
Abstract
Aims
Problematic gaming is a distinguishable problem associated with impairments to personal well-being. The Restart program is a novel digital intervention that was designed to help individuals improve their control over excessive gaming. This study aimed to investigate the feasibility and preliminary outcomes of the Restart program on gaming behaviour and well-being among problematic gamers.
Methods
We utilised a quasi-experimental design, including one group with pre-and post-test measurements; no control group was employed. The analysed data described individuals’ life situations, gaming behaviour, problematic gaming, compulsive internet use and subjective well-being. Data were collected at the baseline and post-program time points, as well as 3 months after the end of the program, and analysed using a linear mixed model. At the baseline, 110 individuals engaged in the intervention, and 50 participants completed all pre-, post- and follow-up tests.
Results
Statistically significant differences between the baseline and post-program scores were discerned for all variables. Moreover, the total time spent on gaming and the proportion of problematic gaming time decreased across the post-intervention and follow-up time points, a trend that may reflect changes in gaming control and behaviour. The results also revealed improvements in subjective well-being among participants.
Conclusions
Participants showed improvements in gaming behaviour and well-being, suggesting that participation in the Restart program may be associated with positive changes; however, the findings remain preliminary. Future research should focus on the long-term benefits of such therapeutic approaches.
Introduction
Despite increasing recognition of problematic gaming as a public health concern, there is still a significant lack of evidence-based digital interventions targeting individuals with problematic gaming behaviours, particularly in Western populations and within the framework of selective (secondary) prevention. Most existing interventions are reactive, focusing on treatment after the disorder has emerged, whereas opportunities for prevention and early intervention remain largely unexplored. This study aims to fill these gaps by examining the feasibility and initial outcomes of a new digital intervention developed to support Finnish adults experiencing problematic gaming. We evaluate changes in gaming behaviour and subjective well-being among participants, providing preliminary evidence to inform the development of future interventions and treatment strategies for problematic gaming.
Epidemiology and Aetiology of Problematic Gaming
In Finland, digital gaming is pervasive, with 60% of the population playing at least monthly. Recent data show that about 14% of active gamers experience issues with controlling their gaming at least occasionally, whereas 2.4% report recurrent difficulties (Kinnunen et al., 2024). This minority underscores the need to understand the potential risks associated with gaming, especially given its increasing recognition internationally as a public health issue.
In response to rising concerns, the World Health Organization (WHO) formally classified Gaming Disorder in the International Classification of Diseases, 11th edition (ICD-11) in 2018 (WHO, 2022). This classification emphasises the clinical importance of the condition, characterised by a persistent or recurrent pattern of gaming behaviour – whether online or offline – that leads to substantial impairment in personal, social, educational or occupational functioning. Diagnostic criteria include impaired control over gaming, prioritisation of gaming over other life activities, and continued engagement despite adverse consequences. Although a 12-month duration is typically required for diagnosis, shorter periods may be considered in severe cases. Moreover, the ICD-11 introduced Hazardous Gaming, a related diagnosis that pertains to gaming patterns that elevate the risk of physical or mental health issues. The inclusion of Gaming Disorder has ignited significant debate within the academic community. Critics have expressed concerns regarding the potential overpathologisation of typical gaming behaviour, the absence of strong empirical evidence and the risk of stigmatising gamers, especially young individuals. These issues suggest that its inclusion in the ICD-11 may have been premature and could lead to unintended consequences in both clinical and public health spheres (Aarseth et al., 2017).
Terminology related to gaming issues varies across the literature, with terms such as Internet Gaming Disorder and Problematic Gaming Behaviour often used interchangeably. In the present study, the term “problematic gaming behaviour” is employed to encompass a range of gaming-related issues, from mild to severe impairment.
Globally, the prevalence of problematic gaming is estimated to be around 3% (Kim et al., 2022a; Stevens et al., 2021), although this figure varies significantly by age, gender and region. Males are generally more affected (Mihara & Higuchi, 2017; Paulus et al., 2018), but recent trends indicate an increase in prevalence among females (Kim et al., 2022a; Stevens et al., 2021). In Finland, men still dominate in overall gaming frequency (Kinnunen et al., 2024). Regionally, the highest rates are reported in Asian countries, suggesting that cultural and environmental factors may influence gaming behaviour (Paulus et al., 2018).
Adolescents represent a particularly vulnerable group due to developmental factors. Pertaining, for example, to the maturation of the prefrontal cortex, which governs impulse control and decision-making (King & Delfabbro, 2019). This neurodevelopmental vulnerability has been shown to be further exacerbated by intrapersonal factors such as excessive gaming time, loneliness, anxiety, depression, low self-control, sensation seeking, and impulsivity (Zhuang et al., 2023). Additionally, certain game design features, such as endless gameplay, immersive narratives and reward systems, can heighten engagement and reinforce problematic behaviours (King & Delfabbro, 2019; Paulus et al., 2018).
Interpersonal dynamics have also a significant influence on gaming behaviours. Poor peer relationships, limited social support, and dysfunctional family environments have all been associated with a heightened risk of problematic gaming (Zhuang et al., 2023). Environmental factors such as low school engagement and exposure to adverse life events are also associated with this vulnerability (Zhang et al., 2024). These factors and circumstances often interact, creating a complex web of risk factors that can reinforce and perpetuate problematic gaming behaviours.
This interplay is effectively illustrated by the ecological model of behavioural and mental health (Glanz & Bishop, 2010), which emphasises the interactions among individual, social and environmental domains. For example, individuals with poor emotional regulation may turn to gaming as a coping mechanism, motivated by negative reinforcement (Bender et al., 2020). Likewise, tendencies toward high sensation seeking may result in gaming becoming a primary source of excitement and reward, thereby reinforcing the behaviour through positive feedback loops (Kochuchakkalackal & Reyes, 2020). Additionally, comorbid conditions such as depression and attention deficit hyperactivity disorder (ADHD) are commonly linked to problematic gaming, which may indicate bidirectional relationships that complicate diagnosis and treatment (Brand et al., 2019).
