
Abstract
The treatment options for infra-renal arteriosclerotic occlusive (ASO) vascular disease have never been more varied. The history of open revascularization procedures now exceeds 60 years. This represents three generations of vascular surgeons, the most recent of whom have witnessed more than 30 years of endovascular surgery development and dissemination. Both open and endovascular treatments should be considered mature; moreover, we are improving our understanding of the strategies and tactics that lead to the clinical application of one approach instead of the other. There are other important factors in the choice of a treatment modality to be used for a specific patient. Prime among these is evolving patterns of occlusive disease and the increasing severity of arterial calcification.
INTRODUCTION
The risk factors under whose influence arteriosclerotic occlusive lesions develop are now better understood and also more susceptible to modification and control. The implementation of smoking cessation, control of arterial hypertension and diabetes management plus new medical management advances such as antiplatelet drugs and cholesterol-lowering drugs with their pleiotropic effects have changed the diseases that we treat. The incidence of large vessel occlusive disease and superimposed long segment thrombosis in the aorto-iliac and femoro-popliteal segments so common in the mid-20th century appears to be declining. In contrast, the epidemic of diabetes has brought with it neuro-ischemic ulceration and a growing population of patients with infrapopliteal arterial occlusive disease whose management has increasingly attracted the attention of endovascular practitioners. European and American investigators have comprehensively addressed these diverse arrays of occlusive disease and have produced evidence-guided classifications systems for disease severity scoring and treatment practices in the 2000 and 2007 TASC documents (1, 2). It is against this background of an evolving pattern of arteriosclerosis and newer medical management that we synopsize the current status of open surgical revascularization below the renal arteries with special attention to bypass grafts.
THE AORTO-ILIO-FEMORAL SEGMENT
Aorto-iliac and aorto-femoral bypass grafting (ABFB) both became popular at about the same time as endarterectomy (TEA) (3) of the same surgical territory in the early 1950s; today endarterectomy has become a rarity (4). Early after the introduction of balloon angioplasty ABFB continued to find favor because of iliac re-stenosis (TASC l). Since the introduction of arterial stents, however, predominately the balloon-expandable type (5), ABFB is performed less frequently, partly because stents provide more effective and durable arterial remodeling but also because symptomatic aortic athero-thrombotic disease is less prevalent.
In our practice several disease characteristics influence the use of specific surgical techniques. Arterial calcification is increasingly more common in the last decade and influences anastomotic technique at both the aortic and femoral termini (6). Severe calcification makes it difficult to find “soft spots” in the aorta for placement of the proximal clamp and a site for the aortic anastomosis. Often the aorta just below the renal arteries is soft which affords vertical or, more often, horizontal clamping; supra-renal clamping is occasionally required and, in this instance, the clamp is usually applied vertically. More often than not there is neither a place for the distal clamp nor a place for the graft anastomosis. Clamp placement across a calcified artery may lacerate the aorta and when the clamp is removed the ensuing aortic bleeding may be difficult to control. We use one of three techniques to address the calcified plaque at the distal clamp site. First, the plaque can be gently but firm squeezed and compressed with the fingers prior to clamp placement; second, the outflow may be controlled (sometimes only partially) by camping the common iliac arteries and third, an intraluminal occlusion balloon can be placed after the aortotomy is completed. A partial or complete aortic endarterectomy is almost always necessary if the calcified plaque restricts needle passage and construction of the proximal anastomosis
Brewster has described the circumstances under which end-to-side versus end-to-end aortic anastomosis is selected (4). As diabetics tend to have more internal iliac artery occlusive disease so in recognition of the desirability of maintaining in-line aortic continuity we prefer end-to-side anastomoses. The body of the bifurcated graft should be placed as high as possible and kept as short as possible; this places the graft bifurcation well above the native aortic bifurcation. We believe that the best way to avoid aorto-duodenal fistula formation is to separate the graft and the proximal anastomosis from the duodenum and the intra-abdominal contents. If it is not possible to plicate the retroperitoneum over the end-to-side anastomosis to achieve complete separation we recommend placing omentum between the graft and the abdominal viscera.
