
Abstract
Background and Aim:
Single-incision laparoscopic surgery is a rapidly progressing field as it combines some advantages such as cosmesis and less incisional pain. However, it also has some disadvantages such as limitation of movement and clashing of the hand instruments, which increase the complexity and technical challenges of the operation. In this study, we describe a pilot trial of single-incision laparoscopic cholecystectomy through a paramedian access site.
Material and Methods:
A total of 25 patients underwent single-incision laparoscopic cholecystectomy with this method. Acute cases with empyema and patients with history of previous abdominal surgery were excluded. Single-incision is established on the right upper quadrant, right latero-superior of the umbilicus, so that trocar sites and projection of the gallbladder on the abdominal wall are on the same vertical line. Standard laparoscopic instruments were placed into the abdominal cavity providing triangulation. Once the laparoscope, grasper, and dissector are in place, the overall procedures are similar to the standard laparoscopic cholecystectomy.
Results:
Single-incision laparoscopic cholecystectomy through an extraumbilical access site was successfully completed in all 25 patients without conversion to open surgery. Additional skin incisions and trocar access were required only in two patients. The mean operative time was 39.3 min (range: 20–75 min). The mean body mass index was 27.2. Postoperative course was uneventful in all patients. The mean postoperative hospital stay was shorter than 24 h, and all patients were discharged at first day postoperatively. No postoperative complications including seroma, wound infection, and trocar-site hernia were observed at 6-month follow-up.
Conclusion:
We described a new access site for single-incision laparoscopic cholecystectomy using standard laparoscopic instruments. We believe that this type of access site overcomes the technical difficulties of performing single-incision laparoscopic cholecystectomy, and it is a promising alternative method for the treatment of patients with symptomatic gallstone disease as a minimal invasive abdominal surgery.
Introduction
Single-incision laparoscopic surgery (SILS) is an area of current investigation for laparoscopic surgery. In 1997, Navarra et al. (1) first described one-wound laparoscopic cholecystectomy, and in 1999, Piskun and Rajpal (2) performed SILS by inserting two trocars through the umbilical incision and putting additional stay sutures to retract and stabilize the gallbladder. SILS is evolving and adapted to different surgical procedures such as appendectomy, colectomy, nephrectomy, splenectomy, hepatectomy, and so on (3–13).
A number of advantages of single-incision laparoscopic cholecystectomy (SILC) have been proposed, such as cosmesis (scarless cholecystectomy) and ability to convert to standard four-port laparoscopic surgery when needed (14). A few different methods have been described for trocar access to perform SILC, including transumbilical single-port access (SPA) with the use of novel trocar access devices such as Unix-X™ (Pnavel Systems, Brooklyn, NY, USA) and R-port™(Advanced Surgical Concepts, North Attleboroma, USA), multiple fascial punctures through one transumbilical skin incision, and SPA with the use of additional transabdominal retraction sutures to retract the gallbladder (15). The major disadvantages of SILC are restriction of hand movements and clashing of the instruments either intra-abdominally or extra-abdominally, making the operation more complex and technically difficult. In this study, we describe a new access site to overcome some of these technical challenges in performing SILC.
Material and Methods
All patients underwent surgery after obtaining approval from the local Ethics Committee. Written informed consents were obtained from all patients. The differences between single-incision and the standard four-incision approach were explained to volunteers.
Patients
A total of 25 patients underwent SILC with the new technique. All the patients underwent surgery by a single surgeon, experienced in laparoscopic surgery. Five patients had history of previous biliary pancreatitis, and all had symptomatic gallstones. Patients with previous open abdominal surgery and acute cases with empyema were excluded (Table 1).
The demographic and operative data of the study group.
