
Abstract
Backgrounds and Aims:
Due to growing interest into body contouring has abdominoplasty become one of the most common aesthetic operations. New techniques have appeared to reduce the relatively high incidence of complications in abdominplasty. One technique is the tension suture technique, which can be combined with lidocain-adrenalin-saline-infiltration. Our aim was to analyse the results of this combined technique.
Material and Methods:
This retrospective study consisted of 95 women operated on in a private hospital by one senior plastic surgeon between years 2004 and 2009. Sixty patients had other operations in addition to abdominoplasty: 49 liposuctions, six breast reductions or mastopexies, three umbilical hernioplasties, one brachioplasty, one partial excision of labias, and one blepharoplasty.
Results and Conclusions:
The operative time was 82 minutes ranging from 45 to 173 minutes. Peroperative bleeding was a mean of 196 ml in abdominoplasty only and 254 ml when combined with additional operation. Patients did not have any major complications and the total incidence of minor — not clinically significant — complications was 12.6%. Obesity, smoking, comorbidities, previous operations on belly area or additional operations did not affect the complication rates. Our study supports the view that the tension suture technique combined with lidocain-adrenalin-saline-infiltration decrease the formation of seroma and wound complications in abdominoplasty. Lidocain-adrenalin-saline-infiltration also fastens and eases the operation without increasing the risk of bleeding in experienced hands.
INTRODUCTION
During the last years body contouring has become more common due to increased bariatric surgery and demands on body image (1, 2). Massive weight loss results in functional problems due to excessive skin. Body contouring improves quality of life and body image of post-bariatric patients (3). As a part of body contouring abdominoplasty has become one of the most common aesthetic operations (1). Abdominoplasty, with or without liposuction, is a major operation sometimes with major complications. Studies on complications of abdominoplasty have revealed quite high incidence of seroma formation (5%–17.4%), haematomas (3%–5.8%) and skin necrosis (1.5%–6.7%) (4–7). On rare occasions some patients have been reported to have pulmonary embolism and small bowel obstruction (8, 9).
Because of these rather common problems, new techniques have appeared in order to minimise the rate of complications in abdominoplasty (10). As one of these, the progressive tension suture technique has been developed to decrease morbidity and postoperative complications (2, 11–14). In a closure of abdominoplasty the sutures are used to eliminate dead space between the flap and fascia (14–16). These sutures also eliminate shearing forces between the two layers; these forces are believed to be one reason of seroma formation. Tension sutures also decrease wound dehiscence and flap necrosis. This is because the sutures allow a tension-free closure by advancement of the abdominal flap in a proximal to distal direction (17). The sutures can be combined with tumescent technique which have been concluded to be a safe and effective technique i.e. by decreasing postoperative pain (18).
The aim of this study was to analyse the results of tension sutures in abdominoplasty combined with lidocain-adrenalin-saline-infiltration. Results were compared to those previously published materials of abdominoplasty.
MATERIAL AND METHODS
This retrospective study consists of 95 consecutive patients who had tension suture abdominoplasty combined with 1000 ml injection of saline mixed with 500 mg lidocain-adrenalin in the operating area prior to incision. All patients were operated on in a private hospital of Plastic Surgery Hospitals KL between years 2004 and 2009 by senior plastic surgeon AS. Every patient voluntarily sought for the operation. They were examined beforehand to state the need and suitability for an operation.
All the patients were women. Their average age was 42.8 years (range 20.3–66.8). Mean Body Mass Index (BMI) was 27.1 (range 18.8–38.8, SD 4.5). 15.8% of the patients were smoking. Two thirds of them were healthy; 4.3% had diabetes, 8.4% high blood pressure, 7.4% asthma, 8.5% hypo- or hyperthyreosis (1%), one had epilepsy, one had von Willebrand's disease and one psoriasis. More than half of the patients (61%) had had one or more previous operations on the belly area; most abdominal operations were ceacarean sections.
We divided the patients into two groups by their BMI to find out if obesity had any effect on the rate of complications: group 1 with BMI ≤ 30 (n = 68) and group 2 with BMI > 30 (n = 23). The same comparison of the incidence of complications was done also in groups of smoking, comorbidities, previous operations on belly area, and additional operations.