Not all sick patients with multiple co-morbidities can be treated with endoluminal revascularizations. Therefore, the morbidity of open bypass surgery is mitigated in several ways. If the patient has a wide costal angle, a transverse incision that divides the rectus abdominus muscles produces less respiratory stress than the vertical midline incision. Many prefer the left retroperitoneal approach which provides exposure equivalent to the midline incision (7) with added benefits of reduced ventilatory challenge and the earlier return of GI tract function post-operatively. Three minor limitations, however, are the lack of access to the right renal artery, the usual need to divide the inferior mesenteric artery and the occasional eventration of the flank. These disadvantages are further balanced by the relative ease in gaining access to the supra-renal aorta if a more proximal clamp placement becomes necessary. If only one leg requires reconstruction, the extent of the bypass can be minimized by making a small flank incision and using the common iliac artery as the inflow site; the even more distal external iliac artery is occasionally used if there are no occlusive lesions above the chosen inflow level. Neither of these more distal inflow sites precludes the possibility of revascularizing both legs by adding a femoro-femoral graft.
If an even less stressful open procedure is required there are two popular options; the axillo-bifemoral bypass (AxBFB) (8) and the femoro-femoral bypass (FFB) (9). The minimally invasive nature of the AxBFB derives from the use of subcutaneous tunneling of the graft. This promotes early ambulation of the patient within 24 hours or less post-operatively. If necessary, the procedure can be performed under local anesthesia. Using the prefabricated ringed polytetraethylene (PTFE) graft the three anastomoses can be effectively completed in two hours or less. We usually reserve AxBFB for patients with limited life expectancy and multiple co-morbidities. Its wider application is constrained by the possibility of restricted inflow from the subclavian artery and the eight mm diameter of a long graft that may reduce distal flow volume and pressure. It is, nevertheless, a highly useful revascularization for the appropriate patient. Femoro-femoral bypass has many proponents but in the infrequent instances we use it, the standard configuration is modified. Our preferred configuration is to achieve inflow from the distal external iliac artery (“donor”) through a small hernia-type retro-peritoneal incision. The tunnel is placed in the Space of Retzius with the graft exiting to the recipient artery under the inguinal ligament. In addition to being more resistant to infection and thrombosis, this technique avoids the awkward supra-pubic tunnel that not infrequently requires proximal SFA inflow and outflow to avoid graft kinking.
Thoraco-bifemoral bypass (Th-BFB) (10) is, in our opinion, under-utilized for patients that require a robust and durable revascularization but have restrictions to the standard aorto-femoral reconstruction (e.g, the “hostile abdomen”) or for the management of the infected aortic bypass. The relative morbidity of a small T-7 or 8 thoracotomy is offset by the substantial aortic inflow from the descending thoracic aorta, a shorter graft and an extra-anatomic tunnel that requires only a small flank incision. The cross femoral tunnel can be placed either subcutaneously or in the Space of Retzius.
ILIO-FEMORAL ENDARTERECTOMY
Changing risk factors and clinical populations have manifested a pattern of ASO disease that was uncommon before the explosion of diabetic vasculopathy. Whereas the absence of palpable or diminished femoral pulsations resulted from aorto-iliac ASO and thrombosis, focal femoral calcification and coral reef plaques formation is not only much more common but also diagnosed and treated differently.
When the femoral artery is palpated, not only is there no discernable pulse but the artery feels hard; surprisingly, the distal external iliac artery (EIA) pulse above the inguinal ligament is normal and a femoral bruit is often auscultated. Two arteriographic patterns are commonly observed; the artery is densely calcified and non-compliant and consequently is non-pulsatile; nevertheless, the arteriographic appearance demonstrates a normal patent luminal conture. The second more common pattern demonstrates a “coral reef plaque” essentially confined to the common femoral artery with normal runoff into the superficial femoral artery (SFA) and a larger deep femoral artery (DFA) than one usually sees on diabetic vascular disease. This lesion with disease-free EIA inflow appears to be distinctive to the diabetic.
