
Abstract
Background and Aims
In the era of expanding costs of healthcare, this study was conducted to perform a cost analysis of introducing a laparoscopic liver surgery programme for left sided liver lesions.
Materials and Methods
Consecutive patients treated by laparoscopic liver resections of left lateral segments were included. Controls were a group of 14 patients undergoing open resection for similar pathology. Primary outcomes were costs. Secondary outcomes were complications, conversions, blood loss, length of operation, and length of hospital stay.
Results
The laparoscopic approach for hepatic left lateral resection (bisegmentectomy 2 and 3) was performed in fourteen patients (group I, median age 54 [range 26–82] years). In the open group, fourteen patients from a prospectively collected database with the same type of resection were selected (group II, median age 64 [range 29–76] years). Costs of theatre usage in the laparoscopic group were significantly lower (p = 0.031). No significant differences in costs of disposable instruments, ward stay and total costs were observed between the two groups. There were three complications in the laparoscopic group compared with two complications in the open group. In the laparoscopic group there were 2 conversions (14%). Median blood loss was significantly lower in the laparoscopic group (50 mls [range 0–750], (p = 0.001) versus the open group (500 mls [range 150–750]). Furthermore, operation time was also significantly lower in the laparoscopic group (116 [range 85–261] minutes) versus the open group (165 [range 96–217] minutes, p = 0.016). Median length of stay was 6 [range 4–11] days in group I versus 6 [range 5–13] days in group II (p = 0.508).
Conclusion
Costs of laparoscopic liver resections proved to be equivalent to open surgery. Furthermore, implementation of a laparoscopic liver resection programme seems feasible and safe with reduced blood loss and operation time and comparable morbidity and length of stay.
Keywords
INTRODUCTION
Liver resection remains one of the few procedures where the extended use of laparoscopic techniques has not found its way in everyday practice yet. Several international hospitals have reported their series of laparoscopic liver resections(1 –6). Although laparoscopic liver resections are gaining popularity world wide, the experience in the Netherlands is still limited. Several studies have reported the feasibility and safety of laparoscopic resections for liver tumours in centres with extensive experience in both hepatobiliary surgery and laparoscopic surgery (1 –6). The evidence is mostly based on case-series and shows a technique that is reproducible with limited morbidity and mortality. A consensus statement was published on laparoscopic liver resections by Buell J et al (7) which makes one of its conclusions that resection of segments 2 and 3 by laparoscopic approach should be the standard of care. However, implementation of new techniques mostly coincides with expanding costs, especially laparoscopic surgery where expensive, disposable tools are required and more operation time is needed (8 –10). Worldwide, both governmental organisations and health insurance companies have a major influence on cost regulation issues in health care. Hospital managements have budgets for Operation Room (OR) cost and often surgeons are required to make business plans before introducing new techniques. In contrast to many feasibility studies on laparoscopic liver surgery, there is scarce evidence about the cost analysis of this surgical approach. Therefore, the present study was conducted to assess the costs of introducing a laparoscopic liver surgery programme for left sided lesions.
MATERIAL AND METHODS
The study describes the first consecutive group of patients undergoing laparoscopic liver resections for solid liver lesions in Maastricht University Medical Centre in the years 2003 to 2008. This group of patients was compared with a group of patients undergoing the same type of liver resection as an open procedure in a period from 2001 to 2008. Fourteen patients underwent a laparoscopic approach for left lateral resection (group I) and fourteen patients were included in the open group (group II). Pre-operative assessment consisted of liver function tests, pre-operative radiological evaluation with abdominal ultrasonography, contrast enhanced Computed Tomography (CT) and/or selectively Magnetic Resonance Imaging (MRI) scanning and/or CT PET scanning and multi-disciplinary consensus regarding treatment. All lesions smaller than 10 cm in diameter and limited to the left lateral liver segments were included. Indications for surgery included presumed benign and malignant liver lesions. The indications for resection were not altered for the minimally invasive group. For patients with presumed benign disease, the indications were presence of symptoms, suspicion of a hepatocellular adenoma or cystadenoma or in cases of uncertain nature of the tumour. Indications for liver metastases were synchronous or metachronous liver tumours from colorectal malignancies. Patients were informed about the operative procedure and consent was obtained.
Primary outcomes were costs. Secondary outcomes were complications, conversions, blood loss, length of operation, and length of stay. Complications were defined according to the grading system of Dindo et al (11).
