
Abstract
Background and Aims
High ligation of the inferior mesenteric artery may jeopardize blood supply to the proximal bowel. We undertook this study to review the clinical features and outcomes of patients who developed proximal bowel necrosis after high ligation of the inferior mesenteric artery, and to assess the incidence and the risk factors for this complication.
Materials and Methods
A retrospective analysis of patients undergoing high or low ligation for sigmoid colon and rectal cancer with a primary anastomosis between April 2004 and March 2009 was performed. Patient and tumor characteristics and the incidence of bowel necrosis were reviewed.
Results
Four hundred and nine patients were included to the analysis. Six out of 302 patients (2.0%) with high ligation developed proximal bowel necrosis, while the remaining 107 patients with low ligation did not suffer from this complication. All patients who developed proximal bowel necrosis underwent secondary surgery with resection of necrotic bowel. The pathological examination of the resected specimen revealed mucosal to transmural ischemic necrosis without the evidence of vascular thrombosis or embolic occlusion. Univariate analysis revealed that advanced age, cerebrovascular disease, and hypertension were significantly associated with proximal bowel necrosis. Multivariate analysis demonstrated that cerebrovascular disease was an independent predictor of this complication. Of these six patients, two died from associated complications.
Conclusions
Proximal bowel necrosis after high ligation is potentially fatal, and this report provides a warning in clinical settings where high ligation is indicated. Further studies are warranted to evaluate its distinct relationship with high ligation and to clarify whether low ligation would be a safeguard.
Keywords
INTRODUCTION
The optimal level of vascular ligation of the inferior mesenteric artery (IMA) in left-sided colon and rectal cancer surgery remains an area of debate with regard to anatomical, technical, and oncologic perspectives. These debates continue, however, with the lack of prospective, randomized controlled trials (1, 2). Generally, the level of vascular ligation of the IMA is divided into high ligation (ligation at the origin from the aorta) and low ligation (below the origin of the left colic artery (1, 2). High ligation is typically performed with an en bloc lymphadenectomy along with the IMA trunk including apical lymph nodes, allowing precise tumor staging and more accurate prognostic predictions (2).
Of particular concern is whether high ligation contributes to a decreased blood supply to the bowel and thereby increases the incidence of an anastomotic leak. Previous studies have demonstrated that intestinal blood flow or tissue oxygen tension was significantly reduced after high ligation of the IMA (3, 4, 5). Seike et al (5) suggested that the patients exhibiting significant fall in blood flow after clamping of the IMA may be at risk of developing anastomotic ischemia and therefore the left colic artery should be preserved for those individuals, while Corder et al (6) found no statistical difference in anastomotic leak rate between the patients with flush aortic tie and those with whom the ascending left colic artery was preserved. Despite the well-known risk of ischemia in the proximal bowel after high ligation, there is a paucity of literature demonstrating the actual incidence and the factors predictive for proximal bowel ischemia.
Over the past five years, we have inadvertently experienced that six patients developed an anastomotic leak after high ligation of the IMA, due to ischemic necrosis of the proximal bowel limb (proximal bowel necrosis). Therefore, we undertook this study was to review the clinical outcomes of patients who developed proximal bowel necrosis after high ligation of the IMA, and to assess the incidence and the risk factors for this complication.
MATERIAL AND METHODS
PATIENTS
Following approval of the Institutional Bioethics Committee, the records of 488 patients who underwent surgical resection with high or low ligation of the IMA for sigmoid colon and rectal cancer with a primary anastomosis between April 2004 and March 2009 were retrospectively reviewed. Seventy-nine patients with pathological diagnosis of T1 or less were excluded, since high ligation is unnecessary in these individuals for oncologic reasons (7). Tumor location was classified according to the rules of the Japanese Society for Cancer of the Colon and Rectum (8). Finally, patient and tumor characteristics, surgical data, and the incidence of proximal bowel necrosis were analyzed in 409 patients.
SURGICAL PROCEDURE
Surgery was performed by a team drawn from two senior colorectal surgeons, three staff surgeons, and the surgical residents under their supervision. General surgical principles followed were based on published practice parameters (9, 10). High ligation included ligation of the IMA at its origin from the aorta including a dissection of apical lymph nodes (11). Indications for high ligation included clinical diagnosis of stage T2 or greater tumors, patients without systemic co-morbidities that significantly increase surgical risk, non-elderly patients, and those without substantial atherosclerosis found pre- or intraoperatively at the root of the mesenteric arteries. Atherosclerosis at the root of mesenteric arteries was defined as severe lumenal stenosis with calcification on preoperative CT or defined intraoperatively when encountered technical difficulty for arterial ligation due to profound sclerosis. Patients who do not qualify these indications underwent low ligation.