Interventions and Prevention Strategies for Problematic Gaming
Mental health professionals have expressed growing concerns regarding the psychological and physical ramifications of problematic gaming. In response, a greater focus has been placed on developing effective interventions for both treatment and prevention. Review studies have explored various approaches, including psychotherapeutic methods and pharmacological treatments, to address this emerging issue (Chang et al., 2022; King et al., 2017; Mestre-Bach et al., 2022). Among the most extensively researched interventions are cognitive behavioural therapy (CBT), motivational interviewing (MI) and reality training, which are often incorporated into broader therapeutic programs (King & Delfabbro, 2018). These interventions are typically customised to address specific risk and maintenance factors, thereby reducing gaming time and promoting healthier coping strategies.
The therapeutic strategies employed target various psychological and social domains. For example, interventions frequently aim to correct distorted cognitions, improve family dynamics, strengthen social connections, and enhance stress management and self-awareness (Chang et al., 2022; Huang et al., 2024; Kim et al., 2024; King et al., 2017; Mestre-Bach et al., 2022). These multifaceted approaches reflect the complexity of problematic gaming and the necessity for individualised treatment plans.
A recent meta-analysis conducted by Danielsen et al. (2024) provides a thorough overview of the effectiveness of various therapeutic approaches. The findings indicate that, while interventions demonstrate moderately positive effects, the evidence base remains limited. The review highlights the preliminary efficacy of various treatments, including psychotherapy, behavioural interventions and preventive strategies, while also emphasising the need for more rigorous research.
In addition to treatment, the review examines preventive interventions aimed at reducing the incidence of gaming-related issues. These interventions included participatory learning programs, family-based approaches, single-session prevention initiatives and school-based recreational activities. Although some studies reported favourable outcomes, particularly in alleviating symptoms of gaming disorder, the overall evidence remains mixed. Most of these studies were randomised controlled trials. However, only two assessed digital interventions were identified: one focused on virtual reality-based physical activity training for university students (Maden et al., 2022) and the other implemented an online multi-risk prevention program targeting adolescents (Ortega-Baron et al., 2021). These digital interventions tackled both behavioural and relational risks; additionally, their evaluations primarily relied on self-report measures.
Despite the promising findings, the review by Danielsen et al. (2024) identified several limitations within the existing literature. These include potential publication bias, small sample sizes and a lack of long-term follow-up data. Additionally, many studies conflated problematic gaming with broader concepts such as Internet Addiction and a substantial portion of the research originated from East Asian contexts, which may limit its generalisability. Consequently, the authors advocate for more high-quality, pre-registered studies that are adequately powered and utilise standardised outcome measures to enhance the evidence base.
From a public health perspective, early detection and intervention are crucial for alleviating the burden of mental disorders and minimising healthcare expenses (Carney & Myers, 2012). Meta-analyses indicate that selective (secondary) prevention, which focuses on high-risk subgroups, is more effective and cost-efficient than universal or tertiary approaches (Horowitz & Garber, 2006). However, most existing interventions for problematic gaming tend to be reactive, focusing primarily on treatment after the disorder has manifested (Danielsen et al., 2024). The scarcity of evidence-based selective prevention programs (Rumpf et al., 2018; Zajac et al., 2020) highlights a significant gap in current prevention efforts.
In this context, digital health interventions present a promising avenue. These initiatives harness technologies such as smartphones and computers to provide accessible, private and scalable mental health support (Lakes et al., 2022). Digital formats are particularly advantageous for individuals who may be hesitant or unable to seek traditional face-to-face care. Research has demonstrated that digital interventions can be effective for behavioural addictions and other mental health conditions (Andersson & Titov, 2014; Boumparis et al., 2022; Gainsbury & Blaszczynski, 2011). Nevertheless, few digital programs have been specifically tailored to prevent or manage problematic gaming (Balhara & Anwar, 2019), necessitating further research to evaluate their effectiveness and optimise their design (Gorowska et al., 2022; Kim et al., 2022b; Mestre-Bach et al., 2022; Park et al., 2022; Sharma et al., 2022; Zajac et al., 2020).
Ultimately, qualitative research from Finland has shed light on the motivations that drive individuals with gaming problems to seek treatment. Alongside issues of time management and loss of control, financial and social consequences were frequently mentioned as reasons for seeking assistance (Karhulahti et al., 2023). These findings highlight the multifaceted impact of problematic gaming and underscore the importance of developing interventions that cater to a wide range of individual needs and life circumstances.
The Present Study
The aim of this study was to investigate the feasibility and preliminary outcomes associated with a new behavioural coaching component of the digital Restart program aimed at changing gaming behaviour and improving well-being among problematic gamers. The key components of this intervention include the identification and provision of feedback on the relevant risk-related thought/thinking patterns and behaviours, the establishment of goals, the transformation of habits, and the integration of psychoeducational elements. These psychoeducational elements encompass, for example, the identification of automatic detrimental thought patterns and cognitive defusion techniques aimed at managing stress and cravings, as well as enhancing protective behavioural strategies. In other words, this study aimed to explore information on the observed changes in relation to online training and individual coaching in terms of gaming control, gaming behaviour, and the well-being of players. The knowledge gained from this research can be used to develop interventions and treatment methods for gamers who realise they have a problem with video games. The research was guided by the following two questions:
What changes in problematic gaming and gaming behaviour are observed among Restart program participants from baseline to post-intervention and at 3-month follow-up? What changes in participants’ well-being are observed from baseline to post-intervention and at 3-month follow-up after completing the Restart program?
