
Abstract
Background and Aims:
Although endovascular stent treatment is increasingly used in infrainguinal atherosclerotic occlusive disease, outcome with focus on gender differences has not been reported in detail.
Material and Methods:
One hundred and twelve consecutive patients (67 [60%]) women, undergoing endovascular nitinol stent treatment of atherosclerotic lesions in the femoropopliteal segment were analysed concerning improvement in ankle brachial index (ABI), reinterventions, complications, amputation and survival rates up to 12 months after intervention. Risk factors for amputation and death were analyzed with logistic regression.
Results:
At presentation, women showed critical limb ischemia (CLI) more often than men (87% vs. 58 %; P = 0.001). After 12 months ABI had improved (from 0.40 ± 0.26 at baseline to 0.86 ± 0.22 after 12 months, P < 0.001), but 16 patients (15%) had been amputated and 27 patients (24 %) had died. After adjustment for age, diabetes mellitus and smoking, female gender was an independent risk factor for amputation (OR 9.0; 95% CI 1.1–76.5; P = 0.045).
Conclusions:
Stent treatment of lesions in the femoropopliteal segment had favourable effects on ABI and limb salvage. Treated women more often had CLI and ran a higher risk for amputation within 12 months than men. This might reflect failure of clinicians to adequately appreciate symptoms of atherosclerotic leg artery disease in women.
Keywords
INTRODUCTION
Occlusive disease of the femoro-popliteal arteries is associated with symptoms ranging from pain in the calf on exertion (intermittent claudication, IC) to critical limb ischemia (CLI) with pain at rest and ultimately ulceration and gangrene. Treatment options include a) conservative measures, with attention to medical risk factors, smoking cessation and exercise programmes, b) minimally invasive treatments such as percutaneous transluminal angioplasty (PTA) and c) surgical procedures such as femoro-popliteal bypass grafting (1).
PTA has been widely used in the treatment of femoro-popliteal disease for many years. However, medium and long-term results have been suboptimal with restenosis rates of 60–70 % with PTA alone in long lesions in the superficial femoral artery (SFA). The presence of occlusion rather than stenosis, lesion length, and the severity of run-off vessel disease all contribute to poor results (2, 3).
Stents are expandable metal mesh tubes which have superior patency than PTA alone when used in the coronary, renal and iliac arteries (4). In the treatment of SFA lesions several studies have investigated patency of balloon expandable stents. These stents have low flexibility and therefore run a high risk of deformation when placed in the SFA. Medium and long-term results with these stents are therefore not better than with PTA alone (5).
Self expanding nitinol stents, on the other hand, have higher flexibility and exert moderate to high radial force. Promising results have been obtained with placement of such stents in the SFA (6). Prospective randomised series, such as the Sirocco I and II studies showed 7 % restenosis rate at 6 months and 18% at 12 months (7, 8). Later studies have shown that higher restenosis rates are correlated to the length of the stented segment, the number of stents placed, and the stent brand used (9).
In a prospective randomised trial on patients with severe claudication or CLI with long (130 ± 60 mm) lesions, primary stenting in the SFA showed superior results to PTA with bailout stenting on restenosis rate, ankle brachial index (ABI) and walking distance at 12 months (3). Furthermore, 2-year results confirmed sustained benefit of primary SFA stenting compared to PTA with optional stenting (10). These and other promising results (11) have lead to an increase in stent treatment of SFA lesions.
The prevalence of both asymptomatic peripheral arterial disease (PAD) and severe leg ischemia such as CLI is higher among women than in men (12), whereas the prevalence of IC is higher in men. This might, however, reflect gender differences in disease presentation rather than in prevalence (13). Furthermore, the diagnosis of PAD is more often delayed in women who also have a poorer outcome after interventions (14). Female gender has also been reported to be associated with limb loss in infrainguinal endovascular PTA treatment (with secondary stenting in 26%) in CLI (15).
The aim of this study was to assess the outcomes of endovascular treatment of PAD in the femoropopliteal segment with nitinol stents in a Swedish county hospital. In particular, we aimed to detect potential gender differences with respect to treatment indication and results.