The splenic flexure was not routinely mobilized, but was taken down as necessary to achieve a tension-free anastomosis based on the experience and judgment of the attending surgeon. The anastomotic technique included single or double stapling, and transanal hand-sewn coloanal anastomosis. The length of proximal bowel resection margin was obtained at least 10cm, with consideration of the arterial blood supply to that segment. Perfusion of the proximal bowel limb was assured by either direct vision of vascular pulsation or hemorrhage upon cutting the edge of the marginal vessels. The integrity of the anastomosis was ensured by an air-insufflation test, followed by placement of a pelvic drain.
POSTOPERATIVE HEMODYNAMICS AND FLUID MANAGEMENT
Postoperative hemodynamics management consisted of basic non-invasive monitoring of heart rate, arterial pressure, and arterial hemoglobin saturation until ambulation within 24 hours after surgery. The standard protocol for postoperative intravenous fluid support consisted of hypotonic crystalloid solution with 5% glucose and the fluid was maintained with 1.5ml/kg/hour during fasting period. Vasoactive drugs were not administered routinely. If significant fluid loss through drain or stoma, or clinical signs indicating dehydration was observed, isotonic crystalloid solution was given to achieve a minimum arterial pressure of 80 mmHg.
STATISTICAL ANALYSIS
Univariate analysis was performed using the chi-squared test or Fisher's exact test for categorical values, and the Student's t-test for numerical values. Multivariate analysis with stepwise logistic regression model was performed in order to identify independent factors associated with proximal bowel ischemia. Only factors that were found on univariate analysis to be statistically significant (p < 0.05) were assessed in the multivariate analysis. Statistical analyses were carried out using SPSS version 11.0J software (SPSS, Chicago, IL). A p-value less than 0.05 was considered statistically significant.
RESULTS
PATIENT AND TUMOR CHARACTERISTICS, SURGICAL DETAILS AND INCIDENCE OF PROXIMAL BOWEL NECROSIS
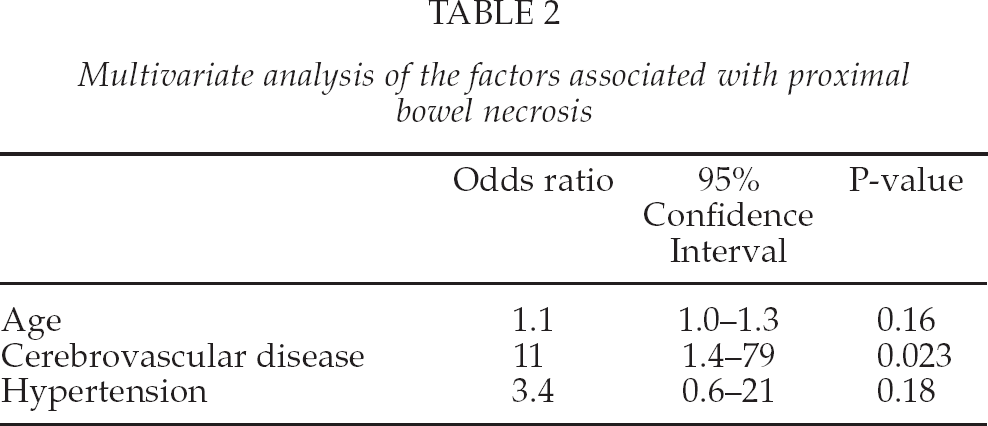
The information regarding the level of arterial ligation (high or low ligation) was successfully retrieved from the operative reports in all 409 patients included. High ligation was performed in 302 patients and low ligation was performed in 107 patients. Six out of 302 patients (2.0%) with high ligation developed clinically evident and pathologically confirmed proximal bowel necrosis, while no patients with low ligation suffered from this complication. There were 8 patients who were clinically diagnosed as occlusive peripheral arterial disease in those underwent low ligation, while there was no such patient in those underwent high ligation. As proximal bowel necrosis occurred exclusively in patients with high ligation, subsequent analysis was performed in order to identify the risk factors in those with high ligation. Patient and tumor characteristics and surgical details are summarized in Table 1. Univariate analysis of the significance of each factor reviewed shows that patients with proximal bowel necrosis were statistically significantly (p < .05) of advanced age, have a history of cerebrovascular disease, or a history of hypertension. Multivariate analysis revealed that a history of cerebrovascular disease to be an independent factor predictive of proximal bowel necrosis (Table 2).