Unit costs and costs of disposable surgical instruments were obtained retrospectively from the Financial Controller of the Department of Surgery. Costs of ward stay were €225/full day (first day €55 extra). This was based on rates from 2007 onwards. Costs of theatre use were divided into an hourly rate for surgery and for anaesthesia, which were respectively €190/h and €560/h. Costs of disposable surgical instruments were as follows: CUSA (Valleylab, Boulder, Colorado, USA) dissecting device €622, Argon plasma coagulator (hand piece) (Bircher Ind., Ltd., Englewood, Colo. USA) €850, Autosuture EndoGIA (Covidien, USA) €256 (reload cartridge€144), Ethicon Ultracision Harmonic ACE (Ethicon Endosurgery, Johnson & Johnson, USA) €567, Autosuture ENDOBAG (Endocatch Autosuture, Covidien, USA) €99, 5–12 mm trocar (Versaport Autosuture, Covidien, USA) €73 and 15 mm trocar (Versaport Autosuture, Covidien, USA) €126. Costs of TachoSil (Nycomed, Zurich, Switzerland) and Tissuecoll (Baxter, Vienna, Austria) for haemostasis were €315 and €547 per application, respectively. The number of disposable instruments being used per operation was analysed. After surgery all patients went to the recovery ward for the first 24 hours. The costs of the recovery ward were equal to the general ward. Costs of sterilising of reusable instruments were considered to be equal since almost the same number of reusable devices are used for both procedures in our hospital setting. Main endpoints for the cost comparison were costs of theatre usage, disposable surgical instruments and ward stay.
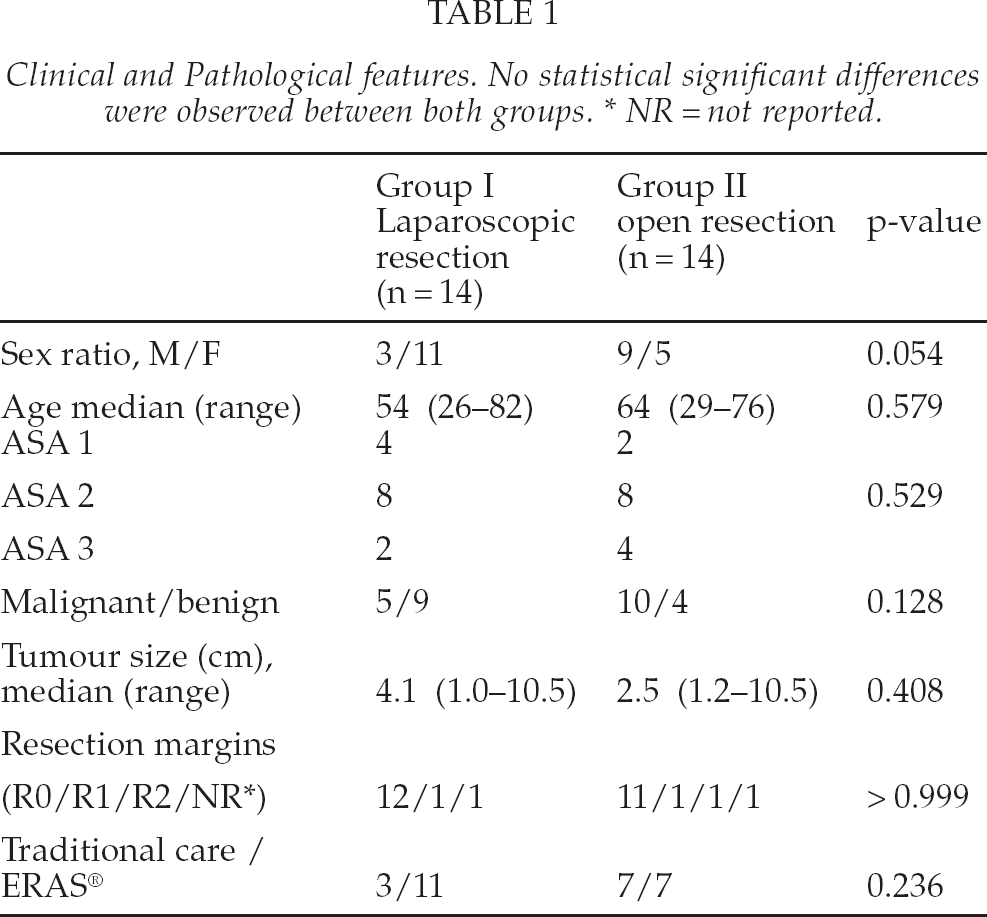
Clinical data were obtained retrospectively from a prospectively collected database. During the selection process, the investigators were unaware of the primary outcome and careful matching was assessed to have similar complexity of procedures and tumour diameter in both groups (Table 1). The groups were matched for type of resection and for tumour location and size. The following data were recorded: operation time, blood loss, post-operative complications, histology of the resected liver specimen with diameter of the lesions, resection margins, and hospital length of stay. During the introduction of the laparoscopic liver surgery programme, a multimodal perioperative enhanced recovery programme (ERAS®) was instituted for all patients undergoing liver surgery in the MUMC and this was also recorded as a parameter.