MATERIAL AND METHODS
POPULATION
We studied all 112 patients at Helsingborg County Hospital, Sweden, undergoing endovascular nitinol stent placement for atherosclerotic lesions in the SFA from January 1, 2006 to December 31, 208. The decision to use open or endovascular treatment was made based on patient characteristics such as age and lesion characteristics for example lesion length. During the same period 78 infrainguinal PTAs without stenting and 11 failed attempts to SFA-recanalization were performed at the hospital, and 37 patients (14[38%] women and 23[62%] men) were treated with bypass surgery. Treatment indication, ABI, symptom duration, co-morbidity, smoking habits, type of lesion (stenosis or occlusion), lesion length, run-off situation (1–3 vessels and presence or absence of vessels in the foot arcade), intraluminal or subintimal lesion passage, stent brand, number of stents, length of the stented segment, and concomitant medication were prospectively recorded before or at intervention. Minor and major early treatment complications were recorded up to 30 days after treatment. A complication was considered as minor if it did not influence the early treatment result and did not prolong hospital stay, for example a hematoma, a pseudoaneurysm or a nonsignificant embolisation.
Twelwe months after the intervention, follow-up data including ABI, results of duplex scanning after 1,6 and 12 months, need for open or endovascular reintervention, ulcer healing, amputation, and death were gathered from the Swedish Vascular Registry (Swedvasc) (16), and clinical records. Clinical outcome were reported as improvement in ABI, amputation-free survival and death. Risk factors associated with amputation or death was analyzed with logistic regression.
ETHICS
The study was approved by the Ethics Committe at Lund University (Ref. no. 2010/549) and was based on a quality follow-up registry in ordinary health care. In accordance with the ethical approval subjects had the opportunity to deny participation after a public announcement.
STATISTICS
