
Abstract
Background and Aim:
Operative treatment is often indicated in unstable pediatric diaphyseal forearm fractures. Recently minimally invasive reduction and elastic stable intramedullary nailing have been of increasing interest, instead of open reduction and internal fixation with plates. There are several disadvantages of metallic intramedullary implants, such as soft-tissue irritation and a risk of disturbing later imaging. Thus, they are generally removed in later operations. We aimed to develop a new technique to stabilize pediatric forearm fractures by the bioabsorbable intramedullary nailing.
Material and Methods:
We developed a new, two-stage mini-invasive surgical technique to stabilize the unstable diaphyseal fractures in children. The procedure is bioabsorbable elastic stable intramedullary nailing. Ultra-high-strength bioabsorbable intramedullary nails of poly(lactide-co-glycolide) were manufactured for our purpose. The material has been widely proven to be biocompatible and stable enough for fracture treatment as screws and pins. We have used the new technique in the unstable both-bone diaphyseal forearm fractures in children between the ages of 5 and 15 years. We report the technique and our clinical experience in the series of those three cases that have been followed up for at least 12 months. The present series has been randomized for the procedure instead for titanium elastic stable intramedullary nailing, and the series represents a part of ongoing randomized trial.
Results:
The reported cases operated by the new technique referred good union in the fractured bones and acceptable alignment in the follow-up. Removal of the implants was not required. No troubles with the procedure or implant per se were noticed, indicating good feasibility. One high-energy refracture occurred half year after the primary trauma. Traditional titanium implants were used to control the refracture.
Conclusions:
We report our preliminary experience of a new surgical mini-invasive procedure to stabilize the unstable pediatric forearm shaft fractures by bioabsorbable elastic stable intramedullary nailing. Our clinical experience suggests that the procedure combined with long-arm casting is feasible in treating the pediatric forearm fractures. The technique may bring benefits to handling these challenging fractures. The disadvantages of metallic implants may be avoided. In addition, removal of the implant will not be required. There was one refracture in the series, but it was due to new high-energy trauma. According to our understanding, it was not related to the type of former osteosynthesis. However, ignoring the good preliminary experience, still we do not have results of the superiority of the procedure over traditional elastic stable intramedullary nailing. Our ongoing randomized multicenter study is aimed to determine its long-term outcome against the present golden standard. Nevertheless, due to encouraging preliminary results, we see it necessary to report the technique.
Keywords
Background
The rate of pediatric forearm fractures is increasing (1, 2). Most cases can be treated by means of closed reduction and casting (3). Commonly, unacceptable reduction, an unstable fracture pattern, segmental fractures, an open fracture, loss of reduction, and compartment syndrome are considered as indications for surgical intervention in cases of diaphyseal fractures of the radius and ulna (4–6). Since the encouraging reports in the early 1980s, elastic stable intramedullary nailing (ESIN) has become a well-accepted surgical technique-of-choice for treatment of long-bone fractures in children and adolescents (7, 8).
There is no doubt that ESIN of forearm fractures is a safe, effective, and user-friendly technique with good outcome (9, 10). Compared to plate fixation, ESIN offers a much less invasive procedure, even if open reduction is needed. Removal of nails is also less invasive than removal of a plate. ESIN offers a number of advantages to both surgeon and patient (8). However, there are some problems when using metallic nails. They can cause stress shielding, pain, and local irritation (11, 12). The surface of a metallic device provides an attractive area for bacterial infection. Release of metal ions from the implants is also a potential toxicological risk in the case of long-term implantation. Soft tissue like the skin and tendons are commonly irritated by the tips of nails (7). In many pediatric trauma centers, metallic intramedullary nails are routinely removed later in reoperation, and loss of reduction after implant removal can occur (13).
