
Abstract
Aims
Over the past 20–25 years, Sweden has placed growing focus on local alcohol prevention, as reflected in national action plans. However, municipal efforts vary considerably. Identifying the factors that influence stronger local alcohol prevention is important, given its association with reduced alcohol-related harm. The present study aims to examine the characteristics of municipalities with more comprehensive alcohol prevention efforts, focusing on: (i) need, indicated by alcohol consumption and related problems; (ii) financial resources; (iii) political orientation; and (iv) sociodemographic and socioeconomic factors.
Methods
Local alcohol prevention is measured using a developed version of the Alcohol Policy Magnitude Measure (APMM), covering 209 municipalities from 2011 to 2021. Linear and logistic regressions examine how APMM scores relate to factors such as alcohol use, harm, resources, politics and demographics. Both crude and adjusted models assess the robustness of these associations.
Results
Left-wing governance, larger populations and younger demographics were consistently linked to higher alcohol prevention levels. Of four need indicators, only one showed a consistent association. Financial resources were significant only in adjusted models, while education and foreign background showed mixed results. Unemployment was not associated with alcohol prevention, and income was significant only in crude models. These patterns were largely confirmed in analyses focusing on the top 10% of municipalities in terms of prevention activity.
Conclusions
Stronger alcohol prevention was not linked to higher consumption, harm or resources, but rather to left-wing governance, larger populations and younger residents. This highlights the influence of political and sociodemographic factors on local prevention levels.
Introduction
Over the past 20–25 years, many countries have increasingly emphasized local alcohol prevention initiatives in response to a weaker national alcohol policy (Giesbrecht, 2007; Mooney et al., 2017). This development is evident in Sweden where local alcohol prevention has been repeatedly highlighted in national alcohol action plans (Nilsson et al., 2020). Although Swedish municipalities are legally responsible for licensing and supervising alcohol sales in the municipality under the Alcohol Act (2010:1622), they are not legally obliged to conduct specific local alcohol prevention work. This absence of a formal mandate may help explain some the substantial variation in the scope and intensity of local alcohol policy efforts across Swedish municipalities (Leifman et al., 2018). Because increases in local prevention efforts are likely associated with a reduction in alcohol-related problems (Nilsson et al., 2018, 2020), it is essential to get a more comprehensive understanding of the factors contributing to these differences – particularly the characteristics of municipalities with stronger prevention efforts. The present study aims to examine characteristics of Swedish municipalities that demonstrate a higher level of prevention activity, with a focus on the following aspects:
Need, indicated by the level of alcohol consumption and alcohol-related problems in the municipality. Financial resources, reflected by the municipality's overall economic capacity. Political will, inferred from the political leadership and governance of the municipality. Sociodemographic characteristics of the municipality such as age distribution, population size and socioeconomic indicators.
It is reasonable to assume that alcohol prevention efforts are prompted by a clear need in terms of widespread alcohol-related harm impacting both individuals and society. This idea is in line with the concept of “problems stream”, which is a key component in Kingdon's influential model for understanding policy making (Kingdon & Stano, 1984). In this context, a key driver of stronger local alcohol prevention is a visible occurrence of alcohol-related problems. To date, no study has specifically examined this question in the context of local alcohol prevention in Sweden. However, one study using a broader prevention measure, including alcohol, drugs, tobacco and doping, found that municipal levels of harm in Sweden did not correspond to differences in prevention efforts in 2016–2017 (Folkhälsomyndigheten, 2020). A similar conclusion was reached in a recent report to a Swedish governmental inquiry, which analyzed roughly the same data on local prevention and harm, but for the more recent period 2016–2021 (Leifman, 2023). However, international research examining harm rates in relation to local alcohol prevention suggests that levels of need may influence prevention efforts. For instance, an Australian study found that the level of alcohol-related harm significantly influenced local government prevention efforts (Guizzo et al., 2021) and another study of local policy drivers in England found that community experiences of alcohol-related harms were important support for new local licensing policies (Reynolds et al., 2020). Thus, existing research offers mixed findings.
Studies in health economics suggest that health care spending tends to increase as gross domestic product (i.e. GDP) per capita rises (Fedeli, 2015) and reviews highlight adequate funding as a key factor for successful implementation of local health policies (Guglielmin et al., 2018; Weiss et al., 2016). These findings seem reasonable: given a similar level of need and ambition, municipalities with greater wealth should have more funds to allocate toward preventive measures, enabling them to design and sustain comprehensive initiatives.
