
Abstract
Background and Aims:
Atrial fibrillation (AF) is the most common arrhythmia after coronary arteryby pass surgery (CABG). Intravenous metoprolol and biatrial pacing have been reported to be effective in AF prophylaxis after cardiac surgery. The purpose of this trial was to compare the efficacy of intravenous metoprolol versus biatrial pacing combined with oral metoprolol in the prevention of AF after CABG.
Methods:
A single-centre prospective randomized open trial of 165 consecutive patients undergoing their first CABG. Patients were randomized to receive either intravenous metoprolol infusion 1–3 mg per hour or biatrial overdrive pacing and oral metoprolol (50–150mg) daily for 72 hours after CABG starting immediately after the surgery. AAI pacing with a pacing rate of 10 beats/minute above the baseline heart rate was used. Patients had continuous ECG-monitoring. The primaryend point was the first episode of AF.
Results:
The incidence of postoperative AF in the intravenous metoprolol and biatrial pacing groups did not differ from each other (14% vs. 18% respecively, p = 0.66). There was no difference in the time of AF on set between the groups (28.2 ± 16.2 h vs. 30.1 ± 21.2 h respectively, p = 0.8). Intravenous metoprolol infusion had to be temporarily interrupted for one hour in eleven patients because of hypotension or bradycardia. One case of bleeding from the left atria related to the pacemaker electrode wire was found.
Conclusion:
We found no difference in the incidence of AF between patients treated with intravenous metoprolol or the combination of biatrial pacing and oral metoprolol.
Keywords
INTRODUCTION
Atrial fibrillation (AF) remains the most common arrhythmia after cardiac surgery. The reported incidence varies between 18% and 57% and is higher after combined coronary artery bypass grafting (CABG) and valve surgery than after CABG alone. Postoperative AF may cause stroke after on-pump CABG. In addition, it increases the frequency of other complications and is associated with a need for additional treatment, prolonged hospital stay and increased costs (1–10).
The efficacy of beta-blockers in the prevention of AF after cardiac surgery has been demonstrated in numerous studies. In a meta-analysis consisting of 27 prospective randomized trials and 3840 patients, the incidence of AF ranged from 33% in the control group to 19% in the group treated with beta-blockers (11). However, the bioavailability of orally administered beta-blockers is markedly reduced during the early phase after cardiac surgery (12). It has been shown that intravenous metoprolol is superior to oral metoprolol in the prevention of AF after cardiac surgery (13). Several studies have assessed the efficacy of atrial pacing in the prevention of AF after cardiac surgery (15–17). One prospective study and one meta-analyses concluded that only biatrial pacing is effective in AF prophylaxis after cardiac surgery (14, 18). In addition, biatrial pacing combined with beta-blockers seems to be more efficient in AF prophylaxis than biatrial pacing alone (17, 19).
The aim of this trial was to compare the efficacy and safety of intravenous metoprolol versus biatrial pacing combined with oral metoprolol in the prevention of AF after cardiac surgery.
PATIENTS AND METHODS
This was a single-centre prospective randomized open trial. The study enrolment took place between January 2007 and June 2009. The study protocol was approved by the Kuopio University ethics committee, and all patients gave written informed consent.
The study population consisted of 165 consecutive ethnic Finnish patients scheduled to undergo their first CABG surgery. Exclusion criteria were previous AF or flutter, 2nd or 3rd degree atrioventricular block, pulse rate < 60 beats per minute, acute cardiac failure, emergency operation, and patients refusal. The study flow diagram is presented in Fig. 1. The off-pump CABG procedures were performed from a medial sternotomy, using pericardial bottom stitch, a suction stabilizator and a vessel-sized intracoronary shunt. The on-pump patients underwent standard cardio-pulmonary bypass, and intermittent cold crystalloid cardioplegia was administered via the antegrade and/or retrograde route. The cardioplegia solution consisted of 32 mEq/l magnesium, and no extra magnesium substitution was administered.
