
Abstract
Background and Aims:
The World Health Organization’s surgical safety checklist is designed to improve adherence to operating room safety standards, and its use has been shown to reduce complications among surgical patients. The objective of our study was to assess the impact of the implementation of the checklist on safety-related issues in the operating room and on postoperative adverse events in neurosurgery.
Material and Methods:
From structured questionnaires delivered to operating room personnel, answers were analyzed to evaluate communication and safety-related issues during 89 and 73 neurosurgical operations before and after the checklist implementation, respectively. From the analyzed operations, 83 and 67 patients, respectively, were included in a retrospective analysis of electronic patient records to compare the length of hospital stay, reported adverse events, and readmissions. In addition, the consistency of operating room documentation and patient records was assessed.
Results and Conclusions:
Communication between the surgeon and the anesthesiologist was enhanced, and safety-related issues were better covered when the checklist was used. Unplanned readmissions fell from 25% to 10% after the checklist implementation (p = 0.02). Wound complications decreased from 19% to 8% (p = 0.04). The consistency of documentation of the diagnosis and the procedure improved. The use of the checklist improved safety-related performance and, contemporarily, reduced numbers of wound complications, and readmissions were observed.
Keywords
Introduction
The surgical safety checklist is part of the World Health Organization’s (WHO) “safe surgery saves lives challenge” to improve the safety of surgical care by ensuring adherence to proven standards (http://www.who.int/patientsafety/safesurgery/en/index.html). The 19-point checklist covers the most important safety-related items during the operation. In 3 years, it has spread all over the world, with over 4000 registered hospitals, of which nearly 1800 are active users.
Preoperative checklists and briefings have been reported to improve communication and teamwork in the operating room (OR) (1–6). Enhanced cooperation among OR personnel correlates with reduced postoperative complications (7–10) and mortality (9–11). Preoperative briefings also correlate with enhanced safety attitude (12). The quality of communication can be perceived differently by nurses and doctors (13), but with the use of the checklist, the communication failures are reduced (14).
In a pilot study accomplished in eight hospitals across the world, the surgical safety checklist improved compliance with standards and reduced morbidity and mortality (15). In that study consisting of more than 7500 noncardiac surgical patients, inpatient complications and death rate declined by one-third after the implementation of the checklist, especially the rate of surgical site infections and unplanned reoperations decreased (15). Subanalysis of urgent patients showed a decrease in complication rate by one-third, and the death rate declined by two-thirds (16). In contrast, in a British study on orthopedic patients, the use of the checklist did not have a significant effect on mortality, complication rate, surgical site infections, or reoperations (17).
To our knowledge, this is the first study in which the use and the effects of the surgical safety checklist are examined in neurosurgical patients. The aim of this study was to determine whether the use of the checklist has an impact on safety-related issues, including communication and teamwork in the OR, and the rates of adverse events, complications, unplanned readmissions, and the length of hospital stay.
Material and Methods
In 2009, the surgical safety checklist was implemented in four Finnish hospitals in a prospective pilot study: a structured multiple-choice questionnaire was directed to surgeons, anesthesiologists, and circulating nurses in consecutive operations during a 6-week period before and after the implementation of the surgical safety checklist. Between the two study periods, an interim of 2 weeks was held, during which the checklist was introduced to all surgical team members. The original checklist was translated with minor changes in order to suite Finnish OR environment. All original steps of the checklist were maintained. Participation in the study was voluntary in emergency operations. The results of the questionnaire study and a subanalysis in otorhinolaryngology on communication and attitudes of the personnel are reported elsewhere (14, 18).
Adverse events of neurosurgical patients operated in Turku University Hospital, who were the neurosurgical subgroup of the pilot study, were retrospectively analyzed from electronic patient records. Altogether 228 neurosurgical procedures were performed during the study period. Of these, the personnel answered the questionnaire in 162 procedures. The patients of these procedures were tracked down and included in adverse event analysis. Children were excluded. The operations included in the analysis were the first operations of each hospital stay. These criteria excluded three children and eight procedures of same patients. One procedure was excluded due to inadequate operation information. The total number of patients studied was 150: 83 before and 67 after the checklist implementation (Fig. 1).