Political will at the local level is another potential determinant of local policy efforts. Local democracy in Western countries, including Sweden, is based on the principle of representative democracy, where popular will is translated into policy through three core mechanisms (Karlsson, 2013). First, elections and accountability systems identify and aggregate citizens’ preferences. Second, elected representatives transform these preferences into policy decisions, requiring political authority and expertise. Third, public authorities implement the adopted policies, demanding administrative capacity and resources. In Sweden, political commitment to local alcohol prevention appears to vary across parties because local politicians differ significantly in their views on alcohol policy (Karlsson et al., 2019). Politicians from left-wing parties tend to be more supportive of alcohol policy measures than those from right-wing parties both on a national and local level. Based on this information, we anticipate that municipalities governed by left-wing parties in Sweden will demonstrate a higher level of alcohol prevention activity than those led by right-wing parties.
Previous Nordic research on local alcohol prevention has mainly been directed towards specific community-based programs using various types of environmental strategies to reduce the supply of alcoholic beverages (e.g., the Pakka project in Finland) (Holmila & Warpenius, 2007) and specific prevention initiatives such as Responsible Beverage Research programs in Sweden, Finland and Norway (Skardhamar et al., 2016; Trolldal et al., 2013; Warpenius et al., 2010). A major focus has been on evaluating the impact of these programs in terms of harm whereas studies of determinants of local alcohol prevention work in general are missing in the scientific literature. A few earlier reports of determinants of local prevention in Sweden have suggested that the magnitude of work is related to sociodemographic factors of the municipality such as population size and socioeconomic profile. In short, it seems that larger municipalities, as well as those that are socioeconomically better-off, tend to engage in more preventive work (Folkhälsomyndigheten, 2020; Leifman et al., 2018). Indicators of sociodemographic and socioeconomic conditions in the municipalities will therefore also be related to alcohol prevention in the present study.
To address the research questions outlined above, the magnitude of local alcohol prevention in 209 municipalities in Sweden during the period 2011–2021 will be analyzed in relation to the following characteristics of the municipality: alcohol consumption and prevalence of alcohol-related problems, financial resources, political orientation, and sociodemographic and socioeconomic profile.
Methods
Measures
Municipal alcohol prevention activity was measured by a development of the Alcohol Prevention Magnitude Measure (APMM) (Nilsson et al., 2015) and includes 45 indicators across five categories: (1) policy (e.g., having an alcohol prevention program) (13 indicators); (2) staff and budget (e.g., having av local coordinator) (three indicators); (3) inspections and licenses (e.g., number of supervisions in bars) (six indicators); (4) cooperation (e.g., with the police) (12 indicators); and (5) activities (e.g., working with the joint method against drunk driving) (SMADIT) (Gustafsson et al., 2016) or responsible beverage serving (RBS) (Trolldal et al., 2013) (11 indicators). Each category contributed up to 20 points, for a total of 100. Policy, staffing, and cooperation, comprising key foundations for activities, have been found to be positively correlated with activity scores, while inspections and licenses were not, possibly because they are often handled separately and not seen as direct prevention (Nilsson et al., 2015).
Most of the data used to develop APMM for the period 2011–2021are drawn from a series of annual web-based surveys known as the County Report conducted by the Public Health Agency of Sweden (https://www.folkhalsomyndigheten.se/folkhalsorapportering-statistik/tolkad-rapportering/lansrapporten). The validity of the original APMM is supported by previous research, which indicates that it effectively captures actual changes in local prevention activities (Nilsson et al., 2015).
The analyses include 209 municipalities (out of 290) that had no more than one year of missing data per prevention category in the Alcohol Prevention Index between 2011 and 2021. Missing index values for the years 2012–2020 were imputed using the average of the preceding and following years. For 2011, missing values were imputed using data from the following year, while, for 2021, imputation was based on the previous year's data.
To obtain a broad assessment of co-variates of the level of local alcohol prevention we use two specific outcome measures; the total APMM score (0–100) and whether a municipality belongs to the top decile in terms of the APMM score.
Measures of alcohol prevention need were based on alcohol sales per inhabitant 15 years and older and in 100% ethanol (as an indicator of drinking level in the municipality), as well as alcohol-related mortality, hospitalizations and drunk driving (as indicators of alcohol-related harm). All measures were age-adjusted and reported per 10,000 inhabitants aged 15 years and older.