In this study, gaming disorder, along with the typical features, is described as problematic gaming. The concept of problematic gaming also considers that no precise diagnostic prerequisites have been set for participating in the Restart program; instead, participants self-assess the severity of their problem and the impairments they experience. Consequently, the nature of this intervention could be considered a selective (secondary) prevention as it targets a high-risk subgroup of problematic gaming. In this respect, problematic gaming may be less complex than gaming disorder or addictive behaviour, and the focus of the phenomenon studied in the presented research is the harmful consequences experienced by gamers who are concerned about their gaming behaviour. In this study, digital gaming is considered as playing games online or offline using a computer, gaming console or mobile device.
Methods
Intervention
The Restart program is a digital intervention for problematic gaming that combines an online CBT workbook and MI phone sessions. It was developed by the Finnish Blue Ribbon and launched in April 2020 as part of Peluuri, a Finnish online service for individuals with gambling and gaming problems. The program is intended for adults 18 years of age or older, and is available free of charge. To apply for the program, individuals fill out an online survey that can be completed anonymously and without a referral from a healthcare professional. The primary aim of the program is to support participants in achieving self-set goals for changing their problematic behaviour. As such, the program's objective is not to have participants quit gaming altogether unless they set this goal themselves. The 8-week program progresses according to pre-planned weekly themes; namely, 1) gaming history and the significance of gaming, 2) my gaming now, 3) how others see my gaming and alternative directions to take, 4) setting a goal, 5) all thoughts cannot be trusted, 6) making choices: when and how?, 7) time and priorities, and 8) the journey so far. The program consists of an online workbook, which was designed to support participants in self-reflection, and weekly MI phone sessions with a coach (Peluuri, 2022). Details of the intervention components and constructs are provided in Table 1.
Intervention Components and Constructs.
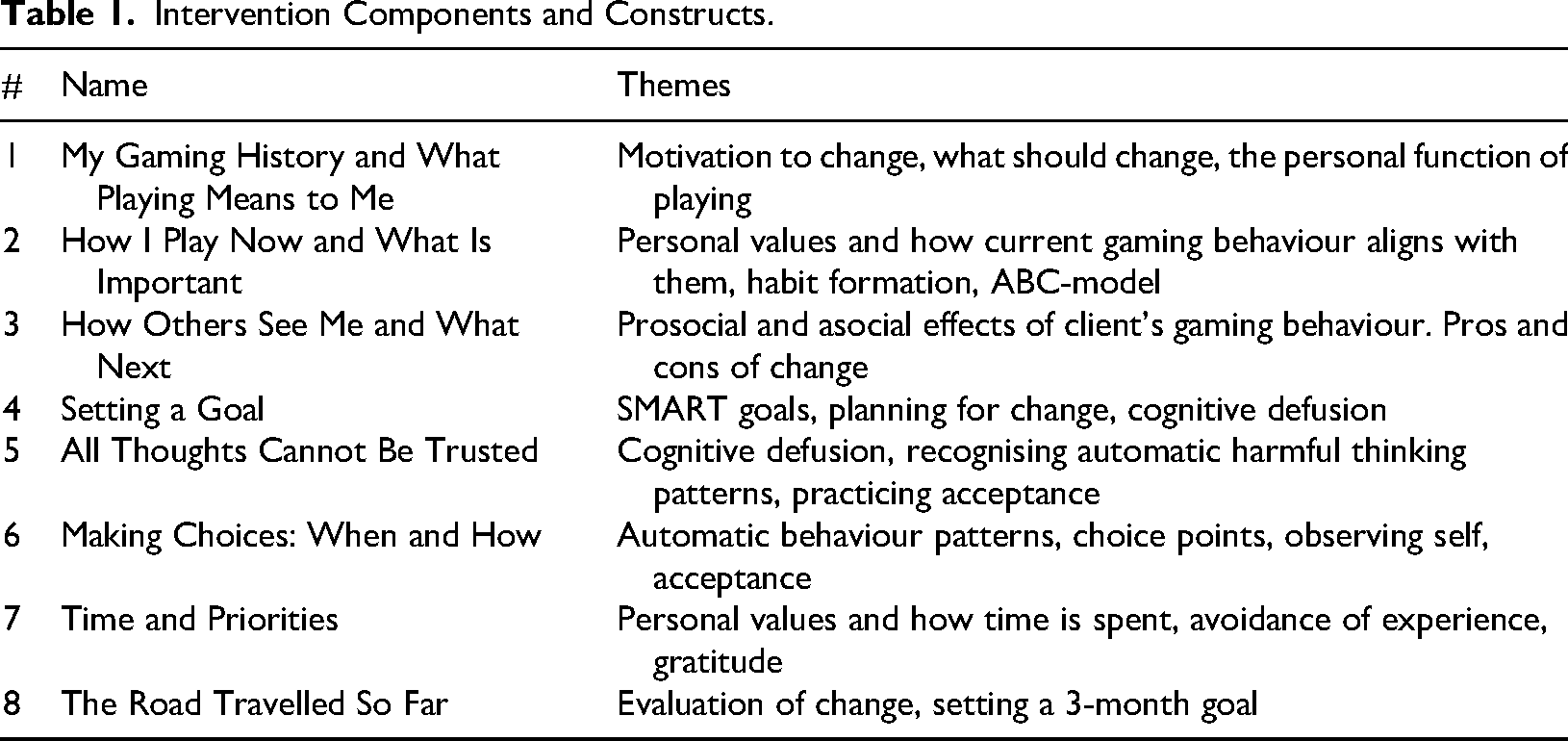
The online training assignments within the Restart program are informed by principles of CBT and acceptance and commitment therapy (ACT) (Peluuri, 2022). Both CBT and ACT analyse the interplay between human thinking patterns, behaviour, and emotions (Beck & Beck, 2021; DiGiuseppe et al., 2017; Karila & Koivisto, 2021). The primary goal of CBT is to assist individuals in identifying and modifying maladaptive cognitive processes and behaviours that contribute to emotional distress and impaired functioning (Podina & David, 2017). Although ACT belongs to the broader family of cognitive behavioural approaches, it focuses on increasing psychological flexibility by changing one's relationship to thoughts and feelings (not altering their content), fostering acceptance of experiences, and committing to value-based actions (Beck & Beck, 2021).
