
Abstract
Background and Aims:
Both cemented and uncemented hemiarthroplasties are acceptable methods for treating displaced femoral neck fractures. Cemented hemiarthroplasty has traditionally been recommended as being more safe and reliable. However, the cementing process carries a risk of fat embolism and cardiovascular problems. This study attempted to determine whether these complications can be avoided when using a modern uncemented stem.
Material and Methods:
We retrospectively compared 222 hip fracture patients treated with hemiarthroplasty in our hospital. A total of 100 of these patients were treated with a hydroxyapatite-coated uncemented hemiendoprosthesis (Bi-Metric BFx) and 122 patients with a cemented hemiendoprosthesis (Lubinus SPII). Information on mortality and complications during the first 18.7 months was retrieved from patient files.
Results and Conclusions:
Nine perioperative fat-embolic events were found in the cemented group and none in the uncemented group. During the initial hospital treatment, there were five deaths (4.1%) in the cemented group and one death (1%) in the uncemented group. There were significantly more perioperative fractures in the uncemented versus cemented group (7% versus 0.8%). We conclude that uncemented hemiarthroplasty is associated with more perioperative fractures than cemented hemiarthroplasty. However, perioperative cardiovascular disturbances may be less frequent with uncemented hemiarthroplasty, and early mortality may be lower with uncemented hemiarthroplasty.
Introduction
Hemiarthroplasty is the preferred method to treat displaced femoral neck fractures among elderly patients, although it is associated with a 10% incidence of reoperations (1–3). Several designs of hemiendoprostheses are currently in use. The stems may be modular or nonmodular, with a unipolar or bipolar head. Hemiendoprostheses can be implanted with or without bone cement. Cemented prostheses have been thought to ensure more rapid mobilization of the patients than uncemented prostheses (4). However, such conclusions are based on studies comparing nonmodular, older prosthetic designs, such as the Austin-Moore or Thompson stems (5–7). To our knowledge, there are four prospective randomized studies comparing modern, modular femoral stems (8–11). The results achieved using cemented and uncemented implants were comparable in these studies.
Severe cardiovascular disturbances may occur during the preparation of the femoral canal when using a cemented femoral stem (12). It has been shown that during the cementing process, fat and bone marrow contents may embolize to the lungs (13). The risk of fat embolism and its cardiac effects may be significantly reduced but not completely avoided when using an uncemented stem (14).
In our hospital, we use a noncemented modular stem as an alternative to the cemented stem in the treatment of hip fractures in elderly patients. Noncemented stems are offered to the most risky patients with cardiovascular diseases. During the years 2005–2006, we treated 222 hip fracture patients with either a cemented or a noncemented hemiarthroplasty. In this study, we reviewed these patients retrospectively to determine whether our policy is justifiable. Institutional approval was obtained for this retrospective study.
Material and Methods
A total of 222 hip fracture patients were treated with a hemiendoprosthesis during 2005–2006 in Kuopio University Hospital. All were included in this retrospective study. Medical records including anesthetic data were retrieved from the patient files. The medical records were again re-retrieved 12–24 months after the surgery (18.7 months in average). Postoperative X-rays were checked in order to identify periprosthetic fractures. Institutional permission for the use of human medical records was obtained.
During the study period, there were no institutional guidelines regarding the choice between cemented and noncemented stems. However, the noncemented stem was usually chosen for patients who had several cardiovascular risk factors.
A suspected fat-embolic event was defined as any of the following events: (1) any intraoperative drop in blood pressure of more than 30 mmHg occurring during or immediately after the implantation of the stem (including during cementing), (2) any unexplained drop in SaO2 of more than 5% occurring during or immediately after implantation of the stem, or (3) any unexplained cardiovascular disturbance occurring during or immediately after implantation of the stem that led to an increased medical attention perioperatively and postoperatively. The criteria chosen by us have also been used by others (15).