Financial resources were measured by the income of the municipality consisting of three parts: (1) income from municipality activities (e.g., daycare fees), but also various direct government subsidies; (2) general state grants and equalization representing an “expense” for some, but an income for other municipalities; and (3) municipal taxes expressed in price level of 2011 and per inhabitant in the municipality.
The measure of local political governance was based on data from the Swedish Association of Local Authorities and Regions (SKR) and applied to the three mandate periods during the study period (2010–2014, 2014–2018 and 2018–2022). Municipalities were classified as left-wing governed if led by one or more of the following parties: The Social Democrats (Socialdemokraterna in Swedish), The Left Party (Vänsterpartiet) or The Green Party (Miljöpartiet). Right-wing governance referred to leadership by one or more of the following parties: The Moderate Party (Moderaterna), The Centre Party (Centerpartiet), The Liberals (Liberalerna), The Christian Democrats (Kristdemokraterna) or The Sweden Democrats (Sverigedemokraterna). Mixed governance included coalitions with at least one party from both blocs. The last two categories were combined in the analysis as a reference group to left-wing governance.
Measures of sociodemographic and socioeconomic characteristics of the municipalities were based on data from Statistics Sweden and the Public Health Agency of Sweden and included: population size (number of registered inhabitants living in the municipality), mean income (earnings per inhabitant 20 years and above), mean age, unemployment rate (%) in the age group 20–64 years, proportion (%) with post-secondary education in the age group 25–74 years and proportion (%) with foreign background (i.e., foreign-born or domestically born with two foreign-born parents).
Procedures
Linear regression was used to explore whether alcohol consumption, alcohol-related harm, financial resources, political orientation, and sociodemographic and socioeconomic factors were related to overall APMM scores. Logistic regression was used to assess covariates of being in the top decile of municipalities with the highest prevention levels.
Crude models were estimated to identify the association between each covariate and alcohol prevention and adjusted models were estimated to assess the robustness of the findings when differences in all other co-variates across municipalities were considered. All models controlled for time and focus solely on cross-municipality co-variation.
Sensitivity Analysis
As a sensitivity analysis we performed the analyses on two other samples of municipalities: one with a stricter selection criterium only including municipalities without any missing observation during the study period (N = 122) and one with less strict criteria including municipalities with up to three missing observations per prevention category but not two or more in a row (N = 242).
Results
Differences in Local Alcohol Prevention Efforts in Relation to Municipality Characteristics
Table 1 presents the APMM for 209 Swedish municipalities during the period 2011 to 2021 in deciles in relation to indicators of need, financial resources, political governance, and other socioeconomic and demographic factors.
