
Abstract
Background and Aims
Total hip arthroplasty significantly improves patient's life quality. However, total joint replacement is associated with possible complications, such as dislocations, infections, fractures and periprosthetic osteolysis. The goal of this study was to evaluate a large head metal-on-metal total hip arthroplasties and analyse short term complications related to them.
Material and Methods
Between 9/2005 and 6/2009, a total of 691 hip replacements were performed on 635 patients with the use of Magnum M2 large head cementless metal-on-metal prosthesis in Turku University Hospital. All patients had a scheduled follow-up at two to three months, and at one year. The results were evaluated using X-rays, Harris Hip Score (HHS), and evaluating post-operative complications and reasons for re-operations.
Results
During our follow-up the HHS median raised from its preoperative value of 59.8 to 86.4 two to three months after the operation, and to 93.9 one year after the operation. As a complication we had five infections requiring single open debridement (early infection) or a two stage revision. Seven patients had a periprosthetic femoral fracture that was operated and 11 patients were reoperated because of acetabular component malposition, fracture or early loosening. We did not observe any dislocations, n. ischiadicus damages, squeeking or complications related to high metal ion release (ALVAL-reactions (Aseptic Lymphocyte-dominated Vasculitis-Associated Lesion) or pseudotumours).
Conclusions
The metal-on-metal bearing pair allows large femoral head size, which decreases the risk for dislocation. It may also decrease the risk for osteolysis and aseptic loosening in a long run. Early complication rate related to the bearing surface is minimal. Metal-on-metal prosthesis is a good choice for young and active patients with good bone quality.
INTRODUCTION
In most patients a total hip arthroplasty significantly improves life quality and helps them survive in everyday life. There are also complications with protheses, such as dislocations, infections, fractures and periprosthetic osteolysis caused by wear debris. Periprosthetic osteolysis is the single most important factor causing aseptic loosening of the prosthesis.
The most common articulative bearing pair is metal-on-plastic, more specifically a cobalt-chromium — polyethylene pair. However, plastic bearing releases a significantly greater amount of wear debris than a metallic bearing (1). Wear debris causes osteolysis, and osteolysis might lead to aseptic loosening.
The smaller the femoral component head size, the greater the risk of dislocation. Smaller femoral head size decreases motion range. On the other hand, bigger femoral head size in metal-on-plastic bearings are thought to cause more wear debris and therefore increase the rate of osteolysis (2). Contrastively, metal-on-metal bearings with a larger femoral head size decrease friction and improve the lubricative features of the prosthesis, which improve abrasion resistance. In metal-on-metal prosthesis, the formation of wear debris has been minor and osteolysis rare (3, 4, 5, 6).
The theoretical advantages of recently developed metal-on-metal prostheses are a lower dislocation rate and a decrease in osteolysis caused by wear debris. Accordingly, the amount of prosthesis loosenings are lower. A metal-on-metal bearing pair may also have some limitations, such as squeaking, increased metal ion levels in the blood stream and urine, and pseudotumours. However, the clinical importance of these findings is still unknown.
The purpose of this study was to analyse the short term results and complications of metal-on-metal prostheses.
MATERIAL AND METHODS
Between 9/05 and 6/09 there has been a total of 691 cementless metal-on-metal hip arthroplasty operations in 635 patients in Turku University Hospital. The Bi-Metric stem and Recap-Cup (Biomet, Warsaw, ind) with metal-on-metal articulation and large diameter head (Magnum) was used in all cases. Three hundred sixty-nine of the patients were women (58%) and 266 were men (42%). The average BMI was 28,1 and the average age at the date of surgery was 63 years. All the operations were done through Hardinge's anterolateral approach.
This research was a follow-up study, and material was collected retrospectively. All the patients had a scheduled follow-up with a surgeon and a physiotherapist in two to three months postoperatively, and again one year later.
Patients
The results were evaluated using the Harris Hip Score. In addition, postoperative complications and reasons for re-operations were included in the study.
The immediate complications of total hip arthroplasty are dislocations, infections, venous thrombosis, pulmonary embolies and periprosthetic fractures. Late term complications are infections, periprosthetic fractures, dislocations, breaking of the parts and periprosthetic osteolysis.
All the information was gathered and saved to an electronic database, called Implant DB.