Each participant in the Restart program is assigned a coach with whom they have weekly phone sessions. The content of the conversation is determined based on the weekly theme, as outlined above, and the participant's current life situation around gaming. The coaches utilise MI during phone sessions because this approach aims to identify and strengthen an individual's motivation for lifestyle changes (Järvinen, 2020). The key methods associated with MI are: 1) encouraging a client to discuss change by asking open-ended questions and 2) affirming client strengths and listening reflectively in a collaborative, compassionate, accepting and empowering way (Miller & Rollnick, 2023).
Study Participants and Procedure
The research utilised a quasi-experimental design that did not incorporate a control group. This approach was adopted to conduct a preliminary evaluation of whether the planned novel intervention, along with the methods used, was associated with observable changes in the post-test and the 3-month follow-up test. The 3-month follow-up was selected to balance feasibility and participant retention, while still allowing for the observation of short-term sustainability of changes. Although the current evidence has highlighted the lack of long-term follow-up data in the field, this study aimed to contribute preliminary longitudinal insights within a manageable timeframe for a feasibility study.
The study population consisted of adult Finnish gamers who perceived their gaming as problematic or harmful. Participants were recruited through an online application on the Restart website, where PC, console and mobile gamers voluntarily signed up for the programme seeking to alter their gaming habits. The research focused on gamers who took part in the Restart programme. The inclusion criteria matched the programme requirements: a minimum age of 18 years and a subjective perception of problematic gaming. The exclusion criterion applied to gamers who believed that gambling partly contributed to their issues with digital gaming. Those participants who were found eligible were assessed at the baseline, post-program and 3-month follow-up time points using a semi-structured online questionnaire. The authors developed the questionnaire for the present study.
The study used retrospective data collected through an existing intervention programme (Restart), and the researchers did not initiate new data collection or direct interaction with participants. According to the Finnish National Board on Research Integrity (Finnish National Board on Research Integrity TENK, 2019) guidelines, ethical review is not necessary for retrospective studies as long as the research follows good scientific practice, including proper anonymisation and data protection. The study was not preregistered. The research plan was reviewed by the Finnish Blue Ribbon's research permit committee, which assesses the study plans of external researchers when granting access to data. Study participants gave informed consent and the dataset was anonymised before being shared with the researchers.
Measures
The survey included measures of well-being (e.g. Clinical Outcomes in Routine Evaluation Outcome Measure), gaming behaviour, and problematic gaming (Ten-Item Internet Gaming Disorder, Problematic Online Gaming Questionnaire), as well as indicators of compulsive internet use (Compulsive Internet Use Scale).
Sociodemographic information (age, gender, relationship status, educational level and employment situation) was collected at the baseline time point. At this stage, the participants were also asked which game type was the most problematic (puzzle and card games, adventure, shooting, strategy, sports, action, driving, simulation, role-playing, or music and social games) and which gaming platform(s) they had used the most in the last 12 months (mobile device, gaming console, computer, internet browser and hand console). For both questions, participants were able to choose more than one option.
Measures for research question 1: problematic gaming and gaming behaviour
The questionnaire also included the IGDT-10 (Ten-Item Internet Gaming Disorder; Király et al., 2017) scale, which measures problematic digital gaming. Respondents were asked to answer 10 questions that measured the severity of problematic gaming that had occurred in the previous 12-month period. The scale's items were rated using the three-point Likert-scale. The answer options were “never”, “sometimes” and “often”. The answers were then converted into a two-point scale (“yes” and “no”), so that the total score for the scale would range from 0 to 9; more specifically, the answer “often” had a score of one point, while the answers “never” and “sometimes” received a score of zero points. During scoring, questions 9 and 10 were combined in such a way that respondents would only receive a score of one if they provided an answer of “often” to both questions. In this scale, higher scores indicated more severe problems, and the cut-off point for problematic gaming was at least five out of nine points (Király et al., 2017). The scale has previously demonstrated adequate psychometric properties in a sample of Finnish people (Männikkö et al., 2019). In this study, the scale showed acceptable internal consistency (Cronbach's α = 0.79) based on the baseline data.
Problematic gaming tendencies were evaluated using the POGQ (Problematic Online Gaming Questionnaire; Demetrovics et al., 2012), an instrument that includes six dimensions: preoccupation with games, withdrawal symptoms, immersion, social isolation, overuse in terms of the amount of gaming and interpersonal conflict. The POGQ consisted of 18 items, to which participants responded using a five-point Likert scale. The answer options were: 1= Never; 2= Rarely; 3= Sometimes; 4= Often; and 5= Almost always. As such, the total score for the instrument ranged from 18 to 90 points, with higher scores indicating more severe problems; the cut-off score for problematic gaming was 66 points (Demetrovics et al., 2012). The scale has previously demonstrated satisfactory psychometric properties in a Finnish sample (Männikkö et al., 2020). According to the baseline measurements, the instrument showed excellent internal consistency (Cronbach's α = 0.91).
The CIUS-5 (Compulsive Internet Use Scale) is a shortened, five-question version of the CIUS (Meerkerk et al., 2009) used to assess problematic Internet use. Participants provided answers to questions using a five-point Likert scale. The options were: 1 = Never (0 points); 2 = Rarely (1 point); 3 = Sometimes (2 points); 4 = Often (3 points); and 5 = Almost always (4 points). The total score could range from 0 to 5 points, with higher scores associated with more severe problems (Lopez-Fernandez et al., 2019a). The scale has previously been validated in the Finnish language (Lopez-Fernandez et al., 2019a). In this study, the instrument demonstrated acceptable internal consistency when analysed according to baseline data (Cronbach's α = 0.86).