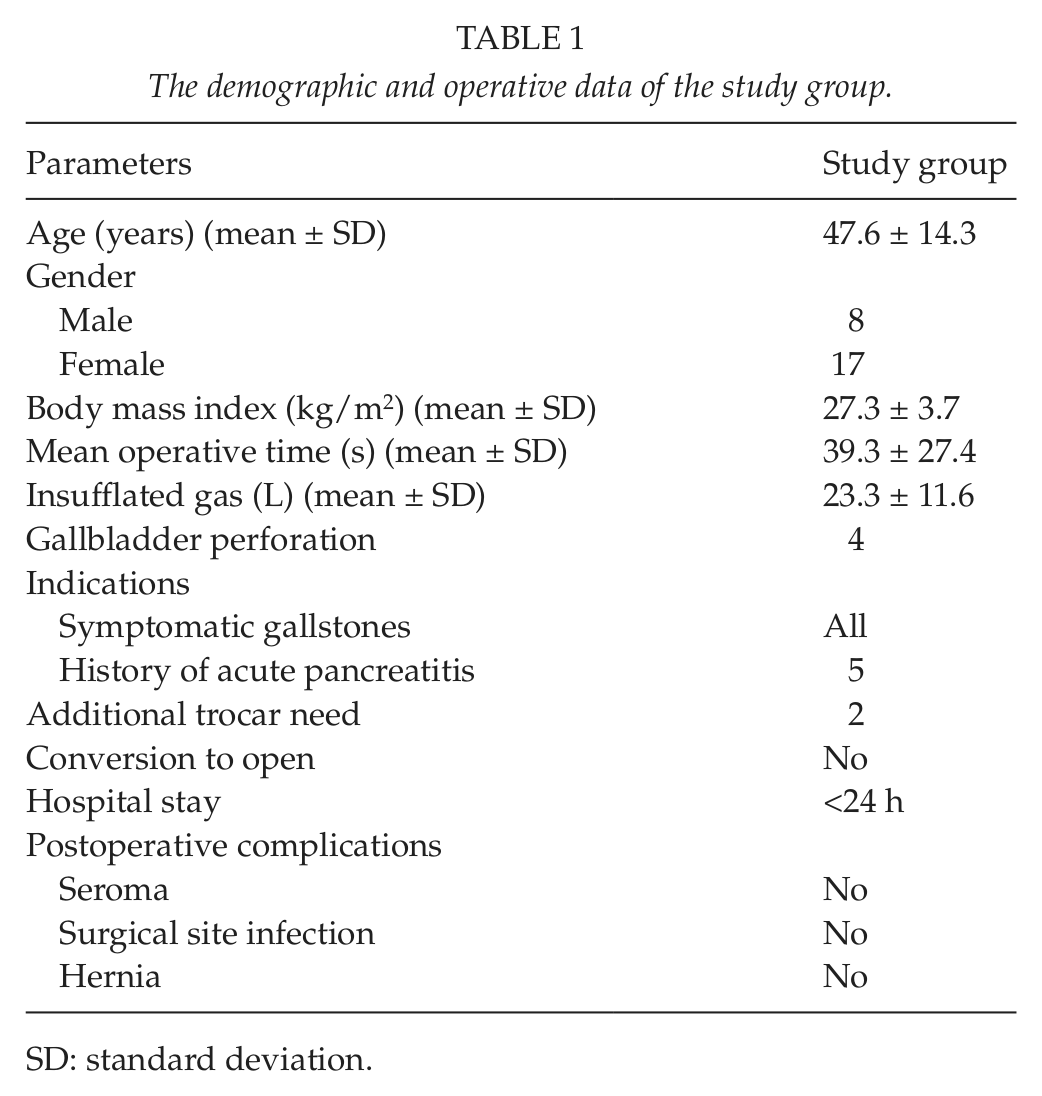
SD: standard deviation.
Postoperative Analgesia
Postoperative analgesia was provided by intravenous diclofenac sodium and tramadol injections. In case of first analgesia need, patients were given diclofenac sodium. For recurrent or persistent pain, tradamol was given as second-line therapy.