Just as the plaque is localized so too is the revascularization. It must be emphasized that this lesion is, however, not readily amenable to endoluminal therapy. The bulky calcified plaque occupies all or nearly all of the arterial lumen so that neither atherectomy nor angioplasty/stenting will re-establish a normally functioning ilio-femoral segment. Open endarterectomy and patch angioplasty through a short inguinal incision (which can be performed under local or regional anesthesia) restores pulsatility and, if the SFA is patent, palpable popliteal pulse; in a minority of patients a bridge graft from the distal EIA to the femoral bifurcation will provide an equivalent result. We have repeatedly observed that ilio-femoral TEA will sufficiently augment pedal perfusion to enable healing of Grade 1 and 2 foot ulcer without the need for distal bypass or establishment of a pedal pulse. If, however, further revascularization is required a shorter bypass with an inflow site more distal to the common femoral artery has been enabled. After pedal bypass, the ilio-femoral TEA/patch angioplasty operation has become our most commonly performed open revascularization for diabetic ulceration.
HYBRID PROCEDURES
The vascular surgeon is favorably positioned to combine disparate procedures. In the aortoiliac segment inflow can be enhanced with a peroperative balloon angioplasty while the femoral outflow is optimized with a surgical endarterectomy that removes femoral plaque and widens the distal outflow track. For the inflow angioplasty we commonly stent the dilated artery to secure the inflow channel so as not to jeopardize the distal revascularization/endarterectomy. Piazza et al. (11) have used femoral TEA technique together with proximal stent angioplasty as a substitute for aorto-femoral and ilio-femoral bypass. It also fosters careful attention to reconstruction of the femoral bifurcation and its runoff which we commonly widen with Dacron patch angioplasty. As with aorto-femoral (and thoraco-femoral) bypass we normally implant albumin-treated knitted Dacron graft material.
INFRA-INGUINAL BYPASS
The concepts governing infra-inguinal bypasses have undergone evolution as have the aorto-ilio-femoral, so-called “inflow” procedures. The dominant feature of most open revascularizations today are that they are performed for limb salvage. And since most limbs at risk of amputation are in diabetics we usually limit open surgical procedures to patients who are attempting to heal foot ulcers. That is not to say that claudication is an invalid indication for non-diabetics or diabetics. But in the case of the latter patient group, the patients do not usually present with leg symptoms induced by walking.
Limb salvage bypass procedures are most often infrainguinal and vary widely because of the disease pattern. The Deaconess/Joslin group, in their report on dorsalis pedis bypass (12), has provided a broader background on the diversity of infra-inguinal procedures that are enlisted to deal for this population (Table 1).
Total Deaconess- Joslin bypass experience of 3731 bypasses to 10 different distal anastomic sites (12)
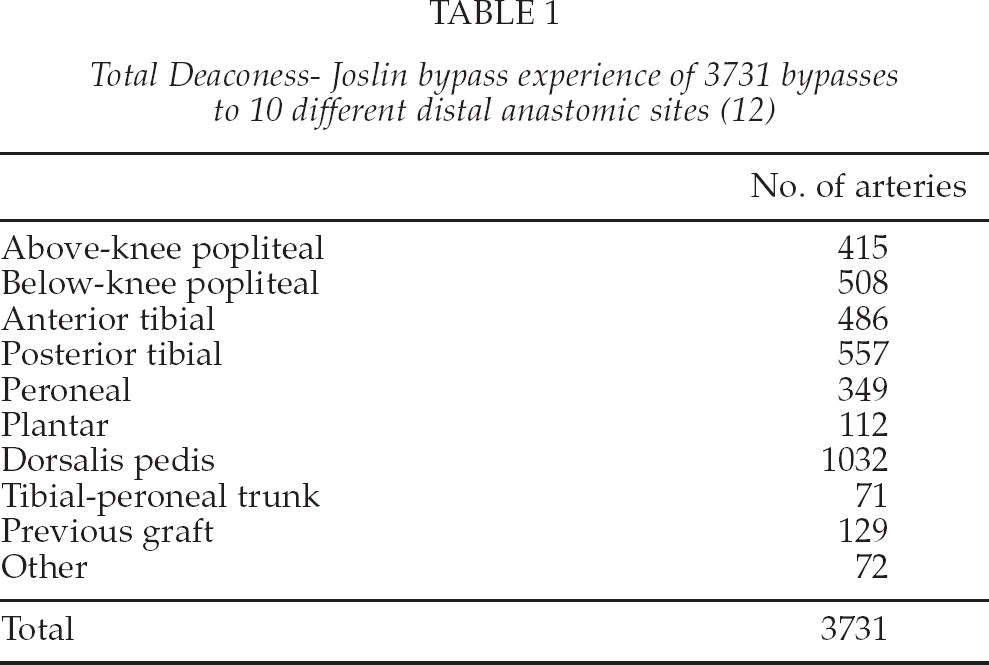
The principle that all bypasses should originate from the common femoral artery for maximum graft durability has been widely refuted. More distal inflow sites provide durable inflow (13, 14). Likewise, more proximal outflow is associated with durable patency when there is no significant obstruction between the distal anastomosis and the arterial segment leading to the foot. The shorter bypass conduits resulting from distal inflow and proximal outflow appear to have intrinsic advantages (15). These include the obvious decreased operative morbidity of a smaller scale operation; the ability to select portions of autogenous venous conduit when greater lengths are unavailable.