To measure gaming behaviour, participants were asked about the number of days per week they played games, the frequency of individual gaming sessions per day, the duration of a single gaming session, their perceptions of problems with time spent gaming and the proportion of time spent gaming that was problematic. During the baseline and post-program measurements, participants were asked to rate their gaming behaviour over the past 2 months, while participants were asked to assess their gaming over the last 3 months during the follow-up measurement. The answer options for the number of gaming days per week (weekly gaming days) were: 0 = I haven’t played at all; 1 = Less than once a week; 2 = 1–2 days in a week; 3 = 3–4 days in a week; 4 = 5–6 days in a week; and 5 = Daily. The answer options for individual gaming sessions per day (single gaming sessions) were: 0 = I haven’t played at all; 1 = once; 2 = 2–3 sessions; 3 = 4–6 sessions; 4 = 7–9 sessions; and 5 = 10 or more. The answer options for the duration of a single gaming session were: 0 = I haven’t played at all; 1 = Less than 15 min; 2 = 15–30 min; 3 = 30–60 min; 4 = 1–2 h; 5 = 2–4 h; and 6 = More than 4 h. The answer options for problems with the time spent gaming were: 0 = No problems at all; 1 = Yes, sometimes; and 3 = Yes, all the time. Regarding the proportion of problematic gaming time, participants were asked to provide a percentage between 0% and 100%.
Measures for research question 2: well-being
To measure well-being, participants were asked to assess their own mental and physical health through two questions such as: “How do you perceive your current mental health?” and “How do you perceive your current physical health?”. Participants responded to these questions using a five-point Likert scale (1 = Very bad, 2 = Bad, 3 = Neither good nor bad, 4 = Good and 5 = Very good). In the scoring, the answers were assigned values between 1 and 5. Lower values represented lower self-assessed well-being across all questions.
The CORE-OM (Clinical Outcomes in Routine Evaluation Outcome Measure) instrument was used to assess subjective well-being and clinical outcomes (Barkham et al., 2001). The measure includes 34 self-reported items, which participants scored using a five-point Likert scale, with the following options: 0 = Not at all; 1 = Occasionally; 2 = Sometimes; 3 = Often; and 4 = Most or all the time. As such, the total score could range from 0 to 136. A higher total score reflected a situation in which the individual experiences more frequent problems (i.e., distress symptoms), but the results cannot be used to classify participants as either healthy or sick. The measure could be administered at multiple predefined time points, including before and after an intervention, to assess the effectiveness of treatment. Changes in a participant's scores over time, particularly a reduction in the total score, could indicate improvement in the condition (Barkham et al., 2001). The full 34-item version of CORE-OM has demonstrated adequate psychometric properties in both a clinical and non-clinical Finnish sample (Honkalampi et al., 2017). According to the baseline scores, the instrument exhibited excellent internal consistency (Cronbach's α= 0.93).
In this study, the IGDT-10 and POGQ scales were considered the primary measures for research question 1, assessing changes in problematic gaming. The CORE-OM and self-rated mental and physical health questions were considered the primary outcome measures for research question 2, evaluating changes in subjective well-being. Additional behavioural metrics and the CIUS-5 scale served as secondary indicators.
Data Analysis
The collected data were analysed using a linear mixed model (LMM) available through SPSS, version 28 (IBM Corp., Armonk, NY, USA). For the data collected via the POGQ-, CORE-OM, CIUS-5 and IGDT-10 instruments, sum variables were first formed according to the scoring instructions of each instrument. Measurements were taken at three time points: baseline (pre-intervention), post-intervention and a 3-month follow-up. These time points were conceptualised as Level 1 variables, nested within participants at Level 2, to handle the repeated measures design over time adequately. Participant ID was used as a random intercept effect; that is, variance was allowed in the intercepts between participants. Due to maximum likelihood estimation, LMM can deal with missing data in the dependent variable. The models were adjusted for sociodemographic variables, including age, gender, relationship status, educational level and employment situation. Paired contrasts with 95% confidence intervals (Cl) were calculated for the baseline vs. post-program and post-program vs. 3-month follow-up measurements. Changes were considered statistically significant when p < 0.05 (Krueger & Tian, 2004). All of the LMM models satisfied the assumptions of linearity. Q–Q plots indicated that the model residuals and random effects were normally distributed and homoscedastic.
The participants’ background data were analysed using descriptive statistical methods, with the characteristics of each variable described in terms of frequency and percentage. The age variable was transformed using the reported year of birth, which could then be transformed into a distribution, average value, and standard deviation of age. Differences between the baseline scores of groups who had completed or discontinued the program were assessed using a t-test.
Results
In total, 138 potential volunteers responded to the questionnaire at the pre-program time point. Ultimately, 110 individuals who enrolled in the intervention program completed the informed consent. In total, 63 participants (with an attrition rate of 42.73%) completed the program, including all its activities, and answered the questionnaire at the post-program time point. In total, 50 participants (attrition rate 54.55%) completed all pre-, post- and follow-up tests. The recruitment and study process for the participants is illustrated in Figure 1. The participants who discontinued the program had slightly higher baseline scores, relative to participants who completed the program, for the IGDT (4.41 vs. 3.72; p = 0.187), CIUS-5 (11.01 vs. 10.32, p = 0.42) and CORE-OM (52.81 vs. 49.13; p = 0.281) instruments, along with the number of single gaming sessions (3.62 vs. 3.10, p = 0.70) and duration of single gaming session (4.83 vs. 4.73; p = 0.636). As could be expected, the participants who dropped out of the program reported slightly lower subjective mental health scores at the baseline time point (2.89 vs. 3.08, p = 0.223) than participants who completed the program. However, no statistically significant differences were discerned in any of the scores between participants who completed the program and those who discontinued it.
