
Abstract
Introduction:
Resurfacing hip arthroplasty (RHA) has been suggested to provide an alternative to conventional total hip arthroplasty in younger, active patients. It seems to have an ability to conserve the bone mass on the femoral side. Some controversy exists regarding to the possible disadvantages of RHA and some of them are connected to poor femoral bone quality after surgery. Hence we wanted to study the bone mineral density changes 3 and 12 months after RHA.
Materials and Methods:
A total of 26 patients (22 men and 4 women, 28 hips) underwent a hip resurfacing arthroplasty. The mean age of the patients was 55,2 (range 38–69) years. Bone mineral density (BMD) of the proximal femur was measured by using the dual-energy X-ray absorptiometry (DXA) postoperatively and within 3 and 12 months from surgery. For analysis, we divided the femoral neck area into four equal-sized regions of interest ranging from the prosthesis to the trochanter level.
Results:
At three months follow-up the BMD changes varied between −5.1% (ROIC) and + 1.9% (ROIA), as compared with the immediate postoperative values. After one year follow-up the BMD changes were + 1.1% in the ROIA, + 5.4% in the ROIB, −3.9% in the ROIC and + 1.3% in the ROID. The changes in BMD were not statistically significant.
Discussion:
While there is still much debate and room for additional research in this topic, the results suggest that BMD is conserved in the femoral neck one year after hip resurfacing arthroplasty.
Keywords
INTRODUCTION
Resurfacing hip arthroplasty (RHA) is an alternative to standard hip replacement in young, active patients with osteoarthritis (1). The theoretical advantages of resurfacing include preservation of bone, in particular proximal femoral bone, which aids any possible revision surgery compared to a standard hip replacement (2). Despite obvious preservation of bone, as seen in radiographs, only a few studies that quantify proximal femoral bone loss postoperatively have been published.
Proximal bone resorption is a common phenomenon around femoral stems after cementless and cemented total hip arthroplasty (THA) (3 –7). Maintenance of the quality of proximal femoral bone is thought to require normal and physiological transfer of load to the proximal femur. Smaller stems and shorter stems as well as partial bone ingrowth into a proximal coating seem to be effective as indicated by the periprosthetic bone mineral density (BMD) (4,–5, 8).
Surface replacement of the hip is the most direct way to maintain load in the proximal femur. However, there is debate if the hip resurfacing arthroplasty offers a viable option to the standard THA. Carrothers et. al. just recently studied the modes of failure with 5000 Birmingham hip resurfacings. At a mean follow-up of 7.1 years, 182 (3.6%) hips have been revised because of fracture of the neck of the femur, loosening of the acetabular component etc. (9). Kishida et al (10) investigated bone density in the proximal femur in patients who underwent resurfacing or uncemented standard total hip replacement. The authors concluded that bone density increased in the Gruen zones of the proximal femur and in the femoral neck area in RHA.
Harty et al. measured the bone density of the femoral neck after resurfacing and compared the results with those from the contralateral unoperated hip (11). They concluded that bone density was similar in the operated and unoperated hip, although the bone density measurements were only performed postoperatively with no measurement preoperatively or during the “at risk” period. Recently Cooke et. al. showed that the bone density decreased from 6 weeks to 3 months postoperatively but was restored back to the preoperative stage at one year after surgery (12).
The aim of the present study was to study if bone mass under the femoral component is preserved and to bring additional information how bone mineral density of the femoral neck changes after resurfacing hip arthroplasty.
MATERIALS AND METHODS
For inclusion in this study, the patients had osteoarthtitis which could be operated using the hip resurfacing arthroplasty. The selected patients were relatively young and physically active. Most of the patients had grade two or three osteoarthritis according to the Kellgren-Lawrence classification (13) (Grade two n = 12, Grade three n = 15 and Grade four n = 1). Four different brands of prostheses were used since during the time of the study our clinical unit was testing these implants. A total of 26 patients (28 hips) received hip resurfacing arthroplasty either using Birmingham hip resurfacing system (Smith & Nephew UK, London, WC2N 6LA, UK.) (n = 5), Conserve (plus) (Wright Medical Technology, Inc. Arlington, TN 38002, USA) (n = 3), Cormet (Stryker, Kalamazoo, MI 49002, USA) (n = 6) or Biomet Recap (Biomet, Inc. Warsaw, Indiana, 46581-0587, USA) (n = 14).