We have developed a new bioabsorbable ESIN (BESIN) technique to stabilize diaphyseal forearm fractures in children and adolescents. The technique takes advantage of the use of bioabsorbable implants, and hence the known weakness relating to metallic implants are avoided. In preclinical works, bioabsorbable implants have been strong enough to be used for intramedullary nailing of femoral diaphyseal osteotomies in three animal species (14). Removal of the implant becomes unnecessary, and thus, there is no psychosocial stress and morbidity caused by an additional operation. This is also important from an economic point of view, as the incidence of ESIN in cases of forearm fractures is increasing rapidly (15–17). In this study, we describe the surgical procedure and report our preliminary clinical experience.
Technique
The Procedure
Our technique, BESIN, is a two-stage mini-invasive surgical procedure to perform osteosynthesis in the long bones by intramedullary nailing. The technique reminds the one used in intramedullary nailing with titanium alloy nails. However, there are major differences.
The procedure is performed under general anesthesia in the operation theater (OT). First, angulated or dislocated bone is reduced. We aim at closed reduction, but open reduction throughout a small incision is performed if needed. A tourniquet is not used. A minimal longitudinal incision is made dorsally in the distal part of the radius and laterally in the proximal part of the ulna. With a bone awl, an entry portal is made into the cortical bone. Then, an important step in the procedure is as follows: we perform temporary intramedullary fixation by using a commercial titanium elastic nail (TEN). In order to create a satisfactory space for the final implant, we ream the bone marrow canal by rotating the metallic bent tip of the nail. Thus, the hooked tip of the TEN is used not only to drive the nail over the fracture line but also to achieve extra space in the bone marrow. The metallic implant is not disposable—we have prepared a forearm-fracture fixation kit that includes 2.0-, 2.5-, and 3.0-mm titanium nails as permanent instruments for reaming.
At the second stage, after achieving fracture reduction and having the titanium nails in their place, we replace the temporary titanium nails by the bioabsorbable nails one by one. The bioabsorbable intramedullary nails are introduced into the canals with the help of a device-specific nail inserter. There is no bent tip in the implant. Therefore, it is not possible to rotate or control the movement of the nail. Just light tapping is used instead when pushing it into the intramedullary channel. Only minor force should be needed in introducing the bioabsorbable nail into the canal, and reaming must be sufficient for that purpose. Osteosynthesis is perioperatively controlled by fluoroscopy. The nail in itself is not visible in radiography. However, an embedded bioabsorbable tricalcium phosphate X-ray marker is inserted in the tip of the nail. It makes it possible to monitor the position of the implant by using an image intensifier during the operation. Reduction must be held externally by an assistant during the time of replacement of the nails. One or both bones are treated; we prefer treating both bones. The nail is cut tangentially on the surface of the bone by using a hot wire device. After wound closure, a dorsal long-arm plaster cast with a volar support is made at the OT.
Owing to the hydrolytically activated memory effect of the implant material, the diameter of the material increases and the length decreases by 1%–2%, which may increase the stability of the fixation. However, immobilization will be required for 4–6 weeks. We prohibit sports for 2–6 months.
The Implant
We use the ultra-high-strength poly(lactide-co-glycolide) (PLGA) ActivaNail IM™ nails, which are designed for our purpose and manufactured by Bioretec Ltd., Tampere, Finland. There are nails of three thicknesses (2.0, 2.7, and 3.2 mm), and they all are 400 mm in length. They have been developed on the basis of the (trademarks blinded),™ which are bioabsorbable devices widely used in trauma surgery in different indications (18). The material of the implant has been shown to be safe in medical use. Since the first operations in 2007 in the United States and globally, about 25,000–30,000 patients have been operated with these implants. To our knowledge, only one adverse event report exists in Europe, and none has been made via the Food and Drug Administration (FDA) Maude-database so far. Nevertheless, both polylactide and polyglycolide have been found to be biocompatible in preclinical works in animals (19).
Preclinical testing of our implant was not required. However, we performed a risk analysis according to ISO standard 14971:200 for the study. In the analysis, the risk that the implant in question would cause any bioincompatibility reactions in this indication was negligible.