Clinical and Pathological features. No statistical significant differences were observed between both groups. * NR = not reported.
All patients were carefully followed after discharge according to the MUMC liver surgery protocol: patients were followed periodically in the first, third, sixth and twelfth postoperative months in the first year and at least twice a year thereafter. The follow-up procedure included physical examination, laboratory tests, ultrasonography of the abdomen, and CT scanning in cases where this was considered necessary.
SURGICAL TECHNIQUE
The laparoscopic procedures were performed by two surgeons; one with specific expertise in advanced laparoscopic surgery and one expert in hepatobiliary surgery. Prior to the first liver resections, surgeons visited expert centres in laparoscopic liver surgery outside the Netherlands. Liver resections were defined according to anatomical planes (Couinaud's classification). Only lesions in the left lateral segments requiring anatomical resection of segment II and III were included in the laparoscopic resection group. In the laparoscopic approach group, patients were placed in the supine position under general anaesthesia, with lower extremities apart (6). The surgeon was standing between the legs with an assistant on each side. An open introduction of the subumbilical port was used to produce the CO2 pneumoperitoneum. Abdominal pressure was monitored at 10–12 mmHg and a 300 laparoscope was used in all cases. Four extra trocars were placed to facilitate the procedure (6). The liver was inspected visually and laparoscopic-ultrasound was used in all cases to confirm the number of lesions in relation to the main anatomical structures. The round, falciform and left triangular ligaments and the lesser omentum were divided. Hepatic transection of parenchyma and minor crossing vessels and biliary radicals was performed with harmonic scalpel (Ultracision, Ethicon Endosurgery, Johnson & Johnson, USA) without the use of a clamping method (Pringle's manoeuvre). The parenchyma transection with this device is reported to be sufficient for vascular and biliary structures up to 3 mm (6). The portal pedicles and hepatic veins were stapled using a vascular stapler (EndoGIA Autosuture, Covidien, USA). Resected specimens were placed in a plastic bag (Endocatch Autosuture, Covidien, USA) and removed through a separate suprapubic incision or, in cases where a laparotomy had been performed in the past, through a small subumbilical or subcostal incision. No hand-access devices were used for the laparoscopic approach.
For the open approach, a bilateral subcostal incision was mostly used to enter the abdomen. After abdominal exploration in search of extrahepatic disease, the round, falciform and left triangular ligaments and the lesser omentum were divided. The liver was inspected visually and intra operative ultrasound was performed in all cases to confirm the number of lesions in relation to the main anatomical structures. Hepatic transection of parenchyma was done using the Cavitron Ultrasonic Surgical Aspirator (CUSA®; Valleylab, Boulder, Colorado, USA) and argon beam coagulator (Bircher Ind., Ltd., Englewood, Colo. USA) with or without the use of Pringle's manoeuvre. Minor crossing vessels and biliary radicals were divided using polypropylene sutures or clips. The portal pedicles and hepatic veins were divided and ligated with a running polypropylene suture. After removal of the liver specimen, the raw surface of the liver remnant was subjected to argon beam coagulation and sealed with TachoSil ® (Nycomed, Zurich, Switzerland) or Tissuecoll (Baxter, Vienna, Austria) if appropriate (12).
STATISTICAL ANALYSIS
Continuous variables were expressed as median (range). Statistical analysis of cost comparison was performed using a Mann Whitney U Test, since the groups were small and a non-normal distribution in both groups was assumed. Costs were expressed as mean (± SD), to be able to compare the results from this cost analysis with other studies. Data were analysed according to the intention to treat principle. The Chi-square test (or Fisher exact test where appropriate) was used to investigate differences in demographic parameters: sex, ASA classification, pathology, resection margins, perioperative care programme and the primary outcome parameter complications. Mann-Whitney U Test was used to investigate differences in age, tumour diameter, duration of operation (min.), blood loss (mls) and hospital length of stay (days). A p-value of ≤ 0.05 was considered to indicate statistical significance. SPSS statistical software (version 15.0, Chicago, Illinois, U.S.A.) was used for the analysis.