The time from admission to operation was noted. The approach was selected by the operating surgeon although the anterolateral approach was encouraged. When cemented stem was used, hydrogen peroxide was used to dry the femoral canal before cementing. A distal plug was used for cemented stems. The polymethyl-metacrylate cement with gentamycin (Palacos R+G; Heraeus Medical, Hanau, Germany) was used for cemented stems in all cases. Lubinus SPII stem (Link GmbH, Hamburg, Germany) was used as cemented stem and Bi-Metric Bfx stem (Biomet Inc, Warsaw, IN, USA) as uncemented stem in our patients.
Low-molecular-weight heparin (enoxaparin 40 mg once a day, started 6 h after the operation) was administered for antithrombotic prophylaxis in all patients for 3 weeks after surgery. Cefuroxime was used as a single-dose (3 g, iv) antibacterial prophylaxis and was given 30–60 min prior to incision.
A postoperative X-ray was taken the day after surgery. Patients were transferred to a ward in their own health center usually within the first few days after the operation (median: second postoperative day, range: day 1 to day 16).
No routine checkups are scheduled for patients receiving a hip hemiendoprosthesis in Kuopio University Hospital.
It is a regional policy that all surgical complications (excluding benign superficial wound infections) of operatively treated hip fracture patients are treated in Kuopio University Hospital. Our hospital is also only one admitting acute orthopedic trauma patients in the area. Therefore, we assume that we are aware of all surgical postoperative complications in these patients.
For the statistical analysis, a two-tailed Students’ t-test was used for continuous variables and a chi-square test for noncontinuous variables. The statistical analysis was conducted using SPSS version 17.0 (SPSS Inc., Chicago, IL, USA).
Results
The baseline patient characteristics are shown in Table 1. Patients treated with an uncemented hemiendoprosthesis tended to be older, had more comorbidities (reflected by a higher average American Society of Anesthesiologists (ASA) Classification), were more often demented, and were less likely to live independently before the fracture. The average follow-up for both groups was 18.7 months.
Patient characteristics.
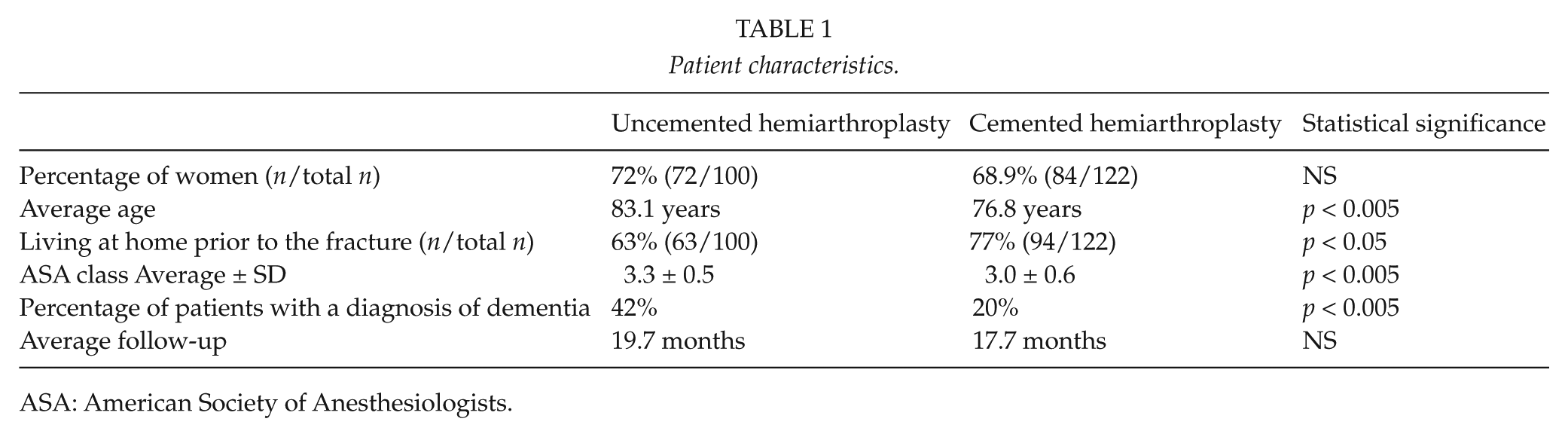
ASA: American Society of Anesthesiologists.
