
Abstract
Aim:
To assess the early and short-term outcome of fenestrated and chimney grafting for juxtarenal aortic aneurysms.
Material and Methods:
A prospective vascular registry of 28 patients who had undergone elective primary endovascular repair for abdominal aortic aneurysm between December 2007 and August 2011 with infrarenal neck anatomy unacceptable for conventional endovascular repair. Fenestrated endografts were designed based on reconstructed computed tomography (CT) data by the authors. Off-the-shelf grafts and stents were used for chimney cases. Patients were followed up until 31 May 2012.
Results:
A total of 21 (75%) patients were treated with fenestrated endografts, while 7 (25%) received chimney grafts. The mean aneurysm diameter was 65 mm (standard deviation = 7 mm) and the median neck length 2.5 mm (range: 0–10 mm). Altogether, 63 (mean = 2.3/patient) visceral arteries were incorporated (42 renal, 21 superior mesenteric arteries). The overall primary technical success rate was 93% (one type I and one type III endoleak). The mean follow-up was 22 months (standard deviation: 14 months). The primary type III endoleak resolved spontaneously with thrombosis of the target vessel, while the patient with primary type I endoleak died of acute myocardial infarction 3 weeks after the procedure. Two late endoleaks developed: one type II endoleak without aneurysm sac growth remains under surveillance, while in another patient, multiple attempts to treat type I endoleak proved unsuccessful and the patient later died of gastrointestinal bleeding. A total of 4 (14%) patients so far required additional procedures. Two patients died within 30 days of the device implantation and another six during the follow-up. No rupture occurred. The cumulative survival for patients with fenestrated endografts was 85% at 1 year and for those treated with chimney technique 57%.
Conclusions:
The treatment of juxtarenal aortic aneurysms seems to be feasible by exploiting various endovascular techniques. Even with a low volume of cases, good immediate and short-term results can be achieved, especially with fenestrated endografts.
Introduction
Endovascular aortic repair (EVAR) has developed as a less-invasive technique for the treatment of infrarenal abdominal aortic aneurysms (AAAs) (1, 2). However, 30%–50% of AAA patients are not suitable for elective conventional endovascular repair due to anatomical reasons such as a short (<10 mm) proximal landing zone (3, 4). These juxtarenal aortic aneurysms (JAAs) account for approximately 15% of all AAAs (5). Alternative treatment options for JAA repair include open reconstruction, fenestrated endovascular aneurysm repair (FEVAR), and chimney grafts (CGs).
Recent results of open JAA repair show that the procedure is generally safe and has an acceptable postoperative mortality rate compared to infrarenal aortic reconstruction (6). However, due to the perioperative renal ischemia associated with suprarenal cross-clamping, postoperative deterioration in renal function is common and the need for permanent hemodialysis is reported to be up to 13% (4, 6, 7). Furthermore, the 1-year mortality rate of patients over 70 years of age with chronic obstructive pulmonary disease (COPD) is almost 30% (8).
FEVAR, as an alternative endovascular solution for patients with a short infrarenal neck, was first introduced in 1999 (9). Fenestrated grafts were designed to extend the proximal sealing zone from the infrarenal segment to the juxtarenal and suprarenal aorta by tailoring fenestrations or scallops in the proximal portion of the stent graft. These grafts can be used with or without bridging stents to permit perfusion of the visceral vessels. The long manufacturing time and significant cost related to the individual design limit the use of this technique. Severe neck angulation and inadequate iliac access may also hamper the use of fenestrated endografts.
The chimney technique was originally described in 2003 as a bailout procedure for misplaced endografts (10). This technique exploits off-the-shelf endografts and stents to exclude a JAA. Even though the data are still sparse, it seems that CGs can be used as an alternative for fenestrated endografts in an emergency setting or when the patient’s anatomy precludes the use of more sophisticated grafts (11). The purpose of this study was to assess the early and midterm outcome of fenestrated and chimney grafting for JAAs in an academic institution.
