
Abstract
Background and Aims:
Delayed or wrong diagnosis in patients with appendicitis can result in perforation and consequently increased morbidity and mortality. Serum bilirubin may be a useful marker for appendiceal perforation. The purpose of this systematic review was to evaluate studies investigating elevated serum bilirubin as a predictor for appendiceal perforation.
Material and Methods:
Medline, Embase, and Cochrane databases were searched for studies evaluating elevated bilirubin in the diagnosis of perforated appendicitis. Study selection criteria included English language papers evaluating serum bilirubin as a marker of appendiceal perforation in humans. A total of 189 abstracts were screened for eligibility, of which five clinical studies were included in this study.
Results:
Bilirubin was significantly higher in patients with appendiceal perforation compared with patients with appendicitis without perforation. Elevated serum bilirubin had a sensitivity ranging from 0.38 to 0.77 and a specificity ranging from 0.70 to 0.87 in predicting appendiceal perforation.
Conclusions:
Elevated serum bilirubin for determining the risk of perforation in appendicitis has low sensitivity but higher specificity. This measure can therefore be used as a supplement in the diagnostic process.
Background
Acute appendicitis is one of the most frequent surgical conditions, and the lifetime risk for appendectomy is estimated to be 12% for males and 23% for females (1). Acute uncomplicated appendicitis can be difficult to distinguish clinically from perforated appendicitis, especially in the elderly and in children (2, 3). Simple acute appendicitis can be a minor surgical procedure with limited complications; however, delayed diagnosis and subsequently appendiceal perforation can result in a potentially lethal condition (4). The mortality associated with simple acute appendicitis is reported to be 0.3% but increases to 6% in cases with perforation (5). Early diagnosis of appendiceal perforation is important to limit the associated abdominal sepsis. Moreover, where radiological modalities such as computed tomography (CT) scan and ultrasound (US) are effective in supplementing the diagnosis of acute appendicitis (6, 7), both modalities have lower sensitivity in detecting perforated appendicitis (8, 9). Development of supplementary tools besides clinical examination and radiology could be beneficial in the early diagnosis (5). Several studies have found bilirubin to be a useful serological marker for predicting acute appendicitis (10, 11) and appendiceal perforation (5, 11–14).
The purpose of this systematic review was to evaluate the current literature regarding elevated serum bilirubin as a diagnostic marker for appendiceal perforation.
Methods
Literature Search
Using the preferred reporting items for systematic reviews and meta-analysis (PRISMA) (15, 16) guidelines, a systematic literature search was performed in Medline (January 1966–February 2012), Embase (January 1980–February 2012), and Cochrane databases (April 1996 to February 2012). The aim of the search strategy was to identify human clinical studies evaluating serum bilirubin as a prognostic factor for appendiceal perforation. In Medline, the following search terms were used: ((appendix(MeSH Terms) OR appendix (All Fields)) OR (appendicitis (MeSH Terms) OR appendicitis (All Fields))) AND ((hyperbilirubinaemia (All Fields) OR hyperbilirubinaemia (MeSH Terms) OR hyperbilirubinemia (All Fields)) OR (hyperbilirubinemia (MeSH Terms) OR bilirubinemia (All Fields)) OR (jaundice (MeSH Terms) OR jaundice (All Fields)) OR (bilirubin (MeSH Terms) OR bilirubin (All Fields))). The Embase and Cochrane search used the multifield advanced search function with the same search terms.
Study Selection Criteria
Regarding language, only English language studies were included. Only original human studies on admitted patients with perforated appendicitis (histologically or surgically verified) and evaluating hyperbilirubinemia were included. The primary study outcome was evaluation of serum bilirubin as a diagnostic marker in acute perforated appendicitis compared with simple acute appendicitis without perforation. The outcome was measured either by absolute numeric values or by specific cutoff values and estimates of sensitivity, specificity, positive predictive value (PPV), and negative predictive value (NPV). Studies not evaluating bilirubin values and studies evaluating the use of elevated bilirubin for simple acute appendicitis compared with no appendicitis were not included. For details on specific study selection, see Fig. 1.