Operations were mainly performed by orthopedic residents in both groups (68% vs. 71%). There was no statistically significant difference in the approach used (anterolateral or posterolateral approach) or intraoperative bleeding between the groups. The operating time was longer when a cemented hemiendoprosthesis was used (p < 0.005; Table 2).
Operative details.
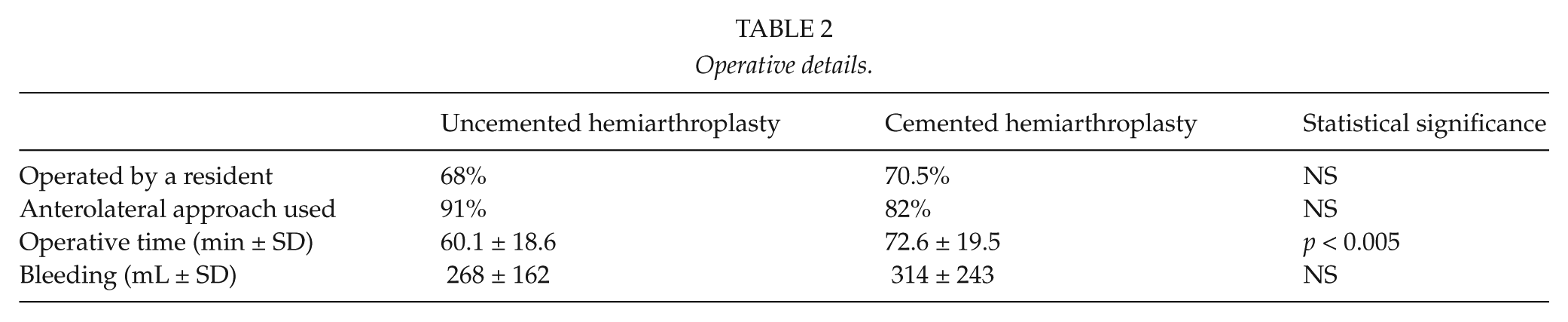
Table 3 shows that 1 of 100 (1%) of the patients in the noncemented group died during the initial hospitalization. There were five deaths (4.1%) in the group receiving a cemented stem. The difference was not statistically significant (Table 3). Autopsies were performed for all patients who died during the initial hospitalization. The cause of death of the patient in the noncemented group was coronary heart disease. In the cemented group, large fat emboli were found in one patient. The cause of death in another patient was large, acute myocardial infarct. The cause of death in the remaining three patients was coronary heart disease.
Mortality, cardiovascular parameters, and surgical complications in patients with femoral neck fracture.