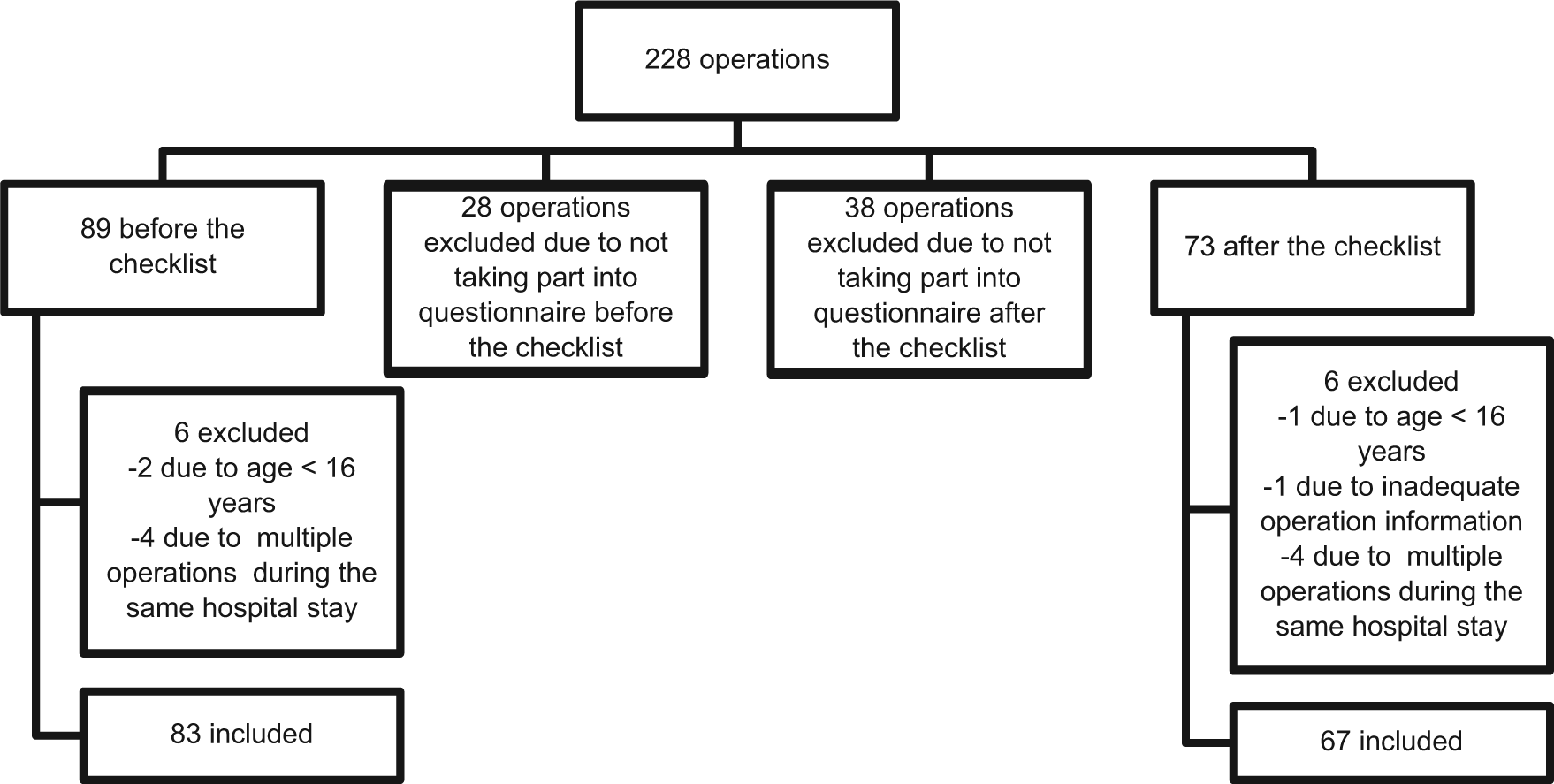
Exclusion and inclusion of neurosurgical patients into the adverse event analysis from the operations performed during the questionnaire pilot study period.
The length of hospital stay and predetermined adverse events were systematically collected from the electronic patient records. The durations of hospital stays and stays in the intensive care unit (ICU) postoperatively and time periods between the primary operation, unplanned reoperation, discharge, and unplanned readmission were monitored. The reason for an unplanned reoperation or readmission needed to be related to the primary operation in order to be included in the analysis. Furthermore, the electronic patient records were compared with the electronic OR records to assess the consistency and accuracy of recorded diagnoses and procedure codes.
After the primary operation, adverse events were monitored for 30 days, and after reoperation or readmission, the adverse events were monitored for 120 days. The monitored adverse events were stay in the ICU longer than 24 h; decreased level of consciousness longer than 24 h in the ICU; mechanical ventilation longer than 48 h; readmission to the ICU; unplanned reoperation; acute renal failure; sepsis; septic shock; systemic inflammatory response syndrome; myocardial infarction; pulmonary embolism; intracranial hemorrhage; cerebral infarction; meningitis; pneumonia; blood loss of 500 mL or more during the operation, or bleeding requiring the transfusion of at least four units of red blood cells; cardiac arrest requiring cardiopulmonary resuscitation; deep-vein thrombosis; wound disruption; surgical site infection; surgical site hematoma or seroma; cerebrospinal fluid (CSF) leakage from the wound; CSF deposit of the surgical site; pressure ulcer; peritonitis caused by shunt infection; paresis; urine retention; unplanned readmission; and death. Urinary tract infection was not considered as a complication. Diagnosed infections and suspected infections treated with antibiotics, excluding urinary tract infections and upper respiratory tract infections, were all monitored.