RESULTS
The laparoscopic approach for left lateral resection (bisegmentectomy 2 and 3) was performed in fourteen patients and completed laparoscopically in twelve patients (Table 1). In the open group, fourteen patients were included (group II). Demographics of both groups are reported in Table 1. There were no significant differences in sex, age, ASA classification, benign lesions, tumour size, resection margins and perioperative care programme.
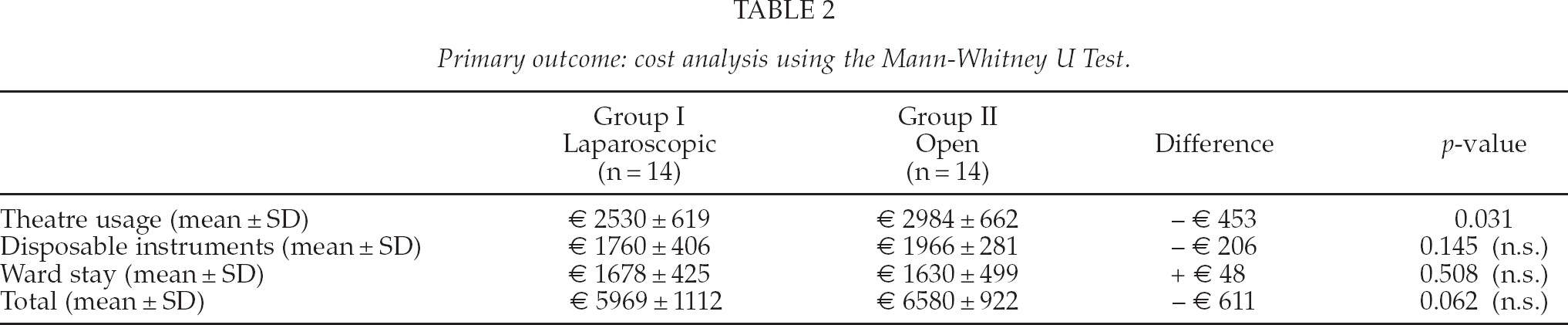
Costs of theatre use were significantly higher in the open group (Table 2). The costs of disposable surgical instruments were on average €206 per patient lower for laparoscopic surgery. No significant differences were observed in ward stay. Overall, total costs tended to be on average €611 per patient lower in the laparoscopic group, but this failed to attain statistical significance (Table 2).
Primary outcome: cost analysis using the Mann-Whitney U Test.
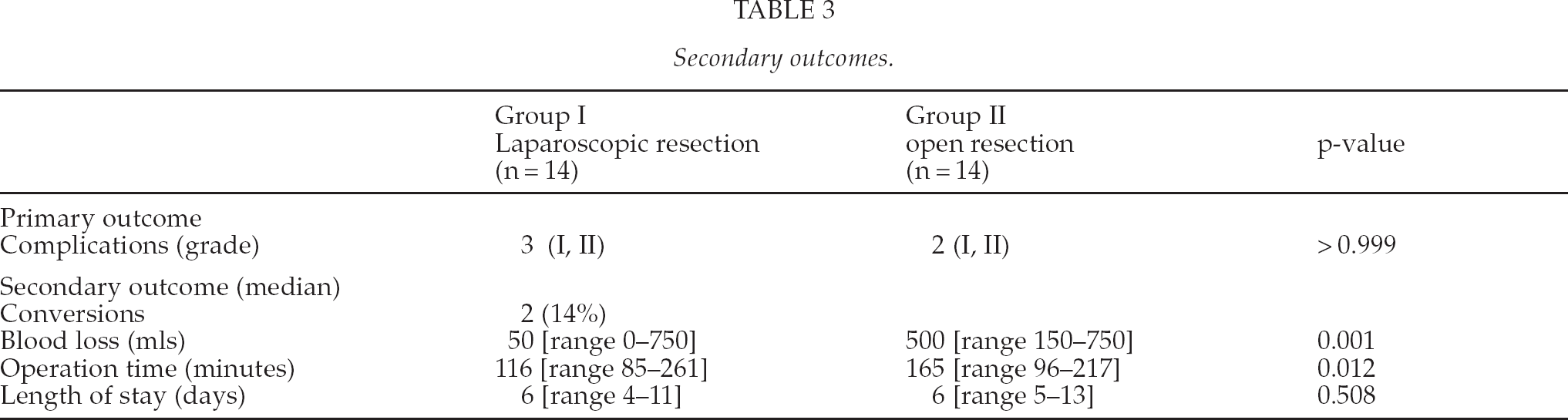
There was one grade I complication and two grade II complications in the laparoscopic group (Table 3). One patient remained longer in hospital due to constipation, one patient had a urinary tract infection and another patient was treated for atrial fibrillation. In the open group there was one grade I complication and also one grade II complication. One patient had a delayed functioning of the gastrointestinal tract and one patient was treated for a myocardial infarction. Respectively, eleven and twelve patients in each group had an uneventful recovery. The two conversions (14%) were due to tumour size, additional unanticipated lesions and close relation with the left liver vein. One patient appeared to also have a lesion in segment IV and the exposure was considered insufficient to perform a safe resection. The second conversion was performed because of the close relation to the left hepatic vein, large diameter of the lesion and uncertain nature of the tumour. Median blood loss was significantly higher in the open group than in the laparoscopic group (p < 0.001). Duration of operation was also significantly reduced in the laparoscopic group (p = 0.012). The data on secondary outcomes are presented in Table 3. There were no deaths within 30 days after surgery.