SURGICAL TECHNIQUE
Preoperative markings were made in the standing position. All patients received one dose of prophylactic antibiotic peroperatively (Kefuroxim 1.5 g intravenously) and received 20–40 mg KlexaneR s.c. at the end of the operation. Every operation was done under general anaesthesia. Before the skin was incised a mixture of lidocain-adrenalin and saline was infiltrated into the whole operation area using a 2 mm (diameter) and 20 cm long cannula. Both flanks were also infiltrated if liposuction of the flanks were made. Every patient was operated on by using conventional procedure of abdominoplasty i.e. skin and fat were removed with a boat shaped incision from the umbiliculus distally to pubes. Proximal skin flap was raised cranially up to processus xiphoideus. Midline rectus muscle fascia plication was performed in almost all cases (n = 93) by using single 1–0 SurgilonR X-sutures and second layer with continuous 1–0 PDSR loop. The progressive tension sutures were used for closure: 2–0 VicrylR sutures were used with 2–3 cm intervals to close the gap between fascia and fat. The skin was closed with intradermal 3–0 VicrylR sutures and intracutaneous 3–0 MonocrylR continuing suture. All patients wore an elastic belt for 4 weeks postoperatively and they were told to avoid heavy lifts (> 10 kg) for the next 5–6 weeks.
Sixty patients had additional operations with abdominoplasty: 49 had liposuction of both flanks (100–350 ml fat/flank), six patients breast reduction or mastopexy, three umbilical hernioplasty, one brachioplasty, one partial excision of labias, and one blepharoplasty. Drains were used for the first 12 patients. However, due to minimal bleeding, drains were abandoned for the rest 83 patients. After the operation every patient was recommended to use elastic garments for four weeks. The majority of patients were discharged from the hospital on the day after surgery. Only three patients needed additional 1–2 nights.
STATISTICAL ANALYSIS
All information was collected from patient charts. The data was analysed by using the Statistical Package for the Social Sciences (SPSS), version 18.0.0. Means and percentages are used for describing the data. Skewed data was analysed with Mann-Whitney U-test. Differences in proportions were compared with Fisher's exact test.
RESULTS
The mean operative time was 82 minutes (SD 28, Table 1), consisting of the time from infiltration of the mixture of lidocain-adrenalin and saline to the closure of the wound. For those patients who had abdominoplasty only (n = 35), the operation lasted in average 65 minutes (SD 15).
Operative data.
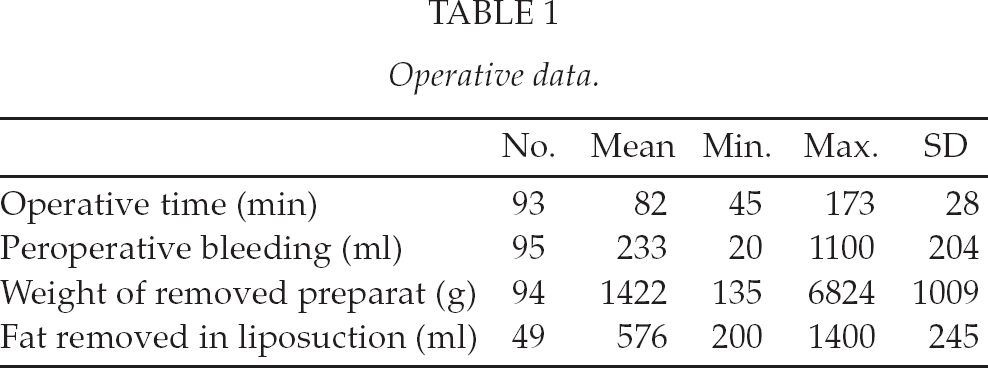
Because of the high quantity of additional operations, we viewed peroperative bleeding more closely. When looking at patients with abdominoplasty only, the mean peroperative bleeding was 197 ml (SD 184). For abdominoplasties with additional operations (n = 60) the mean peroperative bleeding was 255 ml (SD 214). The difference between patient groups was statistically significant (p = 0.047).
The senior surgeon followed up the patients. The patients (n = 84) had their first follow-up at one month. The second follow-up was at 4–8 months. Patients did not appear to have any major complications such as pulmonary embolus, deep vein thrombosis or flap necrosis. The total incidence of minor complications was 12.6%: small seroma formation 2/95, small haematomas 3/95, local wound infection 1/95, partial necrosis of wound edge 1/95, local (suture) fistulas of wound 3/95 and other complications 2/95. Both seromas were only palpable and needed no needle aspiration. Only one patient, who had haematoma in flanks after liposuction, received two units of blood two days after the operation. Three haematomas were small and did not need to be evacuated. One local wound infection was treated by antibiotics for a week. This same patient had a small wound edge necrosis in the umbiliculus, which was revised at local anaesthesia. The local fistulas caused by 2–0 VicrylR sutures were treated conservatively. One umbiliculus was lost because of insufficient blood flow and one small fascia defect was sutured with three 2–0 PDSR sutures in local anaesthesia.