The mean age was 55.2 (range 38–69) years at the time of the operation. We included 22 (24 hips, since two patients had both sides operated) men and 4 women on this study. The mean BMI was 27.8 (17.9–34.8). Operation was performed through a posterolateral approach with the standard operative technique. The surgeon decided which prosthesis was used in the operation. All the patients were allowed full weight bearing on the second post-operative day. Clinical and radiological evaluations were made at each visit, and any adverse events were registered. Kuopio University Hospital Ethics Committee approved the study protocol.
Periprosthetic BMD was measured using the Lunar DPX-IQ dual energy X-ray absorptiometry (DXA) instruments (Lunar Corp., Madison, WI, USA). During scanning, the patient was placed in the supine position on the scan table. In each scan the femur was kept in neutral rotation using the standard knee and foot supports to minimize the measurement errors. The scan window included soft tissues, bone and the metallic implant. The special orthopaedic software in use, version 1.2 (Lunar Corp.), automatically excluded soft tissues and the metallic implant from the analyses. Bone mineral content (BMC, g), areas (cm2), and BMD (g/cm2) were determined from four manually determined regions of interest postoperatively, at three months from surgery and finally at one year from surgery. The femoral neck was divided in to four regions of interest (ROI). Area A is located superolaterally, B superomedially, C inferolaterally and D is inferomedially. The areas range from the prosthesis to the base of femoral neck (Fig. 1).
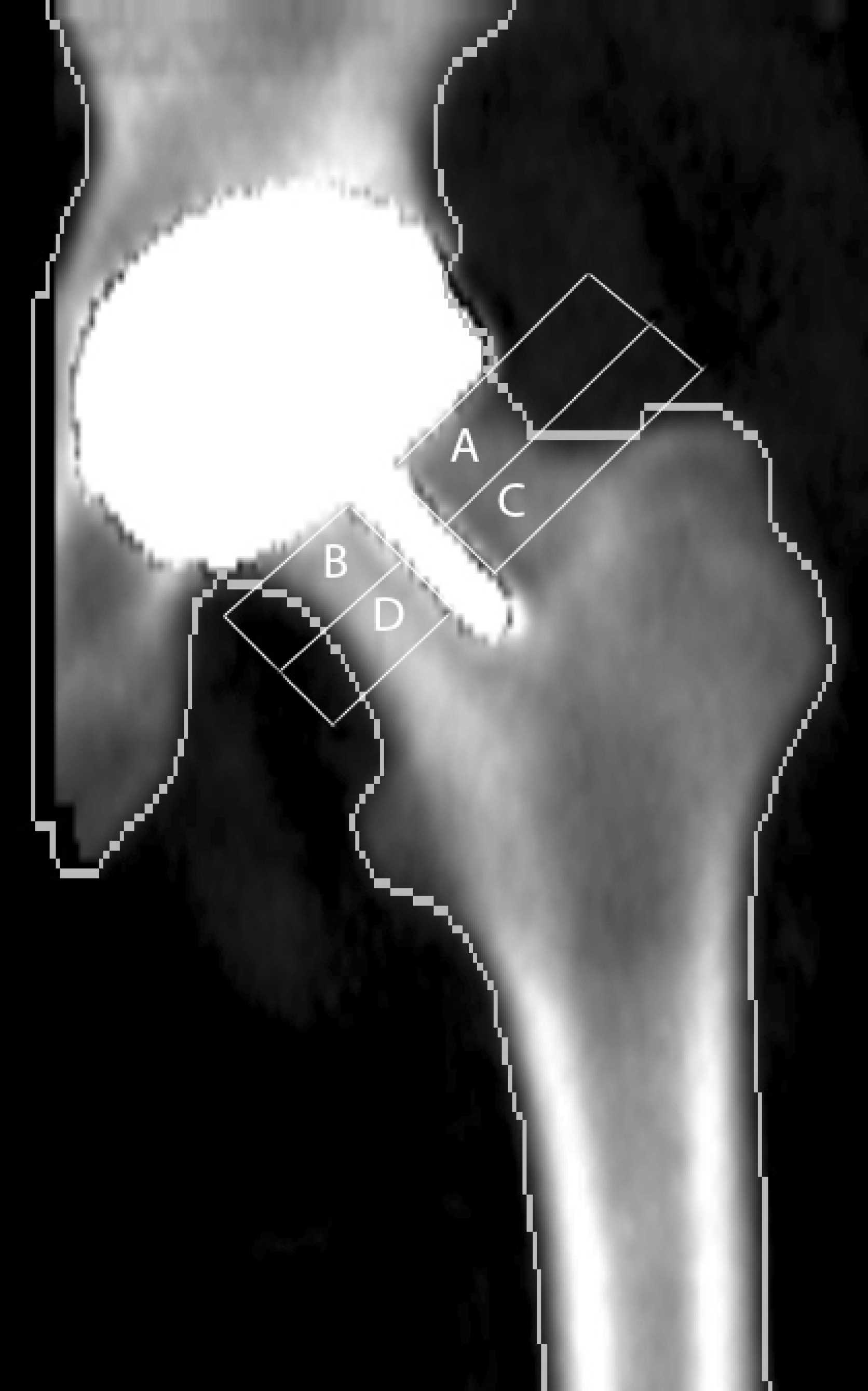
Picture of the four regions of interest in the femoral neck area.