FEMORO-POPLITEAL BYPASS
Even if the infra-inguinal bypass needs to extend only to the above knee popliteal artery, most surgeons would preferentially use autogenous ipsilateral greater saphenous vein (GSV) if it was available. In the absence of GSV alternative autogenous conduits such as arm vein and contralateral GSV are usually eschewed in favor of synthetic grafts. There appears to be little advantage to either knitted Dacron or PTFE and are both are widely used. Likewise, there is no need to use more distal inflow sites such as the DFA or the proximal SFA as graft availability is not a problem; the CFA is the preferred inflow site unless contraindicated. If the above knee popliteal artery is soft and patent any target will suffice, but in the presence of calcification we elect either to unroof the adductor tendon where the popliteal artery is usually spared from calcification to find a soft distal target or extend the bypass distally to the below popliteal artery or beyond. In the case that the knee joint is crossed, we strongly prefer autogenous conduit.
“DISTAL BYPASS”
With the re-introduction of the in situ bypass (16) it became apparent that long bypasses to the ankle and foot – so-called paramalleolar bypass – achieved patency and effectiveness equivalent to shorter grafts. Additional lessons from the in situ bypass experience included the observation that the vein could be implanted either reversed or non-reversed and that the graft would function with equal effectiveness either in a deep, orthotopic tunnel or subcutaneously. Some surgeons selected subcutaneous tunnel because that provided easier graft surveillance by physical examination or duplex ultrasonography.
The infra-popliteal artery to paramalleolar artery bypass has expanded its use because infrapopliteal arterial occlusive disease is the predominant pattern seen in diabetes requiring revascularization and because the prevalence of diabetes and the indications for diabetic interventions are rising dramatically. Like the longer bypasses to the foot, they must be constructed of autogenous vein. Homograft GSV has been advocated but have not been able to achieve durable patency expected with autogenous grafts (17, 18). The argument over the superiority of reversed versus nonreversed versus in situ bypass was investigated and most surgeons now agree that all three are equivalent (19). A concordance of opinion was expressed as follows: vein is vein.
The ingenuity of surgeons carrying out infrapopliteal bypass grafts has been rewarded in many ways. First and foremost, because they are performed for pedal ulceration and gangrene, countless major amputations that seemed inevitable have been avoided. Second, the patency of these somewhat shorter grafts approximates that of the standard femoro-popliteal bypass. Third, bypasses to the foot, in most instances, are to “isolated (arterial) segments” because the primary pedal arch is incomplete. This has not diminished their effectiveness and consequently bypasses to isolated tibial artery segments, in selected patients are a useful option (20). It is the unpredictablility of the intrapedal circulation and the fact that diabetic ulcerations are initiated by factors related to neuropathy and repetitive trauma that continues to confound the proponents of the “angiosome hypothesis” (21, 22).