Univariate analysis of the factors associated with proximal bowel necrosis
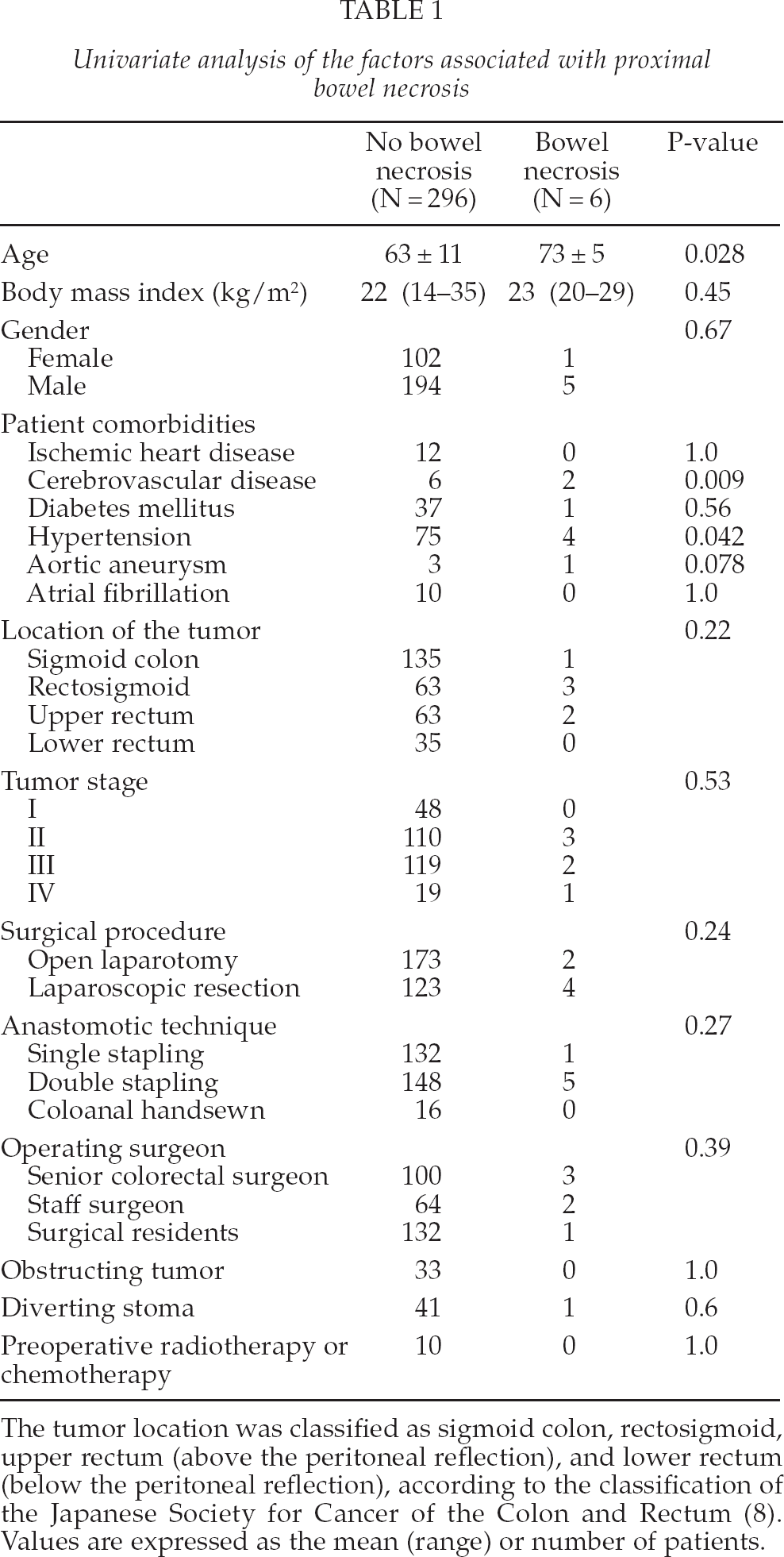
The tumor location was classified as sigmoid colon, rectosigmoid, upper rectum (above the peritoneal reflection), and lower rectum (below the peritoneal reflection), according to the classification of the Japanese Society for Cancer of the Colon and Rectum (8). Values are expressed as the mean (range) or number of patients.