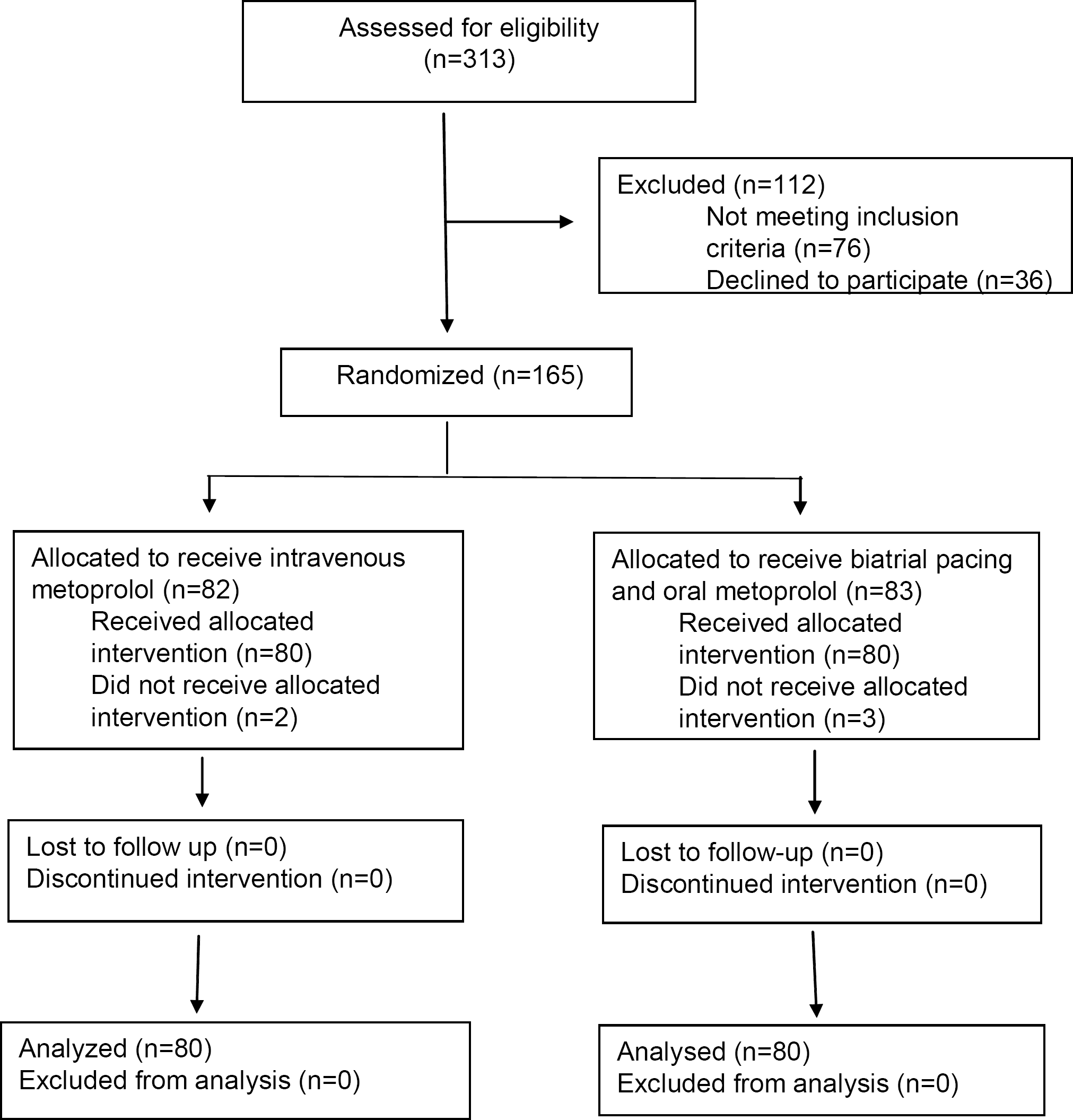
Flow diagram of the progress through the phases of the parallel randomized trial of intravenous metoprolol and biatrial pacing groups. Reasons for exclusions were as follows: Previous AF or flutter, 2nd or 3rd degree atrioventricular block, pulse rate <60 beats per minute, acute cardiac failure, emergency operation and patient's refusal.
After the surgery, patients were followed in the intensive care unit and weaned off mechanical ventilation when they fulfilled the following criteria: hemodynamic stability, peripheral temperature of more than 32°C, co-operativity and no major bleeding. Chest drains were removed on the first postoperative day and patients were referred to the surgical ward.
All patients were connected to three-channel ward monitors for continuous electrocardiographic monitoring for the 72-hour study period. The ECG was reviewed by the cardiac anaesthesiologist on duty. The rhythm was defined as AF when there were no consistent P waves before each QRS complex and ventricular rate was irregular. AF episodes lasting longer than 5 minutes were recognized.