Operative Technique
Under general anesthesia, the patients were placed in a supine split-leg position, then put in a reverse Trendelenburg position with the left side slightly rotated down to allow the surgeon to stand between patient’s legs, and then, intra-abdominal pressure of 12–14 mmHg was achieved. A single 3-cm horizontal skin incision, 4 cm lateral and 3 cm superior to the umbilicus on the right upper quadrant, was established, so that the trocar site and the gallbladder’s projection on the abdominal wall were on the same vertical line to minimize the angle between them and in order to prevent clashing of the hand instruments (Figs 1, 2). Subcutaneous flaps were established to provide a sufficient area for placement of three trocars. This approach reduces the difficulty of the hand movement and clashing of the devices in the abdominal cavity during cholecystectomy. Then, the 5-mm camera trocar was placed into the abdominal cavity from the lowest inferior point, midline of the dissected area. Other two trocars were placed into the abdominal cavity by direct vision, both superior to the camera trocar (Fig. 3). We preferred to use 30° laparoscope for laparoscopic cholecystectomies. After exposure of the hepatocystic triangle, the cystic duct and artery were clipped. The gallbladder was dissected away with a hook electrocautery. The gallbladder was removed within an endoscopic retrieval bag (Endo Catch™, Covidien Inc., Mansfield, MA, USA) and sent for pathological analysis.
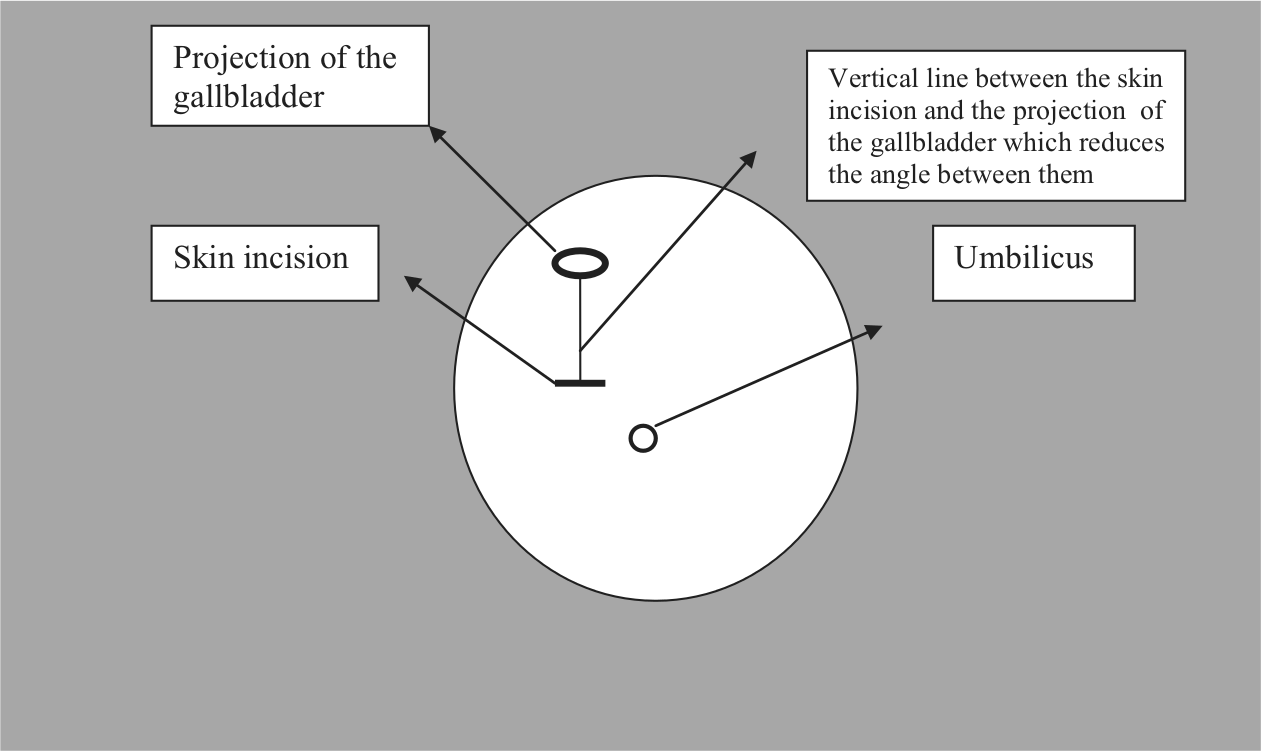
Illustration of the incision site.