Material and Methods
Patients
We utilized data from the prospectively collected local vascular registry at Tampere University Hospital (TAUH), Finland. TAUH serves as a tertiary referral vascular surgical center for approximately 1.2 million inhabitants, with more than 70 conventional EVARs performed annually. All consecutive patients undergoing an attempt to repair an intact juxtarenal AAA with FEVAR or the chimney technique between December 2007 and October 2011 were included in this study. The cohort was followed up until 31 May 2012.
Comorbid Conditions
The patients were evaluated for preexisting medical comorbidities including diabetes mellitus, hyperlipidemia, hypertension, smoking within 5 years, any cardiovascular disease (peripheral arterial disease (PAD), coronary heart disease (CHD), cerebrovascular disease), respiratory disease, and chronic renal failure. The diagnosis for each disease was considered positive if it had been previously established at TAUH or mentioned in the referral or if the patient was on appropriate medication. The patients were further classified using the American Society of Anesthesiologists (ASA) guidelines. Renal function was evaluated preoperatively and at 1 month postoperatively by calculating the estimated glomerular filtration rate (eGFR; >90 mL/min considered normal) (12). A shift of one stage downward or initiation of hemodialysis was considered a significant postoperative deterioration in kidney function.
Treatment Options
In order to be considered for endovascular repair of JAA (including pseudoaneurysms), the patients had to have an aneurysm of at least 55 mm (50 mm in women) in diameter and be unsuitable for open reconstruction. The contraindications for open surgery included a hostile abdomen (4 patients), advanced age (>75 years; 17 patients), and an unfavorable combination of comorbidities (7 patients). Patients with an aortic neck of less than 45° and adequate access vessels (available) were deemed for FEVAR, while those with more severe neck angulation and poor iliac access were considered candidates for chimney grafting. All procedures were performed under spinal anesthesia (combined with an additional local anesthesia for brachial access) in a hybrid suite.
Endografts
For FEVAR, a three-component CE-approved fenestrated endograft (Zenith; Cook Australia Ltd, Australia) was used (Fig. 1). All customized fenestrated devices were designed based on computed tomography (CT) reconstructions (slice thickness of maximum 1 mm) by the authors. Arteriography was utilized selectively to evaluate concomitant occlusive disease of the visceral or iliac arteries. The design, planning of the fenestrations (scallops), and implantation procedures have been described previously (13). Covered stents (Advanta V12; Atrium, USA) were used to bridge the main graft and branch vessels. If the anatomy was considered unsuitable for FEVAR, we used off-the-shelf endografts (Excluder; WL Gore, Arizona, USA) and covered renal stents (Advanta V12, Atrium) to create a CG (Fig. 2). For this purpose, the renal arteries were catheterized with a brachial approach employing a standard endovascular technique. A detailed technical description of the chimney technique is provided elsewhere (11).