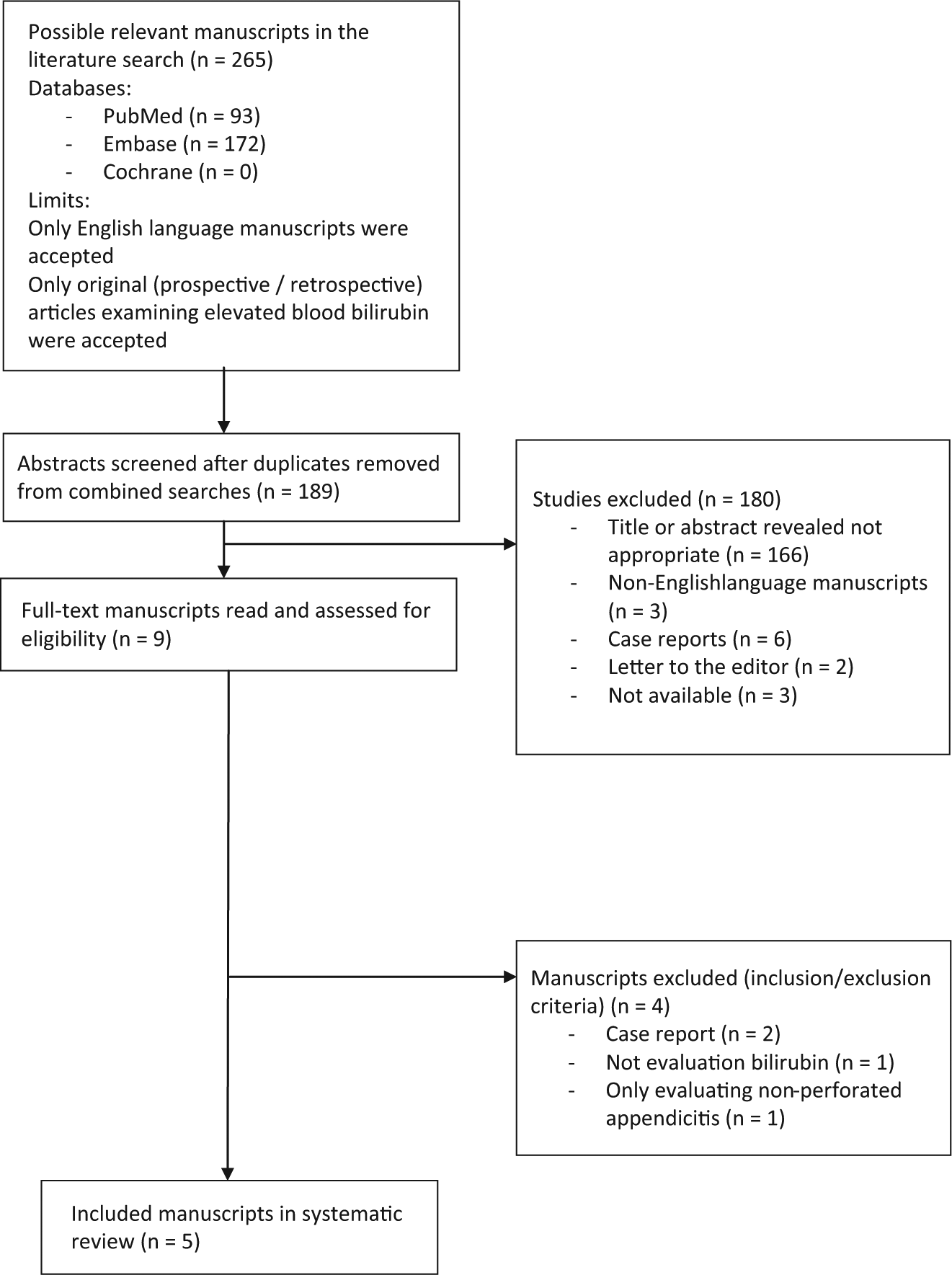
Flowchart of literature search and included studies.
Initial Abstract Screening And Full Text Assessment
Titles and abstracts were independently assessed for eligibility by two reviewers according to the selection criteria. Any uncertainties between the reviewers were settled by discussion. Full manuscripts were obtained and evaluated in detail from the studies assessed suitable for inclusion.