RESULTS
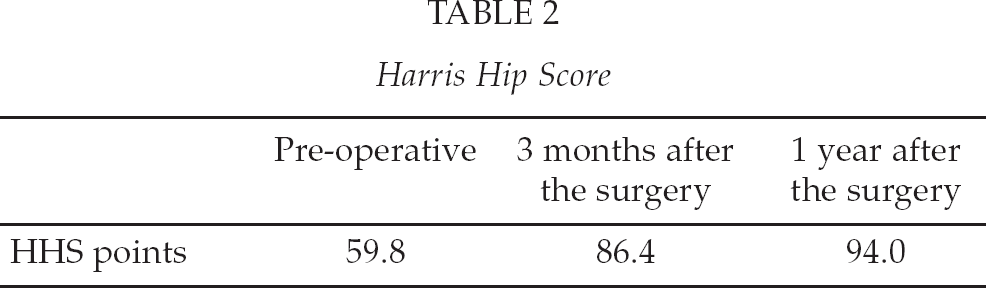
The preoperative Harris Hip Score (HHS) was 59.8, with a postoperative median of 86.4 HHS two to three months later, and 94.0 HHS one year after the operation.
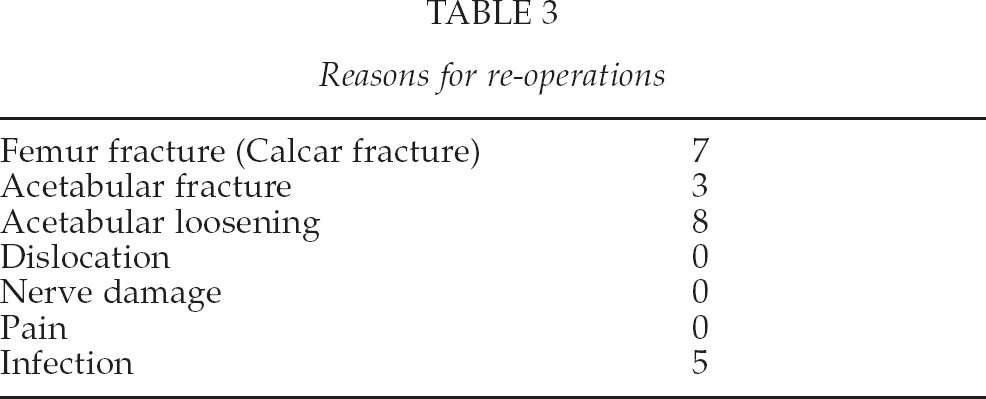
The most common reason for a reoperation was a typical periprosthetic calcar fracture of femur. A total of seven patients suffered from that and had to go through a reoperation. We also experienced five trochanteric fissures, which were treated concervatively. A total of 11 patients had to go through reoperation because of early loosening, fracture or malposition of the acetabular component. A total of five patients suffered from postoperative infection, three of them were prosthetic infections and two of them were superficial infections.
We did not experience any n. ishciadicus laesions, dislocations, squeaking of the prosthesis or a release of metal ions into the blood stream. Additionally, we did not observe any complications related to metal ions in the blood stream, such as ALVAL-reactions or pseudotumours.
DISCUSSION
Metal-on-metal bearings approve a larger femoral head size without increasing the risk of osteolysis. The greater the femoral head size, the smaller the risk of dislocation (7). We did not experience any dislocations in our study. Dislocation is one of the most common complication in total hip arthroplasties. One major advantage of the metal-on-metal total hip arthroplasty is that the dislocation rate is lower than with the other articulation surface options.
Harris Hip Score
Reasons for re-operations
In our study, patients were allowed full body weight bearing and free mobilization without any restriction immediately after the operation. We believe that this has speeded up the recovery process and shortened the time required for hospital care. We also believe that this has allowed better functional end-results than could have been accomplished with strict restrictions. Recovery has been faster because patients have been able to begin the rehabilitation process immediately. The immobilization time is lessened due to fast patient mobilization, and therefore complications caused by immobilization (DVT, pulmonary emboli) are also thought decreased.
In our study, 11 patients had to go through re-operation because of the acetabular component. Eight patients had an aseptic loosening, and three patients had a fracture. The number of aseptic loosenings is quite high. The system does not allow any kind of screw fixation. The cup stability relies purely on the press fit concept. In the beginning of the analysis of patient material, we probably pushed the limits of this concept. Accordingly, the number of aseptic loosenings at acetabular side has declined. Additionally, we noticed one aseptic loosening and one malunion of the femoral component. The durability of uncemented metal acetabular components is good, and osteolysis doesn't normally appear even over a long period of time (8). This is an important factor, especially for younger patients, who need a long-lasting prosthesis with high wear resistance.