The study protocol was approved by the Ethical Committee of Hospital District of Southwest Finland and accepted by the Chief of Operative Group of Turku University Hospital, and the registry database was formed following national legislation in accordance with the ethical standards laid down in the 1964 Declaration of Helsinki.
The statistical analysis was performed with SPSS 17.0 for Windows. The normality of the distributions of the variables was tested with the Kolmogorov–Smirnov test. The significance of categorical variables was tested using the Pearson’s chi-square test, of normally distributed numerical variables (age) using the independent sample t-test, and of non-normally distributed numerical variables (durations and periods, average complication rate) using a nonparametric Mann–Whitney U-test. The significance of difference in type of operation was tested using the Kruskal–Wallis test. A p value less than 0.05 was considered statistically significant.
Results
Questionnaire Study
The statistically significant results of the questionnaire study are presented in Fig. 2. Missing answers were included in the analysis, representing 3%−16% of answers per question. When regarding the “yes” answers of all the answered questionnaires, the possible critical events during the operation were discussed more often after the checklist implementation according to both surgeons (“yes” answers 54% versus 71%, p < 0.001) and anesthesiologists (37% versus 59%, p = 0.008). The anesthesiologists confirmed the patient’s identity more frequently when the checklist was used, and the awareness of patient’s allergies and relevant medical condition improved. When the