Magnitude of Alcohol Prevention (APMM) in Deciles (1–10) in Relation to Indicators of Prevention Need, Financial Resources, Political Governance and Other Socioeconomic and Demographic Covariates (209 Municipalities, Average for 2011–2021).
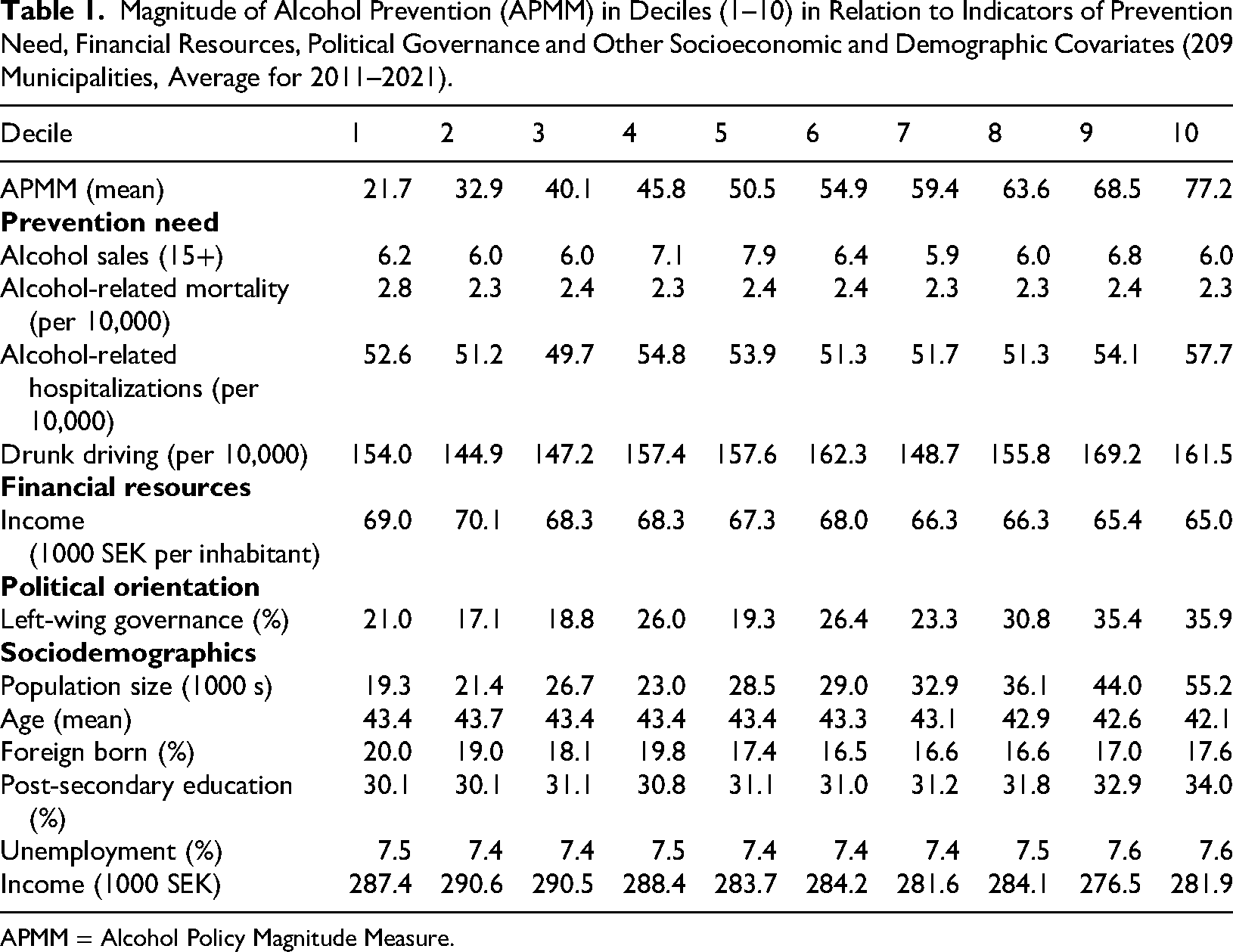
APMM = Alcohol Policy Magnitude Measure.
The findings reveal significant variations in alcohol prevention work, with municipalities in the top decile of the APMM scoring 77.2, which is almost four times higher than municipalities in the lowest decile (21.7). Notably, local alcohol prevention efforts do not appear to align with indicators of need. There is no clear association between the extent of prevention work measured in deciles and levels of alcohol sales, alcohol-related mortality or drunk driving. A similar pattern is observed for alcohol-related hospitalizations, although the highest hospitalization rates are found in the top 10% of municipalities in terms of prevention activity. Furthermore, financial resources do not seem to increase with local prevention efforts, as the level of prevention remains relatively stable across municipalities with varying income levels. Regarding political governance, however, left-wing governance tends to be more common with higher levels of alcohol prevention in the municipality. In the lowest prevention decile, approximately 21% of municipalities are left-governed, compared to 36% in the highest prevention decile.
Among sociodemographic factors, population size is positively associated with alcohol prevention efforts, with an average of 19,000 inhabitants in the lowest prevention decile compared to 55,000 in the highest. Age shows a weaker association, with a slight tendency for higher prevention levels in municipalities with a younger population. The proportion of foreign-born residents decreases as prevention levels increase, while the proportion with post-secondary education rises. Unemployment rates do not appear to be associated with prevention levels, whereas lower average income is linked to higher levels of alcohol prevention.
Estimation of Linear Regression Models
Findings in crude and adjusted linear regression models are presented in Table 2. In crude models, the only significant indicator of need was alcohol-related hospitalizations, while alcohol sales, alcohol-related mortality, and drunk driving had no significant association with the magnitude of local alcohol prevention efforts. The municipalities’ income was not significantly associated with alcohol prevention, whereas the estimate for political orientation in terms of having a left-wing government was positive and significant. Among sociodemographic factors, larger population size, younger age and a higher proportion with post-secondary education were all significantly associated with greater alcohol prevention efforts in the municipality. Alcohol prevention efforts were not associated with unemployment and proportion of foreign-born inhabitants.
Estimated Correlates of Local Alcohol Prevention in Swedish Municipalities 2011–2021 According to Crude and Adjusted Linear Regression Models.
