
Abstract
Background:
Unstable antebrachium diaphyseal fractures in children are nowadays increasingly treated operatively by elastic intramedullary nailing.
Aim:
Aim of the study was to critically assess both radiological and functional outcome of antebrachium fractures treated by titanium elastic nail (TEN) in a pediatric cohort.
Material and Methods:
This retrospective study investigated 75 consecutive children, who were treated for antebrachium shaft fractures at Tampere University Hospital during the time period from January 2001 to December 205. All the fractures were classified according to OTA. Thirty-five children (mean age 12.3 years) were treated by TEN-nailing. Twenty four of the forearm fractures were instable, five were open, five were re-fractures and one had ulnar nerve deficit. In all but one patient both forearm bones were fractured. Twelve (34%) operations were managed by closed reduction, open reduction was needed in 23 (66%) patients. In 29 cases both bones were fixed with TEN-nail. In the four patients with re-fracture in both ulna and radius only the radius was TEN-nailed. In one case radius was fixed with TEN-nail and ulna with K-wire and in another case radius was fixed with TEN-nail and ulna with plate. Fracture pattern, mode of reduction, surgical approach, short- and long-term complications and outcome were recorded.
Results:
Twenty three (66%) patients achieved healing of the fractures without any limitation in range of motion. Twelve patients with postoperative complication were followed up 31–74 (median of 54) months. Eleven (31%) patients had minor postoperative complications and one (0,3%) patient had a Volkmann's ischemic contracture. Five of complicated patients had more than one problem. Immediate post-operative problems were noted in these five patients. At follow-up visits four patients complained of ulnar nail discomfort, two had neural symptoms. Additionally, three children suffered from re-fractures.
Discussion:
Despite various minor complications, TEN-nailing is considered suitable treatment for unstable forearm shaft fractures. Most of the problems were related to poor technical performance in nailing.
Keywords
INTRODUCTION
Forearm shaft fractures are common injuries in children. Estimates range from 6% to 10% of all pediatric fractures (1, 2). Most of the diaphyseal angulated fractures of the radius and ulna in children are treated with closed reduction and cast immobilisation (3). Conservative treatment for unstable forearm fracture may, however, lead to poor result in up to 50% of patients (4). Malalignments, more than 10 degree deviation in any direction, displacements of the bone or rotational failures can result in severely limited of motion (5). Dislocated antebrachium shaft fractures are recommended to be treated operatively with intramedullary nailing or in some cases plating. Elastic stable intramedullary nailing (ESIN), also called as Nancy nailing was, developed in France in the late 1970s. The results of ESIN nailing have been generally good (4, 6). The titanium elastic nail (TEN Synthes Paoli, PA, USA) set was developed in USA from the ESIN nail. In Finland TEN-nails are commonly used when treating dislocated shaft fracture in children. Titanium nail allows appropriate plastic bending to gain fixation in the bone, while retaining sufficient elasticity to resist unwanted displacement. TEN-nail offers semi-stable fracture fixation with rapid, biological healing and external callus. Removal of the nail is easy and risk of re-fracture is reported to be low (7). Also occurrence of other complications such as wound infection, skin irritation, nerve deficiency and rotational limitation has been reported only in 14.6–16% of the operated children (8, 9). We wanted to review and critically analyze the results of a cohort of Finnish children treated with TEN-nailing for dislocated antebrachium and find possible risk factors leading to complications.
MATERIAL AND METHODS
All children with antebrachium shaft fractures which were treated with TEN-nailing during the time period from January 2001 to December 2005 were included the study. This retrospective study group was collected by using two antebrachium fracture diagnoses and two operation codes. A total of 35 patients were found. Of these 20 (57%) were boys and 15 (43%) were girls. The age at inclusion of the children ranged was from 5.2 years to 17.4 years with a median of 12.3. In the boys age range was from 6.5 years to 17.4 years (median 12.3 years) and the girls' age range was from 5.2 years to 15.8 years (median 10.7 years). Sixteen (46%) of the injuries resulted from a fall, other fractures were related to skateboarding in seven (20%), gymnastic injury in three (9%), football and ice hockey accident in 2 (6%) patients. Other injury mechanisms were motorcycling, riding, roller-skating and trampoline, one patient in each case, and there was one hammer accident.