checklist was used, the anesthesia equipment was checked more frequently, and the surgeons’ opinion of other OR personnel’s awareness of the operation increased. The checklist did not improve significantly the confirmation of the sterility of instruments (98% versus 95%) or the checking of the availability of cross-matched blood products when a blood loss of over 500 mL was expected (54% versus 67%). The checklist did not change the awareness of the names and roles of each team members, the awareness of the procedure or the procedure side, or the giving of postoperative prescriptions or instructions, nor did it improve the perceptions of the successfulness of communication in the OR. The proper timing of the antibiotics failed both before and after the checklist implementation on average in every third operation (27% versus 37%).
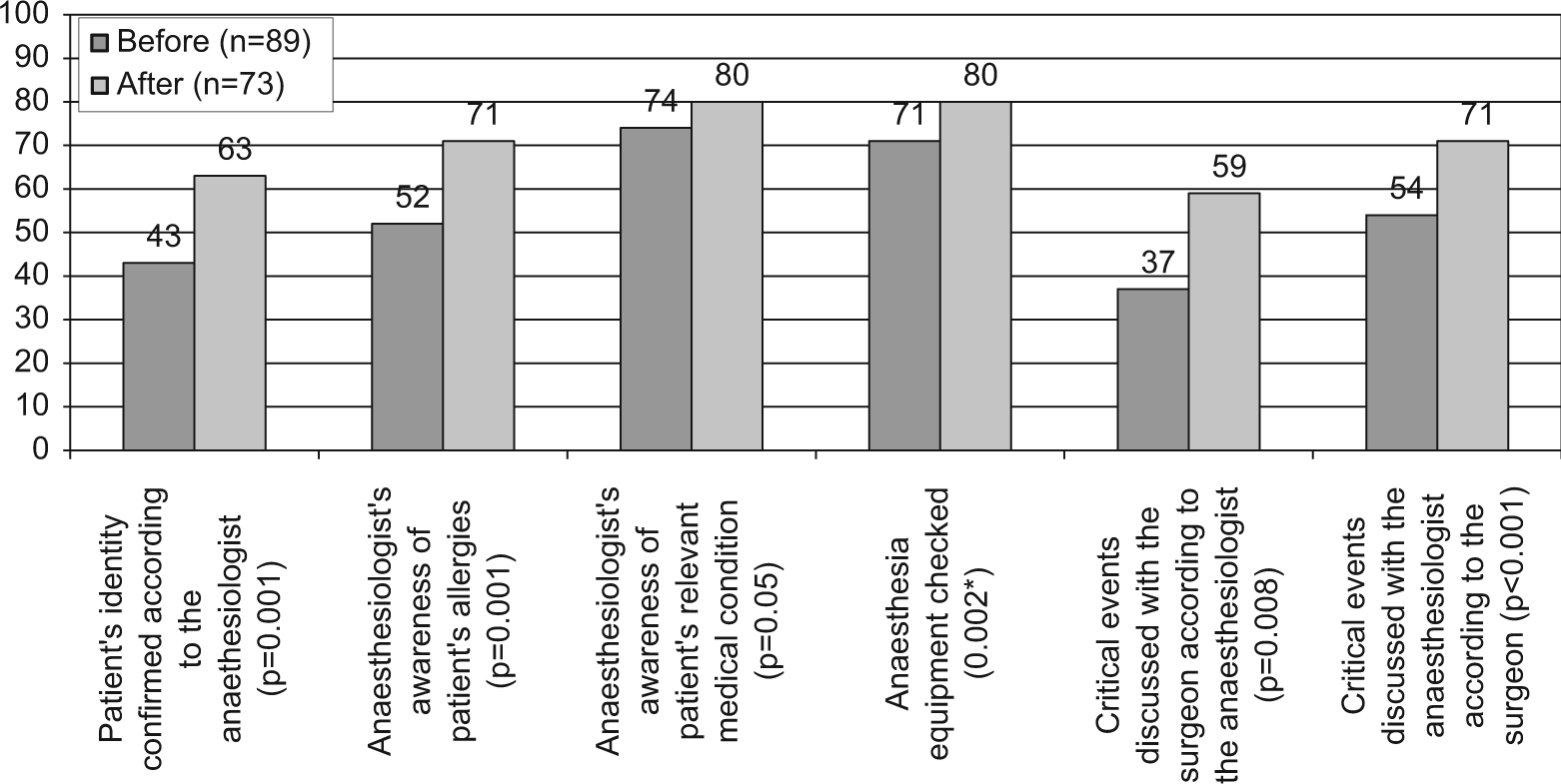
Percentage of anesthesiologists’ and surgeons’ “yes” answers in the questionnaire regarding safety-related issues in the operating room in neurosurgical operations.
Adverse Event Analysis
The demographics of the patients in the adverse event study are presented in Table 1. The neurosurgical diagnoses and procedures of the included patients are listed in Tables 2 and 3. During the first 6 weeks of the study period, that is, before the checklist, the number of patient days on the neurosurgical ward was 1165, and during the 6 weeks when the checklist was used it was 1061.
Demographics of the neurosurgical patients included in the adverse event analysis before (n = 83) and after (n = 67) the implementation of the checklist.
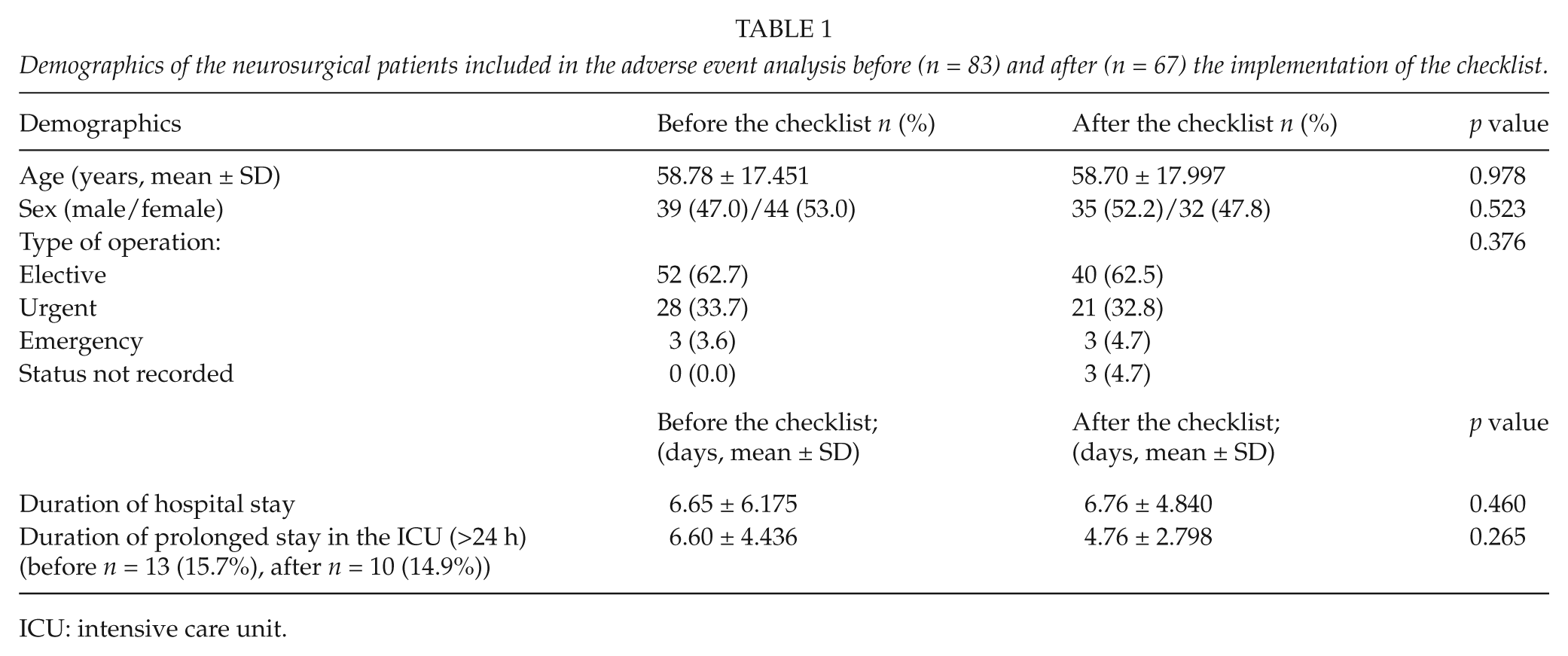
ICU: intensive care unit.