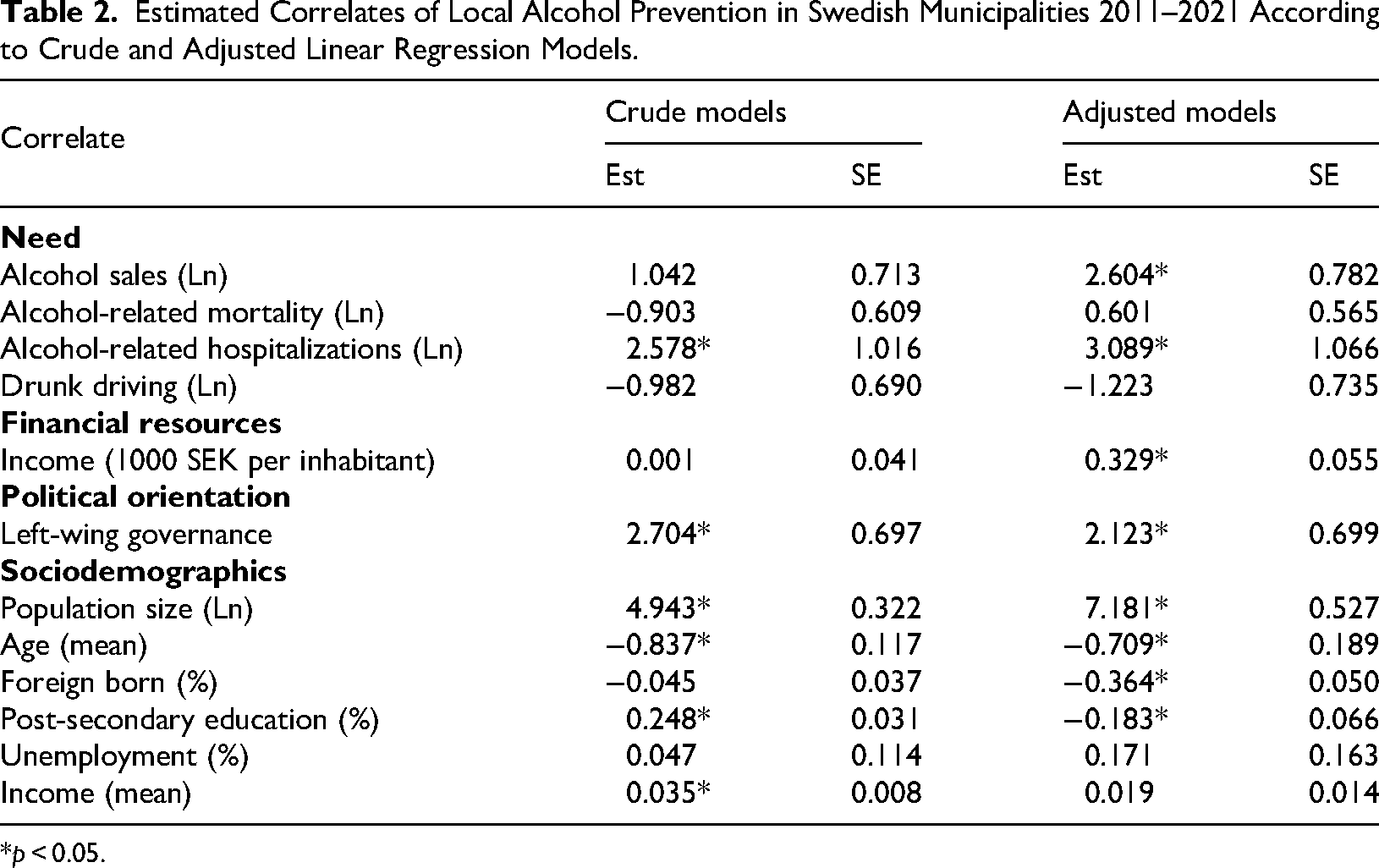
*p < 0.05.
Most results remained in the adjusted model, but some additional variables also reached statistical significance. Alcohol sales and financial resources became positively associated with prevention levels, as did all sociodemographic variables except unemployment and income. Also, the estimate for proportion with post-secondary education changed from positive to negative in the adjusted model.
Estimation of Logistic Regression Models
We also examined whether the same correlates were associated with an exceptionally high level of alcohol prevention by analyzing the likelihood of a municipality belonging to the top 10% with the highest APMM scores.
