
Abstract
Background and Aims:
Stress fractures are common overuse injuries in athletes. Medial malleolar stress fractures are rare but they have an important clinical relevance because of their tendency to cause considerable disability and loss of time in sports without proper treatment. The diagnosis of medial malleolar stress fracture is often a challenge and it is therefore often delayed which may cause even further problems in the treatment. The purpose of this study was to increase the awareness of medial malleolar stress fractures as a possible cause for medial ankle pain and to stress the importance of MRI in the diagnostics as well as to evaluate the results of surgical treatment.
Patients and Methods:
Between 1995 and 2008, a total of ten athletes with a medial malleolar stress fracture were operated at our centre. All operated cases during those years were included in the study. The cases were retrospectively analyzed. Return to pre-injury level of sport was evaluated and considered as an indicator of successful treatment.
Results:
Initially all standard radiographs were negative whereas in MRI the fractures were all visible. After operative treatment all medial malleolar stress fractures healed clinically in three to four months and all except one of the athletes were able to return to their pre-injury level of sports.
Conclusion:
Early MRI is recommended if a medial malleolar stress fracture is suspected. Surgical treatment seems to result in rapid healing of the fracture and return to sports. In our opinion early surgery should be considered especially in athletes.
INTRODUCTION
Lower extremity stress fractures are common in athletes and military recruits (1, 2, 3). The most common site for stress fractures in lower extremity is the distal third of the tibia (1, 4). Medial malleolar stress fractures are rare accounting only 0.6–4.1% of all stress fractures (5, 6, 7). These fractures occur most often in track and field athletes, long distance runners and basketball players, that is in sports where running and repeated jumping is frequent (5, 7).
The rapid increase of stress on tibia is often the main reason for the medial malleolar stress fractures (1, 6, 8). Symptoms of a medial malleolar stress fracture can be vague in the beginning (1). Often the main symptom is localized pain at the medial side of the distal tibia, but pain can also be vague and difficult to localize (6). It usually starts after a longer exercise, gradually aggravating and finally it can be felt in rest as well (1, 8).
In high level athletes fast return to sport after injury is imperative. When considering treatment it is also essential to prevent possible injury-related complications. The aim of this study was to provide more information about the diagnosis and surgical treatment of medial malleolar stress fractures in athletes.
PATIENTS AND METHODS
This is a retrospective study of ten athletes with a medial malleolar stress fracture, who were treated operatively between the years 1995–2008. The patients were referred from all over the country. There were six men and four women with a mean age of 23 years (range, 17 to 39). All the patients were involved in various sporting activities. There were six track and field athletes (jumping events and hurdling), two long-distance runners, one soccer player and one biathlonist.
All the patients complained of vague pain and discomfort in the medial side of the distal tibia. Symptoms had increased gradually and were first typically felt only during training. On clinical examination, tenderness to palpation was reported at the affected area.
A diagnosis of medial malleolar stress fracture was suspected on the basis of history and clinical examination. Plain films had been taken routinely and MRI was used in all cases to confirm the diagnosis (Fig. 1). No other significant pathological findings were seen in MRIs or plain films.
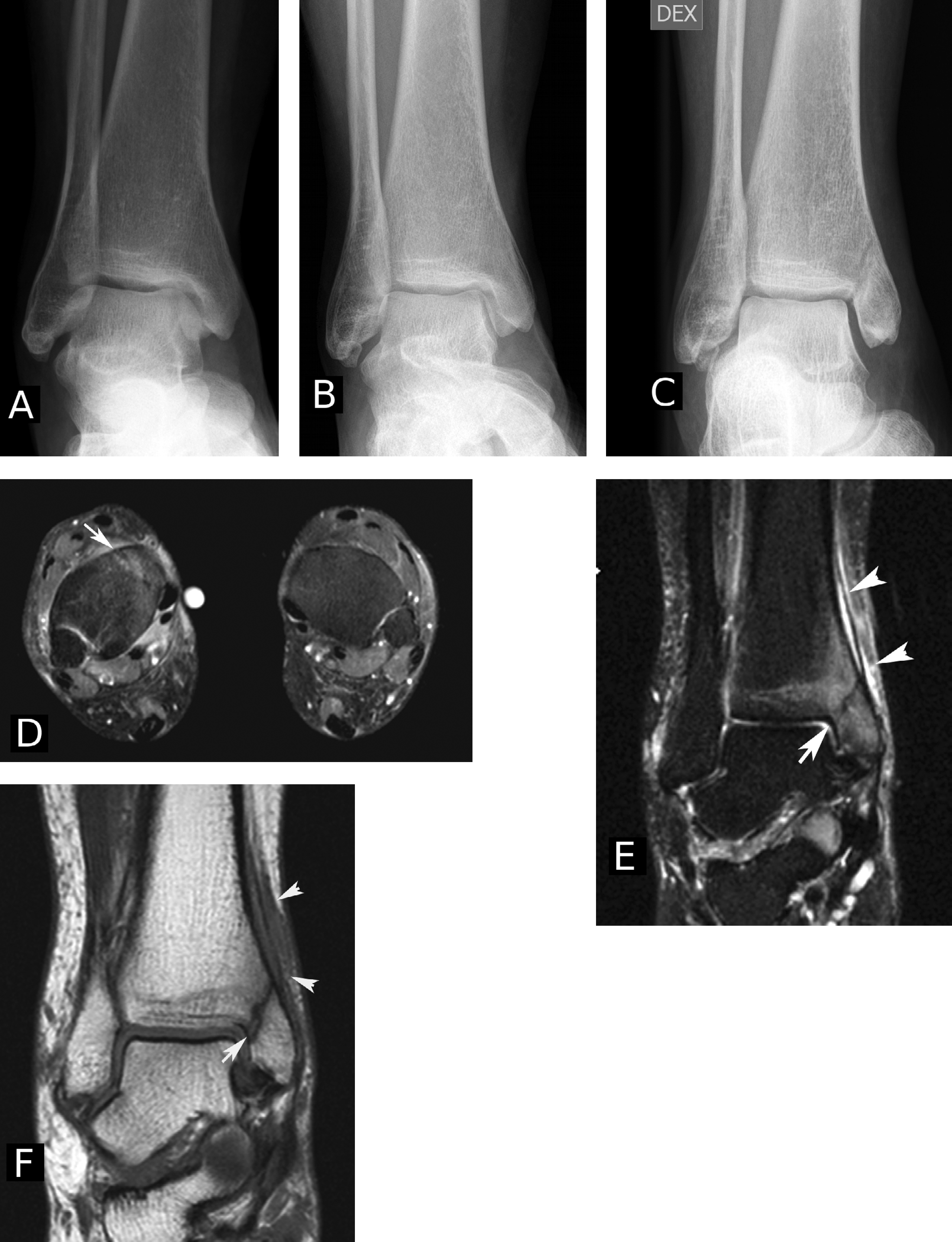