Student's T test was used to evaluate differences in continuous variables, and the Chi2 test was used to evaluate differences in nominal variables between groups. Multiple logistic regression analysis was performed with all factors found to differ between groups in univariate analyses. Amputation-free survival was evaluated by Kaplan-Meier plots. Calculations were performed using SPSS18.0 (SPSS Inc., Chicago, IL, USA).
RESULTS
BASELINE DATA
From January 1, 2006 to December 31, 2008, 112 patients (67 [60%] women and 45 [40%] men) were treated with implantation of nitinol stents in the femoropopliteal segment
(Table 1). Mean age was 74.4 ± 10.8 years (75.8 ± 11.8 in women and 72.5 ± 9.1 in men; P = 0.13). The clinical indication for endovascular treatment was CLI in 84(75%) cases and IC in 28(25%) cases. Women were significantly more often treated for CLI (87% vs. 58 %; P = 0.001). Furthermore, there was a significant gender difference in baseline ABI; (0.33 ± 0.25 in women and 0.48 ± 0.25 in men; P = 0.004).
Baseline data in 112 patients undergoing endovascular stent treatment in the femoropopliteal segment. Mean ± SD or n (%). P-values calculated between genders.
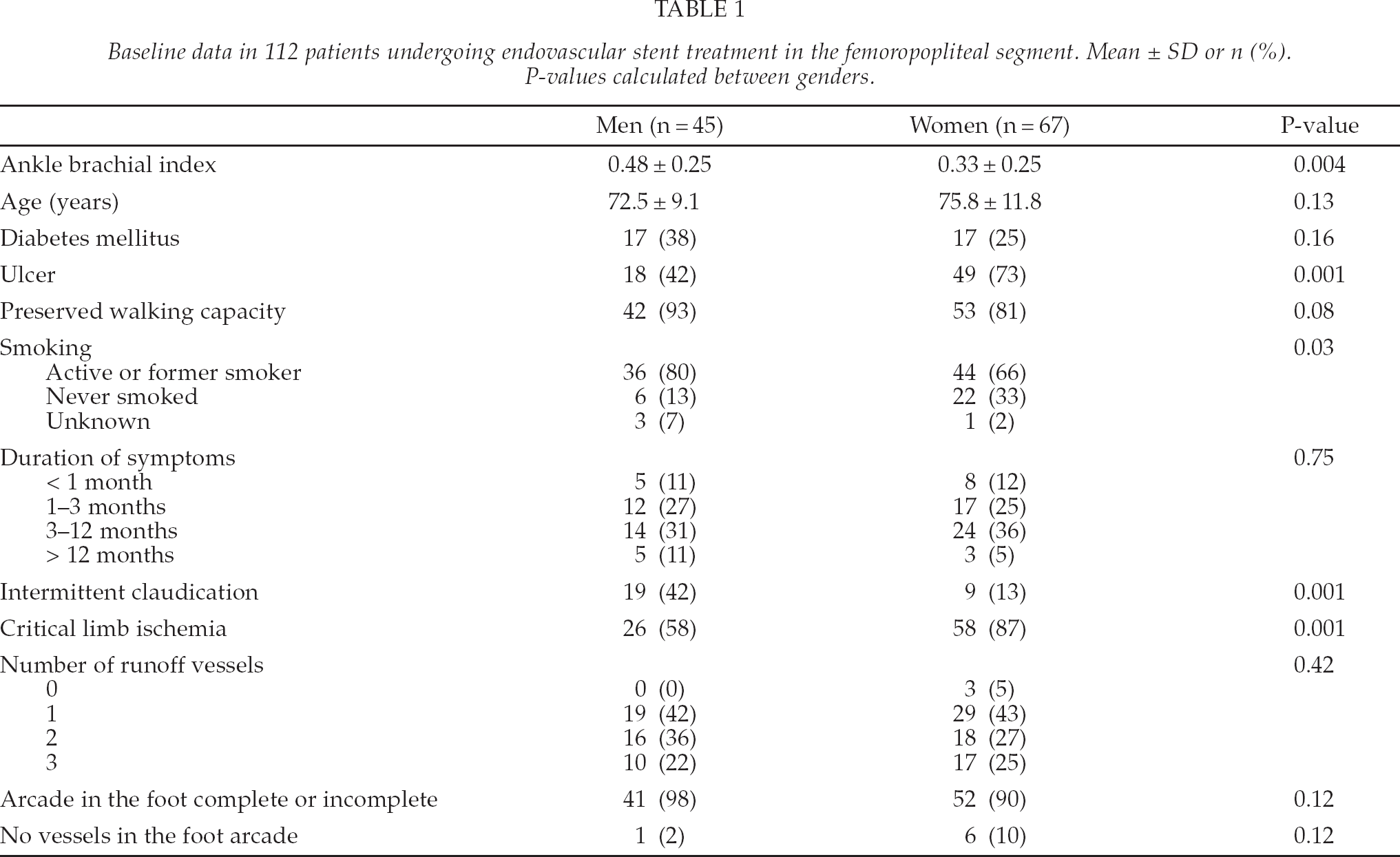
Before the endovascular treatment 95(85 %) patients had preserved walking capacity while 17(15 %) were not able to walk, and 67(69 %) patients had lower limb ulcers. Thirty four (30 %) patients had diabetes mellitus, 80(71 %) were active or former smokers, whereas 28(25 %) had never smoked. Smoking habits were unknown in 4(4%) patients. Men were more often active or former smokers than women (80% vs. 66 %; P = 0.03). The duration of symptoms was < 1 month in 11% and < 12 months in 54% of the cases.
ENDOVASCULAR PROCEDURE
Lesion length was 12.2 ± 8.7 cm (Table 2). The lesion was stenotic (i.e > 50 % lumen diameter reduction) in 50(45%) cases and occlusive in 62(55%) cases. The SFA-lesions were successfully treated with nitinol stents in all 112 patients, after which 58(52 %) patients received clopidogrel in addition to treatment with acetyl salicylic acid.
Technical procedure data in 112 patients undergoing endovascular stent treatment in the femoropopliteal segment. P-values calculated between genders. SFA = superficial femoral artery.