Overall, the results mirrored those found for overall prevention levels. In crude models, only alcohol-related hospitalizations were significantly associated with being in the top 10% of municipalities, while alcohol sales, alcohol-related mortality and drunk driving were not. Financial resources showed no significant association, whereas political orientation in terms of left-wing governance was linked to top-decile prevention levels. All sociodemographic variables were statistically significant except for income.
Adjusted models essentially confirmed these results though financial resources became significant, while political orientation and unemployment no longer reached statistical significance. Again, the estimate for proportion with post-secondary education changed from positive (odds ratio >1) to negative (<1) in the adjusted model as did the proportion of foreign-born inhabitants (Table 3).
Estimated Correlates (odds ratios) of High Local Alcohol Prevention (Belonging to 10% with Highest APMM) in Swedish Municipalities 2011–2021 According to Crude and Adjusted Logistic Regression Models.
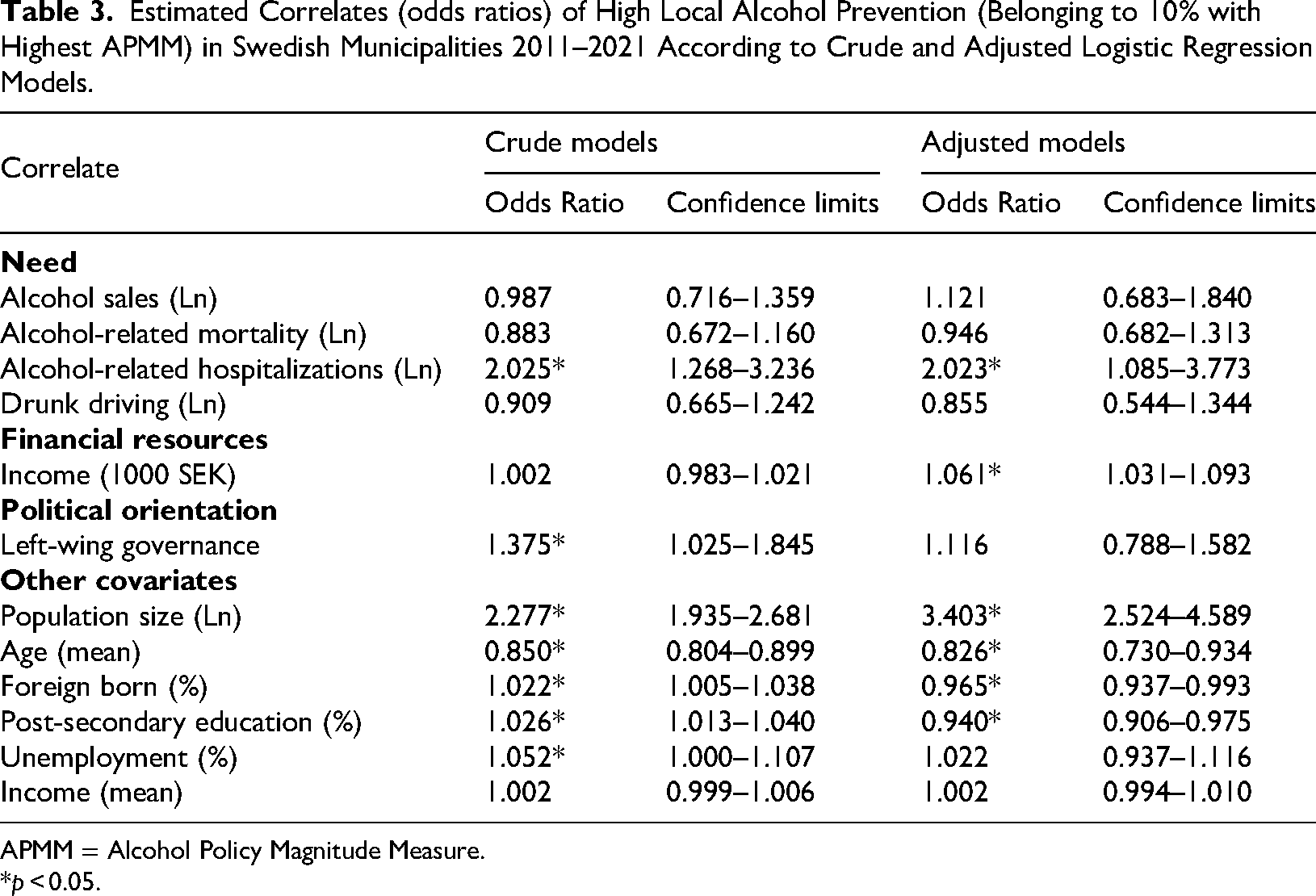
APMM = Alcohol Policy Magnitude Measure.