All the fractures were classified according to the OTA classification (10). There were two 22-A2 type fractures (simple radius fracture), 31 type 22-A3 fractures (a simple fracture of both bones) and two type 22-B3 fractures (simple wedge fracture, or wedge fracture of other bone). Indication for operative treatment was instability in 24 cases, re-fracture after earlier conservative treatment in five cases, grade I open fracture by Gustilo-Anderson in five cases and ulnar nerve palsy with stable forearm fracture in one case (Fig. 1). Thirty-three fractures were intramedullary fixed entirely by TEN-nails. In one operation TEN-nail was combined with plate and in another with K-wire. In four patients only radius was fixed with TEN-nail despite both bones being fractured. Only ulnar or radial fractures were TEN-nailed in one Monteggia- and one Galeazzi-fractures, respectively. In the operation theatre the patient was always positioned supine with the affected arm placed on a radiolucent table. The radial TEN-nail was always inserted retrogradely through a small skin incision and with blunt dissection by protecting the superficial radial nerve. The entry hole on cortex was drilled in proximal to physis and TEN-nail was advanced into intramedullary canal by hand. The ulnar TEN-nail was inserted in similar technique but positioned antegradely from volar proximal medial metaphysis. Both insertion points were verified under image intensifier before skin incision. TEN-nails were buried under the skin to reduce the risk of infection and cut off close to the bone in order to avoid tenting the skin and irritation. Operator was in either a consultant of pediatric surgery or pediatric orthopedics. Twelve (34%) operations were managed by closed reduction and open reduction was needed in 23 (66%) cases. Operation times varied from 20 min to 155 min. Patients without complication median operation time was 70 min and patients with complications 126 min. Two operations took place during night time, both of the resulted complications.

Dislocated antebrachium shaft fracture (22-A3) of a nine-year-old boy.
All patients were immobilised up to the first control examination (Fig. 2). Immobilisation with a long arm cast was used in fourteen patients, short arm cast in eleven patients and with a collar cuff in ten patients. Sports limitation was advised from six to eight weeks after operation. The TEN-nails were removed at an average of 25.6 (range five to 53) weeks after the insertion (Fig. 3). Patients with post-operative problems were followed up from 31 to 74 months, with a median of 54 months. The follow up included radiological and clinical evaluation. Functional outcome was assessed clinically by comparing the operated side to the healthy side.

The antebrachium shaft fracture five weeks after the TEN-nail fixation.

The antebrachium shaft fracture seven months after the TEN-nail fixation.
RESULTS
During the follow up time 23 (66%) fractures united without any problems. Five (14%) patients had short-term and seven (20%) had long-term problems during the follow up time. Complication rate was higher in patients over 10 years (67%, mean age 14.1 years) than in younger ones (33%, mean age 6.9 years). Nearly all fractures were type 22-A3 (Table 1). Five patients had problems immediately after operation (Table 1). The first patient had several complications, he was found to have median nerve neuropraxia already before operation and the neural symptoms were deteriorated postoperatively. At consequent follow up the symptoms persisted and the patient developed 20 degree supination deficit and finally a re-fracture resulted from a fall before removal of TEN-nails. The second patient suffered from post-operative paraesthesia over the dorsum of the thumb. However, this disappeared before second control and the patient recovered fully. The third patient with Monteggia fracture was treated by open reduction. The ulna was fixed with a TEN-nail and the radius was fixed dorsally with a single Kirschner-wire. Before the operation a partial ulnar nerve deficit was noted and postoperatively the ongoing pain over the ulnar nerve distribution was reported by the patient. In the first control visit the flexor contracture was noted, which led to a referral to the hand surgeons and a Volkmann's ischemic contracture was diagnosed. Consequently, the osteosynthesis material was removed by the hand surgeons concurrently with a flexor release operation ten weeks after the primary operation. During the follow up time the patient recovered fully. The fracture of the fourth patient was still unstable after the operation. The short-arm cast of the patient was changed to a long arm cast in the first post-operative day and finally the patient recovered without any additional problems. The fifth patient with complications had the ulnar TEN-nail malposition recognised on next day after the operation. However, the fracture united well without surgical intervention.
