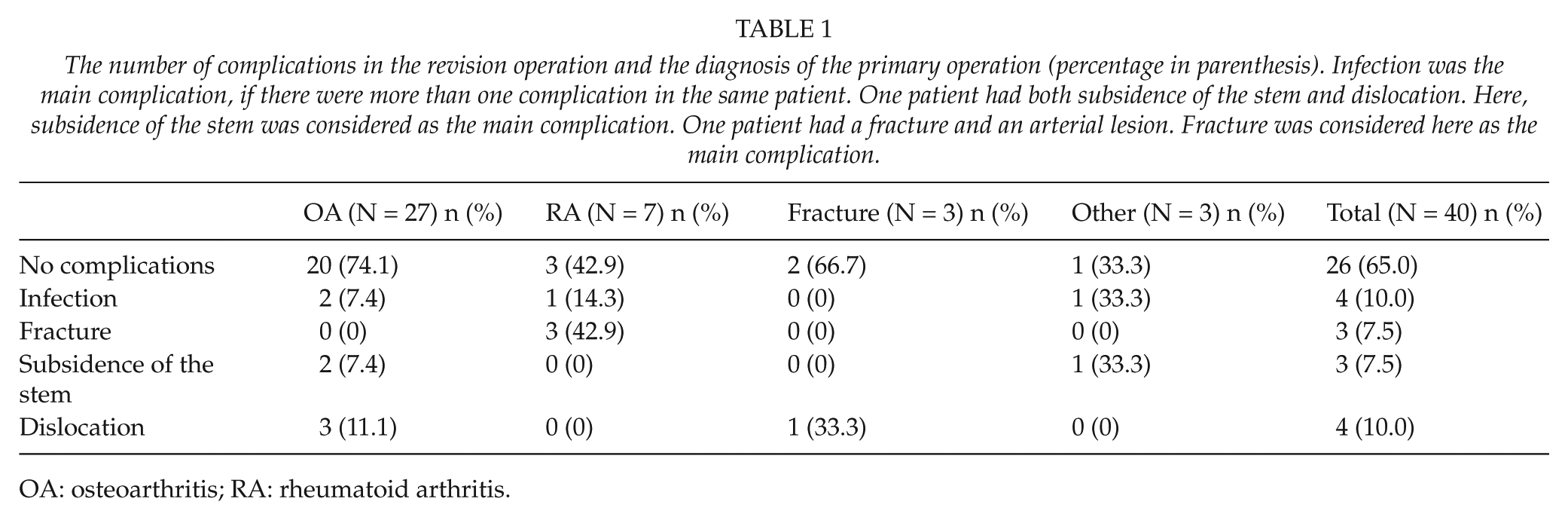
OA: osteoarthritis; RA: rheumatoid arthritis.
The number of complications and the revision indication (percentage in parenthesis). Infection was the main complication, if there were more than one complication in the same patient. One patient had both subsidence of the stem and dislocation. Here, subsidence of the stem was considered as the main complication. One patient had a fracture and an arterial lesion. Fracture was considered here as the main complication.
The number of complications and the revision implant design (percentage in parenthesis). Infection was the main complication, if there were more than one complication in the same patient. One patient had both subsidence of the stem and dislocation. Here, subsidence of the stem was considered as the main complication. One patient had a fracture and an arterial lesion. Fracture was considered here as the main complication.
Infection occurred in 4 of 40 (10.0%) patients during the follow-up, all among female patients. Of the 4 infections, 3 were deep (3 of 40, 7.5%) and 1 superficial (1 of 40, 2.5%). One patient with deep infection was treated by one-stage revision and parenteral antimicrobial agents. The strut graft was removed. The re-revision stem subsided, but the hip was still painful and antibiotic treatment continued. Two patients with a deep infection were treated only with parenteral antimicrobial agents and no surgery. During follow-up, the strut grafts and the revision stems became incorporated and the infections healed. The patient with a superficial wound infection was treated with superficial lavage. The strut graft and the stem became incorporated, and the infection healed during follow-up.
In all, 4 of 40 (10.0%) stems subsided and did not become incorporated. All needed revision. However, the strut graft united in three of these patients despite the loose stem. Overall, 6 of 40 (15.0%) stems became dislocated at least once. These dislocated hips were treated by closed reduction, open reduction, or revision of the cup (constrained liner). No stems were revised because of dislocation. There were 3 of 40 (7.5%) periprosthetic fractures, all among women. The strut graft did not heal in one of these; the stem osteointegrated in all three cases. There was a lesion in the distal part of the femoral artery in one patient who needed vascular reconstruction. The extremity leg and the strut healed. There were 19 of 31 (61.3%) patients without any complications in the cemented stem group and 7 of 9 (77.8%) patients in the cementless group. There were 20 of 31 (64.5%) patients without any complications in the long porous-coated revision stem group and 6 of 9 (66.7%) patients in the distal fixation revision stem group.