The choice of the arterial distal target site in the paramalleolar region is typically not a choice at all. In many cases only one “runoff” artery suitable for an anastomosis is available and that is the artery that is chosen. The dorsalis pedis artery in most series is the distal target for bypass; if the anterior tibial artery above the ankle joint is patent and in disease-free continuity with the intrapedal arteries, anastomosis to this site results in a shorter bypass. Often, only a foot bypass is possible and the target arteries are small, perhaps only one millimeter in diameter. It is bypasses to the medial and lateral plantar arteries and the tarsal artery that are the most challenging and, hence, the most rewarding for the patient. Tunnels to these very distal arteries must be fashioned with greatest care because the skin is fragile. Postoperative edema is to be assiduously avoided.
There are other complementary techniques for bypass procedures that are useful additions to the vascular surgeons technical armamentarium. On those occasions where there are hindfoot (posterior tibial/plantar circulation) and forefoot (anterior tibial/dorsalis pedis circulation) and target arteries in both territories are patent, we will construct bifurcated grafts (Fig. 1). This is beneficial because the plantar arch and/or the primary pedal arch is in most cases incomplete.
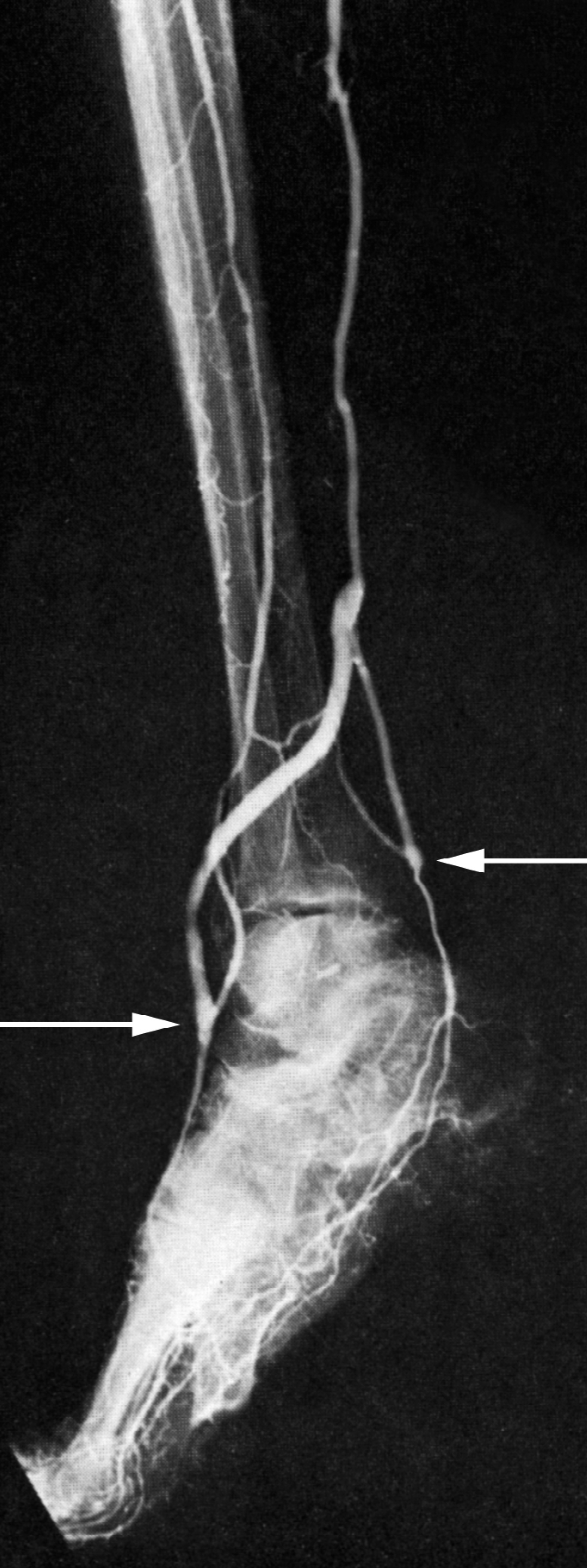
Composite pedal bypass graft, CFA to posterior tibial in situ bypass graft with a side-arm of accessory GSV to the dorsalis pedis artery.