Secondary outcomes.
In the laparoscopic group there were 9 benign lesions and 6 malignant tumours (5 patients). The median tumour size was 4.1 [range 1–10.5] cm (Table 1). In this group, there were three adenomas, three focal nodular hyperplasia (FNH), an angiolipoma, a hemangioma, a presumed metastases, which proved to be an inflammatory pseudotumor after chemotherapy and 6 metastases of colorectal origin. All but one resection margins were free of disease, the R2 resection was found in a resected specimen of an adenoma. In the open group, there were six benign lesions (two adenomas, FNH, polycystic liver disease, inflammatory granuloma, and focal haemorrhage; the latter two in patients with malignant disease) and 10 malignant tumours in eight patients (mostly colorectal metastases, and one sarcoma) with a median tumour size of 2.5 [range 1.2–10.5] cm (Table 1). In all but one patients, an R0 resection was performed.
In group I, there were no late complications specifically related to the laparoscopic procedure within a median follow-up of 43 [range 12–97] months. No port-site metastases were detected in this group. However, 5 patients died during follow-up after 12 (n = 2), 27, 32 and 37 months. Causes of death of these patients were cancer related; all patients died due to progressive metastastic disease. Concerning the late complications in the open group, there were two symptomatic incisional hernias within the median follow-up of 60 [range 11–128] months. In the open group, six patients died during follow-up after 11 (n = 2), 14, 28, 39 and 87 months. All but one of these patients died with progressive metastastic disease. One patient died due to a cancer unrelated cause.
DISCUSSION
Laparoscopic surgery is considered to be more expensive compared to open procedures, especially because most laparoscopic procedures need more operating time and more disposable devices than their open counterparts (8 –10). Although peri-operative outcome remains the surgeon's main focus, the costs of the procedure should also be accounted for when deciding between a laparoscopic or open approach. The use of disposable surgical instruments and prolonged operation room-usage consequently may lead to an increase in costs. We therefore performed a cost analysis, calculating the costs of laparoscopic and open liver resections. The results of this cost analysis show that, apart from significantly lower costs of theatre usage in the laparoscopic group, no statistically significant differences in costs of disposable instruments, ward stay and total costs were observed between the laparoscopic and open group. The present results are favourably comparable with a recent study on this subject, where no differences were found in operation time and costs (13). Other reports showed that the total costs for laparoscopic surgery were significantly lower (14, 15). In these studies, a considerable difference was seen in hospital days, which consequently led to lower costs in the laparoscopic groups. In the present study no difference in length of hospital stay was observed between both groups. Moreover, both CUSA and argon beam coagulator are used in the MUMC for the open resections which leads to considerable costs of disposables, in contrast to the laparoscopic approach where only the harmonic scalpel is used for the liver transection.
This study confirms previous reports in the literature that the introduction of a new technique such as laparoscopic resection of solid liver tumours in segment II and III is feasible and safe. It was suggested that laparoscopy is a safe approach in a selected group of patients with reduced blood loss and reduced morbidity (5, 16 –20). To date in the era of evidence based medicine, however, there is scarce high-level evidence that properly compares laparoscopic liver resection and open hepatic resection. There are no randomised studies available to confirm the observations in the prospective and retrospective studies hitherto reported. Some prospective case-series studies have been published with similar conclusions of reduced blood loss and morbidity (14, 18, 21). However, apart from the previously mentioned advantages, most investigators observed a longer operation time and have postulated increased costs of laparoscopic surgery.
