
Abstract
Background
Emergent cricothyroidotomy remains an uncommon, but life-saving, core procedural training requirement for emergency medicine (EM) physician training. We hypothesized that, although most cricothyroidotomies occur in the emergency department (ED), they are rarely performed by EM physicians.
Methods
We conducted a retrospective analysis of all emergent cricothyroidotomies performed at two large level one trauma centers over 10 years. Operators and assistants for all procedures were identified, as well as mechanism of injury and patient demographics were examined.
Results
Fifty-four cricothyroidotomies were performed. Patients were: mean age of 50, 80% male and 90% blunt trauma. The most common primary operator was a surgeon (n = 47, 87%), followed by an Emergency Medical Services (EMS) provider (n = 6, 11%) and a EM physician (n = 1, 2%). In all cases, except those performed by EMS, the operator or assistant was an attending surgeon. All EMS procedures resulted in serious complications compared to in-hospital procedures (p < 0.0001).
Conclusions
1. Pre-hospital cricothyroidotomy results in serious complications. 2. Despite the ubiquitous presence of emergency medicine physicians in the ED, all cricothyroidotomies were performed by a surgeon, which may represent a serious emergency medicine training deficiency.
INTRODUCTION
Emergent cricothydoidotomy remains the gold-standard procedure for airway access when other orotracheal or nasotracheal methods of airway control fail. The need for this emergent surgical intervention can arise rapidly and unexpectedly during the evaluation of trauma patients in the emergency department (ED). The two most common physician groups exposed to this scenario are emergency medicine (EM) and surgery. Due to the relative rareness of the procedure, technical expertise is required to safely access the airway under duress, which may be obtained through either training program. We hypothesized that, although both groups are present for initial intake and evaluation of trauma patients, EM physicians rarely perform the procedure.
MATERIALS AND METHODS
Following institutional review board approval at two large urban Level One trauma centers, a ten year retrospective analysis of all emergent crocothyroidotomies was performed from 2000 to 2010. Emergency medicine trainees (PGY 3 or 4) and surgery trainees (PGY 3–8) from Accreditation Council for Graduate Medical Education (ACGME) approved training programs are both routinely represented at the initial intake and evaluation of trauma patients at both institutions. Patient demographics, Glasgow Coma Scale, mechanism of injury, cricothyroidotomy operator, cricothyroidotomy assistant, post-graduate year (PGY) level of operator and assistant, complications and subsequent conversion to tracheostomy were noted. The primary operator was defined as the individual performing the majority of the technical portions of the cricothyroidotomy, while the assistant was defined as the individual providing immediate supervision to the primary operator or as providing immediate technical assistance critical to the performance of the procedure. Where appropriate, statistical analysis was conducted using Mantel—Haenszel chi-square tests to compare complication rates.
RESULTS
Over 10 years, 59,371 trauma patients were screened and 84 emergent cricothyroidotomies were identified. Of these, only 54 complete records were available for analysis. Both institutions contributed approximately equally to the data pool (30 patients from Boston and 24 from Miami). Patients had a mean age of 50 +/–15 years, 80% were male and 90% presented as a result of blunt trauma. Of those presenting with blunt trauma, motor vehicle crash was the inciting traumatic event in 95%. Patients had a presenting GCS of 8 +/–5 and 85% had prehospital loss of consciousness. All patients had at least 2 in-hospital failed direct laryngoscopic orotracheal intubation attempts.
Results are summarized in Table 1. In 47 (87%) cases, the primary operator was an attending surgeon or surgical trainee. Of these 47 cases, an attending surgeon was the primary operator in 13 cases, and a PGY 6.4 +/−1.2 surgical trainee in 34 cases. Assistants were attending surgeons in 40 cases and PGY 6.2+/− 1.1 surgical trainees in 7 cases. The complication rate was 10% in this group: 2 minor wound infections and 3 surgical site bleeding events requiring surgical control (suture ligation of an injured vein). EMS performed 6 prehospital cricothyroidotomies, all resulting in a complication: 2 pre-tracheal airways placements, 1 inadvertent tracheostomy, and 3 surgical site bleeding events requiring surgical control upon arrival to the trauma center. One cricothyroidotomy was performed by a PGY 4 EM trainee as primary operator without complication. The serious complication rate for prehospital cricothyroidotomies was higher than in-hospital performed procedures (p < 0.0001). Twenty-four cricothyroidotomies were eventually converted to tracheostomies to facilitate long term respiratory care.