List of the individual complications, timing of the notification and OTA classification of the forearm fractures in pediatric patients treated operatively.
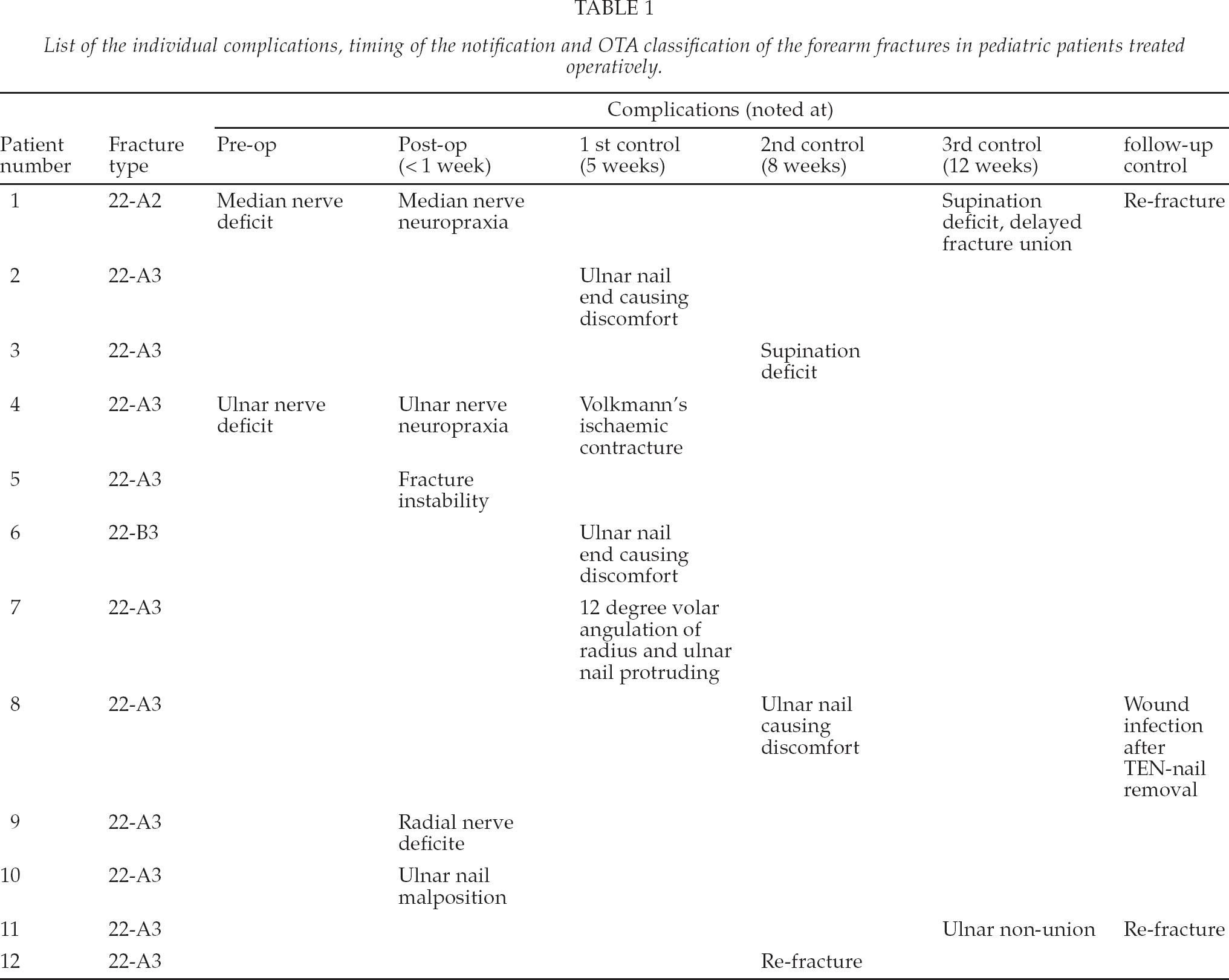
Three out of seven patients with long-term complications had pain caused by ulnar TEN-nail. Supination deficit was recognised in two patients. In one patient 12 degree volar angulation and protruding ulnar nail were noted five weeks after operation. The nail was removed and the patient wore a daytime short arm cast afterwards. Three patients had a re-fracture before removal of TEN-nails. The first patient's re-fracture occurred after first control following heavy tackling in football and the patient was operated on with new TEN-nails and casting. The second patient's fracture occurred three months after primary operation resulting from a fall. In follow up controls there was delayed fracture union. The third patient's radius was TEN-nailed and ulna was plated. During the follow-up controls ulna was poorly united. The re-fracture was treated by plating both the radius and the ulna. The patient with ulnar TEN-nail causing pain suffered also from wound infection after removal of TEN-nail. The infection was treated by oral antibiotics.
During the follow up time all these patients recovered well and the functional outcome was good, including the patient with Volkmann's contracture. Re-fractures were successfully treated by plating, casting and TEN-nailing.
DISCUSSION
Up to 85% of unstable antebrachium fractures in children can be managed by closed reduction and long arm cast immobilisation (11). Reduction without osteofixation leads frequently to limited rotation of antebrachium (12). Tarr et al. (1984) have demonstrated in their cadaveric study the following connection between structure and function; angulation between five and ten degrees at the midsaft of the antebrachium can lead to pronation deficit of 10% to 83% of normal as well as supination deficit of 5% to 27% of normal (13). Although residual angulation is generally well tolerated, there seems to be the consensus that angular deformity > 10 degrees and rotational deformity > 45 degrees are unacceptable (14, 15). Other indications for operative treatment include open, irreducible, pathologic or malunited fractures or fractures with a neurovascular compromise (6, 8, 16). Compared to plate fixation, which is widely used on adult antebrachium fractures, intramedullary nailing is considered more suitable for children (17). TEN-nailing is a minimally invasive procedure for unstable antebrachium fractures, and it offers definitive management, minimal cosmetic deformity and easy implant removal (9, 16, 18).