Multivariate analysis of the factors associated with proximal bowel necrosis
CHARACTERISTICS OF PATIENTS WHO DEVELOPED PROXIMAL BOWEL NECROSIS
None of the six patients required a mobilization of splenic flexure for a tension-free anastomosis. None of the six patients received hemodynamic support with vasoactive drugs during the immediate postoperative period. The median duration between the initial and the secondary surgical procedures was 5.5 (range 2 to 13) days. Clinical signs suspicious of anastomotic leak included fever in 2, abdominal pain in 2, abdominal distension in 2, change in drain content in 3, tachycardia in 3, and hypotension in 2 patients. As for laboratory data, elevation of white blood cell count in 4, C-reactive protein in 6, total bilirubin in 3, and lactate in 2 patients. Bowel ischemia was eventually diagnosed by contrast-enhanced CT in 4, and endoscopic examination in 2 patients.
A representative image of CT scan is shown in Fig. 1. Of the six patients with proximal bowel ischemia, a Hartmann's procedure was performed in five patients, and a primary re-anastomosis with diverting ileostomy was performed in one patient. One patient required re-operation because of further ischemic necrosis of the stoma created at the second operation. A representative image of resected necrotic bowel is shown in Fig. 2. The median length of necrotic bowel segment was 16.5 (range 5–35) cm. Pathological investigation of the resected specimen revealed mucosal to transmural necrosis with neutrophilic infiltration but without any signs of vascular thrombosis or embolic occlusion in all patients.

Contrast-enhanced CT scan shows a gas- and fluid-filled bowel loops with lumenal dilation, hypoattenuating thinned bowel wall, and adjacent mesenteric fat stranding (arrows). These findings suggest transmural bowel ischemia.
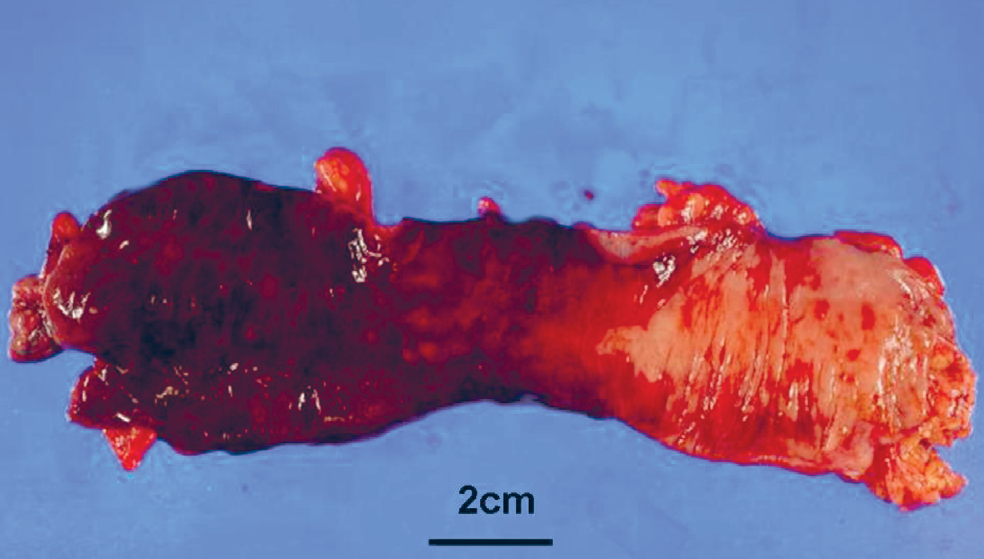
The resected specimen exhibits segmental full-thickness necrosis (left side) and sparing of the normal mucosa (right side).
One patient who underwent colorectal re-anastomosis developed a minor anastomotic leak which was successfully managed by non-operative treatment including pelvic drainage. Finally, stoma reversal was successfully done in only one patient. Two patients died from surgery-associated complications, resulting in an in-hospital mortality rate of 33%.
DISCUSSION
This study demonstrates that life-threatening ischemic necrosis of the proximal bowel occurred in 2.0% of patients undergoing high ligation for sigmoid colon and rectal cancer surgery. Surprisingly few reports have focused on the clinical significance of bowel ischemia after high ligation. Seike et al (5) observed that two patients undergoing sphincter-preserving surgery developed ischemic anastomotic complications (one anastomotic leak and one with stenosis) in a group of 47 patients with high ligation. Their reported incidence of anastomotic leak associated with bowel ischemia (1/47 = 2.1%) is similar to that in the current study.