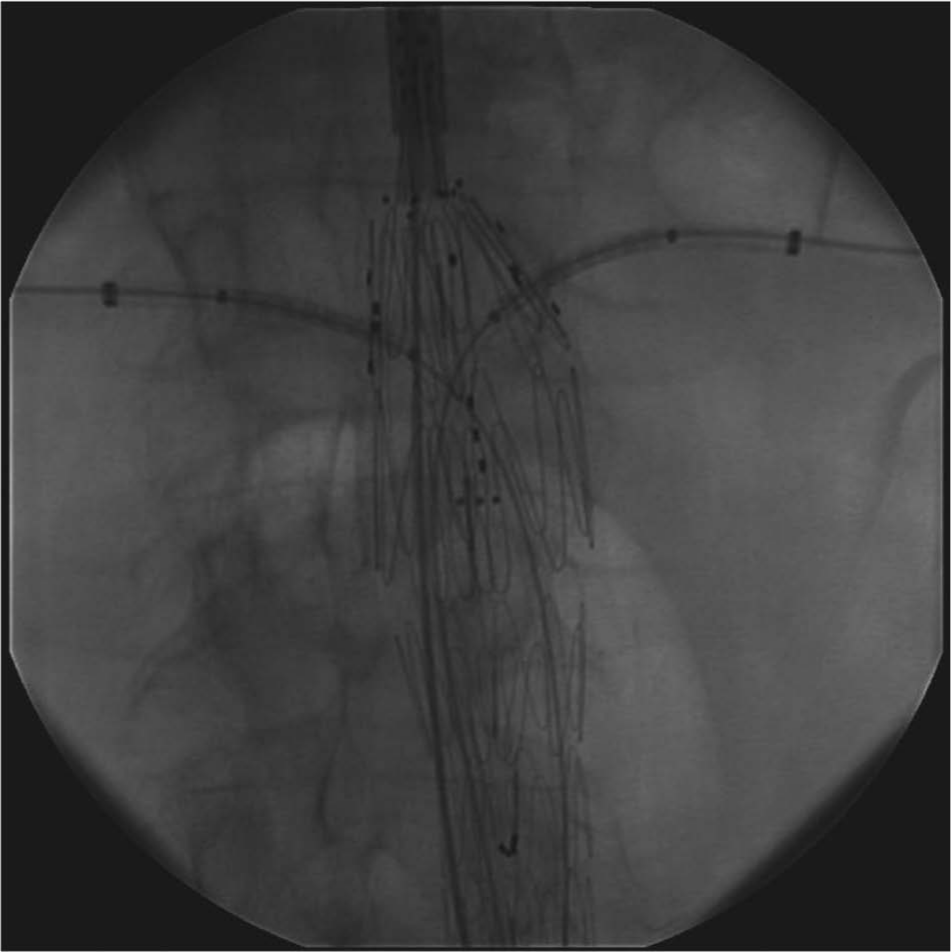
Fenestrated endograft deployment.

Completion angiogram of a chimney graft.
Follow-up
The postoperative follow-up protocol included a clinical examination, laboratory studies (serum creatinine and corresponding eGFR), and a radiological evaluation with CT at 1 month and at 2 years, in addition to duplex ultrasound together with plain film radiographs at 1 year and annually thereafter. The early results cover the period from the initial procedure to the 30-day follow-up and the midterm results from there on up to 5 years.
Outcome Measures
For this article, we used the pragmatic minimum reporting standards for EVAR described by Boyle et al. (14). Outcomes were assessed in terms of survival, target vessel patency (TVP), graft-related complications, and reinterventions. Deaths were ascertained by means of record linkage of the study data with the National Causes of Death Register on the basis of the personal identification code unique to every resident in Finland.
Results
Patients and Comorbid Diseases
A total of 28 patients (26 men and 2 women) were treated. Of these, 21 (75%) were managed with FEVAR, while 7 (25%) received CGs. The mean age was 75 years (standard deviation (SD) = 7 years, range: 57–89 years). Patient characteristics are presented in Table 1. The median ASA score was 3 (2–4). Two patients were on hemodialysis prior to the procedure, and only three had normal renal function according to the eGFR (mean eGFR = 66 mL/min, SD = 23 mL/min).
Baseline characteristics of participants (N = 28).