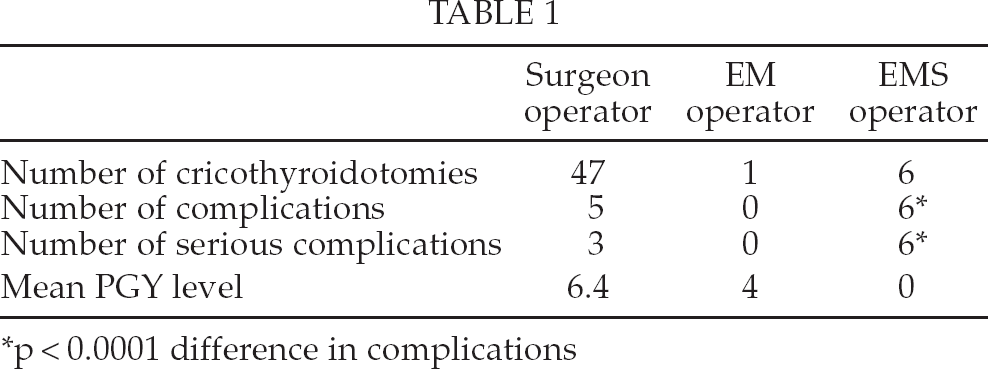
p < 0.0001 difference in complications
DISCUSSION
Emergent cricothyroidotomy is a relatively simple procedure, generally performed under the most undesirable and unexpected of circumstances. Both EM physicians and surgeons may be called upon to perform the procedure on trauma patients. This analysis demonstrates that, despite the ubiquitous, simultaneous presence of both physician groups during initial trauma intake and evaluation, EM physicians rarely perform the procedure. Among the surgeon operators and assistants, the level of training (PGY year) of the surgical trainees performing the airway procedure was quite advanced. We have additionally demonstrated that the cricothyroidotomies performed in the prehospital environment by EMS providers universally resulted in a serious complication.
Both EM and surgical training programs have procedural requirements mandated by the Accreditation Council for Graduate Medical Education (ACGME), American Board of Surgery (ABS), and the American Board of Emergency Medicine (ABEM) (1 –3). The ACGME cricothyroidotomy procedural training requirement for EM residents is 3 procedures, inclusive of patient care and laboratory simulation (1). The ABEM requires 3 procedures in order to be eligible for initial board certification in Emergency Medicine (3). For surgical residents, the ACGME and ABS are less specific with regard to this procedure, requiring 24 head and neck operative cases, 44 vascular cases and 10 trauma cases, without concessions for simulations (1, 2). The 24 head and neck cases may include cricothyroidotomies, but also may include tracheostomies, radical neck dissections, parotidectomies, etc (1). The 44 vascular and 10 trauma cases may include neck surgery, such as carotid endarterectomy and neck exploration for trauma resulting in any variety of neck and tracheal operative experiences (1). This poses an unusual training dilemma for both specialties, as it is entirely likely that both trainees will graduate having never performed a cricothyroidotomy on an actual patient. This is complicated more by the data generated in this study, which suggests that even when the opportunity and necessity for a cricothyroidotomy arises, EM trainees rarely, if ever, perform it. The procedure is clearly dominated by surgeons and surgical trainees.
One may speculate that surgical trainees are far more comfortable operating in the neck due to their additional operating on the same anatomy during related procedures. This could result in development of a certain comfort level for doing a much simpler procedure (emergent cricothyroidotomy) after having performed multiple far more complicated procedures within the confines of the same anatomic region (for example elective tracheostomy, tracheal resection and reconstruction, carotid endarterectomy, neck exploration for trauma, etc). Consequently, when the necessity arises for emergent airway access, the most comfortable operators immediately push their way to the neck of the dying patient. This operator is far more likely to be an advanced surgical fellow-level trainee than an EM trainee. In this series, the operators, on average, were PGY-6 level surgical trainees or greater.
Herein lies the nebulous debate revolving around the training of resident physicians. From the trainee standpoint, it is perhaps unlikely that the PGY-6 surgical trainee with 60 or more neck cases will have profound educational benefit from performing a cricothyroidotomy since this operator has far more experience operating in the neck. The EM trainee, alternatively, stands to educationally benefit dramatically from performance of even a single cricothyroidotomy, as this is likely to be this trainee's only surgical procedure in the neck during their entire residency. Since these procedures are decidedly uncommon, one much question which trainee should be “getting” them when the opportunities present themselves. Some thought should be given to this, likely individualized to each training program.
The importance of appropriate supervision of all trainees performing a surgical procedure by an attending surgeon is clear. What remains unclear, however, is which trainees the attending surgeon should be taking through the procedure. Should we, as surgical faculty, be making a conscious effort to engage our EM colleagues when the need for this uncommon procedure arises? What represents an equitable distribution of training between the two specialties? Should attending surgeons stand aside while EM attendings perform the procedure with their trainees?
Complications from prehospital cricothyroidotomy were universal in this series, and this is consistent with complication rates reported by others for these prehospital procedures (4, 5). Prehospital surgical airway management has also been reported to have an associated mortality rate as high as 40% (6, 7). Other authors suggest that prehospital intubation failures should be ventilated by bag valve mask alone until definitive airway management can be undertaken after arrival to the hospital (8). Clearly, this particular issue requires additional investigation.
This series demonstrates a serious training divide in performance of an uncommon, but lifesaving procedure that all surgery and EM trainees must master. Training remains a core value to the academic trauma surgeon, however, our commitment to training must not end at the borders of our own residency programs. Attending surgeons, for a variety of reasons, appear to be performing or immediately supervising nearly every ED cricothyroidotomy. This places surgeons in a position to facilitate training across specialties. Consequently, attending surgeons must make a conscious effort to include EM trainees in the emergent airway access of the trauma patient.