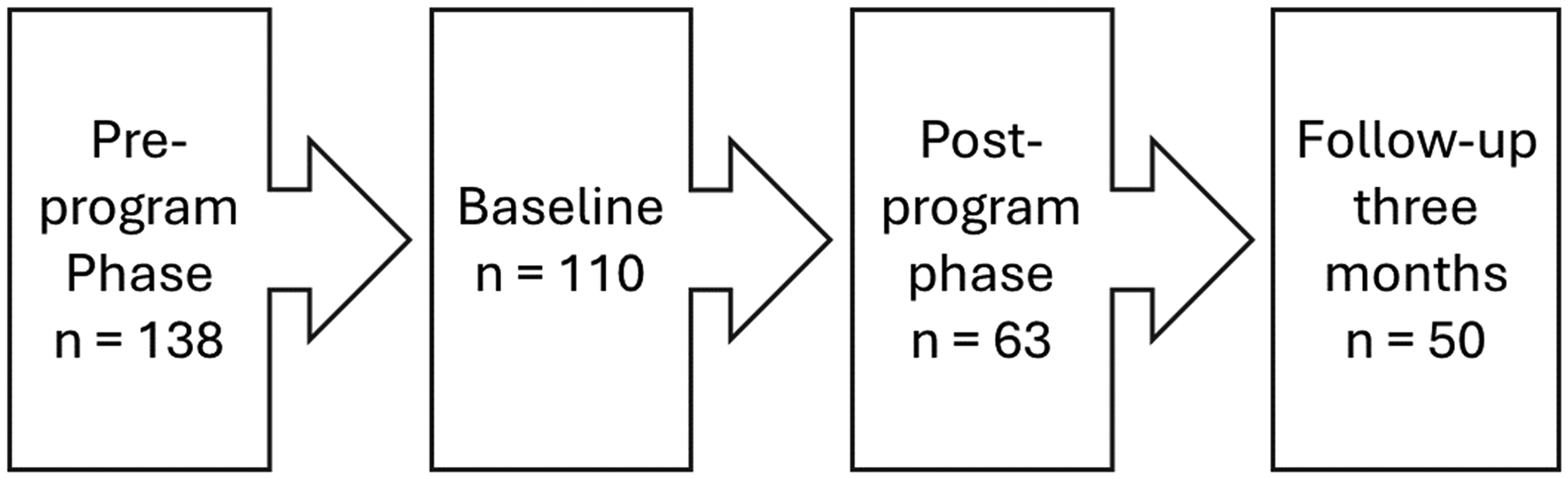
Participants’ Recruitment and Study Process.
Baseline Characteristics
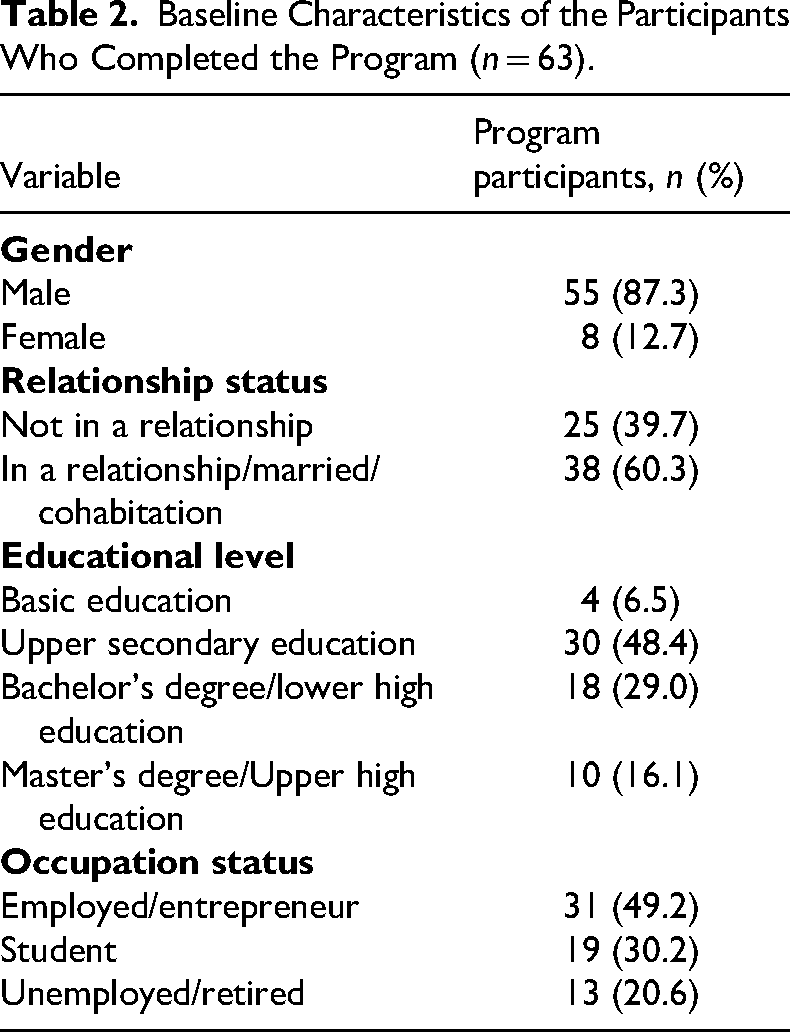
The baseline characteristics of the participants who completed the program (n = 63) are presented in Table 2. In total, 29 (20.9%) of the pre-program survey participants did not start the actual program. No significant differences in baseline characteristics were observed between the participants who completed only the preprogram survey and those who started the program. Regarding the baseline characteristics of the participants who completed the program, most were male (87.3%). The age of participants ranged from 19 to 50 years, with an mean (SD) age of 30.7 ± 6.3 years at the time of analysis. The most common level of education among the participants was upper secondary education (48.4%). Most of the participants were either employed or working as entrepreneurs (49.2%). The most commonly used platforms for gaming were the computer and a mobile device. More specifically, 73.0% of the participants reported using their computer daily for gaming during the past 12 months, while 17.5% reported using their computer for gaming every week. Moreover, 39.7% of the participants used a mobile device for gaming daily, with 14.3% of participants reporting that they used a mobile device for gaming on a weekly basis. The hand console was found to be the least commonly used device because 82.5% of participants reported not using a hand console for gaming. According to the data, the most problematic gaming types were strategy games (50.8%), role games (41.3%), action games (30.2%), shooting games (36.5%) and adventure games (14.3%).