For analysis, we also combined the proximal and distal ROIs i.e. the proximal ROI includes original ROIs A and B and the distal part from C and D.
Postoperative BMD changes were calculated by normalizing the BMD values against the immediate postoperative BMD. Any change was expressed as a percentage (%). In the statistical analysis, we used SPSS software, version 14.0 (SPSS Inc., Chicago, IL, USA). Friedman's test was applied to test the statistical significance of BMD changes during follow-up within the groups. The linear correlations of the periprosthetic BMD change with selected factors were also studied. All tests were 2-tailed, using a critical p value of 0.5.
RESULTS
There were no postoperative complications and all patients recovered without complications. The absolute and BMD values and percentual changes are shown in Table 1. Within three months follow-up BMD decreased in three ROIs and increased in one ROI. In ROI A increase was 1.9%, in B decrease was 1.5%, in C 5.2% and in D 2.7% respectively. At one year follow-up 3 out of 4 ROIs showed a slight BMD increase. There were 1.1%, 5.4% and 1.3% increases in ROIs A, B and D, respectively. The ROI C showed 3.9 % decrease at 1 year follow-up.
The mean periprosthetic BMDs (SD) after resurfacing hip arthroplasty during the one year follow-up time
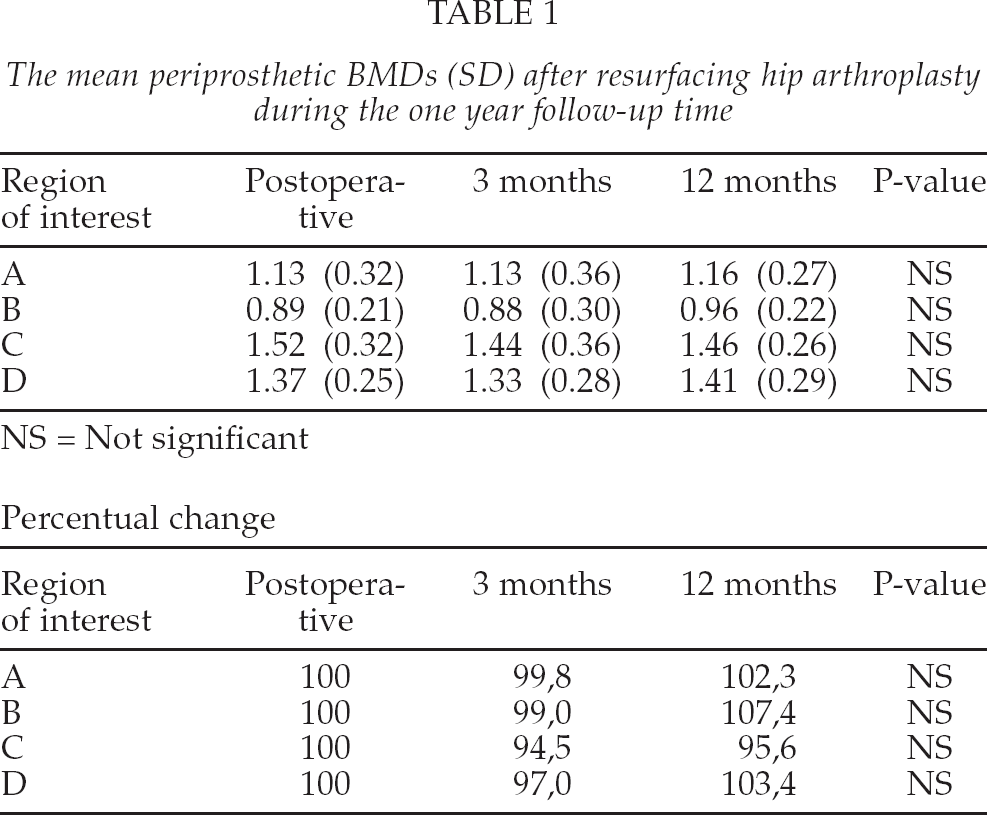
In the proximal ROI (A + B) there was a 0.6% BMD decrease at 3 months postoperatively, but at 1 year measurement the proximal part showed a 4.5% increase. In the distal ROI (C + D) there was a 4.4% and 0.7 % BMD decrease at 3 months and 1 year, respectively. All the changes were statistically non-significant (NS) (Fig. 2).