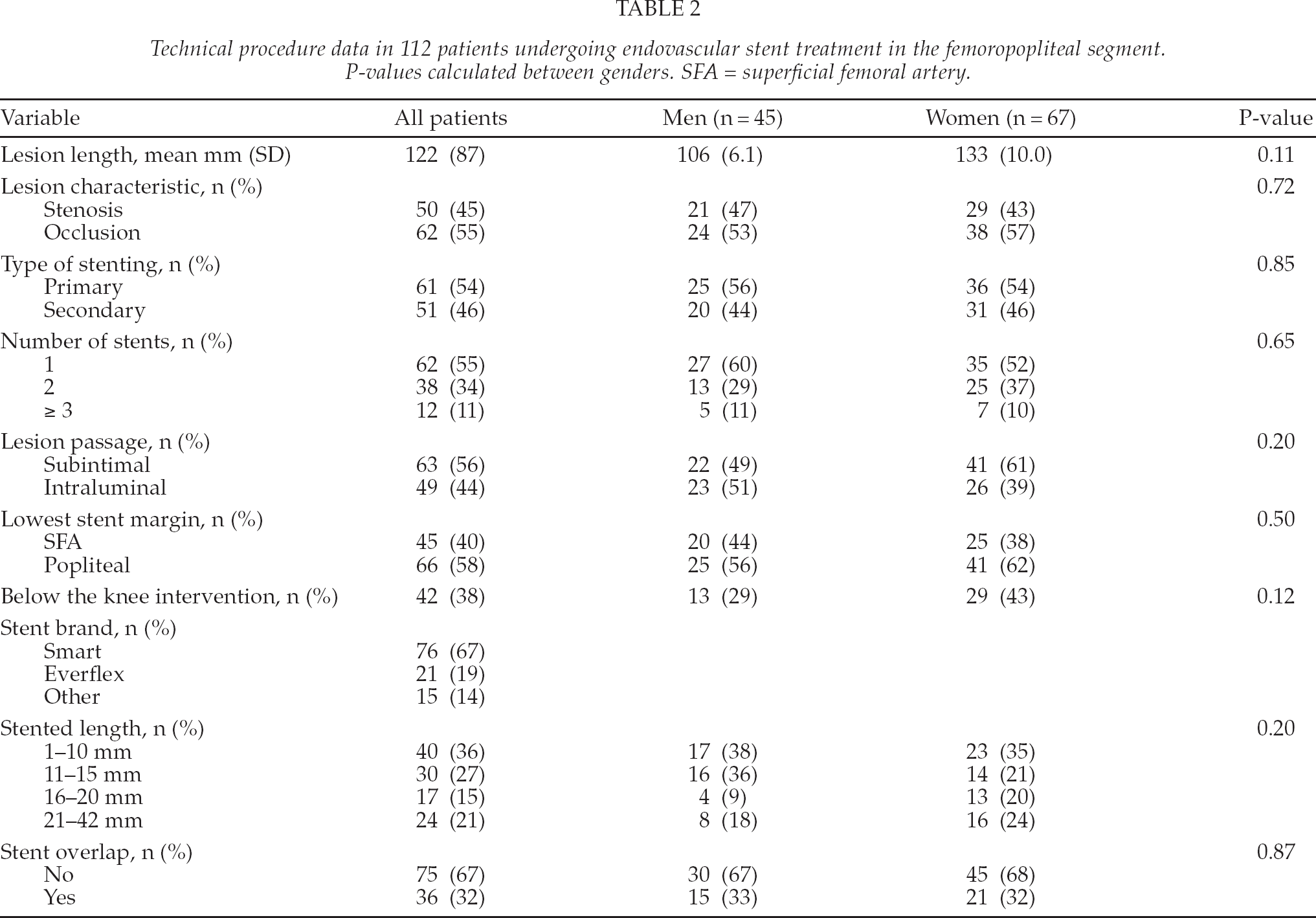
There was no significant gender difference concerning run-off vessel situation, whereas women tended to have longer lesions (13.3 cm vs. 10.6 cm; P = 0.11), and tended to more often be treated with below the knee interventions (43% vs. 29%; P = 0.12).