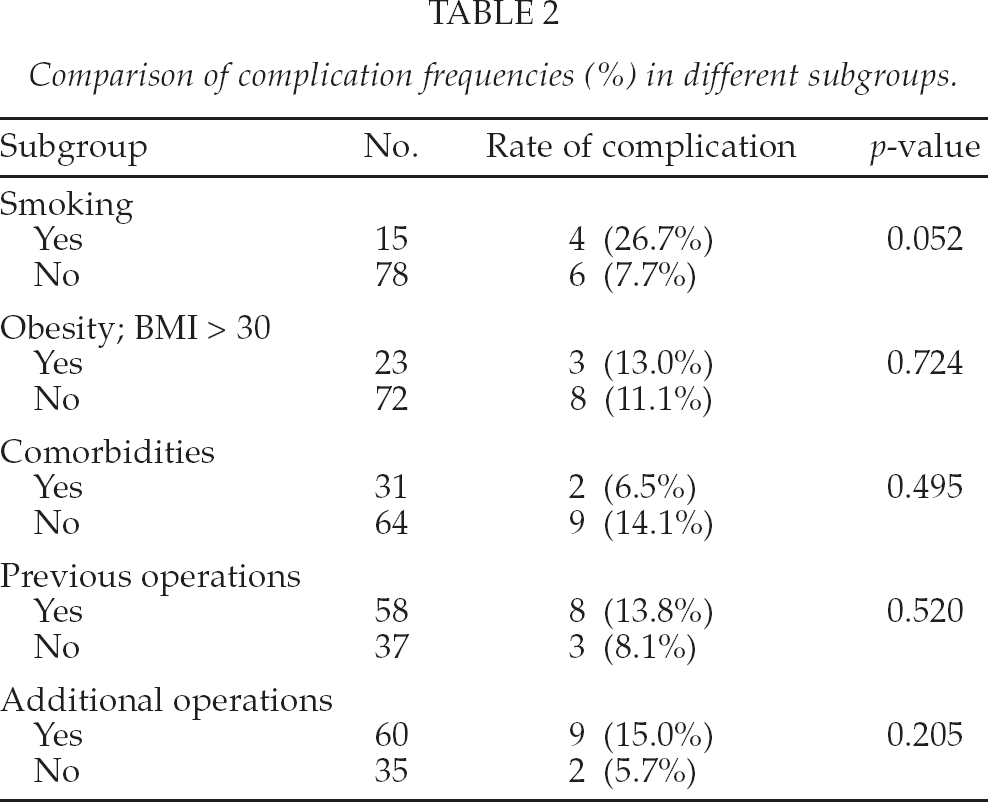
When comparing the incidence of complications in different subgroups, only smoking had a trend to increase the rate of complications. The other factors did not affect the rate of complications (Table 2).
Comparison of complication frequencies (%) in different subgroups.
DISCUSSION
As abdominoplasty has gained constantly growing interest, it is important to develop techniques to reduce complications. One of these techniques is tension suture technique, also called as quilting sutures (19). By using tension suture technique with lidocain-adrenalin-saline-infiltration, we achieved an incidence of complications of 12.6%; this being less than in previous studies (18%–35%) (6, 20).
Although seeking for improvement, a new technique itself can increase morbidity, for instance by lengthening the operative time (21). In our study the mean operative time was 65 minutes when only abdominoplasty was performed. This is much less than in other studies (22). In one study progressive tension sutures increased operative time by 50 minutes without any affect on seroma formation (17). In our study this technique did not increase operative time after an appropiate learning curve. Lidocain-adrenalin-saline-infiltration takes some time to do. However, vasoconstriction reduces blood flow during the operation and makes it easier to coagulate clearly visible veins and arteries (23). Mainly the additive effects on the duration of operation are the additional operations done at the same session.
One reason for the low rate of complications (12.6%) may be that there were few severely obese patients in our patient series. The highest BMI of our patients was 38.8, so there were not any morbidly obese patients in our data. However, it has been concluded that obesity does not increase complication rate (20, 24). We did not exclude patients with diabetes or high blood pressure as Rogliani et al. did in their study (20). Smoking was the only factor showing a trend to increase complication rate. This is a known fact to affect wound healing in abdominoplasty. Manassa et al. found 47.9% of smokers to have significantly more wound healing problems when compared to non-smokers (14.8%) (25). In our study 26.7% of smokers had complications.
In our study lidocain-adrenalin-saline-infiltration was combined with the tension suture technique. The infiltration used in this study seamed not to increase the amount of complications compared to other papers concerning tension suture technique (11, 16, 17). In our experience the infiltration used makes the operations faster by making the dissection easier. Seroma formation is the most usual problem after abdominoplasty. Our study had an incidence of small seromas of 2.1%. There were no clinically significant seromas that needed aspiration. This is clearly lower than in previous studies (17).
CONCLUSIONS
Our study shows that the tension suture technique combined with lidocain-adrenalin-saline-infiltration decrease the formation of seroma and wound complications in abdominoplasty. The technique is safe and no drains are needed. After an appropriate learning curve it does not increase the duration of operation. The lidocain-adrenalin-saline-infiltration also fastens and eases the operation without increasing risk of bleeding.