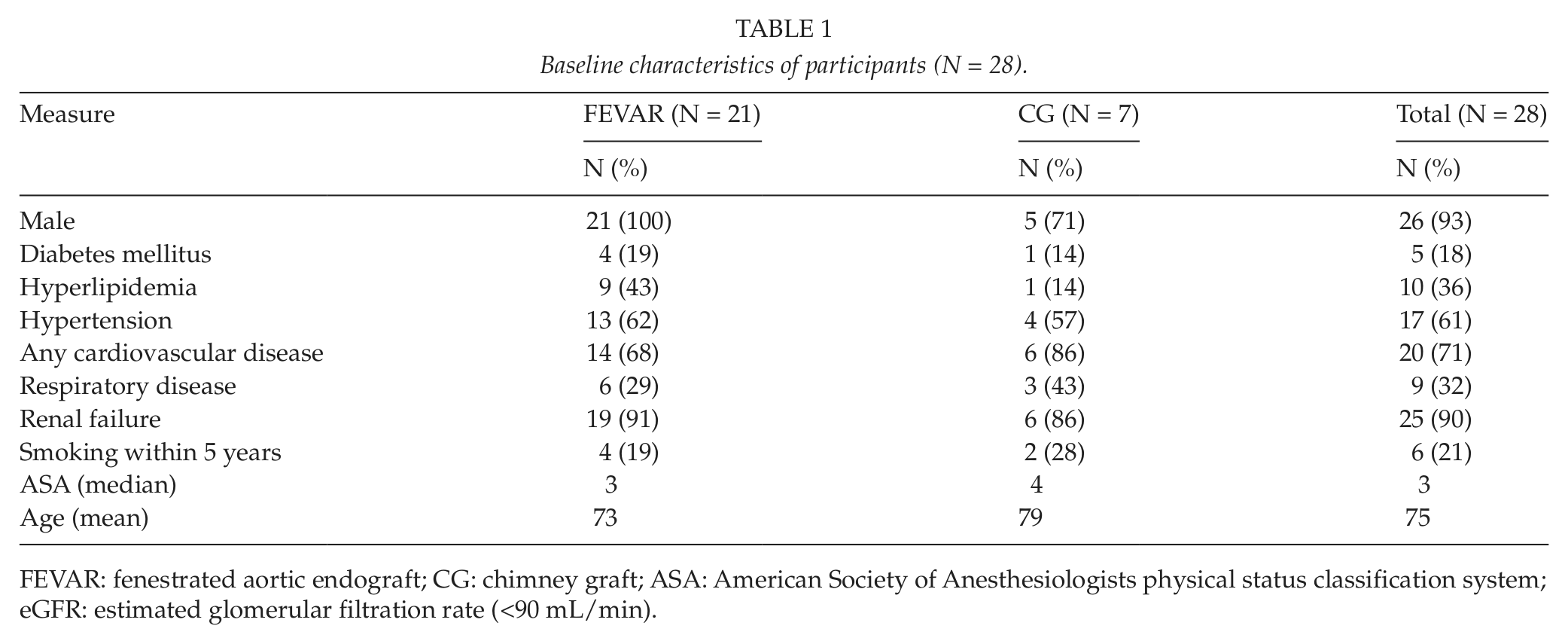
FEVAR: fenestrated aortic endograft; CG: chimney graft; ASA: American Society of Anesthesiologists physical status classification system; eGFR: estimated glomerular filtration rate (<90 mL/min).
Aneurysms
The mean aneurysm diameter was 65 mm (SD = 7 mm, range: 54–79 mm) and the median neck length 2.5 mm (range: 0–10 mm). There were two (7.1%) juxtarenal pseudoaneurysms following previous aortic surgery: one after end-to-end aortobifemoral reconstruction for AAA and the other after end-to-side aortobifemoral reconstruction for PAD. Aneurysm neck angulation of >45° was present in three patients and inadequate iliac access in four patients. These seven cases were consequently treated with the chimney technique.
Endografts
For FEVAR, a three-component system was deployed in each case. The most common configuration for FEVAR was two small fenestrations for the renal arteries and a scallop for the superior mesenteric artery (SMA; 12/21). The FEVAR graft configurations are presented in Table 2. One of the patients on hemodialysis was treated with a single scallop graft for the SMA and the other with a scallop for the celiac artery (CA) and a large fenestration for the SMA. Three patients had one functioning kidney, and therefore, only one small fenestration together with a scallop (large fenestration in one patient) for the SMA was required. Two patients had three fenestrations (large for the SMA and two small for the renal arteries) together with a scallop for the CA, and another two individuals had one large and two small fenestrations without a scallop.