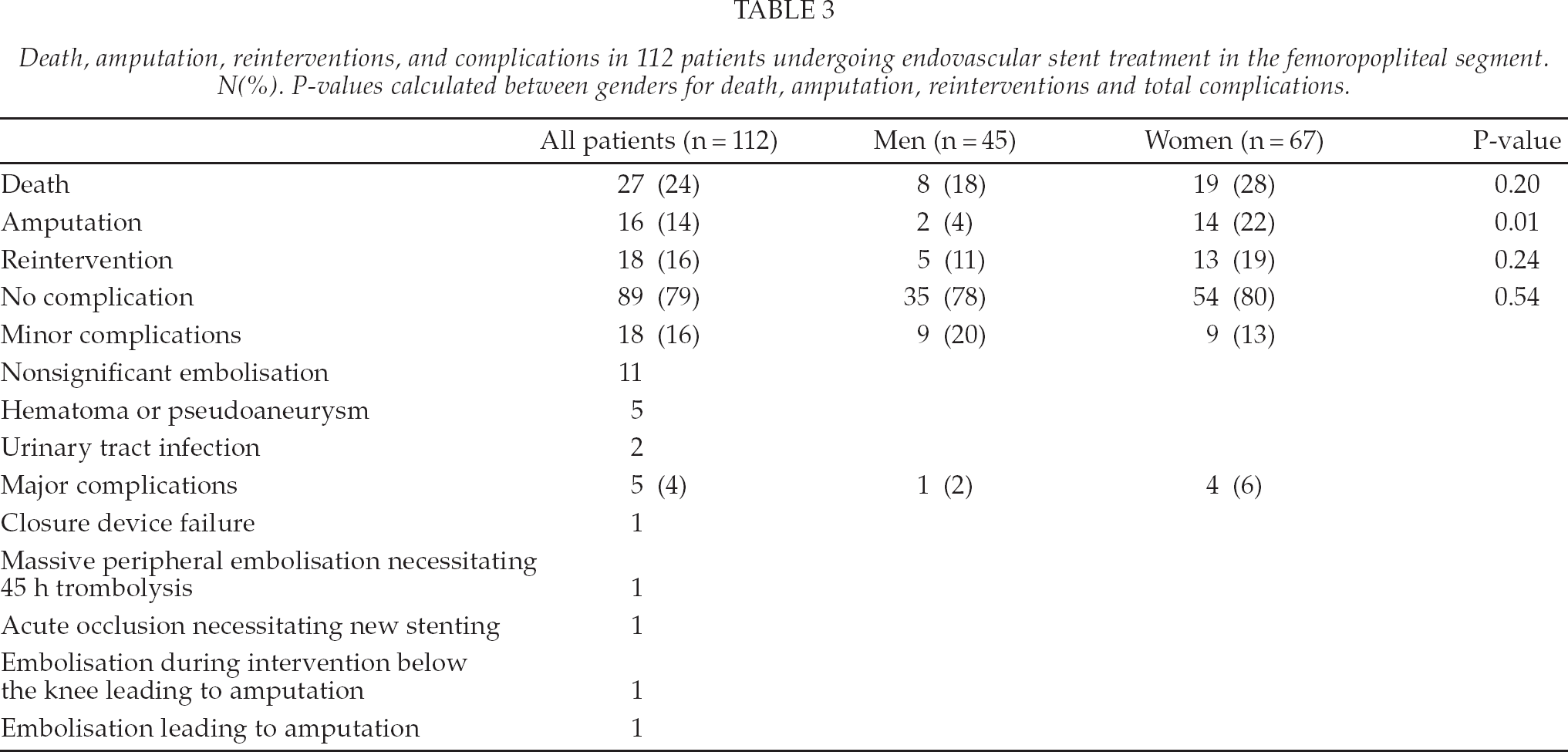
There was at total number of 23 complications (Table 3), of which 18 were considered as minor and five as major. In three of the cases with major complications, the procedure-related clinical course was uneventful, but in two cases a major procedure-related complication led to subsequent amputation.
Death, amputation, reinterventions, and complications in 112 patients undergoing endovascular stent treatment in the femoropopliteal segment. N(%). P-values calculated between genders for death, amputation, reinterventions and total complications.
TWELVE-MONTH FOLLOW-UP
Within the 12-month follow-up period 27 patients died, (19[28%] women and 8[18%] men [P = 0.20]) (Table 3). All deaths occurred within the group treated for CLI, and none was related to procedural complications. The 30-day mortality rate was 4/112(4%), two men and two women with a mean age of 71.5 years.