Data Extraction
Data extraction was performed on five studies. The following data were extracted: study aims, study design, patient material (number, subgroups, demographics), primary and secondary outcomes, bilirubin values, and conclusions. Data were extracted by both reviewers. Data were extracted directly from the studies; however, conversion of the volume of serum bilirubin into micromole per liter was performed in order to standardize the data (Table 1).
Studies included in the systematic review.
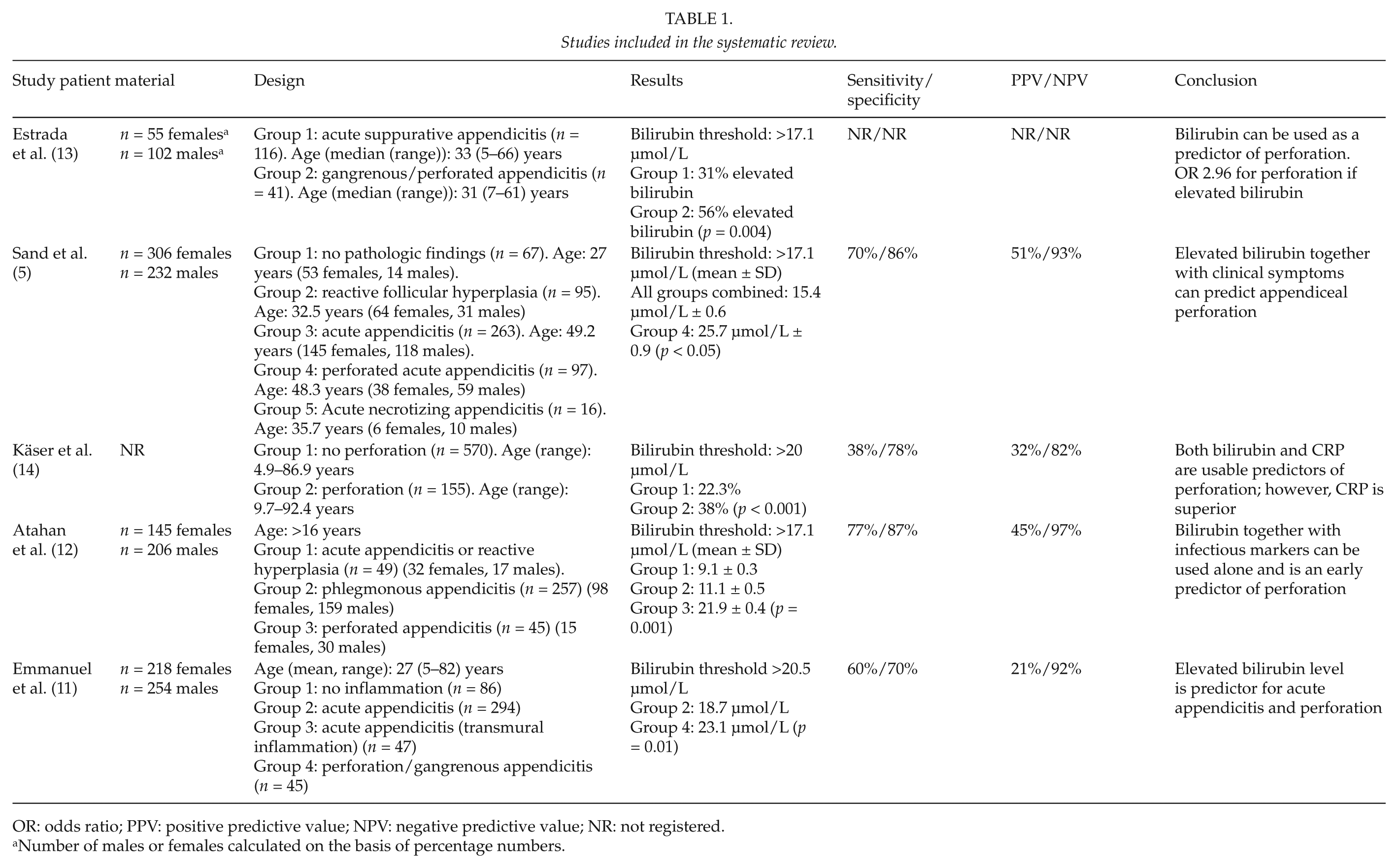
OR: odds ratio; PPV: positive predictive value; NPV: negative predictive value; NR: not registered.