Positioning of the three trocars.
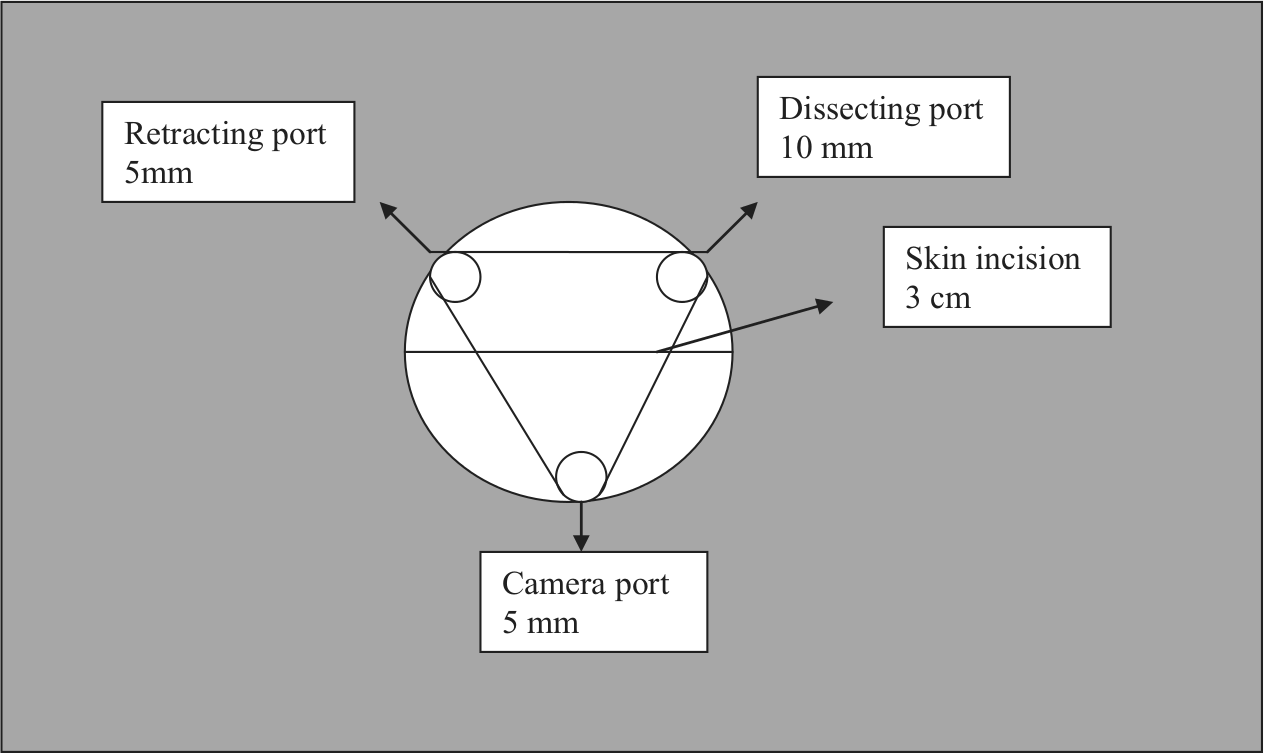
Illustration showing positioning of the trocars.
Results
SILC through an extraumbilical site was successfully completed in all 25 patients without the need for conversion to open surgery. The mean ± standard deviation (SD) age of patients was 47.6 ± 14.3 years (range: 25–78 years), 17 were women, and 8 were men. The mean ± SD body mass index (BMI) was 27.3 ± 3.7 (range: 22–35). Additional skin incisions and trocar access were required only in two patients. The mean ± SD operative time was 39.3 ± 27.4 min (range: 20–75 min). No major bleeding was observed in all cases. The mean ± SD gas requirement was 23.3 ± 11.6 L. Gallbladder perforation occurred in four cases during dissection. The postoperative period was uneventful in all patients. The mean postoperative hospital stay was shorter than 24 h, and all patients were discharged at first postoperative day. No postoperative complication (seroma, surgical site infection) and no trocar-site hernia were observed at 6-month follow-up period after surgery (Table 1).