Sixteen patients (14[22%] women and 2[4%] men [P = 0.1]) underwent amputation. All had been treated because of CLI, in this group limb salvage rate was 82 %. Among the 16 amputated patients, four were amputated within 10 days, another five within 60 days, another two within 90 days and the remaining five within 300 days. The 30 day amputation rate was thus 4/112(4%). Three amputations were only digital and followed by an uneventful course. Duplex were performed only on 5/16 amputated patients, and showed open SFA-stent in four cases and occlusion in one case. The overall amputation-free survival at 12 months was 67 %, significantly higher (P = 0.03) in men (80 %) than in women (58%) (Fig.1).
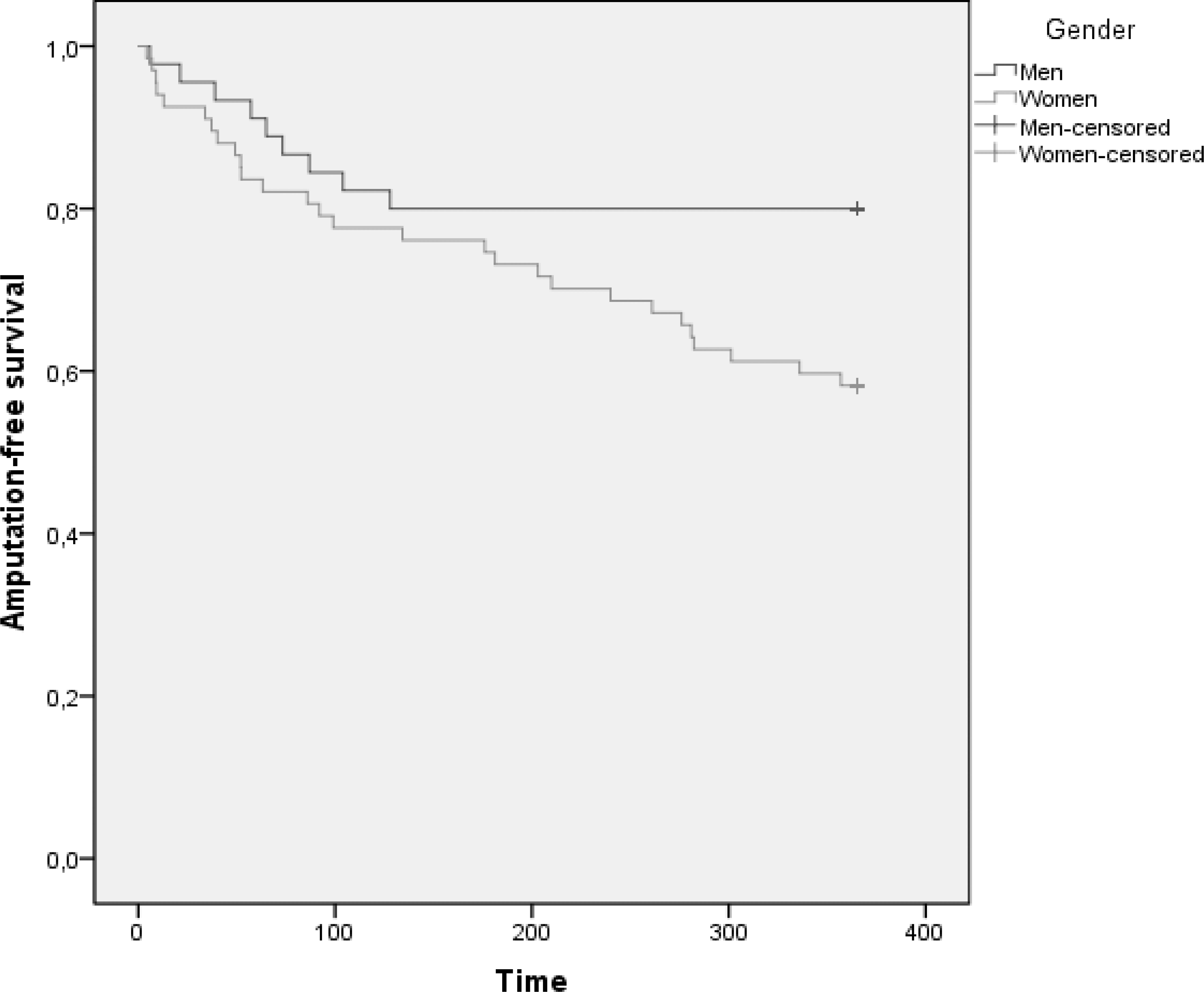
Kaplan-Meier plot of amputation-free survival in 45 men and 67 women undergoing endovascular stent treatment in the femoropopliteal segment.