Although the TEN-nailing procedure is simple and widely used, minor complications are reported in up to 16 % of the patients (8, 9). Most common minor complications are skin irritation or infections at site of the nail insertion, transient nerve injuries, slight loss of reduction or motion and delayed unions (3, 9,19,). Major complications such as compartment syndrome, permanent nerve injuries and poor technical result leading to reoperation are seen less frequently (18).
During four years of the study we found 75 antebrachium fractures needing reposition under anesthesia. Half of these fractures needed operative fixation by TEN-nailing. Our practise with TEN-nailing differs from that of other centres in some respects. It seems that in our institution open reduction of dislocated shaft forearm fractures is performed significantly more frequently than in other centres. Open reduction was needed in two out of three patients. This rate was high compared with other studies, where the need for open reduction varied from 5 to 29% (1, 8, 20,21). Open or closed reduction is, however, reported to result in equal functional outcome (22). The mean operation time on all the study patients was especially long – even double as long as the operation time on similar patient group reported by Weinberg et al (2008) (23). Our patients with complications were operated on almost one hour longer than those without complications. The need for open reduction and low experience of the operator predominantly explain the long operation times. Ninety per cent of postoperative problems reported are caused by the sharp ends of the nails and require sometimes shortening after primary operation (20). Three of our patients had skin irritation at insertion of the nails. This problem could have been avoided by paying attention to suitable length of the nails (or using synthetic caps). The rate of superficial radial nerve injury is reported to be 1.2% (20). Two patients in the present study had transient radial or ulnar nerve injury. The nails were inserted in these cases via a small incision, which increases the risk of nerve irritation. Although the nerves recovered fully, this kind of injury can be avoided by visualizing the soft tissue and bone before inserting the nail (19).