Baseline Characteristics of the Participants Who Completed the Program (n = 63).
Results of the Restart program
The baseline, post-program and 3-month follow-up results, along with the differences between the time points, are presented in Table 3. The mean values, CI and deviations for the IGDT-10, CIUS-5, POCQ and CORE-OM instruments across the time points (outside the LMM model) are illustrated in Figure 2. The mean IGDT-10 and POGQ scores, which measured problematic gaming, fell under the cut-off point at the baseline measurement time point. At the baseline measurement time point, participants played games on an average of 5–6 days per week, with each gaming day consisting of an average of 4–6 sessions. A single gaming session lasted, on average, for 1–2 h. Most participants responded that they repeatedly encountered problems with time spent gaming (mean score = 1.8). There are indications that the Restart program was associated with positive changes because statistically significant differences were observed between the baseline and post-program results. A negative trend was observed for all measures throughout the study period, with the exception of mental and physical health, which exhibited a positive trend (higher scores indicating better subjective well-being). After the program, participants reported gaming between 3 and 4 days per week, with 1–3 sessions (mean 1.7), each lasting 1–2 h per day.
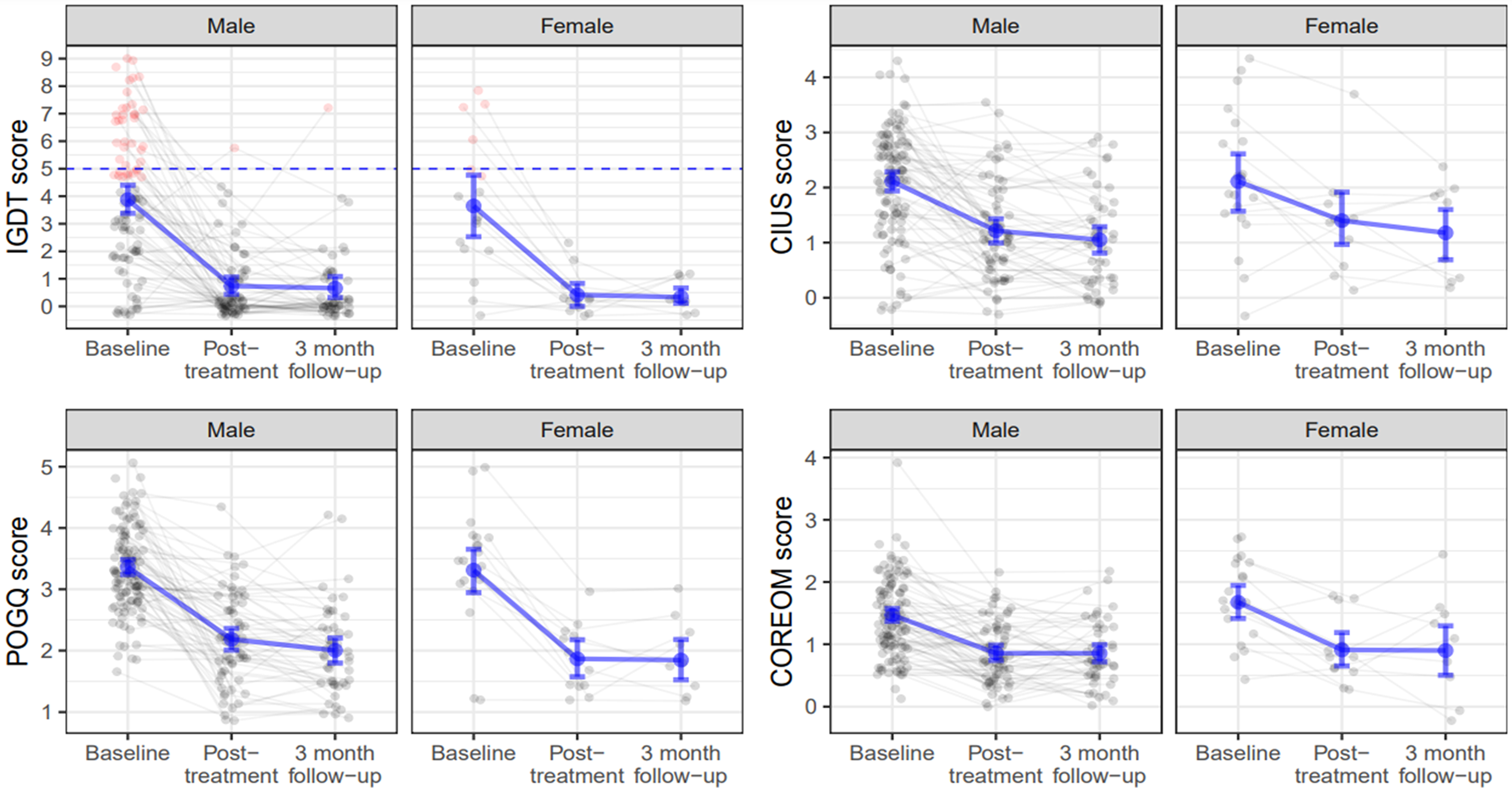
Participant-wise observations across the measurement phases (baseline, end [i.e., post-treatment], and 3-month follow-up), presented separately for both genders and four dependent variables (IGDT-, CIUS-, POGQ-, and CORE-OM scores). Light grey dots represent individual participants, and thin grey lines indicate individual “pathways” from baseline to the 3-month follow-up. For IGDT scores (top left), filled black dots mark observations ≥5, indicating potential clinical relevance. Random jitter has been added to improve visual clarity. Bold black dots represent mean values across measurement phases, and vertical bars indicate bootstrapped 95% confidence intervals. Individual data points are anonymised and jittered; no identifying information is presented. CIUS = Compulsive Internet Use Scale; CORE-OM = Clinical Outcomes in Routine Evaluation Outcome Measure; IGDT = Ten-Item Internet Gaming Disorder; POGQ = Problematic Online Gaming Questionnaire.