Character of procedures and 30-day outcome.
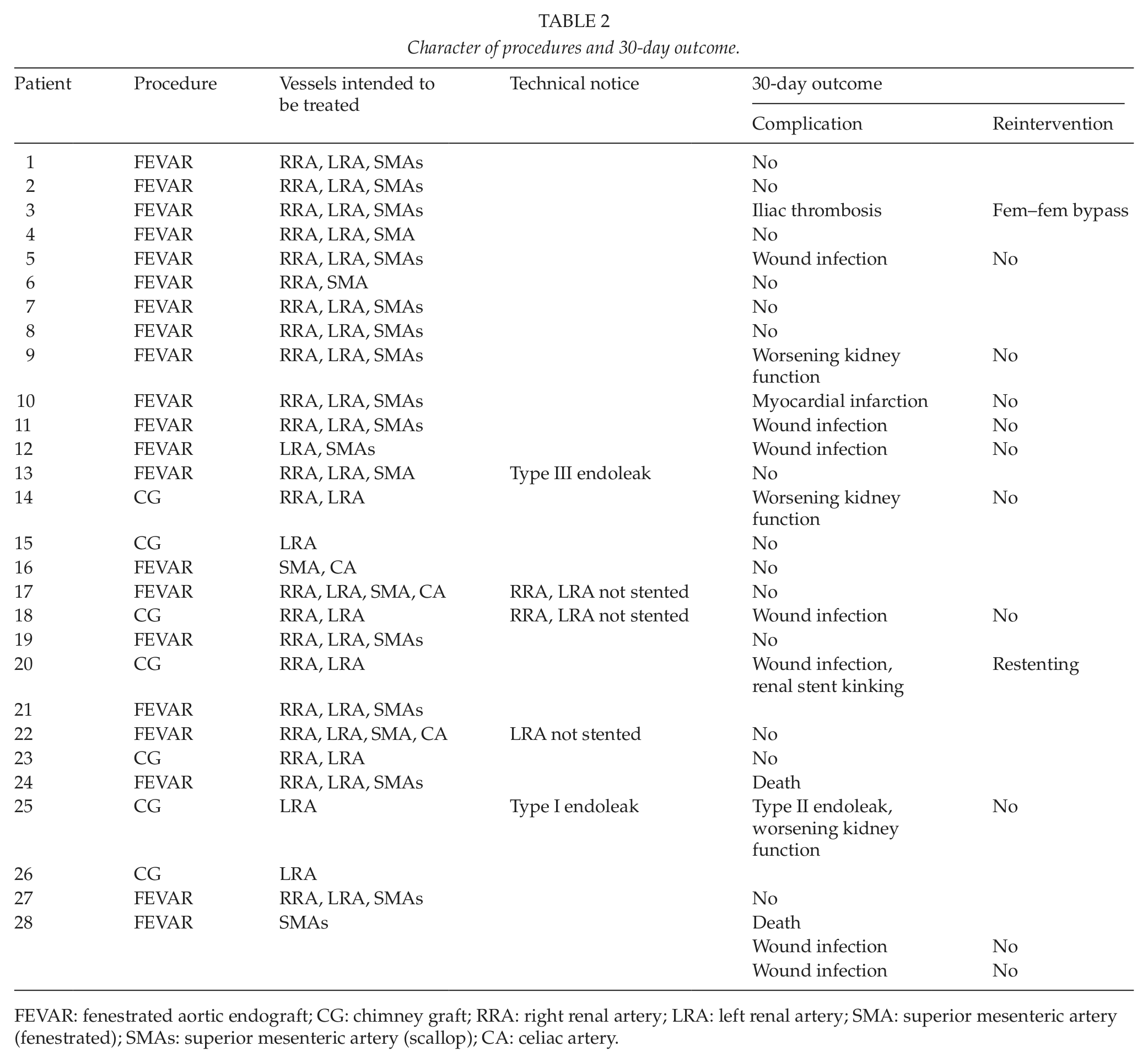
FEVAR: fenestrated aortic endograft; CG: chimney graft; RRA: right renal artery; LRA: left renal artery; SMA: superior mesenteric artery (fenestrated); SMAs: superior mesenteric artery (scallop); CA: celiac artery.