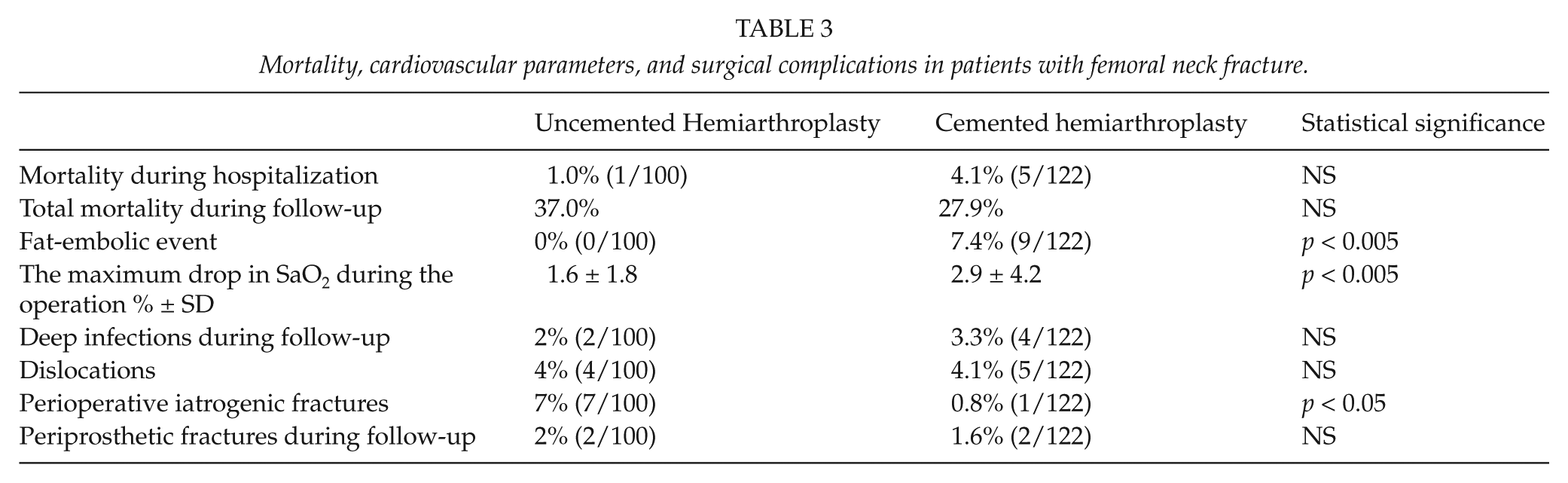
There were no suspected fat-embolic events in the noncemented group. There were nine (7.4%) such events in the cemented group. The difference was statistically significant (p < 0.005). The intraoperative drop in the SaO2 was more pronounced in the group receiving a cemented stem, suggesting less severe cardiorespiratory disturbances may also be more common when using a cemented stem (Table 3).
The occurrence of surgical complications is shown in Table 3. Dislocations were more common when the posterior approach was used compared with the Hardinge approach (9.7% versus 3.1%, p < 0.05). Iatrogenic perioperative fractures occurred more often when an uncemented stem was used. Perioperative iatrogenic fractures were all reparable with cables alone or cables and a trochanteric grip and healed well during the follow-up. The occurrence of periprosthetic fractures later in follow-up was similar in the two groups.
Discussion
Our study showed that the use of a cemented femoral stem was associated with more perioperative fat-embolic events (reductions in blood pressure and oxygen saturation) compared with the use of a noncemented stem. Although we did not monitor emboli directly by transesophageal endoscopy, our findings do have clinical relevance. There was a trend toward higher in-hospital mortality in the cemented group despite the fact that patients receiving a cemented stem tended to be younger and less fragile according to their prefracture residential status and lower ASA class. The patients in the group receiving a cemented stem who died in-hospital experienced an episode compatible with fat embolization during their operation. This suggests that the use of a cemented stem may increase the risk of perioperative death in hip fracture patients.
The strength of our study is the inclusion of all patients treated with a hemiendoprosthesis for a femoral neck fracture in the catchment area of our hospital during the study period. This was possible since our hospital is also the only one taking care of hip fracture patients in its catchment area. Another strength is that patients were treated by a number of surgeons, which reflects the situation in normal clinical practice. The main weakness is the retrospective nature of our study. However, we suggest that our study is warranted because there are only four prospective (8–11) studies comparing modern modular cemented and uncemented stems. Most studies comparing cemented stems with uncemented stems have been conducted using the traditional monoblock stems of Thompson and Austin-Moore design (4–7). It can be argued that stems with a modular design and contemporary instrumentation may produce different clinical outcomes. In a Swedish register study, the use of Austin-Moore design was clearly shown to be associated with more reoperations and complications compared with either cemented monoblock stems or modular newer stems (16). The popularity of monoblock stems has also decreased rapidly in Scandinavia (17), making it difficult to draw clinically relevant conclusions from older studies.