Discussion
We acknowledge that the present study has some methodological shortcomings. Our database does not include systematic data on the classification of femoral bone defects; we made the classification according to Paprosky retrospectively based on preoperative radiographs, and we had not assessed the validity of the available radiographs for interpreting graft incorporation. It is difficult to assess graft incorporation, given the amount of metal that is present, which includes not only the stem itself but also cerclages or Dall-Miles® cables, which cover the femur (10). However, the assessment of the available radiographs was performed systematically by two experienced physicians (H.K. and K.M.). Union of the grafts was defined as complete trabecular bridging between the graft and host bone (9, 10). We excluded patients with a follow-up of less than 1 year.
A mechanical failure rate of 4% has been reported with cementless fully porous-coated stems used with cortical strut allografts for revision THA (10, 15). However, the published series are small and they are not strictly comparable, since the revision methods and patient characteristics differ in different study populations. The revision methods in our clinic during the study period involved the use of long, extensively porous-coated cementless stems and the use of fluted distal fixation stems. The mechanical failure rate (aseptic loosening) in our study was 10.0%. The failed stems were all downsized and they had subsided soon after the index revision. Three stems were extensively porous-coated, and one was a distal fixation stem. Since THA revision with structural allografts is a demanding procedure, the operation should be performed by surgeons who have sufficient experience.
The radiographic union rate of the strut allograft varies reportedly from 92% to 100% (4, 9, 11). The grafts go through the phases of union, revascularization, remodeling, and maturation. The entire sequence takes 3–5 years (8). In this study, 92.5% of the allografts were incorporated into the osseous structure. The three-graft nonunions were associated with one failed revision stem and one periprosthetic fracture. Partial resorption of the strut noticed during the follow-up of one patient did not lead to malpositioning of the femoral stem or to reoperation. The strut graft union and complication rates were similar regarding the fixation method of the revised stem (whether cemented or cementless).
The potential problems associated with excessive use of allografts are devascularization of the proximal femur, increased risk of infection, increased time in surgery, and increased cost (10). The postoperative infection rate after revision THA with strut allografts varies from 6% to 11% (10, 13). The infection rate in this study was 10.0%. Our patients were old, had several medical problems, and needed multiple surgical interventions. Strut graft fixation with cables is nowadays a relatively fast operation compared to the total operation time of a revision THA. However, in contrast to patients with periprosthetic fractures, these patients are prepared for surgery on an elective basis. Infection risk may be increased due to massive strut allografts.
Seven of the 40 patients had RA; 4 of 7 (57.1%) of rheumatoid patients experienced at least one complication, whereas the corresponding rate among the patients with OA was only 25.9%. The overall bone quality of RA patients is usually weaker than that of OA patients due to the disease itself and chronic medication with glucocorticosteroids. The total number of patients was small, and statistical comparisons between the OA and RA groups were not possible.
The strut grafts are removed from the femur or tibia in connection with other organ banking procedures of cadaver donators soon after death. Strictly aseptic conditions are maintained. The method involves ethical and economical aspects. Since usually other organs of the cadaver are also removed simultaneously for recipient use (heart, lungs, liver, kidneys, corneas), the ethical issues are manageable. Having said this, we nevertheless need to be reassured that the use of transplanted organs is in full agreement with the donor’s lifetime wish and with the family of the departed. Allografting is expensive. Still, organ transplants and tissue banking are important part of modern treatment of severe diseases.
There are publications reporting good long-term results of femoral impaction bone grafting in the treatment of bone deficiency in connection with revision THA (16–19). However, these reports are often generated by clinics involved in developing the techniques (16, 19). On the contrary, there are several reports of complications due to femoral impaction bone grafting, especially of fractures and of massive subsidence of the stem (20–22). Our own experience is similar to those of the latter. The use of modular proximal femoral reconstruction prostheses (“megaprostheses”) is an option for treating massive metadiaphyseal bone loss, and recent reports claim quite good results. However, infections and dislocations still constitute a problem (23, 24). Our experience is that the indications for using these reconstruction prostheses are not identical with those for revision with strut grafts or impaction bone grafting. In our hands, reconstruction prostheses are best used as salvage implants under nonneoplastic conditions.
In conclusion, the use of cortical onlay allografts provides a feasible option for restoring the integrity of the proximal femur in revision THA. However, the retrospective results reported in this article show a high percentage of complications, especially among female patients with RA. Since the operative procedure is rather demanding, the surgeon performing these operations should be experienced and familiar with it. We believe that the early mechanical stabilizing effect of the strut grafts contributes crucially to a satisfactory outcome for most patients.