The length of necrotic bowel segments ranged from 5 to 35 cm (median 16.5 cm). This finding may indicate that a more extensive bowel resection would have been necessary to obtain an adequate blood supply to the terminal segment of the proximal bowel. In fact, this assumption has been supported by previous literature, in which the authors concluded that sigmoid colon should be sacrificed based on the observed diminished tissue oxygenation after high ligation (3).
Nevertheless, it is difficult to determine intraoperatively at which point the bowel should be optimally transected. Surgeons attempt to transect the bowel where it is oncologically safe as well as being viable. Extended bowel resection may necessitate mobilization of the splenic flexure to achieve a tension-free anastomosis. However, this requires longer operative time without affecting the incidence of anastomotic leak (12), resulting in unnecessary surgical procedures for a majority of the patients. Moreover, a recent anatomical study showed that low ligation was applicable in 80% of individuals in order to achieve tension-free anastomosis for total mesorectal excision (13). Routine extended bowel resection including mobilization of the splenic flexure may not be the definitive solution for prevention of proximal bowel ischemia.
In patients with proximal bowel necrosis, tumors were located in the recto-sigmoid in three, upper rectum in two, and sigmoid colon in one patient. There were no cases with lower rectal cancer for which a longer bowel limb is generally required to safely perform an extraperitoneal anastomosis. This implies that the level of anastomosis may not contribute to the bowel ischemia.
Inadequate blood supply to the anastomosis is one of the risk factors for development of an anastomotic leak which is multi-factorial in nature (14). To distinguish patients with bowel necrosis from those without bowel necrosis, an attempt was made to identify patient-specific risk factors of bowel ischemia. As shown in Table 1, patients with advanced age, cerebrovascular disease, and hypertension may be at significantly increased risk of developing proximal bowel necrosis. Subsequent multivariate analysis demonstrated that cerebrovascular disease was an independent risk factor of proximal bowel ischemia (Table 2). These parameters are indicators of atherosclerosis. The Aortic Calcification Score (15) provides an objective assessment of the severity of abdominal aortic calcification, therefore it may be useful to employ this score in the future study as one of the predictors of bowel ischemia after colorectal resection. A recent review suggests that patients with atherosclerotic diseases might benefit from low ligation, yet the ability of this to maintain anastomotic perfusion has not been proven (1). However, this study is a retrospective, uncontrolled case series suggesting cautious interpretation of the results. The statistical significance of the aforementioned risk factors was found in an extremely small number of patients who developed proximal bowel necrosis.
Four of the 6 patients with proximal bowel necrosis underwent laparoscopic resection at the initial surgery. Although the univariate analysis did not show statistical difference in the incidence of proximal bowel necrosis between patients undergoing open laparotomy (1.1%) and laparoscopic resection (3.1%), this result can be considered clinically relevant. The contributing factors for this clinical relevance remain to be investigated; for instance, the lack of ability to directly assess mesenteric arteriosclerosis during laparoscopic resection (intracorporeal vascular ligation) might be partly involved.
It is difficult to determine the exact cause of the bowel necrosis which may not have been directly caused by high ligation. Other factors affecting systemic blood supply such as postoperative dehydration or systemic hypotension during the recovery phase can also be implicated. Meticulous postoperative management to prevent dehydration, systemic hypotension or delayed ambulation is part of routine practice and may be less important as a causative role in developing bowel ischemia.
Preoperative assessment of the vascular network using CT angiography, quantitative assessment of blood flow by laser Doppler flow studies (5), or measurement of colonic oxygenation (3, 16) have all been evaluated as methods to assess vascular flow in the bowel. However, these modalities have not been widely implemented, possibly due to the lack of constant availability and/or the variability in interpretation of the values.
On the basis of this study it can be concluded that proximal bowel necrosis after high ligation is potentially fatal, and the predictive factors of this complication include advanced age, cerebrovascular disease, and hypertension. Further studies are indicated to elucidate more precise risk factors of proximal bowel ischemia as well as its distinct relationship with high ligation, and to clarify whether low ligation would be a safeguard. Indication of high ligation for sigmoid and rectal cancer must be carefully considered based on the oncologic standpoint with individual patient's risks, while the oncologic benefit of high ligation with IMA node dissection appears to be more obvious in patients with non-disseminated sigmoid pT4 tumor (17). The ideal method to intraoperatively assess viability of the bowel has not yet been developed, and thus it is impossible to ascertain optimal perfusion of the proximal bowel limb in all patients undergoing colorectal resection. This report provides a warning in clinical settings where high ligation is indicated.
Footnotes
ACKNOWLEDGEMENTS
The authors have no financial support. All authors state that there is no conflict of interest.