According to national regulations, the study plan was processed by Hospital Ethics Committee in every involved center of this multicenter study with acceptance. National Supervisory Authority for Welfare and Health (name blinded) approved the implant for use in this study, too. The participation in this clinical investigation has been voluntary, and the subjects have had a possibility to interrupt the participation at any time. Signed informed consents are required for inclusion.
Clinical Experience
We have performed BESIN for diaphyseal forearm fractures in children and adolescents (5–15 years old) in four pediatric trauma centers in our country so far. Indications for BESIN have been comparable to those for ESIN in these fractures. Patients with open fractures with significant soft-tissue injury and pathological fractures and patients with severe general malaise have been excluded from the procedure. This series includes three foremost cases with displaced fractures that have been followed up at least for 12 months.
Case 1
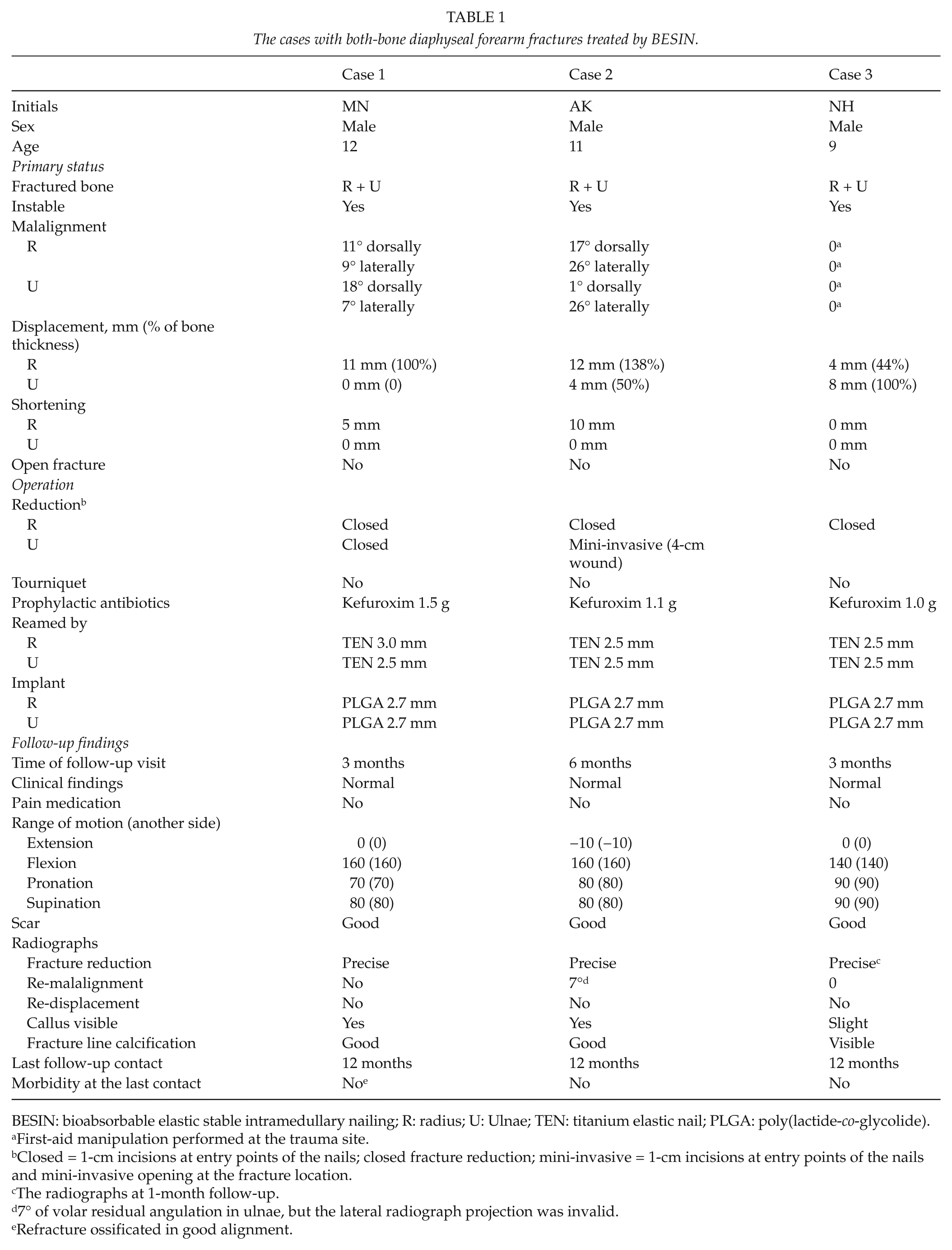
A 12-year-old boy fell when driving an all-terrain vehicle. He was found to have diaphyseal both-bone left forearm fractures. Malalignment was seen in both the bones and displacement and shortening in radius (Fig. 1A, B). Dorsal displacement of radius was 100% of the bone thickness (Table 1). Closed reduction was successful. The bones were internally fixed by BESIN. The tricalcium phosphate tips of the nails revealed suitable positions away from the fracture line. Postoperatively, at 4 weeks of follow-up, radiography illustrated good alignment of both radius and ulna. Union was completed and correct alignment was seen 3 months after the operation (Fig. 1C, D). The patient was symptomless and there was no restriction of the range of motion.

Case 1: An unstable forearm fracture in a 12-year-old boy. A) Primary anteroposterior (AP). B) Primary lateral view. C) AP view after 3 months with good bone healing. D) Lateral view after 3 months. E) A high-energy roller-skate trauma occurred 6 months later, and refracture was seen in AP. F) In lateral view.
The cases with both-bone diaphyseal forearm fractures treated by BESIN.