Early diagnosis of medial malleolar stress fracture can be very challenging. These images are an example of a female patient with no previous injury in her right ankle. She had medial ankle pain even while walking slowly. Radiographs remained normal despite of increasing pain. Radiographs obtained at one month (A) and three months (B) after the onset of pain. The radiographs were normal, and even in retrospective analysis no clear sign of fracture was detectable in antero-posterior or lateral radiographs. Due to consistent pain and swelling around the medial malleolus, stress fracture was suspected, and MRI examination was done two months later (at five months from the onset of symptoms). Axial (D) and coronal (E) fat saturated T2 weighted images revealed bone marrow edema surrounding an oblique fracture line at the base of the medial malleolus (D, E and F). The fracture line is indicated with white arrow in D, E and F images. Soft tissue and periosteal swelling indicated with arrowheads (E and F). In T1 weighted image (F) the fracture line was more visible, but it was less sensitive to edema. Repeat radiograph (C) obtained at the same time as the MRI was already positive for the undisplaced old stress fracture.
In this study group five patients with undisplaced medial malleolar stress fractures first underwent conservative treatment. In these cases the correct diagnosis was done between six weeks to four months after the onset of symptoms. The patients were assigned to only completely pain free limited weight bearing with crutches and with a walker orthosis for six weeks. After that the patients were instructed to avoid all stressful activity for an additional three to four months. Because of continuing symptoms and no signs of healing in radiographs all of these five patients were operated between four to six months after the correct diagnosis.
Because of these failed conservatively treated cases we have nowadays changed our criteria for conservative treatment. In addition that the stress fracture should be in a good position (no diastase or cortical crack in MRI) the right diagnose should also be done in early phase i.e. in two to three weeks after onset of symptoms.
In three cases with early diagnosis there was a visible cortical crack with a small diastase in MRI. Those patients were operated without conservative treatment because of a potential risk for fracture dislocation. The remaining two patients with a delayed diagnosis (five and 18 months after the onset of symptoms) were referred to our hospital from other centers. Both of these were operated on without further attempts of conservative treatment due to the lengthy delay in the diagnosis and longstanding symptoms.
In surgery spinal anesthesia was used in all cases. The patients were positioned supine and a tourniquet was used. A curved incision was made on the medial malleolus and a compression osteosynthesis was performed using two parallel partially threaded 4.0 mm AO cancellous compression screws under the guidance of an image intensifier. In no cases was bone grafts used.
Postoperatively a soft bandage was used for two weeks. No casts were used. Partial weight bearing using crutches was allowed during the first four to six weeks. Swimming and water training was allowed four to six weeks after surgery. Cycling and light gym training, with gradually increasing intensity, were begun six weeks after the operation. Running was allowed three months after the operation. In most cases the screws were removed after ten to twelve months under local anesthesia.
The patients were followed postoperatively at our outpatient clinic. Follow-ups were first arranged routinely with monthly visits. Additional long-term follow-ups were scheduled for the study purposes. The mean length of the follow-up was 62 months (range, 12 to 132). At follow-up, the patients were asked about possible symptoms and their return to the pre-injury level of sports was evaluated.