Reinterventions were done in 18 cases, 13(19%) women and 5(11%) men (P = 0.24).
The cause of reintervention was CLI in 16 and IC in two cases. All reinterventions were performed with endovascular methods and led to significant clinical improvement in all cases but one. Patients undergoing reintervention did not run an increased risk for amputation (P = 0.78) or death (P = 0.16).
Duplex scanning was performed in only 25% of the patients, a number to small to permit assessment of outcome with this method. Data on ABI was obtained in 104 cases before treatment, in 90 cases after one month and 53 cases after 12 months, and showed an overall ABI improvement from 0.40 ± 0.26 at baseline to 0.90 ± 0.14 after one month (P < 0.001), and 0.86 ± 0.22 after 12 months (P < 0.001). The improvement in ABI was significant (P < 0.001) in both genders at one month (Δ value 0.53 ± 0.26 for women and 0.44 ± 0.22 for men) and at 12 months (Δ value 0.50 ± 0.31 for women and 0.35 ± 0.27 for men).
A comparison of the 14 women who subsequently underwent amputation and the 52 who were not amputated showed that the former group had lower ABI (0.17 ± 0.23 vs. 0.36 ± 0.25; P = 0.014), and tended to have more ulcers (13/14 vs. 17/52; P = 0.055) at baseline. Six of 27 women available for follow up of ABI at 12 months had IC and 21 had CLI at baseline, but there was no difference in ABI at 12 months between these groups (IC 0.80 ± 0.21 and CLI 0.86 ± 0.16; P = 0.50).
No technical procedural factors such as lesion length, occlusion vs. stenosis, type of stenting (primary or secondary), number of stents implanted, lesion passage (intraluminal or subintimal), lowest stent margin, stent brand or run-off vessel situation influenced the risk for subsequent amputation when tested in multivariate models.
Among women, those undergoing additional below the knee interventions ran increased risk of amputation (OR 7.1; 95% CI 1.8–28.8; P = 0.006) compared to women undergoing endovascular intervention in the SFA alone.
Associations between female gender and amputation or death were further analyzed with multiple logistic regressions. When controlled for age, diabetes mellitus and smoking, female gender was still an independent risk factor for amputation (OR 9.0; 95% CI 1.1–76.5; P = 0.045), but not for death (OR 2.1; 95% CI 0.7–6.2; P = 0.18). Diabetes mellitus increased the risk of death (OR 3.9; 95% CI 1.3–11.3; P = 0.014), but not the risk of amputation (OR 1.8; 95% CI; 0.47–6.8; P = 0.39). Smoking did not increase the risk for amputation (OR 0.65; 95% CI 0.17–2.5; P = 0.53) or death (OR 2.2; 95% CI 0.66–7.3; P = 0.20).
DISCUSSION
The most important findings in our study were that women more often than men had CLI when undergoing SFA-stent treatment and that female gender was an independent risk factor for amputation, when controlled for age, diabetes mellitus and smoking.
Amputations were in 12 of the 16 cases performed on patients with very severe CLI with ulceration or gangrene already at baseline. Stent patency could be assumed before amputation in 13 cases, whereas stent occlusion was confirmed in one case and information is lacking in the remaining two cases. This indicates that the need for amputations might reflect failure to reverse an already severe ischemic damage at presentation rather than loss of patency of endovascularly treated segments. Limb loss despite patency of endovascularly treated segments has also previously been reported to be the most common cause of limb loss (17). Mortality within the 12 month follow-up period was 24 %, all deaths occurred among patients with CLI. This 1-year mortality is well comparable to what's reported in another recent study of CLI patients in southern Sweden (18).
Five major procedure related complications (4.5 %) occurred, two of which lead to amputation within 10 days in patients with advanced CLI. The clinical course in the other patients suffering major complications was uneventful. This complication compares well with the 7 % rate of significant complications recently reported for SFA recanalization in diabetic patients with CLI (19).