BESIN: bioabsorbable elastic stable intramedullary nailing; R: radius; U: Ulnae; TEN: titanium elastic nail; PLGA: poly(lactide-co-glycolide).
First-aid manipulation performed at the trauma site.
Closed = 1-cm incisions at entry points of the nails; closed fracture reduction; mini-invasive = 1-cm incisions at entry points of the nails and mini-invasive opening at the fracture location.
The radiographs at 1-month follow-up.
7° of volar residual angulation in ulnae, but the lateral radiograph projection was invalid.
Refracture ossificated in good alignment.
Unfortunately, 6 months postoperatively, the patient fell with high energy when roller-skating. Refracture in the radius was noticed (Fig. 1E, F). New operation was necessary. Closed reduction was unsuccessful, and a mini-invasive incision was made dorsally over the fracture. The fracture was new in inspection without any sign of pseudoarthrosis. The bioabsorbable nail was not removable as whole. Therefore, the intramedullary cavity was reamed open through the wound in both directions by a 2.0-mm Kirschner wire. TEN was inserted intramedullary retrogradially from the distal zone of the radius. In the follow-up, refracture healed with good union without a complication. The nail was electively removed 3 months later. There was no morbidity left 12 months after the primary operation.
Case 2
A 11-year-old boy was practicing gymnastic under supervision. He suffered fracture of the right forearm (Fig. 2A, B) with malalignment and displacement. Closed reduction and BESIN was performed in radius. Open mini-invasive reduction through a 4-cm dorsal incision was needed in ulnae. BESIN was then successful. Postoperatively, at 4 weeks of follow-up, there was good alignment in both the bones. In follow-up visits, the subjective result was excellent. After 6 months of follow-up, range of motion in the forearm was similar to that on the left. Radiographic bony healing was near to complete. Alignment was good in the anteroposterior radiograph. The lateral radiograph was defective as the elbow was captured in AP direction and the wrist in lateral direction. Therefore, 7° of residual volar angular deformity of the ulna is uncertain (Fig. 2C, D). There was no symptom left 12 months after the trauma.