Discussion
Laparoscopic cholecystectomy is the gold standard for gallbladder removal. With laparoscopy, the aim is to achieve a better operative outcome with less parietal trauma and faster recovery compared to conventional open surgery. SILS is a rapidly evolving field and offers similar advantages plus cosmesis (14, 16, 17). Although it has the advantage of lower complexity for clinical application compared to “natural orifice transluminal endoscopic surgery” (NOTES), it still has much more technical difficulties than standard laparoscopic approach (18). Therefore, it has not gained widespread use (19, 20).
Rao et al. (21) reported three problems during SILC in their initial experiences. First, the entry of the instruments through a single port leads to clashing of instruments, the so-called chopstick effect and loss of triangulation. Second, the instruments clash with tangential telescope. Third, there is difficulty in inserting a 10-mm clip-applier because tri-port trocar allows ingress of only one 10-mm instrument (21). Gumbs et al. (22) also reported that at least one articulating instrument is necessary to prevent clashing during cholecystectomy and deflecting scope is necessary to minimize external interference of the instrument handles. However, using the SILS instruments can be challenging for the surgeon. For this reason, studies were done indicating that no curved or articulating instruments are needed to perform SILC, in which the procedures were completed safely (23–25).
These technical challenges inspired us to use a new access site. The access site can be accepted as a 3-cm paramedian minilaparotomy. The minilaparotomy techniques were previously described; however, in these studies, the incision site was in subcostal area (26–28). The extraumbilical single-incision technique minimizes the clashing of instruments and gives us opportunity for using 10-mm hand devices such as clip applicator. In all transumbilical techniques, surgeons deal with clashing of the instruments and with limitation of freedom of movements, all of which increase the complexity of the operation (15, 29, 30). These technical difficulties also lead to consumption of more gas, energy, and time. They usually require the use of one or two more trocars or transparietal suspension stitches for exposure of the Callot’s triangle (29, 30). Clashing usually prevents using even two instruments, and some additional trocars are needed. This extraumbilical access site eliminates the 45° angle between the gallbladder and umbilicus, which avoids the clashing and eliminates the limitation of the movement of hand devices (Fig. 4). We overcame this issue during dissection by retracting the Hartmann’s pouch or by using some instruments such as right-angle dissector when needed (Fig. 5). The mean duration of operation was 39.3 min, and these data imply that extraumbilical approach can eliminate the technical challenges of the operation (21, 22). The other advantage of this extraumbilical technique is that no reticulating instrument was needed. We used 30° laparoscope, which provides a safer vision during dissection (Fig. 6).