In the present attempt to study the effects of laparoscopic liver surgery in a comparative setting, we observed a faster resection, less intra-operative blood loss with comparable morbidity, both in the short and long term. The reduced blood loss might be caused by the raised intra-abdominal pressure of the pneumoperitoneum which is necessary for the laparoscopic approach. This may result in a tamponade of low-pressure venous oozing during the procedure, as previously suggested by others (13). Also, different transection devices during the procedure might reduce the need for prolene stitches and haemostatic clips which in some cases can be time consuming. In this study of initial experience of laparoscopic hepatic resections, the conversion rate of 14% was in concordance with previous reports of 1–26% (1 –4, 6, 16). Both conversions were performed after the use of laparoscopic ultrasound to determine whether a safe resection was possible. Furthermore, this study was not designed for long-term outcome; however, no long-term complications were observed in the laparoscopic group in contrast with two symptomatic incisional hernias in the open group.
It is interesting to observe that there were no significant differences in hospital stay between the open and laparoscopic approach. Striking is the relatively long stay in hospital for the laparoscopic procedures. This was previously also observed for colonic resections before and after the start of a peri-operative multimodal fast track setting (Enhanced Recovery After Surgery; ERAS®) (22). Although in this recent study predefined discharge criteria were assessed, almost 90% of the ERAS patients were not going home on the day the discharge criteria were actually met. After careful investigation for valid reasons of prolonged stay, 69% of this extended hospital stay was labelled as inappropriate. Only a minority was rated as medically necessary. Similar observations of prolonged length of stay after the discharge criteria are fulfilled, were also reported in the first study on fast track laparoscopic liver surgery (23).
The oncologic principle outweighs the assumed benefits of the laparoscopic technique such as rapid recovery, short postoperative stay and cosmetic aspect. Improvement of overall survival remains the ultimate goal for resection of liver metastases and should not be compromised for the functional postoperative advantages of the minimally invasive approach. Radical resection, tumour free margins and the ‘no touch’ technique are mandatory (2, 24). This is effectuated with the use of extraction site protections and endo-bags for the specimens. Also, intra-operative ultrasound is reported to be one of the most important factors to reduce positive resection margins and it helps avoiding injury to deeply seated lesions (2). This can be performed laparoscopically to improve outcome (1, 25) and its routine use should be advocated (2). An additional advantage of the laparoscopic approach in combination with the laparoscopic ultrasound is the avoidance of unnecessary exploratory laparotomy in cases with peritoneal metastases or otherwise irresectable disease (26 –28).
Results of long term follow up amongst others in patients with cancer are required to determine the exact place of laparoscopic liver resection in treating patients with solid liver tumours. The data from other studies on laparoscopically resected liver tumours show no difference in oncologic clearance and similar overall and disease free survival rates as in open surgery (1, 29, 30). Laparoscopic liver resections proved to be faster, which is remarkable to some extent as most laparoscopic procedures require more time than their open counterparts. The reasons for this are speculative but may relate to the use of different equipment. This may be a valid subject for a randomised controlled trial.
The indication for laparoscopic liver resection should not be different from an open resection: benign abnormalities as symptomatic liver cysts, hepatocellular adenoma, symptomatic focal nodular hyperplasia, symptomatic haemangioma and malignancies such as hepatocellular carcinomas (HCC) and liver metastases (1, 2, 5, 7). In this study, the pre-operative indications for the minimally invasive technique were malignancy, symptomatic benign solid lesion or uncertain nature of the tumour requiring excision. The choice for the open or laparoscopic approach is mainly determined by the size and location of the lesion and the experience of the surgical team.
In conclusion, the introduction of the laparoscopic technique for left lateral hepatic lesions is equivalent to the open technique with regard to total costs and is safe, feasible, and can be used for diagnosis, preoperative staging and finally resection. The indication for operating benign lesions should not be changed, however, the benefits of the laparoscopic technique especially nominate the use in a selected group of patients with symptomatic benign lesions, uncertain diagnosis or suitable hepatic locations of malignancies.
Footnotes
ACKNOWLEDGEMENTS
We thank T. Lodewick and E. Wong-Lun-Hing of the Department of Surgery of the Maastricht University Medical Centre, for their kind assistance in retrieving the long term follow-up data.