COMPOSITE AUTOGENOUS GRAFTS
Because very distal bypasses are by necessity made from autogenous vein, the compositing of two or more segments of autogenous vein into a single long conduit should not be overlooked (23). Some guidelines for the compositing, based on our experience, have served us well. The segments with largest diameter are placed more proximally; in instances where the vein segment diameters are equal the arm veins are positioned proximal to saphenous veins; veins should be non-reversed with the valves lysed to permit bidirectional flow in the distal end of the graft; compositing is performed over an 8 French catheter and anastomoses are generously beveled and sewn with 7–0 monofilament suture using magnifying loupes; gentle traction while tying the sutures will help to avoid “purse-stringing” the anastomosis. Composite grafts become necessary when segments are damaged by previous inflammatory/phlebitic changes. We advise preoperative systematic duplex graft vein assessment because we have observed graft strictures at the sites where segments are sewn together. We presume that these strictures are, in part, due to pre-existing vein disease. They ought to have been excised as they worsen when the vein is arterialized.
ARM VEINS (AND OTHER AUTOGENOUS ALTERNATIVES)
Introduced in 1968, cephalic veins were convincingly demonstrated to be useful for lower extremity arterial occlusions; their widespread acceptance and clinical application, however, ensued only haltingly (24, 25). Basilic veins were subsequently used effectively but also sporadically for the next decade. Motivated by the marginal results for infrainguinal bypass with synthetic grafts and cryopreserved saphenous vein homografts, surgeons cast about for new bypass materials. Favorable long-term results as far distally as the paramalleolar level helped to accept the arm veins as the second choice for autogenous bypass by many groups who were given the sobriquet “ardent autogenists”.
Contrary to appearances and supposition arm veins are sufficiently long to perform long infrainguinal bypasses (Fig. 2). Cephalic veins have been shown, somewhat surprisingly, to be adequate in length to extend from the CFA to the midcalf crural arteries; the basilic vein, in its entirety and preferentially implanted in the non-reversed, valve lysed configuration, spans from the CFA to the below-knee popliteal artery. To the list of autogenous alternatives headed by the cephalic and basilic veins were added the superficial femoral and lesser saphenous veins whose use has been reported by several groups. The latter, however, never achieved widespread popularity.
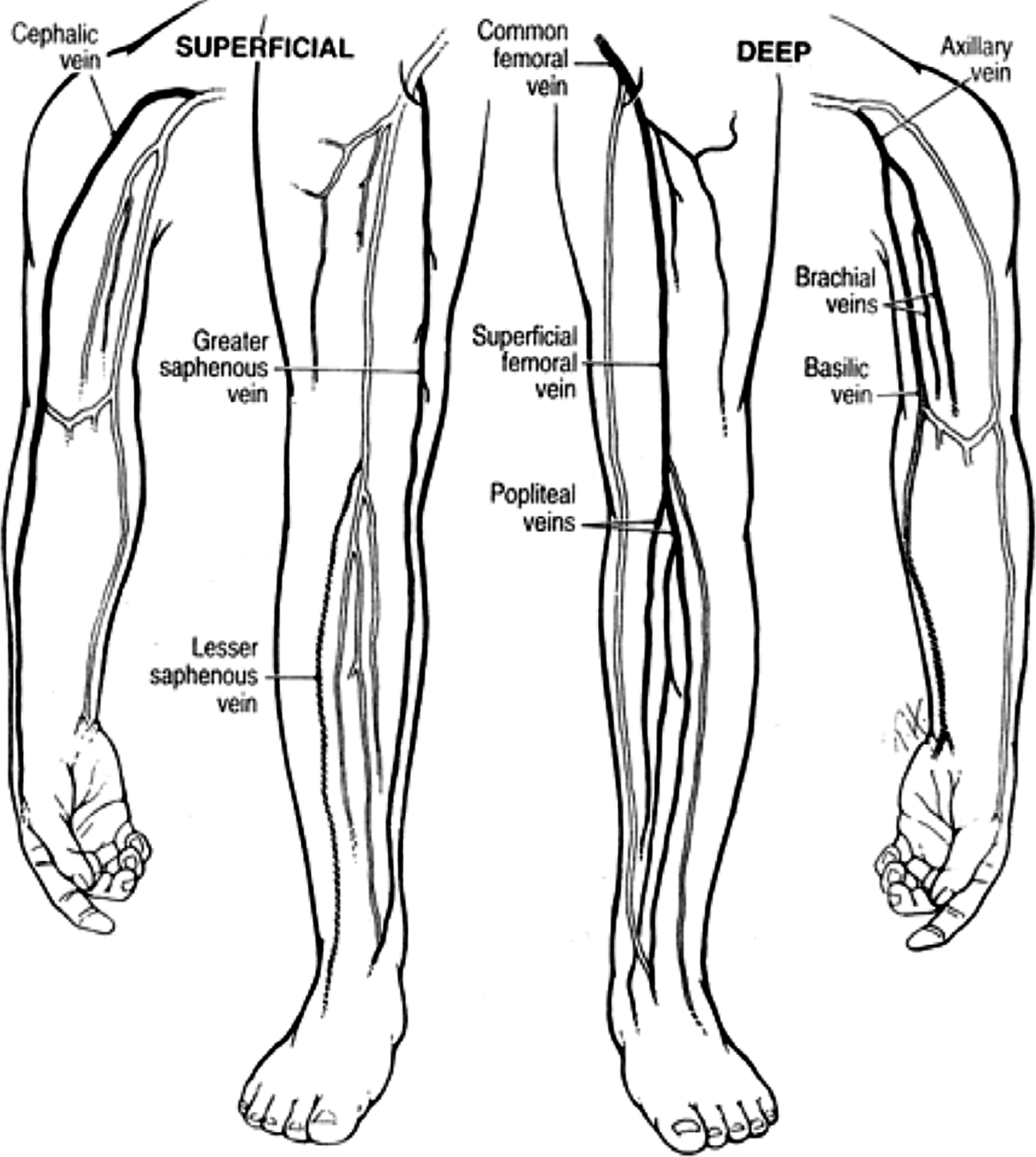
Comparison of cephalic and basilic arm vein lengths in relationship to the leg.