It has been shown that the cementing of a femoral stem is associated with the occurrence of fat embolism. Emboli may be reduced but not completely avoided by using copious lavage before cementing (18) or by using a rather extensive suction system and venting of the cortex intraoperatively (19). It is also known that some surgeons avoid pressurization of cement for fear of producing fat embolism. In elective hip arthroplasty, fat embolism has been suggested as a possible risk factor for early mortality (20), even though the number of deaths potentially related to the use of cement has been shown to be low (21). It can be argued that hip fracture patients are more fragile and “higher risk patients” for fat embolism than patients receiving an elective hip arthroplasty. Our patients’ ASA score was higher than 3 in both groups (Table 1).
We defined a fat-embolic event as cardiovascular disturbances occurring during or immediately after the implantation of the implant. We do not have direct data from transesophageal echocardiography, which is thought to be the most direct method of detecting intraoperative fat embolism (15). However, it has been shown that cementing produces a drop in cardiac output and stroke volume (14) that lead to the similar changes observed in our patients. Our definition for a fat-embolic event also closely resembles criteria proposed by others (12, 15).
The cause of death in our patients who died during the initial hospitalization was coronary heart disease in all but one patient. Indeed, fat emboli detected in the autopsy are relatively uncommon in patients dying early after hip arthroplasty (20). We believe that the well-documented cardiovascular events associated with cemented arthroplasty are the main pathophysiological mechanism behind the early postoperative deaths in our study.
In line with our results, Ahn and coworkers (22) noted a trend for increased risk of perioperative death with the use of cemented stems in their systematic review. The National Patient Safety Agency of the United Kingdom also produced a report in 2009 raising concern over perioperative deaths associated with the use of cement in hip fracture patients (23). In a subsequent database study, no increase in deaths after discharge was associated with cement use in hemiarthroplasty (24). Two other systematic reviews also failed to show an increase in perioperative mortality when cement was used, although these reviews were based on studies comparing older monoblock stems (25, 26). Based on our results and results from Australian Joint Replacement Registry (27), it seems that the possible risk of death associated with the use of cemented implant is confined to early postoperative and perioperative period.
More intraoperative fractures of the femur occurred in the noncemented group. This is in line with observations from systematic reviews (4), and the incidence was similar to that in another study comparing cemented and uncemented hemiarthroplasties (28). Intraoperative fractures are associated with the use of noncemented femoral stems and have been associated with female gender, suggesting osteoporosis may be an additional risk factor (29). Although there are no data comparing different uncemented femoral stems and the risk of intraoperative fractures, we have replaced the uncemented, proximal filling stem used in this study with a tapered stem in our hospital to reduce the unacceptable rate of iatrogenic fractures.
The rate of hip dislocation did not differ between the study groups. However, in agreement with the current literature (30), we detected more dislocations in the patients operated upon using the posterolateral approach. It has been shown that dislocations may be reduced by altering hospital policy to the uniform use of the anterolateral approach (31). After analyzing our results, we have also changed our policy and now use only the anterolateral approach.
A weakness of our study is the lack of information about patients’ pain and functional status during the follow-up. It has been suggested that the use of cemented stems results in better mobilization and less pain when compared with uncemented stems (4, 7). Studies comparing modern cemented and uncemented stems did not detect any difference in function (8–11). We think that despite the lack of information about functional status, our study has its value because there is no inclusion bias. A significant portion of hip fracture patients are demented and fragile patients not able to give informed consent and participate in extensive follow-up. These patients are likely to be dropped from prospective trials. In a recent prospective trial, over one-third of patients declined to participate in the study (10). In order to get a comprehensive picture about the results of hip fracture surgery, studies using different designs are therefore needed.
Conclusions
In conclusion, we found that perioperative cardiovascular disturbances occur when modular cemented stems are used in hip fracture patients. The use of an uncemented stem leads to a 7% incidence of perioperative iatrogenic fractures. It seems that by using uncemented modular stems, the cardiovascular disturbances can be reduced by a cost of perioperative fractures. More data comparing uncemented and cemented hemiarthroplasty in patients with femoral neck fracture are still needed.