Perioperative myocardial infarction was defined as the development of new Q waves. A stroke was defined as a new neurological symptom verified by correlative changes in computerized tomography. Mediastinitis was defined as a deep sternal wound infection requiring surgical intervention.
STUDY PROTOCOL
Randomization was performed preoperatively. The randomization envelopes were prepared by a secretary. Treatment allocations were written onsheets of paper in a blinded randomized manner. The randomization envelope was opened by the investigator. The patients were assigned to the intravenous metoprolol or biatrial pacing groups according to the allocation designated in the next envelope opened in sequence.
Patients in the intravenous metoprolol group were given metoprolol according to the heart rate as follows: at heart rate 60–70 beats per minute (bpm), the dose was 1 mg/h; at heart rate 70–80 bpm, the dose was 2 mg/h; and at heart rate > 80 bpm, the dose was 3 mg/h. If heart rate dropped below 60 bpm or systolic blood pressure dropped below 100 mmHg during the treatment, intravenous metoprolol was discontinued for one hour and then continued according to heart rate, as described above.
Temporary biatrial pacing wires were implanted during the operation (Ethicon Inc. Somerville, New Jersey USA), the cathode into the roof of the left atrium, between the superior pulmonary veins, and the anode into the lateral wall of the right atrium. Pacing and sensing thresholds were measured. AAI (atrium paced, atrium sensed, and pacemaker inhibited in response to sensed beat) mode pacing was started, 10 bpm above the baseline heart rate with pacing output three times higher the pacing threshold. Pacing threshold and baseline heart rate were checked two times per day, and pacing rhythm was adjusted according to the heart rate if needed. The maximum pacing output was 20 mV and the maximum pacing frequency was 100 bpm. Oral metoprolol dosage in the pacing group was based on the underlying heart rate: at heart rate 60–70 bpm, the metoprolol dose was 25 mg 3 times per day, at 70–80 bpm the dose was 50 mg 2 times per day and at the heart rate over 80 the dose was 50 mg 3 times per day. Oral administration of metoprolol was started 16–20 hours postoperatively. Treatments in both groups were started when the patient arrived in the intensive care unit. The primary endpoint of the study was the occurrence of the first AF episode or completion of the study period, which was 72 hours. After the first episode of AF, the study protocol was discontinued.
STATISTICAL ANALYSIS
The difference in continuous variables was analyzed using the Mann-Whitney U-test. Differences in categorized variables were tested using the x2 test or the Fisher exact test. Kaplan-Meier curves were depicted for freedom from AF. The limit for statistical significance was p <0.05. All statistical procedures were performed with SPSS for Windows, release 14.0 (SPPS Inc., Chigaco, IL, USA).
RESULTS
The mean age of the patients was 66 years and 82% were male. There were no significant differences between the groups as regards the preoperative characteristics of the patients. The use of preoperative beta-blockers was similar between the groups. Preoperative data are presented in Table 1. A majority (94.5%) of the patients underwent off-pump surgery. The type of surgery did not differ between the groups. Neither was there any difference between groups with respect to the number of peripheral anastomoses or right coronary artery bypass grafting. Intraoperative data of patients groups are presented in Table 2.
Preoperative data of the patients in the intravenous metoprolol and biatrial pacing groups.