*p < 0.05.
Sensitivity Analysis
The findings remained at large in adjusted linear models using stricter (N = 122) and more inclusive (N = 242) municipality samples. In the stricter sample, political orientation (p < 0.11), university education (p < 0.78) and income (p < 0.46) were not statistically significant. In the larger sample, the results were in general consistent.
Discussion
The overall aim of the present study was to better understand the substantial variation in local alcohol prevention efforts across Swedish municipalities. This question is motivated by research indicating that higher levels of local alcohol prevention are associated with reduced alcohol-related harm. To shed light on this question, we examined whether specific municipal characteristics were associated with the level of prevention activities, as measured by a modified version of the APMM. Key municipality features included indicators of prevention need (level of alcohol consumption and harm), financial resources, political governance, and sociodemographic and socioeconomic profile. To identify the importance of these characteristics, both crude and adjusted regression analyses were performed.
Left-wing governance, larger population size and a younger population were associated with higher levels of alcohol prevention in both crude and adjusted models, suggesting that these were the most robust features of municipalities with stronger alcohol prevention efforts.
That left-wing governance is linked to higher levels of alcohol prevention efforts aligns with previous research showing a clear ideological divide reflected in party affiliations (Karlsson, 2012). Local councilors on the political left have been found to be more likely than those from right-wing parties to view alcohol-related harm as a societal issue requiring restrictive national policies with the exception of The Christian Democrates. This pattern was also found in a study of various opinions in alcohol policy questions among politicians in Sweden including politicians at the local level (Karlsson et al., 2019). For instance, the view that alcohol is a societal rather than individual issue was supported by a majority among left-wing politicians (82% of The Social Democrats and The Green Party, and 92% of The Left Party) compared to local right-wing politicians (24% of the Moderates and 28% of Swedish Democrates). Furthermore, support for liberalizing alcohol sales—such as allowing wine and beer in grocery stores—was significantly lower among local left-wing politicians (13% of Social Democrats and the Green Party, and 5% of the Left Party) compared to local right-wing counterparts (72% of the Moderates and 67% of Swedish Democrates) (Karlsson et al., 2019). These ideological differences thus appear to translate into varying levels of local alcohol prevention activity, underlining the importance of political will in shaping municipal efforts.
That a larger population is related to more alcohol prevention work in Swedish municipalities has been found in previous studies (Folkhälsomyndigheten, 2020; Leifman et al., 2018) and may come with more resources and administrative capacity to implement preventive programs. It is not clear why lower average age is related to more ambitious alcohol prevention work in the municipality. However, it might reflect a greater focus on youth-related issues, including substance use, when a larger part of the population is young. It is also worth noting that many of the preventive initiatives included in the APMM are directed towards young people.
There was limited evidence that prevention need is a major driver of local alcohol prevention in Swedish municipalities. Only alcohol-related hospitalizations were significantly associated with prevention levels in both models, while alcohol-related mortality and drunk driving were not significant in any model and alcohol sales only in adjusted models.
The lack of a clear association between greater alcohol-related harm and more extensive prevention efforts may have several explanations. First, as this is a cross-sectional study, we cannot rule out that alcohol-related harm is lower as a result of a high level of prevention. Another interpretation is that resource constraints prevent high-need municipalities from implementing comprehensive strategies due to limited funding or staff or other social challenges, causing alcohol prevention to be deprioritized. Some municipalities may also lack the capacity to measure and contextualize their problems, and without objective data, may not perceive a need to initiate preventive efforts.
However, the main finding remained in adjusted models taking several of these factors into account such as income, political governance and several sociodemographic characteristics. Thus, although alcohol-related hospitalizations showed a positive association with prevention levels in adjusted models, municipalities with stronger alcohol prevention efforts are not necessarily those with higher alcohol consumption or more alcohol-related harm.
This finding also align with alternative notions rooted in political science and organizational theory, particularly path dependence (Page, 2006; Pierson, 2000) and bounded rationality. Path dependence theory suggests that, once a policy direction is established, it tends to persist due to organizational inertia. Thus, Swedish municipalities with a history of restrictive or permissive alcohol policies may continue on their established path little affected by changing circumstances. This inertia may result from established routines and inherited policy priorities that are costly to change as well as from local policymakers’ embeddedness in networks of civil servants and interest groups that tend to resist changes to the status quo.