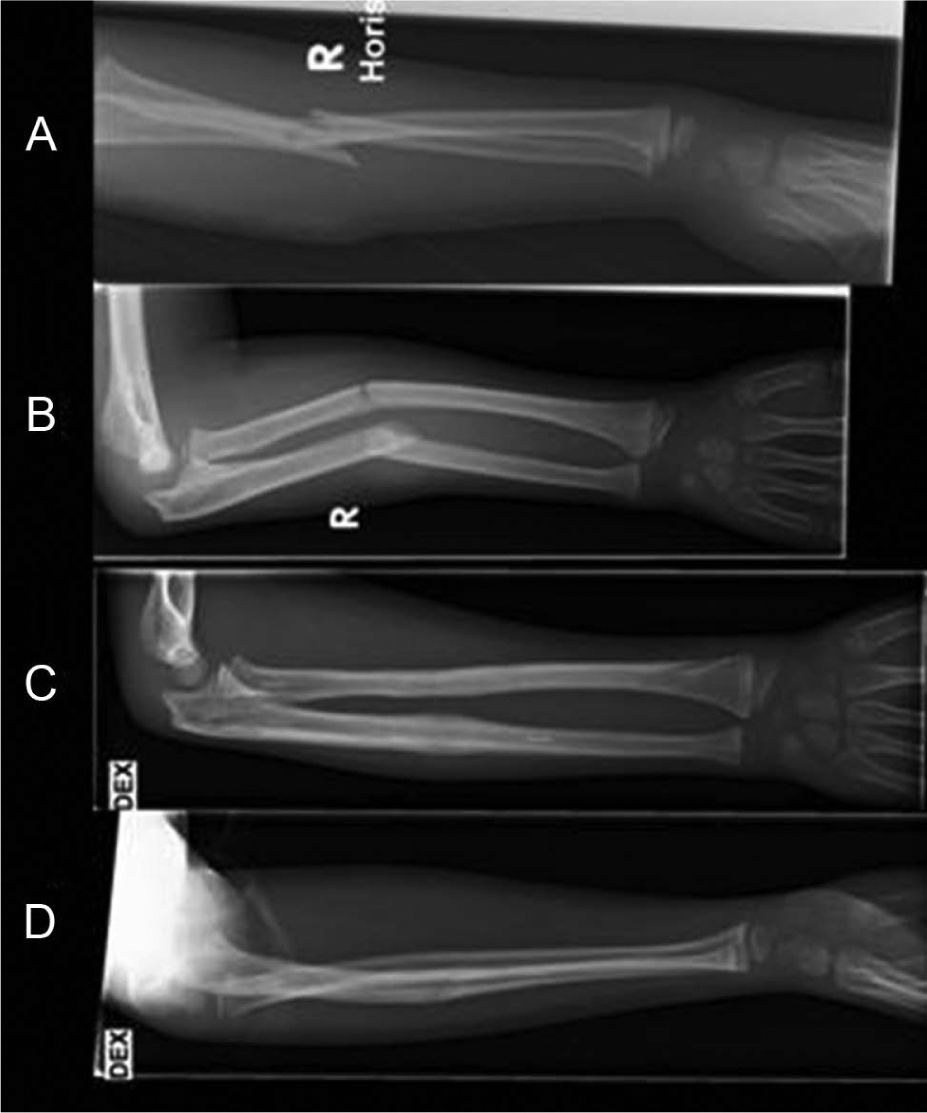
CASE 2: A 11-year-old boy with unstable diaphyseal forearm fracture. A) Primary radiographs in anteroposterior (AP) view. B) In lateral view. C) Radiographs show a good bone healing at 6 months of follow-up in AP view. D) Slight residual angular deformity up to 7° was seen in ulna, but the lateral projection was unsatisfactory.
Case 3
A 9-year-old boy fell when jumping on a trampoline. His father noticed a terrifying visible angular deformity, and he manipulated the forearm straight ex tempore beside the trampoline. An unstable diaphyseal both-bone fracture was found in radiographs at the trauma center (Fig. 3A, B). Urgent operation was performed and closed reduction was successful. Stabilization was achieved by BESIN using 2.7-mm PLGA nails. Postoperative radiographs were good. The extremity was symptomless 1 month after the operation. Range of motion was satisfactory in all directions. The radiographs showed good alignment (Fig. 3C, D). Bone healing was followed by magnetic resonance imaging (MRI) 6 months postoperatively. Uniform callus was seen in both bones (Fig. 3E, F). Edema in the bones and the surrounding soft tissues was slight referring to normal bone healing. No symptoms or complications existed 12 months after the fracture.