Opinions differ whether arms veins or the contralateral GSV should be used in the absence of the ipsilateral GSV. Many cardiac surgeons urged the preservation of the contralateral GSV for future coronary artery bypass and the use of arm veins for proposed leg revascularization. Studies and experience showed, however, that the GSV would seldom if ever be required for CABG; this encouraged many vascular surgeons to harvest vein from the other leg. The increasing use of percutaneous coronary interventions (PCI) and improved medical therapy including statins lead to a decline in all types of coronary revascularizations. This reduction in GSV CABG and the increased use of internal mammary arteries for CABG has contributed to the greater availability of GSV for leg bypass.
In our own practice we have witnessed a gradual decline in the use of arm veins for long segment bypass. We attribute this to an older comorbid patient population whose veins have been subjected to many venipunctures and intravenous infusions; we are particularly averse to the use of peripherally inserted central catheters (PICC lines) for long-term drug infusions because they diminish the subsequent usability of the veins for bypass. With a growing number of diabetics who need both hemodialysis using autogenous fistulas and infrainguinal bypass for ischemic ulceration the performance of bypasses with arm veins has witnessed a further decline.
We employ two additional techniques when only a limited length of venous conduit is available. The first of these is applicable in cases in which the indication for bypass is tissue loss and a pedal pulse needs to be established. If there is a superficial femoral artery occlusion and a transgenicular isolated popliteal artery segment a short bypass above the knee will not provide sufficient pedal perfusion and a second sequential bypass to the foot – constructed of vein – is necessary. The non-reversed autogenous vein is reserved for the distal bypass while the more proximal segment receives a synthetic bypass (Fig. 3).

Hybrid bypass; CFA to popliteal Dacron bypass. Popliteal to pedal vein bypass.
The second salvage procedure that is performed frequently for limb salvage is the distal vein cuff which requires only an 8 to 10 centimeter length of vein; we have used all veins except the cephalic. We view this procedure as a “last ditch” operation but have been surprised by its three year patency of 73% (26). Because many of these procedures are third and fourth attempts at limb salvage and the patients are elderly with only a 18–36 months' estimated survival, we believe them to be justified. We extend so-called “Miller Cuff” bypasses no further than the middle third of the infrapopliteal arterial segments.