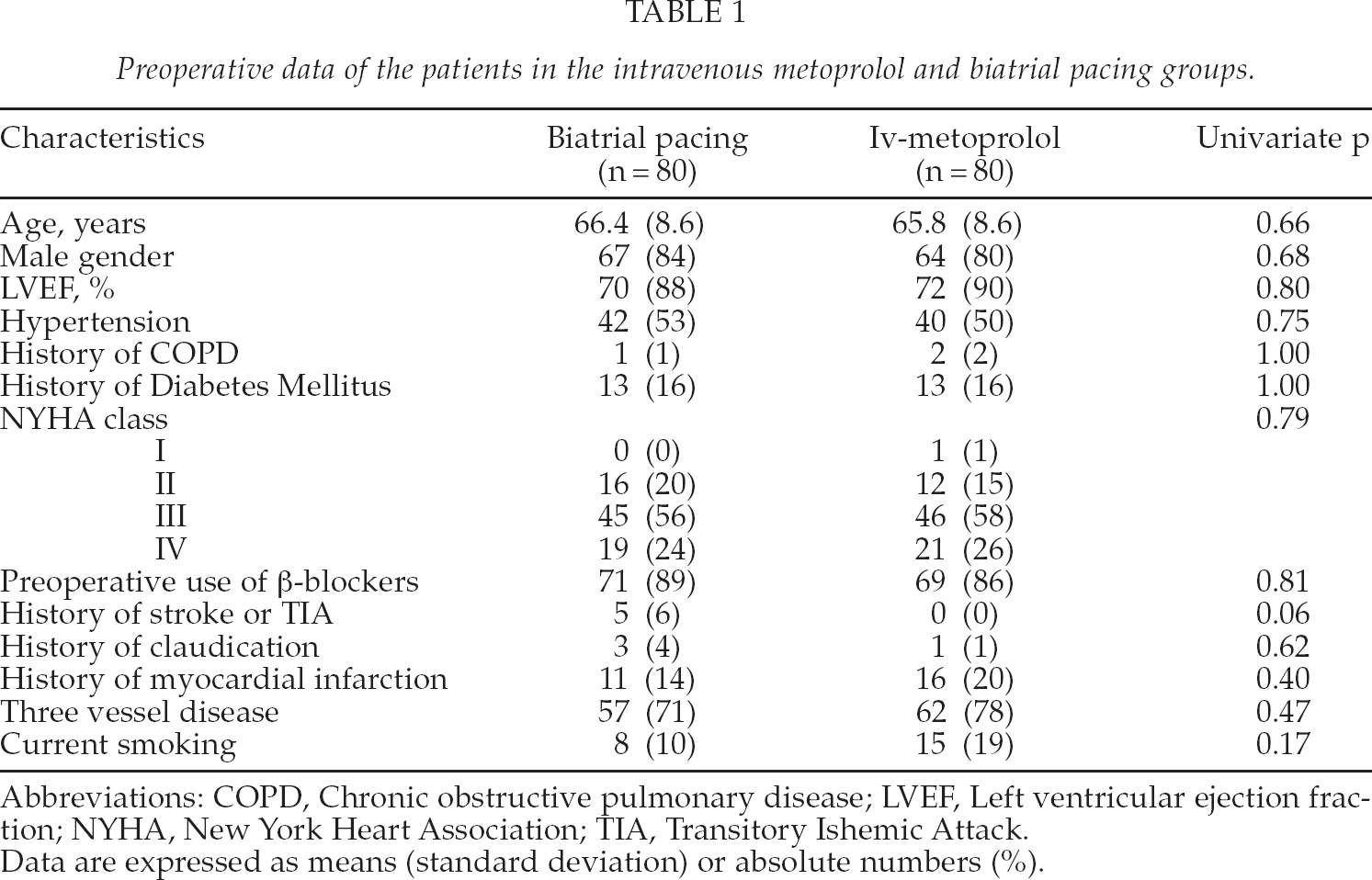
Abbreviations: COPD, Chronic obstructive pulmonary disease; LVEF, Left ventricular ejection fraction; NYHA, New York Heart Association; TIA, Transitory Ishemic Attack.
Data are expressed as means (standard deviation) or absolute numbers (%).
Intraoperative data of the patients in the intravenous metoprolol and biatrial pacing groups.