Compartment syndrome which leads to contracture is reported in 6.7% patients undergoing intramedullary nailing (8). One of our patients suffered from Volkmann's contracture. This patient had Monteggia-fracture operated by radial K-wire and ulnar TEN-nail. Patients who undergo multiple passes with nail during closed reduction are at increased risk to develop soft tissue injury and compartment syndrome leading to Volkmann's contracture. According to Yuan et al. (2004) the fracture should be opened if closed reduction cannot be reached within three passes (24).
Nails require a sufficient diameter, 40% of the smallest diameter of the medullar canal, both for radius and ulna. Tension of the two nails against one another should be appropriate so the interosseus membrane is tensioned. The three-point support has to be achieved and nails must be inserted far from the fracture line (19, 25). One fracture in our patients was unstable after TEN-nailing. The diameter of TEN-nails was not proper. Another patient's TEN-nail was not proximally in intramedullary canal. These technical problems could have been avoided by testing the fractures under X-ray.
Prevalence of supination deficit rate is reported to be low (26). In our series two patients had transient supination deficit. During the follow up time both patients gained full range of motion. Reason for the supination deficit may be an insufficient anatomical reduction. Volar angulation problems are reported especially in patients treated only by casting. To prevent angulation, intramedullary nailing for both bones is recommended (27). In our series one patient with both forearm fractures TEN-nailed had volar angulation of radius and protruding ulnar nail. The patient recovered fully during the follow up time.
Re-fractures occur rarely after nailing, only in 0.5% of cases. In conservatively treated fractures re-fracture rate arises up to 10% (19, 20). It is generally accepted that the fracture should be consolidated before starting sports activity and nails should not be removed before four to six months and the fracture must be completely consolidated (20). In our study three patients had re-fracture. We always immobilize the operated arm with collar cuff or cast to prevent too early mobilisation. In one case, the patient started sports activity too early, before permission was given. One of the patients had unusual fixation combination of TEN-nail and plate. And the third patient with both radius and ulna TEN-nailed had delayed fracture union. Flynn et all (2010) operated two fractures of 149 with combined intramedullary nail and plate fixation without any complications (8). In our series both cases operated on with TEN-nail and plate or K-wire combination, i.e. rigid and semi rigid osteofixations led to poor outcome. We do not recommend the mixed use of different fixation methods.
In our study we found that complication rate was higher in patients older than ten years. Same results have been reported earlier (5, 8). Plate fixation might be better alternative than TEN-nailing for patients near adult age.
The question of routine elective execution of TEN-nail is controversial. Simanouvsky et al (2006) investigated retrospectively 143 children of which 11% were symptomatic before removal of TEN-nails. The execution procedure resulted minor complications in five patients (28). Raney et al (2008) reported the complication rate up to 34% for implant removal surgery in their evidence-based analysis (29). In our series all patients went through a removal of TEN-nails; no complications, however, occurred except one postoperative wound infection. In the future the need for routine elective execution of this procedure may be questioned. The problem may rise to some patients who later in adulthood need surgery for the TEN-nailed antebrachium; the implant removal is difficult or even impossible due to bone growth.
We found that the number of minor complications in forearm fracture treated operatively is higher than previously reported. In our study the problem free cases (66%) contain only fractures that did not have any postoperative radiological or functional impairment or discomfort caused by the nail. We believe that special attention to proper surgical techniques would reduce the rates of complications. Based on this study, TEN-nailing with proper technique is suitable treatment for school age children with unstable antebrachium fracture. It is a safe, minimally invasive technique which allows primary and definitive management of these fractures.