For the CGs, a bifurcated AAA endograft was used in six patients and a tube thoracic endograft in one patient (pseudoaneurysm after end-to-side aortobifemoral reconstruction). For three patients, the intention was to treat only one (patent) renal artery.
Procedure
The mean procedure duration was 213 min (SD = 67 min, range: 118–351 min), including a median fluoroscopy time of 71 min (range: 43–189 min). The mean amount of contrast media used was 267 mL (SD = 80 mL, range: 120–465 mL), and the median perioperative blood loss was 425 mL (range: 100–2200 mL).
A total of 63 (mean = 2.3/patient) visceral arteries were incorporated (42 renal, 21 SMA). In three patients, the intended stenting of the branched vessels proved unsuccessful: in one FEVAR patient with a complex graft (three fenestrations and a scallop), neither of the renal arteries could be stented, and in another FEVAR patient, cannulation of the left renal artery could not be performed. In one chimney patient (pseudoaneurysm), the cannulation of both renal arteries failed due to the very steep neck angulation, and only tube thoracic endograft was placed with a good completion angiography result. All of the aforementioned vessels remained patent. In two patients, however, the completion angiography showed endoleak—one with proximal type I and the other with type III endoleak (from bridging renal stent)—and the overall primary technical success rate (excision of AAA and no target vessel occlusion) was therefore 93% (26/28 patients). No immediate or late conversion was required.
Early Postoperative Outcomes
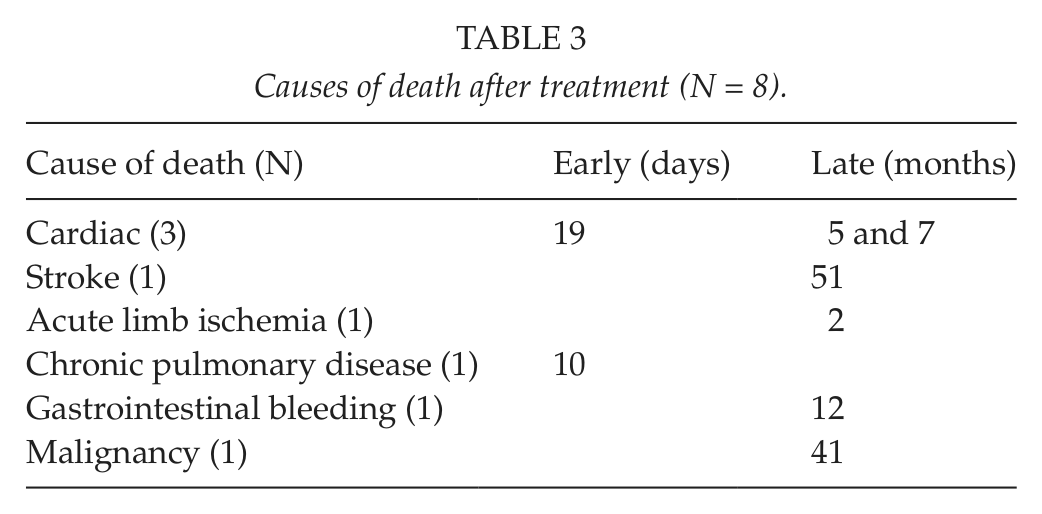
The in-hospital mortality was 0%. Two patients (7.2%), however, died after discharge but within 30 days after the procedure: one of acute myocardial infarction (patient with primary type I endoleak) and the other of pneumonia (Table 3). An additional patient suffered a nonlethal postoperative acute myocardial infarction. Seven patients (25%) developed a superficial groin wound infection, all of which resolved with antibiotic therapy only. One patient developed acute iliac artery thrombosis, which was treated with femorofemoral bypass and later, as the other limb also thrombosed, with axillobifemoral bypass.