The diagnoses of the neurosurgical patients included in the adverse event analysis before (n = 83) and after (n = 67) the implementation of the checklist.
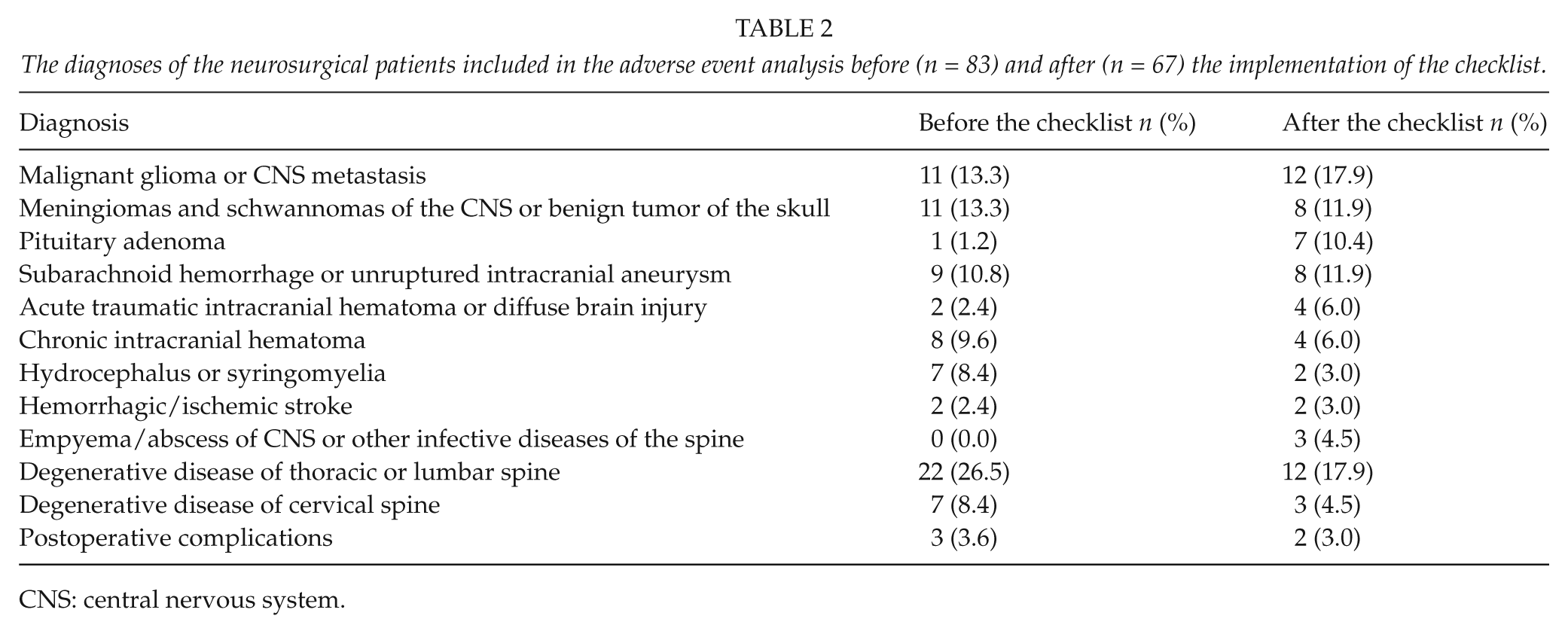
CNS: central nervous system.
The procedures of the neurosurgical patients included in the adverse event analysis before (n = 83) and after (n = 67) the implementation of the checklist.