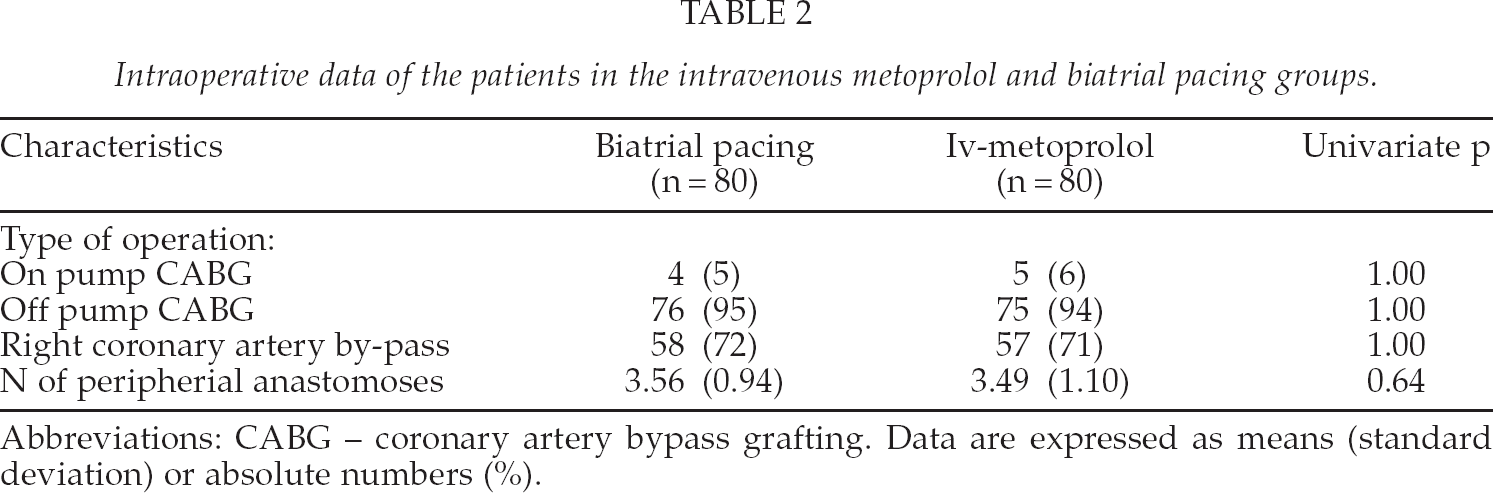
Abbreviations: CABG — coronary artery bypass grafting. Data are expressed as means (standard deviation) or absolute numbers (%).
Two patients in the intravenous metoprolol group did not get the allocated treatment. One patient did not receive metoprolol because he required amiodarone infusion for the treatment of ventricular arrhythmias. Another patient had severe cardiac failure postoperatively and required inotropic medication for several days postoperatively. In addition, the intravenous metoprol group infusion was discontinued for one hour in 8 cases due to hypotension, and in 3 cases due to bradycardia.
Three patients in the pacing group did not receive the allocated treatment. One patient had perioperative bleeding caused by the implantation of the left atrial pacing wire. The bleeding site in the left atria was sutured successfully, but the study protocol was not continued. Two patients in the pacing groups developed AF perioperatively, and they were excluded from the study. A total of 25 patients developed AF during the study period. The incidence of AF in the pacing group n = 14 (18%) and in the intravenous group n = 11 (14%) did not differ significantly (p = 0.66). The mean time of AF occurrence did not differ between the groups (28 ± 16.2 vs. 30.1 ± 21.2). After the study period, seven additional patients experienced AF with no difference between the groups. The effect on the incidence of postoperative AF was similar in both treatment groups (p = 0.52), Fig. 2. There were no postoperative complications associated with AF. Postoperative data of the patient groups are presented in Table 3.
Postoperative data of the patients in the intravenous metoprolol and biatrial pacing groups.
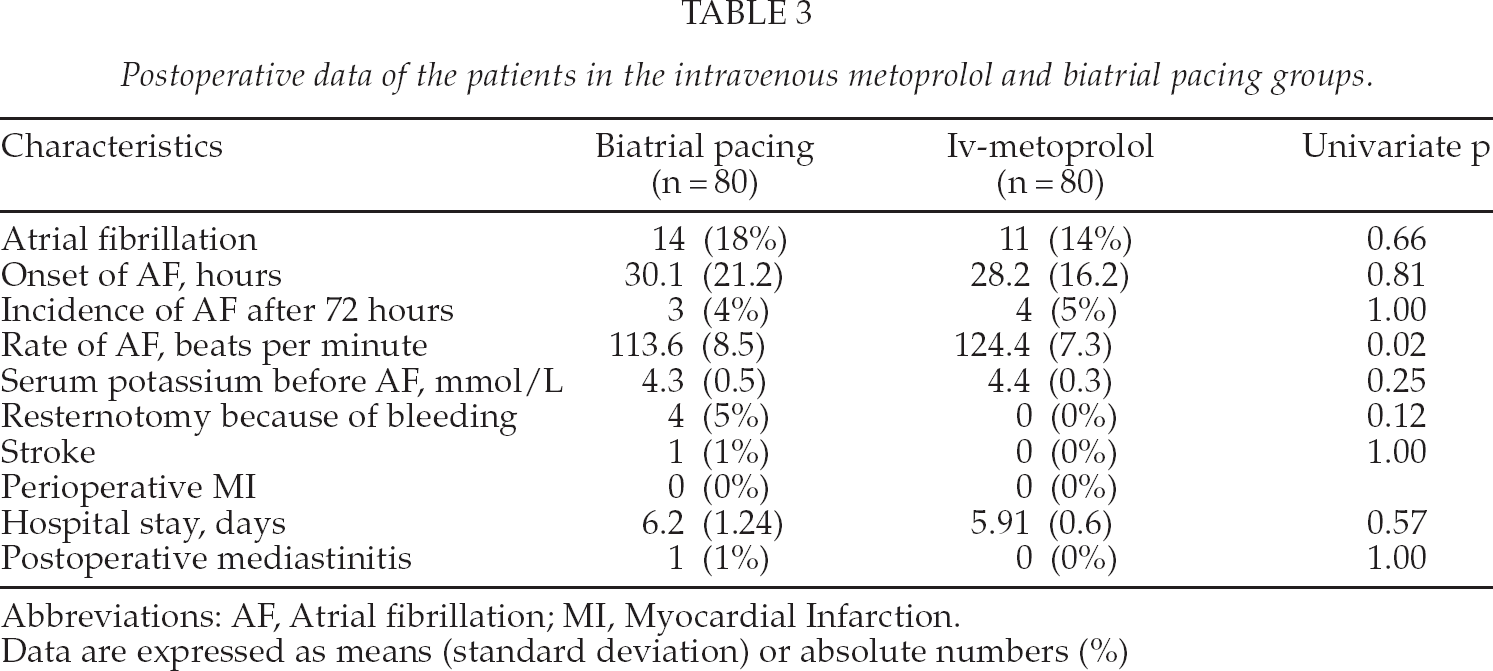
Abbreviations: AF, Atrial fibrillation; MI, Myocardial Infarction.
Data are expressed as means (standard deviation) or absolute numbers (%)