The reintervention rate of 16 % in this study is also well comparable to the 22 % reported after SFA angioplasty and stenting (20). Furthermore, it is interesting to note that the reinterventions done in 18 of our patients (without significant gender difference) led to significant clinical improvement in all cases but one, and were not associated with increased risk for amputation or death.
Since duplex scanning during follow-up was only performed in 25 % of patients in our study, patency rate of the SFA stents was not possible to evaluate in detail. However, the significant improvement of ABI in both CLI and IC patients of both genders and the limb salvage rate of 82 % in the CLI group suggests a high degree of stent patency and efficiency of treatment.
Previous studies have shown an increased restenosis rate with increasing number and length of stents implanted in the SFA (2, 8), in patients with occlusions rather than stenosis, and in those with a poor runoff vessel situation (2, 8). A recent study on a similar clinical material suggests that a smaller stent diameter depicts poorer outcome (21), whereas in our study, none of the technical procedural data significantly influenced the patient's risk for amputation or death in a multivariate model. As the study was insufficiently powered to detect such differences, no firm conclusions can be drawn from this finding, however.
As mentioned above, women had a more advanced PAD than men when undergoing endovascular treatment of SFA disease, as reflected by a higher proportion of CLI. Accordingly, they had a less favourable outcome with a higher risk for amputation during the one year follow-up. Several reasons for these findings could be considered, as for example gender related differences in disease duration. Women with cardiovascular disease have been shown to run a risk for delay of diagnosis and therefore experience poorer outcome after intervention than men (14). They might also arrive later to medical care for cardiovascular disease, as suggested by the fact that women with myocardial infarction arrive later to hospital, and have both more severe infarcts and higher mortality than men (22). In our study, however, it was impossible to judge from the hospital records whether women had experienced a longer duration of symptoms before referral for endovascular treatment.
Failure of clinicians to correctly identify symptoms of PAD in women is another possibility to be considered. This can be due to the fact that perception of PAD symptoms is different in the two genders, with women more often accepting walking difficulties as a part of normal aging (13). CLI is a stage of PAD which is not so easy to neglect as IC, however, which might help to explain the predominance of women with CLI in both our and other materials. For example, data from the national Swedish vascular registry (Swedvasc) (16) corroborates that women more often undergo infrainguinal revascularisation due to CLI and men more often due to IC. No such increased frequency of amputations in women as in this study, on the other hand, was seen in a 10 year registry of all amputations performed on patients in southern Sweden (23), a finding that might reflect possible selection bias in the present study.
Possibly, gender differences in the quality of medical treatment might also contribute to differences in results of PAD treatment (24), and it has been shown that women with intermittent claudication receive less appropriate medical care than men (24). As judged from hospital records, this was not the case in our patients, however.
Technical factors might also influence gender differences in results of endovascular treatment. For example, it has been shown that women may have more narrow vessels than men (25). In the present study no significant gender differences were demonstrated considering technical, procedural, or anatomical details such as number of runoff vessels at baseline, except for a trend towards longer lesions and more below the knee additional procedures in women. The overall complication rate was also equal in both genders, except for a non significant trend towards men having more minor complications and women having more major complications (P = 0.45). In summary, we found no clear evidence indicating that SFA-stent treatment is less technically suitable for women.
The present study has several limitations, however. It is based on a registry comprising a rather small number of patients, increasing the risk for selection bias. Furthermore, patients were included in the registry after stent placement over the SFA lesion had been performed, and cases with failure to pass the lesion were therefore not included.
Although this study shows excellent ABI improvement and a favourable limb salvage rate encouraging the use of stent treatment in SFA lesions, it raises concerns about both the efficacy of the method in women with severe CLI and the ability of the health care system to adequately appreciate symptoms of PAD in women. Further studies on these issues are therefore justified.
Footnotes
ACKNOWLEDGEMENTS
This study was supported by grants from the Gorthon foundation, the Ernhold Lundströ Foundation, Research Funds at Skåne University Hospital, the Albert Påhlsson Foundation, the Hulda Ahlmroth Foundation, and from the Swedish state under the LUA/ALF agreement.
Stefan Bergman, Anders Gottsäter and Peter Qvarfordt have nothing to disclose. Hans Lindgren has received compensation according to a proctoring and training agreement with ev3 Nordic AB and William Cook Europe ApS. These sponsors had no involvement in any part of the study.