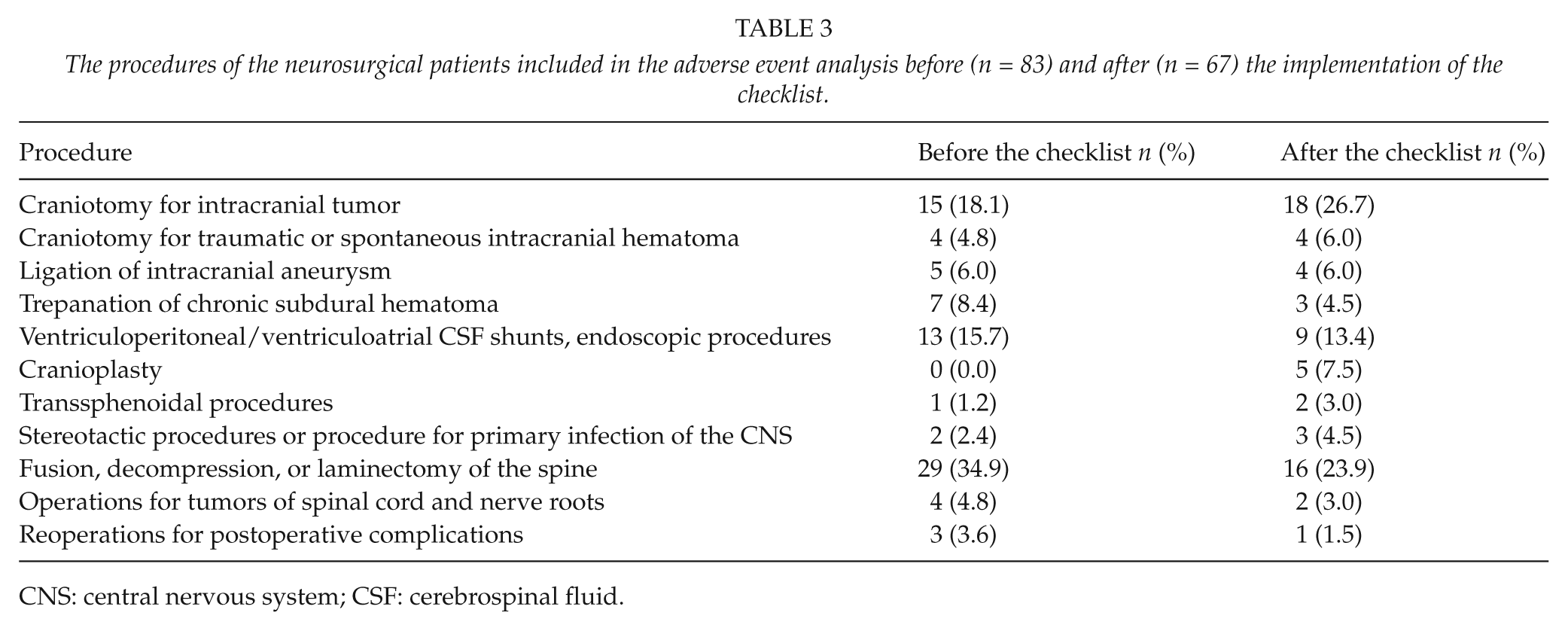
CNS: central nervous system; CSF: cerebrospinal fluid.
The rate of unplanned readmissions was 25% and 10% before and after the checklist implementation, respectively (p = 0.02). The readmissions consequent to the primary operation were 11% and 3%, respectively (p = 0.07). Number of patients with wound complications decreased from 19% to 8% (p = 0.04). The durations of hospital stays or stays in the ICU or the other recorded time periods did not show a statistically significant difference between the patient groups (Table 1). Table 4 presents the occurrence of recorded adverse events perioperatively and postoperatively.
Adverse events in neurosurgical patients included in the adverse event analysis before (n = 83) and after (n = 67) the implementation of the checklist.
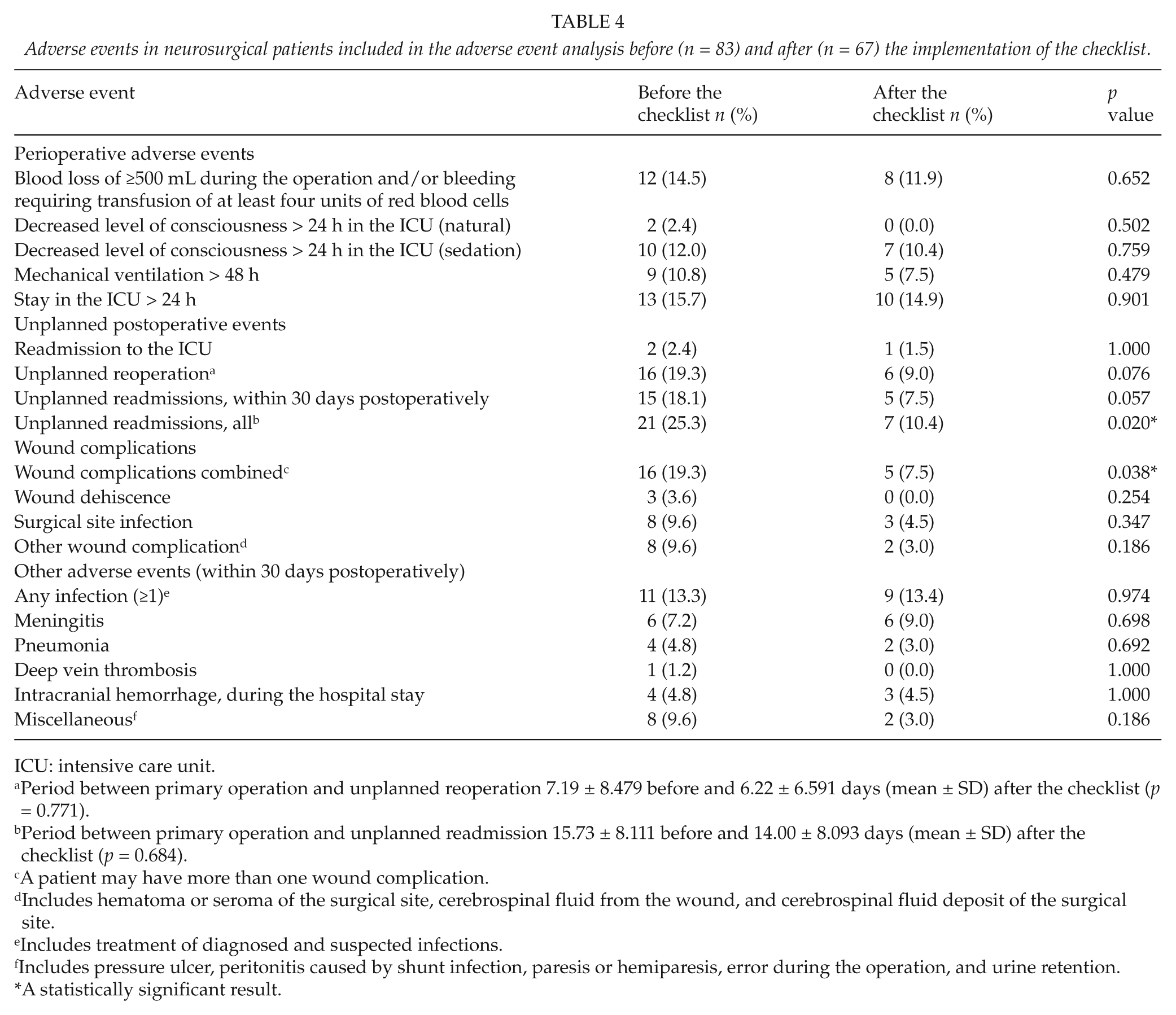
ICU: intensive care unit.
Period between primary operation and unplanned reoperation 7.19 ± 8.479 before and 6.22 ± 6.591 days (mean ± SD) after the checklist (p = 0.771).
Period between primary operation and unplanned readmission 15.73 ± 8.111 before and 14.00 ± 8.093 days (mean ± SD) after the checklist (p = 0.684).
A patient may have more than one wound complication.
Includes hematoma or seroma of the surgical site, cerebrospinal fluid from the wound, and cerebrospinal fluid deposit of the surgical site.
Includes treatment of diagnosed and suspected infections.
Includes pressure ulcer, peritonitis caused by shunt infection, paresis or hemiparesis, error during the operation, and urine retention.
A statistically significant result.