In our material we had seven periprosthetic fractures requiring a reoperation. Additionally, we had five trochanteric fissuras, which were treated conservatively. A hip prosthesis can be fixed with or without cement. With metal-on-metal bearings, uncemented fixation is preferred. Studies have shown that cement fixation in metal-on-metal bearings increase the likelihood of periprosthetic brightening around the acetabular component by 65% (9). The reason for this is thought to be the hardness of metal-on-metal prostheses, and the flexibility qualities, which differ greatly in comparison to normal trabecular bone. This is especially important in young and active patients, since cement fixation of the acetabular component may restrict their active lifestyle (9).
Uncemented prostheses are associated with larger periprosthetic fracture rates than cemented ones. This problem is partly concept related, and the fracture rate is most likely not related to articulating surface or femoral head size. Bad bone quality is the single-most important risk factor when it comes to periprosthetic fracture. Apparently cement strenghtens the femoral cavity from inside (10). In our study, ten hips (1,4%) had to go through reoperation because of a periprosthetic fracture. Old age and bad bone quality are the primary risk factors for periprosthetic femoral fractures (11). Uncemented metal-on-metal hip prostheses may not be the best option for elderly patients, especially if they suffer from poor bone quality.
Uncemented prostheses are 1.5–2 times more expensive than cemented ones. However, they are more reliable in younger patients than cemented prostheses (12). There is no difference in short term pain relief or in recovery time between cemented and uncemented prostheses (13).
The use of metal-on-metal bearings have been restricted by its high price. In addition, the high levels of cobalt and chrome ions found in the blood stream and urine, in association with the use of metal-on-metal bearings, have restricted their use (3). The clinical significance of increased levels of cobalt- and chrome ions has yet to be determined. However, long time studies have shown that metal-on-metal prostheses are not connected to renal failure or an increased number of cancer cases (14). Increased metal ion levels and the possibility of ALVAL-reaction are always a concern; problems with these have been observed especially with some resurfacing prostheses. The problem seems to be implant related. ALVAL-reaction causes joint hydrops with milky, steril fluid, soft tissue necrosis and pseudotumours. It is not sex related. However, these reactions may occur late onset and one year follow-up time might not be long enough to show this problem (15, 16).
These are all difficult problems, and elevated levels of metal ions in blood stream have been well documented. However, it is important to notice that most of the studies with these results consider metal-on-metal resurfacing prosthesis, not metal-on-metal total hip atrhroplasties (17). It has also been thought that metal wear debris may cause DNA damage through chemical reaction or by action of metal ions. However, in a 28-years long Scandinavian follow-up study it has been shown that metal-on-metal total hip arthroplasty does not increase the incidence of cancer (18). In the Magnum M2 –model, these problems have not as of yet been observed, and in our study we did not observe any complications resulting from high metal ion levels or immune reactions.
Ceramic is another option for bearings, it is harder than metal and can be processed smoother than a metal bearing. A harder and smoother surface provides less friction and therefore causes less wear debris, and it is thought to cause less osteolysis. Ceramic wear debris is biologically inert and causes only a slight biological reaction (19). However, osteolysis has been observed with ceramic prostheses as well (20). Ceramic bearings are even more expensive than metal ones and are more likely to fracture due to their hardness. It is also a more difficult material to work with than metal. One advantage that metal-on-metal bearings have in comparison to ceramic-on-plastic, is that they allow for larger femoral head size. A large head improves the head-to-neck ratio, which increases the range of motion of the prosthetic components without impingement. It also decreases the risk for dislocation (7).
During our follow-up time, two patients suffered a deep prosthetic infection and three patients suffered superficial wound infection that needed revision surgery.
In our study, we did not encounter any dislocations. Dislocation is a quite severe complication of hip arthroplastic surgery. The functional results of patients with dislocations are often unsatisfactory, and the daily activities of the patient can be compromised. A metal-on-metal prosthesis with a large femoral head size would most likely be the best prosthesis for younger and more active patients. However, an active lifestyle is also recommended for elderly patients. Our study showed that during a one year period, the Harris Hip Score increased from a preoperative 60 to 94. This is a major change, considering the patients' ability to function in day-to-day life. The increase in the Harris Hip Score also indicated a considerable decrease in the amount of pain experienced by patients.