GRAFT FAILURE
All of the complications of bypass grafts and open surgical revascularization procedures are beyond the scope of this review. Monographs have been devoted to graft infection alone. Graft thrombosis likewise has a broad and deep literature spanning several decades that reflects its multiple causes. Nevertheless, certain features of graft failure and subsequent thrombosis will be touched upon. Although diffuse autogenous conduit disease can lead to extensive and diffuse stricturing ultimately leading to thrombosis, it is most often a focal stenosis that progresses via thrombosis to complete occlusion of the graft. The sites of secondary graft stenosis are the 1) proximal and distal anastomoses, 2) veno-venous anastomoses where grafts are composited, 3) vein valves and 4) sites of venous fibrosis, which in the case of arm veins is a fibrostenosis that resulted from venipuncture when the vein was in the arm. These lesions can occur on up to 40% of grafts and usually develop three to 18 months post-operatively. Detection of these secondary defects with systematic duplex graft surveillance enables their repair before graft thrombosis supervenes; autogenous conduits are precious and they deserve every effort to forestall thrombosis.
Aneurysmal degeneration of autogenous vein grafts of all kinds has been described (27). This is usually a diffuse aneurysmosis and occurs 2 to 3 years after graft implantation. This complication has also been reported in CABGs. If left uncorrected the graft will progress to thrombosis sometimes preceded by distal embolization. Typically, the cardiac patients nearly always manifested thoracic and abdominal aneurysms, whereas the lower extremity bypasses were implanted for the treatment of popliteal aneurysms. Repeat revascularization for aneurysmal thrombosis is problematical because, as we have observed, autogenous conduits from other sites will also become aneurysmal and thrombose. In this situation we have successfully used the PTFE-distal vein cuff procedures to restore perfusion.
COMMENT
To vascular surgeons who spent their careers treating occlusive and aneurysmal disease exclusively with bypass grafts, the characterization of endovascular therapy as “disruptive technology” must be seen as woeful understatement. Up and down the ladder of vascular specialists, from residents to senior professors, the urge to perform catheter-based therapies is now so strong that operative procedures of all types not only bypass grafts but all open procedures have been supplanted; some surgeons have gone so far as to call open surgery obsolete. In recent memory, trainees were fearful that their training programs would not offer sufficient endovascular experience and that once they were in practice, they would be unable to compete without a “toolbox” that was better stocked. Yet in only a few short years the tables have turned completely. In many centers, the majority of arterial and venous interventions are now “minimally invasive” and catheter-based; as a result the judgment and experience of when and how to perform open revascularization is disappearing from the corridors of training and practice. “Endo first” reigns.
Have we come so far down the endovascular superhighway only to arrive at a worrysome and menacing terminus: a one way street or, worse yet, a cul-de-sac?
Since the introduction of balloon angioplasty many practitioners have considered it to be a complementary therapy to open revascularization; variations in disease patterns as codified in TASC l and TASC ll make this premise more valid than ever. The initial TASC document recommended that arteriosclerotic occlusive disease should be stratified for diagnostic and therapeutic purposes into four grades, A through D, of increasing severity and based primarily on its arteriographic extent and characteristics. Grades A and B were less severe and hence suitably treated by endoluminal methods (overwhelmingly balloon angioplasty), whereas grades C and D were comprised of long stenosis/occlusions that were preferably managed with bypass procedures.
TASC l based its recommendations on the outcomes that existed in the evidence-base up to 2000. The second TASC document differed from the first in that it reported practice patterns. TASC ll emphasized current practice patterns that were the result of “stretching the therapeutic envelope” in which endovascular procedures were performed on TASC l C and D lesions. As a result a “classification creep” emerged in the newer guidelines manifested with the recommendation that the more severe C and D lesions from TASC l were reduced to B and C level and, hence, more appropriate for endotherapy. Clinical indications and meaningful outcomes, especially durability of patency, assumed less importance. A third iteration of the TASC document is in preparation. It is hoped that it provides guidelines that not only address the previous deficiencies, particularly for the growing population with diabetes and calcific disease in the infrapopliteal segment, but that it leads to an improved and authentic evidence-base for future analysis.