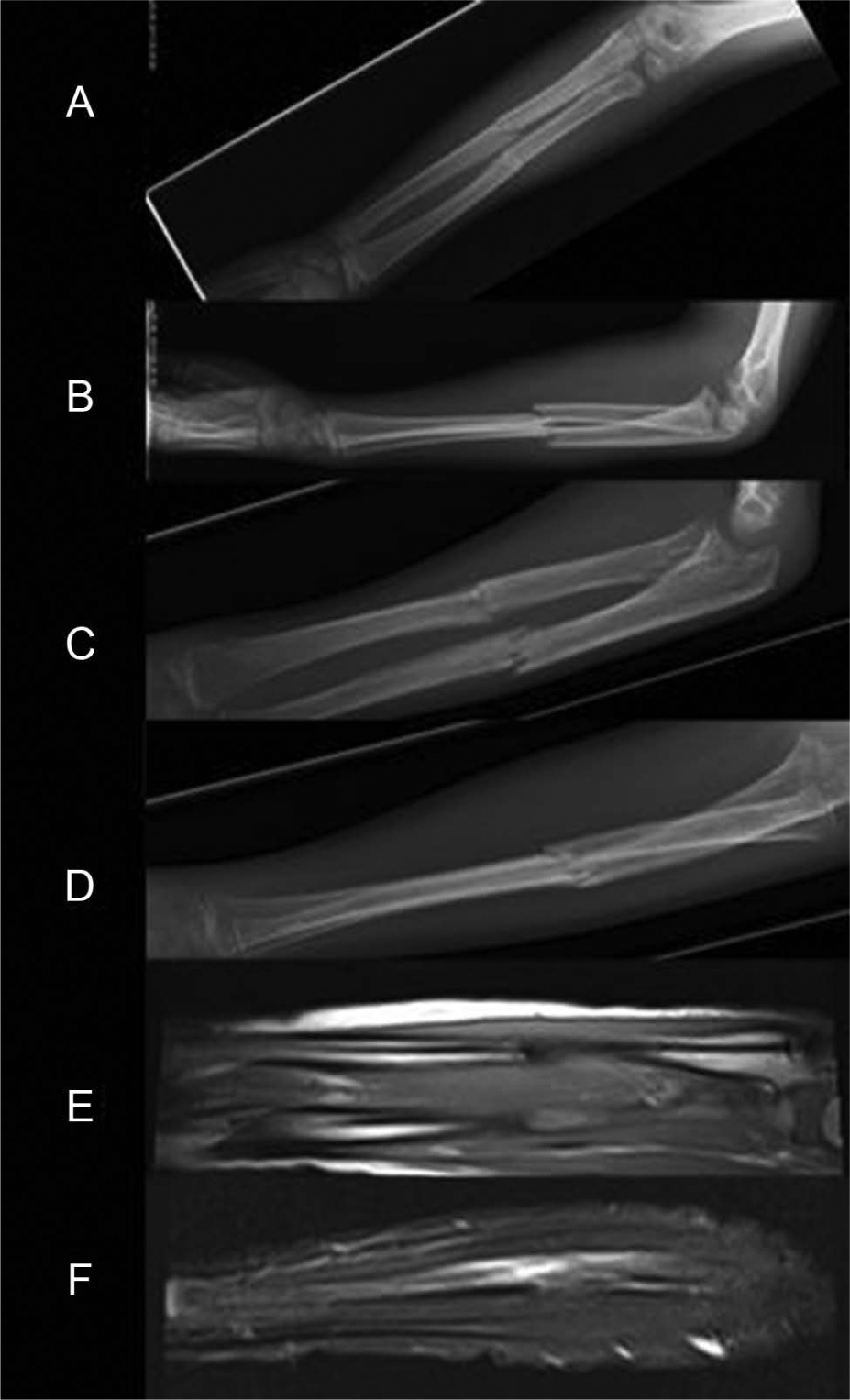
Case 3: The primary radiographs of a 9-year-old boy after falling at trampoline. A) Anteroposterior (AP) view. B) Lateral view. C) Radiograph showed good alignment in AP view 1 month later. D) The lateral projection is unsatisfactory after 1 month. E, F) Magnetic resonance imaging was performed in order to get additional information about the bone healing and soft-tissue reactions after 6 months. Slight edema in the bone and the surrounding tissues was visible as usual in posttraumatic stage. Alignment was good.