There were no events of acute renal failure, sepsis or septic shock, systemic inflammatory response syndrome, pulmonary embolism, myocardial infarction, or cardiac arrest requiring cardiopulmonary resuscitation in either of the patient groups. A total of 4 (5%) patients before the checklist implementation and 1 (2%) patient after the implementation had a stroke postoperatively. None of the deaths (2 patients before and 1 patient after the checklist implementation, respectively) were related to a recorded complication. The overall adverse event rate was 58% before and 46% after the checklist implementation (p = 0.16). On average, patients who had complications had 1.78 adverse events before and 1.25 adverse events after the checklist (p = 0.12).
The use of the checklist improved accuracy in the documentation of the diagnosis and the procedure of the operation. Before the checklist, the diagnoses recorded were missing or discordant in 33% of the cases, whereas with the checklist, there was a discrepancy between the two diagnosis records in 19% (p = 0.07). Between the procedure records, the discrepancy declined from 18% to 6% (p = 0.03), respectively.
Discussion
To our knowledge, this is the first study in which the use of the original WHO surgical safety checklist in neurosurgery is examined. The finding of our study was that the use of the checklist increased safety-related performance in the OR, and a contemporary adverse event analysis showed a reduction in wound complications and unplanned readmissions. Our overall results are in accordance with the studies of Haynes et al., where communication and teamwork improved (7) and complications declined (15) significantly by using the checklist.
The checklist enhanced the safety-related procedures and information transfer between team members. In particular, information transfer between the anesthesiologist and the surgeon improved. Understanding and paying attention to risks and preparing for them may reduce complications. Team members’ better awareness of the procedure may associate with less adverse events in major operations.