Causes of death after treatment (N = 8).
At the 1-month follow-up, renal artery stent kinking was detected in one patient (CG) and was treated with an uncovered stent a few days later. Four patients (15%) suffered from significant deterioration in kidney function after the operation but without the need for hemodialysis.
Midterm Outcomes
The mean follow-up was 22 months (SD = 14 months, range: 1–46 months). Two-year follow-up CT was available for 18 patients. Six patients (23%) died during the follow-up, none of them of AAA rupture. One of the deaths occurred after reintervention to treat stent graft–related acute limb ischemia. The total aneurysm-related mortality rate in our series (including aforementioned two postoperative deaths) is thus 11%. The causes and times of death are summarized in Table 3. The overall cumulative survival at 1 year was 81% and at 2 years 64% (the cumulative survival for FEVAR patients at 1 year was 85% and at 2 years 75%; for CG patients, the rate was 57% at 1 year). The attempt to treat type III endoleak was unsuccessful and resulted in thrombosis of the renal stent together with the loss of the target vessel. This, fortunately, managed the endoleak without significant worsening of kidney function. One late type II endoleak remains under surveillance, as no aneurysm sac enlargement has been noted. The patient with unsuccessful cannulation of both renal arteries during the initial procedure later developed type I endoleak. Despite repeated efforts (three procedures), the problem could not be solved. This patient later died of gastrointestinal bleeding 12 months after the FEVAR procedure. Reinterventions (early or late) were thus required in 4 of 26 patients (15%).
Discussion
According to our results, the treatment of JAA is feasible by exploiting various endovascular techniques. The primary technical success rate of 93% is in line with previous results (4, 13, 15–17). The early (30-day) mortality rate was somewhat higher compared to other contemporary series. The difference can probably be explained by the rather small sample size of the current cohort and by the fact that fenestrated and chimney cases were analyzed together (4, 15–17). The present late survival rate and the number of additional secondary procedures did not substantially differ from earlier studies (15–18).
Although fenestrated endografts have been available for over a decade and the concept of chimney grafting was introduced almost 10 years ago, the number of procedures per unit still remains low, with the exception of a few centers (7, 18). This probably reflects the true low incidence of JAA, which is estimated to account for approximately 15% of AAAs (6). Another factor that may restrict the use of more complex endografts is the fact that, to date, there is no generally accepted definition for JAA (7, 15). Therefore, patients who might actually benefit from more sophisticated grafts are still treated with conventional devices. The costs related to the treatment are also substantial and may limit the use of newer technologies. In Finland, for example, the price of a fenestrated device is currently some €20,000.
The technical success of endovascular aneurysm treatment is usually defined as a complete exclusion of the aneurysm sac during the procedure (7, 15–18). TVP is another determinant of success when treating JAAs. The overall primary success is reported to be roughly 95% for both fenestrated and CGs (4, 13, 15–18). Types I and III endoleaks, that is, inadequate aneurysm exclusion, seem to be slightly more common than target vessel occlusion (7). Furthermore, according to the available literature, primary conversion is a rare phenomenon (15–18). The current results confirm these earlier findings.