Another notion that might be useful to contextualize our findings on need is bounded rationality, meaning that policy decisions are shaped by cognitive limitations, heuristics and institutional constraints rather than purely rational calculations (Jones, 2003; Simon, 1957). Instead of systematically assessing alcohol-related problems or economic resources, policymakers may rely on simplified decision rules, with political ideology serving as a key heuristic. Hence, left-leaning governances may automatically associate alcohol regulations with public health benefits and prioritize restrictive policies, even in the absence of immediate problem escalation. By contrast, right-leaning governances may emphasize individual responsibility and economic considerations, leading to less emphasis on regulatory approaches, independent of the actual problem burden.
Financial resources were not linked to prevention efforts in crude models, whereas, when controlling for need, political governance and sociodemographic factors in adjusted models, greater financial resources were associated with higher levels of prevention. This suggests that, while not a primary driver, financial capacity may facilitate prevention efforts in some municipalities during certain levels of need, political governance and sociodemographic profiles.
Mixed findings were obtained for the remaining indicators of sociodemographic and socioeconomic profile. For instance, municipalities with a high education profile were related to more prevention in crude models whereas the opposite was found in adjusted models. Also, municipalities with a relatively large proportion of foreign-born inhabitants tend to be negative in adjusted models but not in crude models. This suggests that the extent these factors are related to alcohol prevention is very much influenced by other conditions in the municipality.
Limitations and Strengths
The present study has several limitations. First, the analysis is cross-sectional, which limits the ability to draw causal conclusions. On the other hand, the main aim of the study was not primarily to establish causal factors leading municipalities to work with alcohol prevention, but rather to identify characteristics that distinguish municipalities working a lot with alcohol prevention in Sweden during a 10-year period compared with those with less prevention activity. To establish causality, another research design is needed (e.g., an analysis of changes in these characteristics in relation to changes in alcohol prevention). Second, the prevention measure used is binary, capturing only the presence or absence of prevention activities without accounting for their intensity or scope. Thus, individual prevention indicators do not capture variations in the dose of prevention between municipalities. While this is a limitation, it should be kept in mind that when combining several different individual indicators in an index this measure will capture at least some indication of dose in terms of the number of items included in the index. Third, some potentially important factors influencing prevention. such as the presence of dedicated and enthusiastic staff or other ongoing prevention initiatives, were not included in this study. Because these factors have been suggested to be important in previous studies (Leifman et al., 2018), it is possible that the results might have differed if they had been included. Finally, we excluded municipalities with more than one year of missing data per prevention category in the Alcohol Prevention Index between 2011 and 2021, totaling 78 municipalities. Compared with the analytical sample, these municipalities were smaller (on average 12,000 inhabitants versus 27,000) and more frequently left-wing governed (34% versus 27%). However, the sensitivity analyses presented above indicated that this exclusion did not have a major impact on the results.
This study also has important strengths. It uses unique prevention data covering many municipalities over an extended time period which is rarely seen at the municipal level in other countries. By using the modified APMM across multiple years and municipalities, the study provides a novel, cross-sectional mapping of municipal-level alcohol prevention, offering a framework for future comparative research in Sweden and internationally. Additionally, the analysis includes a wide range of control variables, allowing for a more robust assessment of which municipal characteristics are associated with strong alcohol prevention efforts.
Conclusions
Municipalities with stronger alcohol prevention efforts in Sweden were not necessarily those with higher alcohol consumption, greater alcohol-related harm or greater financial resources. Rather, such efforts were more often associated with left-wing governance, larger populations and younger residents. The results align with theories of path dependence and bounded rationality, suggesting that municipalities tend to maintain established policy trajectories and rely on heuristics, such as political ideology, rather than systematically responding to local need. These findings suggest that tailored support and incentives could potentially be beneficial for strengthening alcohol prevention in municipalities with less favorable political or demographic contexts, rather than presuming that prevention efforts will consistently align with areas experiencing the highest levels of alcohol-related harm.
Footnotes
Funding
The authors disclosed receipt of the following financial support for the research, authorship and/or publication of this article: This work was supported by the Forskningsrådet om Hälsa, Arbetsliv och Välfärd, (grant number 2021-01713).
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.