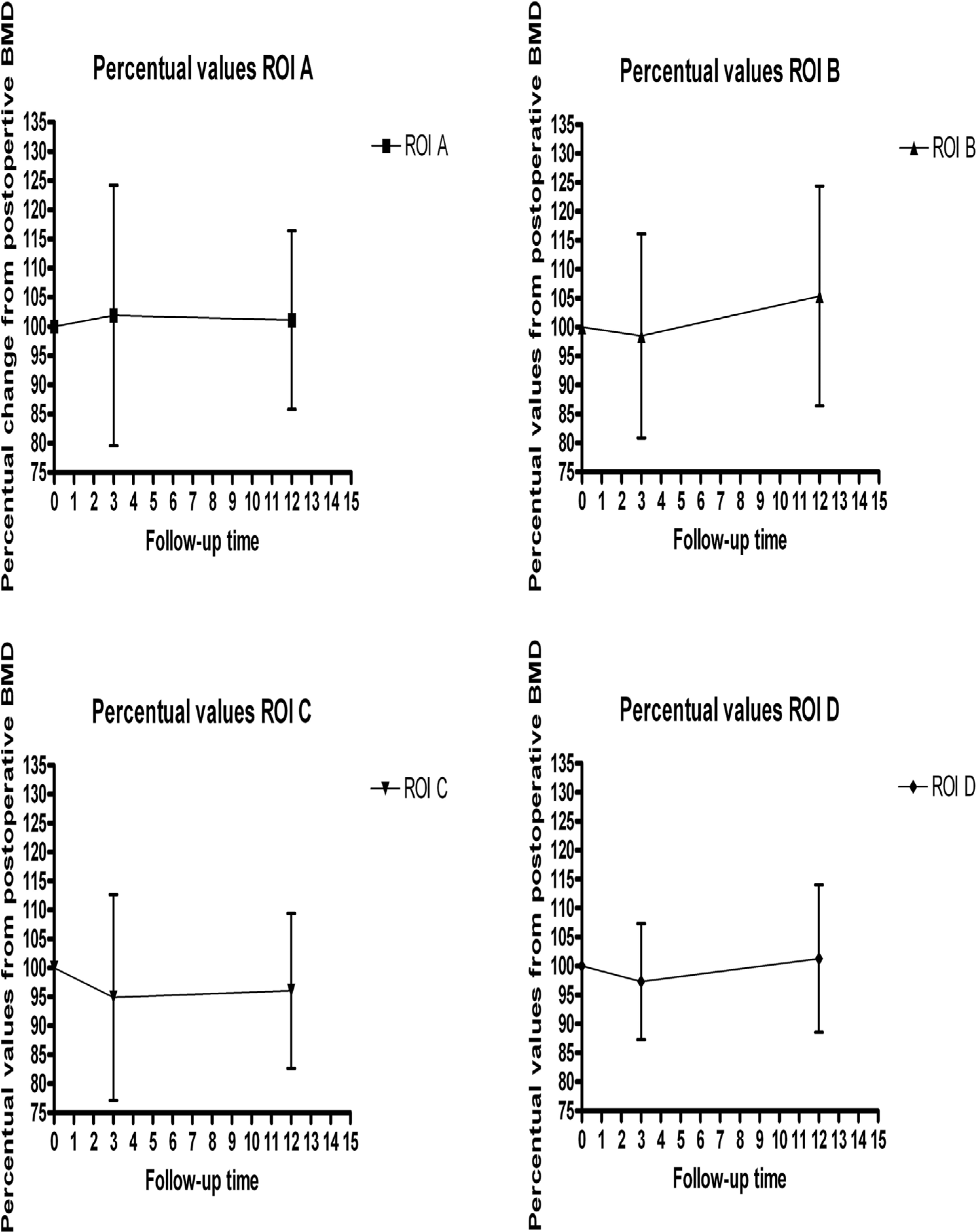
The percentual values from the postoperative BMD. Regions of interest A–D displayed indiviually. The changes between the groups were not statistically different.