Despite major comorbidities among patients treated for JAA, they seem to tolerate the operative stress well as operative mortality rate is 0% in most published series (7, 15–18). Early or in-hospital (<30-day) mortality for fenestrated procedures is reported to be 1%–3% and for chimney grafting 4%–12.5% (7, 18). In the current series, both early deaths occurred in the chimney group, resulting in an early death rate of 28%. This is unacceptable and requires a thorough review of the cases and more careful patient selection in the future. Advanced age and higher prevalence of both cardiovascular and respiratory diseases in the chimney group could explain the high early mortality. No long-term results of endovascular JAA treatment exist. The longest reported follow-ups for fenestrated grafts are 20 months and for chimney procedures less than a year (15–18). In our series, the mean follow-up for fenestrated grafts was 28 months and for CG 16 months. The late mortality rate for FEVAR cases was 24% and cumulative survival rates at 1 and 2 years 85% and 75%, respectively. The cumulative 1-year survival for CG was 57%. The causes of late deaths in our series, like in previous articles, seem to be related to the patients’ comorbidities rather than AAA rupture (Table 3) (15, 16). The patient who died of gastrointestinal bleeding was recovering from septicemia due to Listeria and the bleeding was considered as a consequence of sepsis. However, as no autopsy was performed, the possibility of an aortoduodenal fistula cannot be ruled out completely.
As mentioned, TVP is one of the key determinants of successful endovascular aneurysm excision, and postoperative dialysis dependence reflects a failure in maintaining free renal perfusion. The rate of permanent dependence on dialysis after endovascular JAA treatment is reported to be some 1.5% (7). The incidence of transitory or permanent renal impairment without the need for dialysis is approximately 15%, regardless of the endovascular method used (15–17). The definition of chronic kidney disease preoperatively, however, is not always clearly stated in the published articles. In our series, the majority (90%) of patients had kidney damage of some degree preoperatively. Nevertheless, they seemed to tolerate the procedure well despite a considerable amount of contrast media as no immediate or early hemodialysis was required.
The reintervention rate is an indicator of successful endovascular AAA treatment in the long term. Our recent study on conventional endovascular AAA treatment showed a 76% reintervention-free survival at 7 years (19). Furthermore, according to the available literature, complications requiring reinterventions seem to occur in the beginning of the follow-up, and the incidence levels out as the follow-up continues (20, 21). According to a recent review, the reintervention rate for fenestrated endografts is roughly 15% (percentage of patients) at 1 year (7). In our series, the cumulative reintervention rate at 1 year was 10% for fenestrated and 25% for CGs.
EVAR is an established treatment option for infrarenal aortic aneurysms. With the introduction of fenestrated and branched techniques, treating more complex anatomies has become commonplace. The chimney technique was originally introduced as a bailout procedure for misplaced endografts (10). During the last decade, this method has also been utilized for JAAs with challenging anatomy (e.g. heavily angulated neck) and in emergency/urgent situations where delaying treatment has not been an option. The newly introduced off-the-shelf fenestrated stent graft may, however, reduce the need for the chimney technique in the future (22). Evidently, the cost of this new graft is substantial, and as only preliminary results exist, clinicians should not completely discard the chimney option from their repertoire as yet.
This study is affected by several limitations. First, this is a small cohort study of only 28 patients. This, however, probably reflects the true low incidence of JAA and, as mentioned, is most likely the reality in many other centers as well. Second, although we cannot produce exact numbers, patient selection may affect the results to some extent as occasional patients may have been offered an open reconstruction and some patients no treatment at all during the study. The duration of the follow-up, although longer than in most published series, is still short and therefore restricts far-reaching conclusions. The strengths of this study, on the contrary, include the systematic EVAR registry, the access to all available CT scans and plain abdominal X-rays for review, and, finally, the fact that the number of surgeons (2) and radiologists (1) responsible of EVAR planning and procedures is restricted to a minimum at our institution.
Conclusions
According to our results, the treatment of JAAs is feasible by exploiting various endovascular techniques. Even with a low volume of cases, good immediate and short-term results can be achieved, especially with the FEVAR technique. Long-term results are, however, required to fully appreciate the possibilities and pitfalls of these relatively new methods.