RESULTS
None of the fractures were visible in the initial plain films whereas in the MRI the fracture line and discontinuation of the cortex could be easily observed already at an early phase.
After surgery all ten fractures healed clinically within three to four months. In nine cases the patients were asymptomatic and able to fully return to the pre-injury level of sporting activities. This occurred in three to five months after surgery.
The one patient who was not able to return to his pre-injury level of sports was mostly pain-free in normal activities of daily living but he was not able to continue his sports career. Before the correct diagnosis and referral to our clinic his stress fracture had dislocated causing cartilage damage at the medial corner of the talus and tibia resulting in synovitis and stiffness of the ankle joint. Before the fracture-dislocation he had been symptomatic for 18 months. All the plain films taken before the fracture-dislocation were negative.
There were no intra- or postoperative complications in this series.
DISCUSSION
The etiology of medial malleolar stress fracture is multifactorial involving increased repetitive sub-maximal stresses and axial and torsional forces (9). However, other factors such as abnormal biomechanics (malalignments of lower extremity, broader talus neck, abnormal pronation/supination and chronic ankle impingement), muscular contractions and hormonal imbalances can also have an effect on the nascence of the symptoms (5, 10, 11, 12). These same factors can also have effect on the healing process of medial malleolar stress fracture resulting in delayed healing and non-union of the fracture; and even dislocation (13, 14).
The diagnosis of medial malleolar stress fracture can often be difficult (3, 6, 15). Like in many other stress fractures it is also common for medial malleolar stress fractures that plain radiographs are frequently normal at the early phase (1, 5, 6, 8). Normally a stress fracture can be visualized in plain films after two to four weeks (6, 16). However, medial malleolus consists mainly of cancellous bone, which can explain why the detection of the medial malleolar stress fracture using plain films can be difficult even after the early phase. In our series there were cases in which plain radiographs did not show the fracture reliably even in the chronic phase whereas using MRI early detection of the stress fractures was easily done. Due to these reasons and the fact that this injury may have a tendency to dislocate and cause severe complications we recommend early MRI if medial malleolar stress fracture is suspected.
It seems that most of the medial malleolar stress fractures that are diagnosed early and in which there is neither dislocation nor a cortical crack can heal conservatively in 3 to 5 months with good results (1, 5, 6, 11, 17, 18). However, operative treatment seems to enable the athlete to return earlier to sporting activities (8, 14, 15, 18). It allows also more rapid rehabilitation and has a higher rate of union than conservative treatment (13, 18). These are naturally important aspects when considering treatment methods for athletes. Even though these recommendations are mainly based on small patient series and expert opinions and comparative prospective studies are lacking, many authors suggest operative treatment for medial malleolar stress fractures especially in elite athletes (3, 5, 8, 11, 14, 15, 18). Our experience and clinical findings reinforce these guidelines. In addition, based on our experience operative treatment should be considered in cases in which correct diagnosis is delayed. In these cases it seems that healing capacity of medial malleolar stress fracture will be reduced by time as observed in five cases in our series that were initially treated conservatively before surgery.
This study has limitations. First of all, it is subject to all limitations of retrospective studies. Secondly, because no standardized evaluation scales or rating systems have been developed to assess medial malleolar stress fractures, we set our own criteria for the evaluation of results after surgery. Results were evaluated by the ability of the patient to return to sports, and by assessing the subjective symptoms of each patient. No objective functional measurements were made during the follow-up. Furthermore, because we were unable to include a group of non-surgically treated matched controls, we are not able to comment on patients who had been treated conservatively. However, we estimated that during this study period approximately 10 patients with medial malleolar stress fracture had been treated conservatively. About half of these 10 patients were athletes. Crucial factor for successfully completed conservative treatment was early diagnosis and strict restrictions of exercise. Although this study is to our knowledge the largest so far, the sample size may not be sufficient to draw definitive conclusions. Despite these limitations, the information from this study may be used as a guide in the treatment of especially athletes with medial malleolar stress fracture.
CONCLUSION
Early suspicion and heightened awareness of this special type of stress fracture combined with right diagnostic tools is the key to success in treating this rare injury. Especially the potential severe complications should be taken into consideration when determining the optimal treatment (9, 13, 14). Even though the treatment method in most cases with early diagnosis could be conservative, operative treatment is necessary in certain fractures. We recommend early surgical treatment in patients with discontinuation of cortical bone (i.e. increased risk of fracture dislocation). Nowadays, we also strongly consider prompt operative treatment in cases in which the correct diagnosis is delayed since we believe that these cases respond poorly to conservative treatment. In cases of elite athletes we agree with Shabat et al. and Steckel et al. who recommend early operative treatment because it most often leads to early recovery and return to full sports activities minimizing the risks of long convalescence period (14, 15).
Footnotes
ACKNOWLEDGEMENT
The authors acknowledge Timo Mikkola M.Sc. (Tech) for technical assistance.