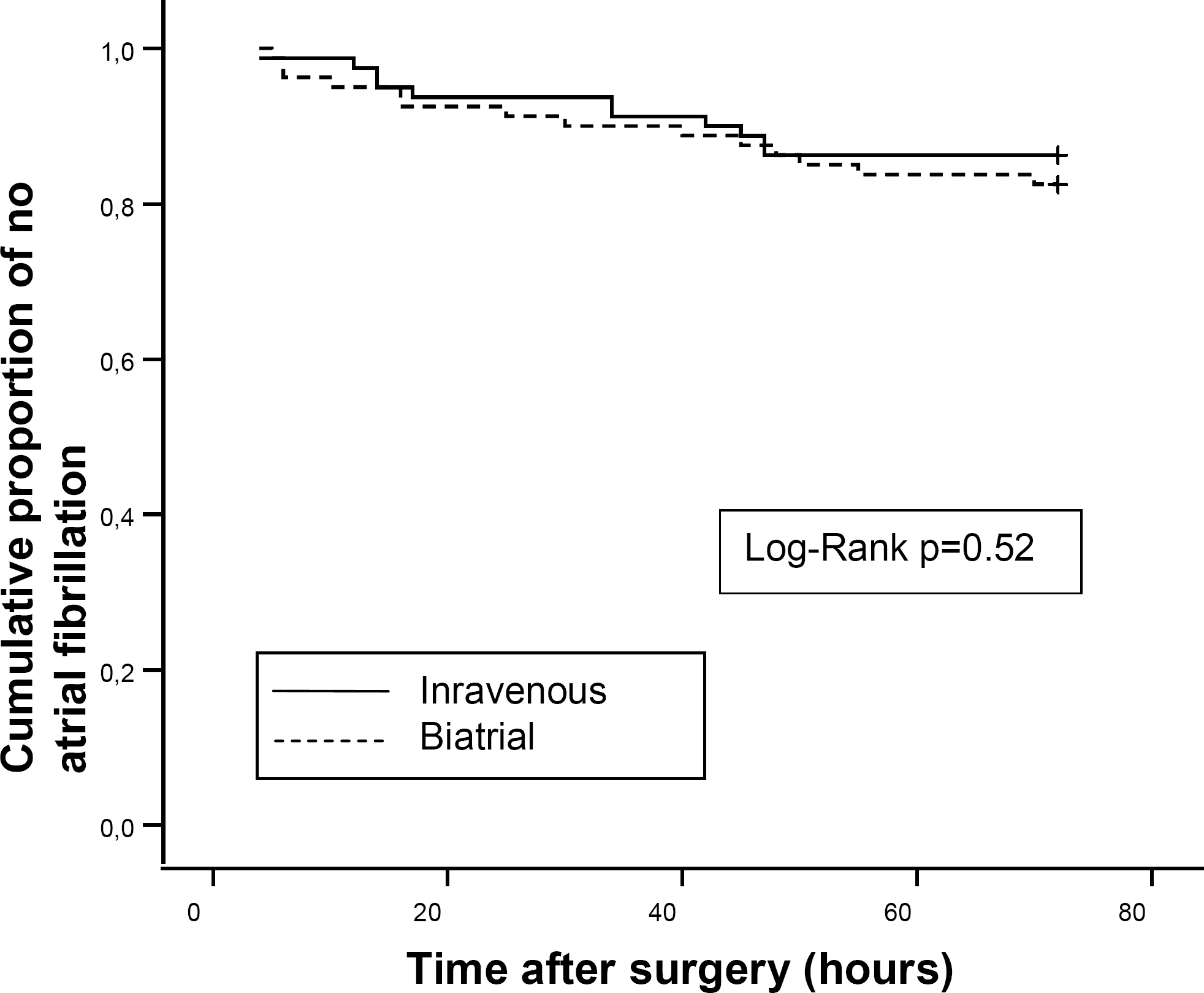
Kaplan-Meier plot of the effect of intravenous metoprolol and biatrial bacing combined with oral metoprolol on the incidence of postoperative atrial fibrillation after coronary artery bypass grafting.
One patient in the intravenous metoprolol group succumbed on the fifth postoperative day to a large stroke. He had no AF postoperatively.
DISCUSSION
The main finding of our study is that there was no difference in the incidence of AF between the biatrial pacing and the intravenous metoprolol groups. Several pacing protocols have been used in the prophylaxis of postoperative AF. Biatrial pacing has been shown to be the most efficient pacing protocol, especially combined with beta-blockers. (17–19). Why was not biatrial pacing combined with oral metoprolol more efficient than intravenous metoprolol alone in the prevention of AF after CABG? All the patients (both groups) were given equivalent amount of metoprolol according to the baseline heart rate. Despite complete gastrointestinal absorption, only about 50% of a single dose of metoprolol reaches the systemic circulation because of extensive first pass metabolism (21). The bioavailability of metoprolol is markedly impaired for a few postoperative days after CABG (12), and it has also been shown that intravenous administration of metoprolol results in higher metoprolol concentration and is more efficient in the AF prophylaxis after CABG than oral metoprolol (13). Thus, our conclusion is that both intravenous administration of metoprolol and the combination of biatrial pacing and oral metoprolol are effective in the prevention of AF after CABG. According to our knowledge there are no earlier studies comparing directly intravenous beta blockers and biatrial pacing in AF prophylaxis.