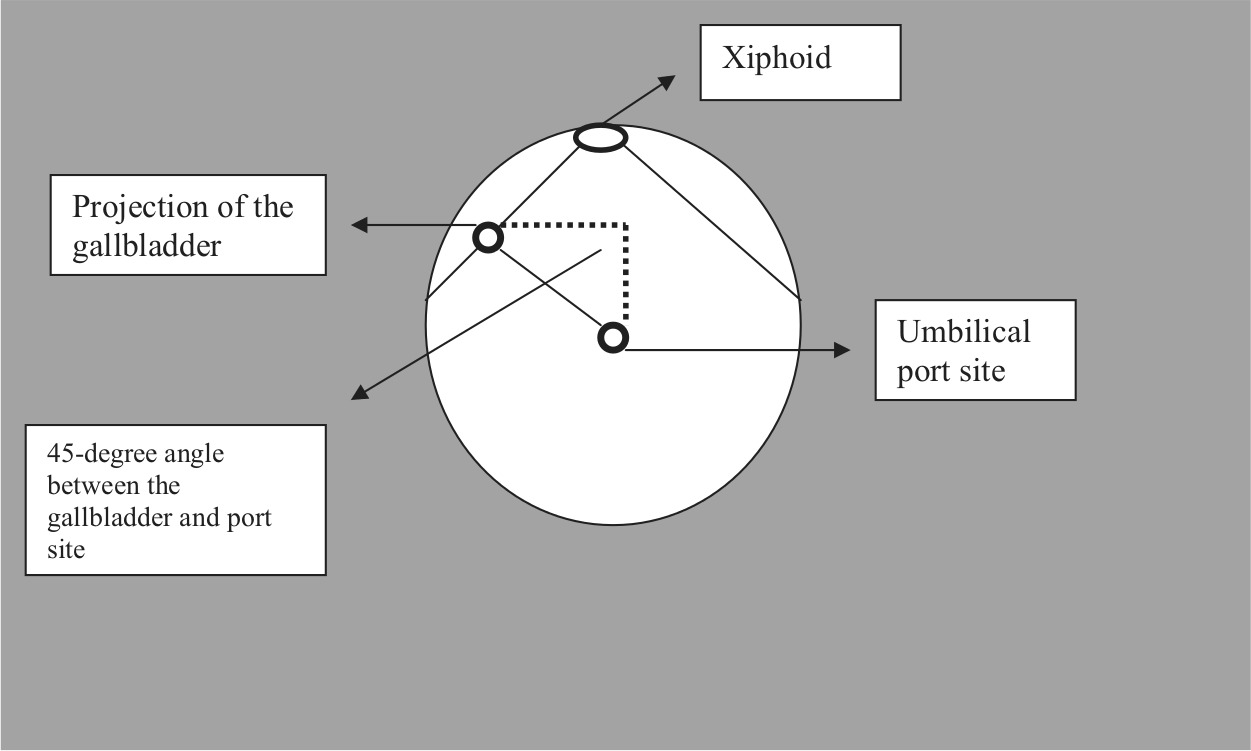
In transumbilical technique, 45° angle between the gallbladder and port access can cause technical challenges.
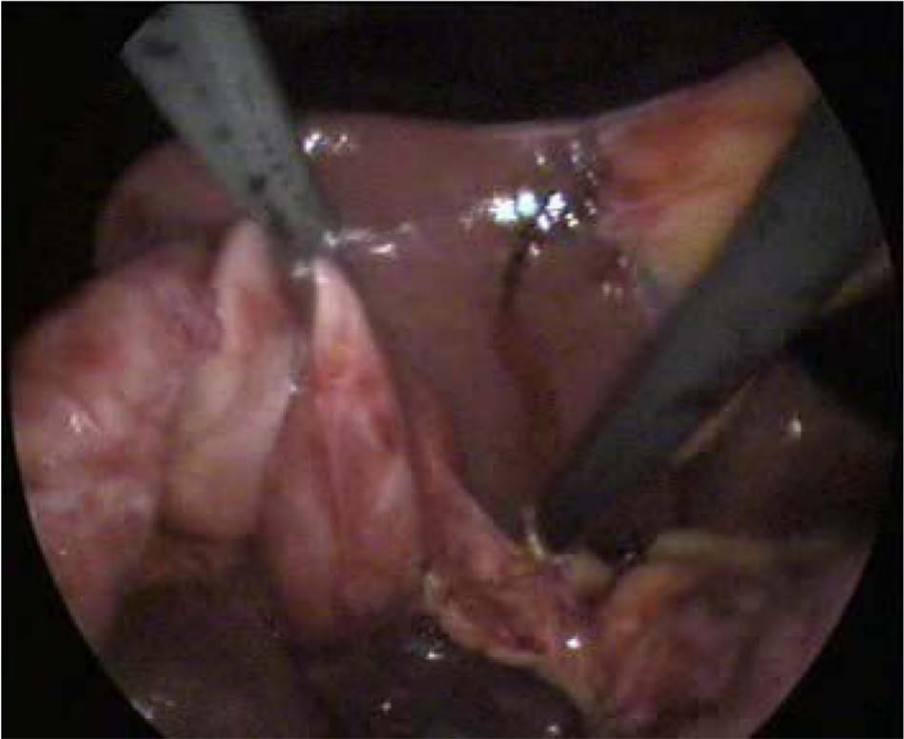
Reduced angulation during the dissection of Callot’s triangle can be overcome by retracting Hartmann’s pouch or with a right-angle dissector.