Number of males or females calculated on the basis of percentage numbers.
Results
A total of 265 possible studies were identified, and after doublets were removed, the search strategy resulted in 189 possible studies for inclusion (Fig. 1). A total of 2243 patients were included in the five studies (Table 1). All studies were retrospective and descriptive in design. No healthy control group was used in any of the studies. All patients included were operated for appendicitis, which was verified by pathological examination; however, in two studies, a subgroup of the patients had pathologically normal appendices (5, 11).
The levels of bilirubin were compared between patients with perforated appendicitis and patients with simple appendicitis without perforation. There were significantly higher levels of serum bilirubin among patients with perforated appendicitis compared with patients without perforation with p values ranging from p = 0.01 to p < 0.001 (Table 1). In the included studies, serum bilirubin was measured as values either above certain threshold values (>17.1 or >20 µmol/L) or in absolute values. The mean serum bilirubin values for patients with perforated appendicitis ranged from 23.1 (11) to 25.7 µmol/L (5). The sensitivity for elevated bilirubin varied among the studies with threshold values. The sensitivity varied between 0.38 and 0.77 and the specificity varied from 0.70 to 0.87. NPVs were between 82% and 93%, and PPVs were between 21% and 51%.
Discussion
Serum bilirubin was significantly elevated in patients with perforated appendicitis compared with patients with simple acute appendicitis without perforation. In general, the patients with perforated appendicitis had mean serum bilirubin values ranging from 23 to 26 µmol/L (Table 1). Depending on the specific threshold values, the specificity was generally high. Moreover, NPV was high for elevated serum bilirubin, but PPV was generally low.
In the studies included in this review, C-reactive protein (CRP) and white blood cell (WBC) count have been evaluated as predictors for appendiceal perforation. It seems that CRP generally has a higher sensitivity but lower specificity compared with bilirubin (5, 11, 14). However, the sensitivity and specificity of CRP and bilirubin are determined by the threshold values. The optimal condition is a maximum value of sensitivity combined with a maximum value of specificity. Therefore, a threshold value has to be calculated from the optimal sensitivity and specificity, which is normally done with the aid of a receiver operating characteristics (ROC) curve. In general, when setting a low threshold value, this generates a high sensitivity and low specificity and vice versa when setting a high threshold. Both CRP and bilirubin have to be measured in absolute values, and in this situation, bilirubin seems superior in predicting perforated appendicitis. However, even though both CRP and bilirubin are mentioned in the included studies, none of the studies presented data on the combined use of CRP and bilirubin as predictors of appendiceal perforation.
Diagnostic scores have been developed in diagnosing acute appendicitis such as the Alvarado score (scale 0–10) (17), the modified Alvarado score for use in pediatric patients (18), pediatric appendicitis score (PAS; scale 0–10) (3), RajaIsteri Pengiran Anak Saleha Appendicitis (RIPASA) score for use in Asian patients (scale 0–14) (19), and appendicitis inflammatory response score (AIRS; scale 0–12) (20). Common for these scoring systems is the use of symptoms (duration of pain, migration of pain, nausea, vomiting), signs (tenderness, fever), and investigations (leukocytosis, CRP). All of these scores have been proven useful in predicting acute appendicitis in patients presenting with pain in the lower right fossa, but none of them evaluate the risk of appendiceal perforation. Furthermore, none of the above-mentioned scores use elevated bilirubin as a marker.