Metoprolol infusion was temporarily interrupted because of hypotension or bradycardia in 11 patients, but the infusion could be restarted after the interruption in all patients. Bradycardia caused by beta blocking can be prevented by atrial pacing. Accordingly, a combination of intravenous beta blocker and biatrial pacing might be even more effective than intravenous beta blocker or biatrial pacing alone. One patient in the biatrial pacing group developed major bleeding from the left atrium, which was successfully sutured and caused no morbidity. There were no other side effects related to either prophylaxis protocol. We found biatrial pacing to be slightly troublesome to implant. The incidence of AF postoperatively was surprisingly low in both groups, which may be due to the excellent treatment impact. A great majority of procedures were made using the off-pump technique, which might be another reason for the low incidence of postoperative AF (20). Patients had good left ventricular ejection fraction in both groups. This fact might be also one reason for low incidence of postoperative AF. We found no rebound effect after the study protocols were completed. Indeed, the incidence of AF after the study period was low in both groups.
The main limitation of our study is the small sample size. We did not perform a sample size calculation prior to the study, but planned to enrol CABG patients for a period of 18 months.
Because of the small number of subjects in the study groups multivariate analysis was not performed. However, randomisation was successful. There was no significant difference in demographic or perioperative data between the groups. Thus, clearly there is no real difference in the efficacy of AF prophylaxis between the groups.
In conclusion, we found no difference between intravenous metoprolol and biatrial pacing combined with oral metoprolol in the efficacy of AF prophylaxis after CABG.
Footnotes
ACKNOWLEDGEMENTS
The study was financed by Savon Sydänpalvelu OY, Kuopio Finland. It had no role in data collection, analysis of the results or preparation of the manuscript