The wound complications in our study consisted of hematoma or seroma of the surgical site, CSF leakage from the wound, surgical site infection, or wound dehiscence. Wound complications cause a substantial risk for an unplanned readmission to the hospital. In our study, the reduction in the rate of unplanned readmissions was not only because of fewer wound complications, as only 43% of readmissions in both groups were due to wound complications. The majority of readmissions were due to other direct or indirect consequences of the operation, such as malfunction of the shunt, neurological symptoms, peritonitis caused by shunt infection, or the underlying disease process, such as hydrocephalus, transient ischemic attack, poor general condition, or pneumonia. These consequences are most likely due to patient’s disease and general condition and cannot be controlled by using the checklist. On average, half of the admissions and most of the readmissions before and after the implementation of the checklist, respectively, were treated in the neurosurgical ward. It is noteworthy that there was still a number of unplanned readmission later than 30 days postoperatively.
The findings in our study were in line with the study by Haynes et al., where the surgical site infections declined almost by half and unplanned reoperations by a quarter (15). In our study, the number of surgical site infections was 10% before and 5% (p = 0.347) after the checklist implementation, and unplanned reoperations 25% and 10% (p = 0.02), respectively. The average incidence rate of surgical site infections in neurosurgery is 4%, and two main risk factors are CSF leakage and a recent reoperation (19). In our study, only 3 patients before and 1 patient after the implementation of the checklist, respectively, had a CSF leakage from the wound. Before the implementation of the checklist, five reoperated patients had a surgical site infection. The reoperations were performed 8–28 days after the primary operations; two of the reoperations were wound revisions and one was a hematoma evacuation from the wound. Other explanations to the decreased rate of wound complications may be possible changes in wound dressing materials or ligatures or differences in the types of operations and operating risks in terms of infection. Overall, the surgical site infection rates were similar in our study and the study by Haynes et al. (15).
In our study, alternate explanations might be attributed to the decreasing wound infection rates. According to some studies, work overload, nurse understaffing, and work stress increase nosocomial infections (20, 21). Seasonal variations on the workload in the ward may have an impact on the surgical site infection rates. During the period before the checklist implementation, there were 9% more patient days on the neurosurgical ward than during the checklist period. Whether this difference was related to the use of the checklist or contributed to the adverse event rates remains unanswered.
According to some studies on surgical site infections in neurosurgery, there is no direct correlation between prophylactic antibiotics and surgical site infections (19, 22). In contrast, other studies have shown that antibiotic prophylaxis does significantly reduce surgical site infections after craniotomy (23 –25). It has been demonstrated that a checklist improves the timing of prophylactic antibiotics (26 –28). In most of the operations of our study, both before and after the checklist implementation, the antibiotic prophylaxis was administered more than 1 h before the incision (data not shown), which is considered suboptimal. This systematic error was noticed and corrected after the study period. After this evaluation and guidance, the timing of antibiotic administration has improved. Further studies will be needed to determine both the effect of the checklist implementation on the timing of antibiotic prophylaxis in our neurosurgical unit and the proper antibiotic prophylaxis timing and surgical site infections.
There are some limitations to our study. The number of patients in our study was small, which may induce type II (β) error. The study population was selected through a survey on the implementation of the checklist, and the setting was not randomized. However, even randomization would have involved a risk of bias, as the personnel would have become familiarized with the checklist after the first operations. Furthermore, it is impossible to blind the use of the checklist, although blinding the analyst of patient records concerning the checklist might have increased objectivity. In our study, a researcher not involved in neurosurgical treatment performed the patient record analysis. It would also have been possible to collect data from a separate control group, but this kind of setting has different kinds of limitations. The types of operations were not equally distributed between the groups, which may have had some impact on the complication profiles. Only predetermined adverse events were taken into account, and for instance, upper respiratory tract infections or urinary tract infections were not considered in the study. Further studies will be needed to confirm our results in larger patient populations.
Conclusions
The implementation of the surgical safety checklist enhanced awareness of safety-related issues among OR personnel. At the same time, a decreased number of wound complications and fewer unplanned readmissions were noticed. These findings are in concordance with previous studies. Furthermore, the use of the checklist improved the accuracy of documentation. Further studies are required to more comprehensively assess the benefits of systematic safety checks in surgery.
Footnotes
Acknowledgements
To Karolina Peltomaa, Riitta Aaltonen, and Ari Katila for their contribution to the planning of the questionnaires and the data collection in the checklist implementation study.
Funding
Funding and financial support for this study came from the State Subsidy for University Hospitals, Turku University Hospital; from Special Governmental Subsidy for the Health Sciences Research in Finland assigned by the Hospital District of Southwest Finland; and from a personal research grant from the Finnish Medical Association.