Discussion
We reported a new technique (BESIN) in treating displaced pediatric forearm fractures. Our preliminary clinical experience of the technique is encouraging. The feasibility of the procedure seems promising. There is increasing interest in ESIN in cases of pediatric forearm fractures (20). Intramedullary nailing offers indisputable benefits in special situations for both patient and surgeon. We hypothesize that most of the known benefits of intramedullary nailing are also available in connection with our procedure. There is already wide experience in the use of bioabsorbable materials in surgery in other indications in children population as well.
There will be some further advantages in BESIN. In our technique bioabsorbable nails will not disturb later imaging of the forearm in computed tomography (CT) or MRI. Tissue reactions against metallic implants are avoided, and the tip of the nail will not irritate soft tissue because it is cut at the surface of the bone. Damage of a tendon is a known complication of metallic ESIN. In addition, disappearing nails will not disturb the natural bowing of the radius during the growth of a child (21). Although bioabsorbable implants may be more expensive than metallic implants, they are economic because later removal is unnecessary. In one of our institutes, for example, removal of intramedullary nails in a forearm costs approximately 1550€. This includes not only the direct costs in the hospital but also the productivity loss suffered by a parent (22).
We had a refracture 6 months postoperatively in a reported case. The fracture occurred due to high-energy trauma, and we do not assume it was dependent on the primary fixation technique. The comparable titanium nails should have been removed before the time of the new trauma. Refracture would have occurred despite the type of former treatment. On the contrary, we hypothesize that there may be fewer refractures in our technique because the implants disappear gradually over a long time, avoiding the stress-shielding phenomenon. Further studies are needed in this regard.
The refracture 6 months postoperatively was undesirable. Nevertheless, it became established that diaphyseal forearm refracture can be controlled by ESIN with titanium nails despite the former BESIN. In addition, we hypothesize it would be possible to perform a plate-and-screw fixation in a case of refracture despite the existing intramedullary PLGA implant, if needed.
A factual concern with regard to any trauma implant is a potential inflammation. If so, it would be hard to remove the bioabsorbable intramedullary nail. Nevertheless, being an unlikely complication, we still postulate that it would be optional to control the complication by reaming or drilling the intramedullary cavity open in two directions by means of opening the fracture line in the diaphysis and performing external fixation together with administering antimicrobial agents.
The preliminary feasibility of our technique in fixation of children’s forearm fractures was good in the series. There was no complication in relation to the surgical technique or material of the implant per se. We noticed no inflammatory responses, infections, or soft-tissue irritation postoperatively.
Despite the good preliminary experience, further studies are needed to analyze feasibility and the long-term outcome and complications of the technique. Randomized ongoing clinical trial (RCT) is obligatory to obtain evidence-based support for BESIN versus titanium ESIN, which is the present treatment-of-choice. We hypothesize that our procedure may bring benefits or even change the traditional methods to handle pediatric forearm fractures.
Footnotes
Acknowledgements
We thank The Finnish Society of Paediatric Surgeons and The Alma and K. A. Snellman Foundation for supporting the study. We also thank Anna-Maija Haltia M.Sc., employed by Bioretec Ltd., which manufactured and provided the implants for this purpose.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.