It has been shown that during appendicitis, an ulceration of the mucosa in the appendix occurs due to the inflammation, which facilitates bacterial translocation from appendix to the portal blood system (21). The most common bacteria to infect the appendix is the gram-negative Escherichia coli. When E. coli reaches the hepatic tissue via the portal venous system, animal models have shown that the bacteria interferes with the hepatocyte microcirculation, which induces damage to the liver cells and compromises excretion of bile acids into the bile canaliculi (22). Furthermore, E. coli has been shown to induce intravascular hemolysis, and both mechanisms may result in an increased amount of bilirubin circulating in the blood (23). Moreover, elevated serum bilirubin can be a result of mechanisms other than hepatobiliary diseases or intravascular hemolysis (24). Bilirubin can be elevated in cases of sepsis, intra-abdominal abscesses from urological, gynecological or gastroenterological origins, antiviral therapy or in patients with genetic diseases such as Dubin–Johnson syndrome, Rotor’s syndrome, and Gilbert’s syndrome (25). Dubin–Johnson and Rotor’s syndrome are uncommon, whereas Gilbert’s syndrome is a benign disease where unconjugated serum bilirubin is slightly elevated, and it is estimated that 3%–10% of Caucasians have this condition (26). Gilbert’s syndrome is remarkably more prevalent among males than females (27). It has been proposed that hyperbilirubinemia is a weaker marker of appendiceal perforation among persons with Gilbert’s syndrome (14). However, since Gilbert’s syndrome is considered a rare condition, this may not affect the value of hyperbilirubinemia as an overall predictor in both males and females.
There exists no single diagnostic test or symptom other than surgery with pathologic examination that can definitely result in a diagnosis. Several prognostic factors such as duration of symptoms, pain migration, indirect pain, abdominal guarding, and fever can be used in combination to predict a possible perforation of the appendix (28, 29). The studies included in this systematic review have all shown that elevated bilirubin can be used as a prognostic factor for the assessment of perforated appendicitis. The above-mentioned combinations of factors are especially important in the evaluation of patients with atypical clinical presentation. Furthermore, in many departments, blood samples including liver functional tests are not standard in children, and often only clinical evaluation is used for diagnosis. Regarding the clinical use of predictors in diagnostics of appendicitis or appendiceal perforation, elevated bilirubin should be considered as a supplement to other diagnostic tools such as CT scans. Data show that CT findings predictive of perforated appendicitis such as presence of extraluminal gas and localized abscess have high specificity of more than 98%, however, with lower sensitivity of 40% (9). A recent study found that the use of a low-dose abdominal CT scan in diagnosing simple appendicitis resulted in a sensitivity and specificity both exceeding 93% (30). However, early perforation or microperforation of the appendix can be very difficult to diagnose using CT (9).
The included studies had several limitations. They were all retrospective and without a healthy control group. The largest study (14) included 725 patients from two different centers, and the study period was different among these centers (5 years in one center and 10 years in the other center), which might have made treatment and diagnostic regimens not comparable in the study. Moreover, possible detection bias was present since the study used different measurement methods to evaluate bilirubin values. These methods were only comparable at the cutoff value and not at the high and low extremes, which makes high and low values of bilirubin not comparable within the study (14). Moreover, a possible selection bias could have been introduced since bilirubin was not measured in all patients. This was also the case in the other included studies (11, 13). The gender distribution was significantly different between the study groups in one study (12) and in two other included studies; it was not reported whether the gender difference between the study groups was statistically significant (5, 14). An uneven distribution of males and females could result in a risk of Gilbert’s syndrome being overrepresented in one group, which would distort the results. Moreover, possible confounders are present in all studies. This confounding can occur when the surgeon is aware that elevated bilirubin can predict perforation. Thus, the surgeon might be more prone to operate in case of an elevated bilirubin and therefore be more likely to diagnose appendicitis, which under different circumstances might not have been diagnosed, for example, subclinical appendicitis that may resolve without treatment.
In conclusion, elevated serum bilirubin can be used as a supplemental diagnostic tool in perforated appendicitis. The other important supplemental diagnostic tool for appendicitis and appendiceal perforation is CT scan that has high specificity for appendiceal perforation, although clinically, it is limited by low sensitivity. It is important to stress that no single predictive factor (serological, radiological) can stand alone in determining the course of action in patients suspected of appendicitis. Clinical examination remains the cornerstone in the diagnosis of simple and perforated appendicitis. Further studies should evaluate whether the predictive values of bilirubin, CRP, and WBC combined would be a stronger diagnostic tool for the clinician.