DISCUSSION
In the present study BMD of the femoral neck was measured after resurfacing hip arthroplasty. DXA is a precise method of measuring small changes in the BMD around femoral components(14). We used immediate post-operative BMD as our reference baseline for all subsequent BMD measurements, since a proper positioning of the leg is then possible and bias from the limited range of motion can be avoided (4, 16). The changes were minor at three months and one year after the surgery. Thus it seems that RHA did not produce bone loss typical for conventional THA. After THA bone loss is most pronounced in the proximal part of femur (calcar) (3.4–18%) at three months after surgery. In several studies it continues up to one year(3,–4, 8, 15,16). However, the ROIs were not identical as measurements were made from the femoral neck area after the RHA and from calcar, trochanteric and diaphyseal areas after THA. Although are manually placed ROIs are located near the calcar region, the ROIs are not perfectly comparable.
Kishida et al. showed that using the Birmingham replacement system bone loss is less than in standard hip systems. Further, in some femoral areas BMD was even slightly increased(10). Cooke et al. came to the similar conclusion in their recent study(12). Our results are consistent with those of the previous studies.
The patients treated with hip replacement system demonstrated preservation of the BMD in the femoral neck area. This suggests that the transfer of load to the proximal femur was more physiologic after RHA than after THA (4, 12, 13, 17,18). When comparing BMD changes after RHA and THA Smolders et al. also found in their prospective randomised study better load transfer in the proximal part of femur. In the calcar area an increase of 5.2% was found after RHA whereas a typical decrease (18%) was found one year after THA (19).
Although RHA seems to preserve periprosthetic bone better than the standard THA, fracture of the femoral neck can still be a problem after RHA. However, fracture of the femoral neck is an early complication after hip replacement and it occurs mainly in female patients with osteoporosis (20, 21). Watanabe et al. conducted a finite-element analysis study and found stress shielding in the femoral neck beneath the prosthesis after RHA(21). They speculated that these abnormal stresses may predispose to fracture of the femoral neck and long-term loosening. The present study and other studies (1, 2, 9, 11, 12,22) could not confirm these results. Instead preservation of bone density was found one year after surgery. Thus, stress shielding, if it occurs at all, is a late phenomena after RHA and is not reason for early failure of RHA. Possibly, other reasons such as avascular necrosis (23), varus placement of the femoral component(24), notching of the femoral neck (25), small femoral heads in male patients, unseated components leaving femoral bone exposed, large cysts within the femoral head, and osteoporosis (26) contribute to this phenomenon. Carrothers el. al. discovered several modes of failure, which seem to be multifactorial but the exact etiology to these phenomena remains unclear (9).
Our study has some limitations. We had no control group including patients operated with a standard total hip arthroplasty or non-operative control group. However, our previous study has shown that the proximal femoral bone loss i.e. BMD decrease from −6% to −22% continue up to six months after uncemented THA (16). As compared to those findings the present results suggest that RHA tends to preserve bone mass better than conventional implants, even though the ROIs we used are not similar to conventional THA.
The limited statistical power relates to the small number of patients, similarly to the previous studies on this topic. We can not draw conclusions regarding different prosthesis types or implant sizes, since the number of individual prosthesis designs was small.
To conclude, consistent with the recent studies the hip resurfacing arthroplasty seems to preserve bone stock of the proximal femur. This may be related to physiological load transfer along the proximal femur after RHA. However, larger, prospective and randomised studies are needed to show whether favourable bone remodelling continues after one year.