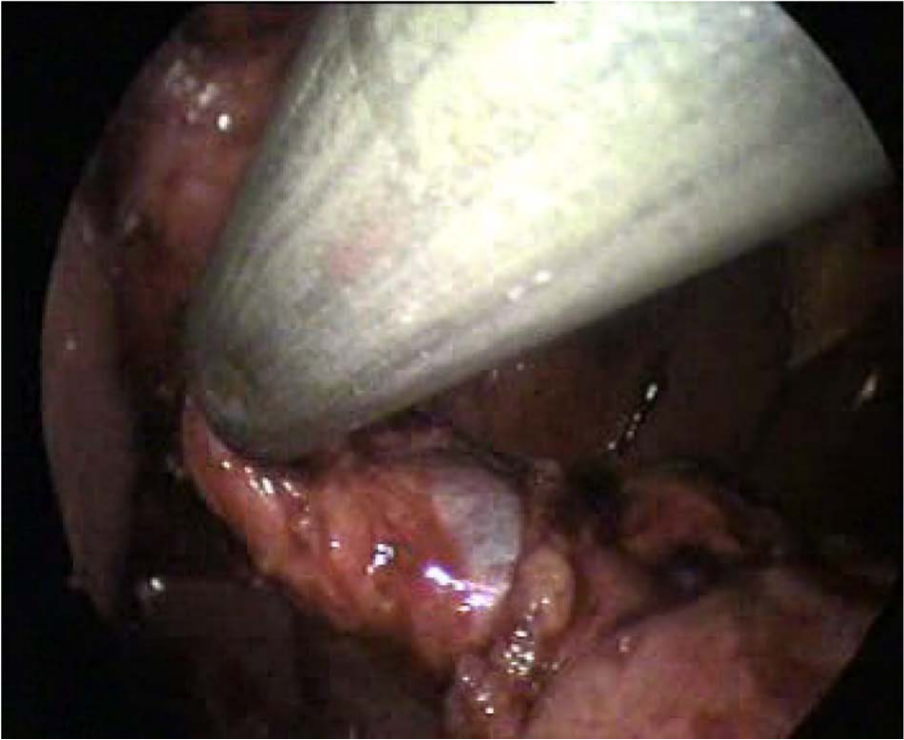
Exposition of the tip of the right angle behind the cystic duct and artery.
The major disadvantage of the technique is that the scar cannot be hidden as in transumbilical approach. Since the primary clinical advantage of SILC is cosmesis, paramedian incision causes a visible scar, but one scar seems to be reasonable compared to standard four-port laparoscopic cholecystectomy.
All of the procedures were completed safely. We have not detected any port-site hernias or wound complications at 6-month follow-up. Our results such as analgesic need and hospital stay have implied that our patients had comfortable postoperative period. Additionally, in all transumbilical single-port techniques 1.5- to 2-cm fasciotomy is required, which carries potential for hernia development and needs fascial suturing. Therefore, in addition to the above-mentioned perioperative advantages, we assume that this new method can reduce port-site hernia rate as we only perform fascial puncture on the paramedian position (Fig. 7).

Performing the fascial puncture.
Conclusion
In this study, we described a new access site for SILC. All procedures were completed successfully within a short time and with a reasonable skin scar. According to our experience, many of the patients with gallstone disease are amenable to this approach. We believe that this type of access site overcomes the technical difficulties of performing SILC, and therefore, this technique is a promising alternative method for the treatment of patients with symptomatic gallstone disease as a minimal invasive abdominal surgery.
Footnotes
Declaration of Conflicting Interests
The authors declare that there is no conflict of interest.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.