Results of the Restart Program.
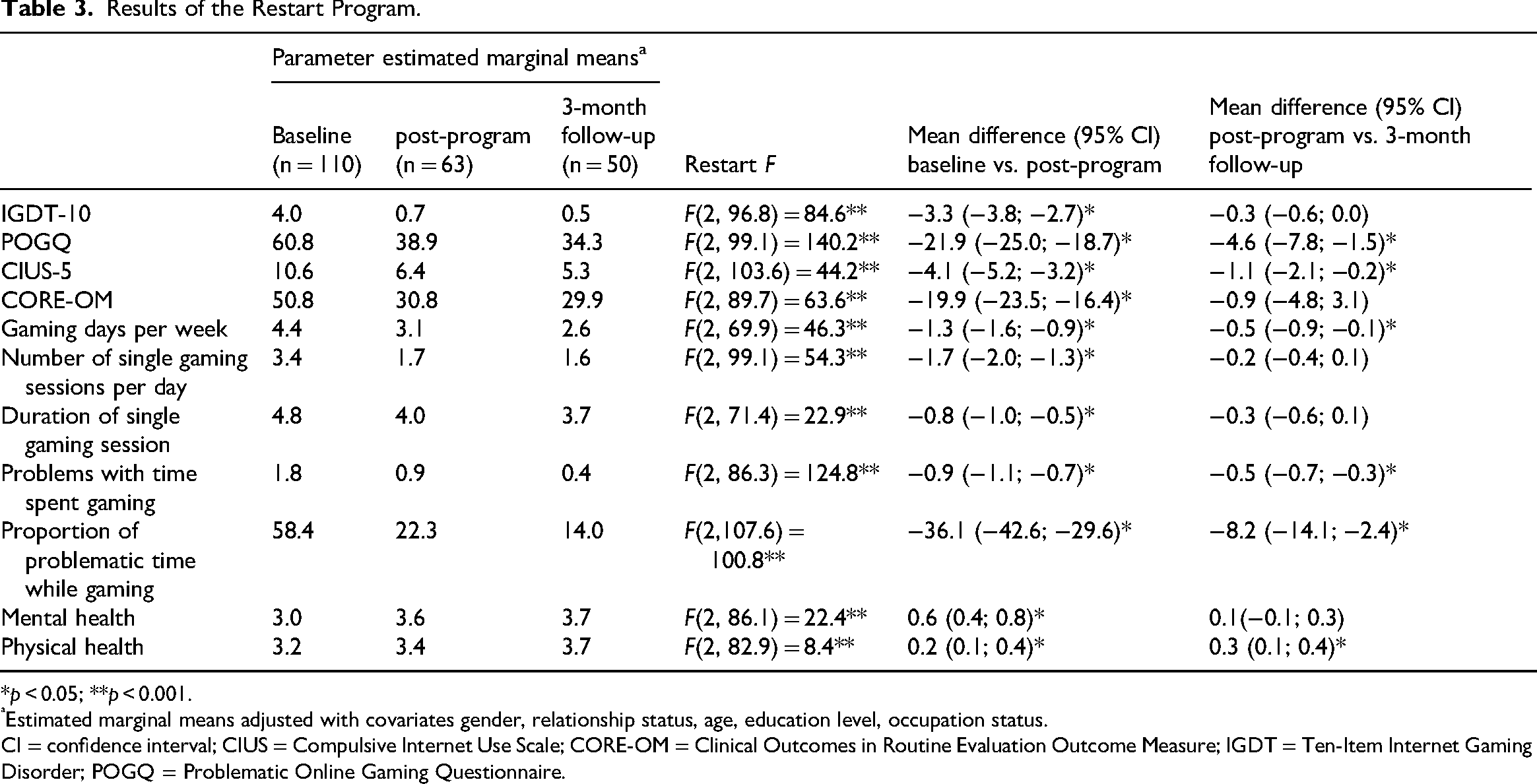
*p < 0.05; **p < 0.001.
Estimated marginal means adjusted with covariates gender, relationship status, age, education level, occupation status.
CI = confidence interval; CIUS = Compulsive Internet Use Scale; CORE-OM = Clinical Outcomes in Routine Evaluation Outcome Measure; IGDT = Ten-Item Internet Gaming Disorder; POGQ = Problematic Online Gaming Questionnaire.
When comparing the post-program and 3-month follow-up time points, statistically significant differences were observed for POGQ score (38.9 vs. 34.3; p = 0.005), CIUS-5 score (6.4 vs. 5.3; p = 0.018), gaming days per week (3.1 vs. 2.6, p = 0.02), problems with time spent gaming (0.9 vs. 0.4; p < 0.001), proportion of problematic gaming time (22.3% vs. 14.0%; p = 0.006) and physical health (3.4 vs. 3.7; p = 0.005). At the 3-month follow-up time point, participants spent an average of 1–2 days per week on gaming, with 1–3 (mean 1.6) gaming sessions per day. At this time point, the respondents reported that a single gaming session lasted from approximately 30–60 min to 2 h. The trends noted between the post-program and 3-month follow-up time points reflected what was observed between the baseline and post-program time points, albeit with relatively smaller differences. In general, the number of gaming days per week and the frequency of single gaming sessions per day decreased across all three measurement time points. Additionally, the duration of a single gaming session showed a negative trend (F(2, 71.4) = 22.9, p < 0.001). However, the difference between the post-program and 3-month follow-up measurement points was not statistically significant.
The baseline characteristics (Table 3) (i.e., age, gender, relationship status, education level and occupation status) served as covariates for parameter estimations. The conducted analyses revealed that relationship status significantly influenced the number of gaming sessions per day (−0.4; p = 0.008), whereas education level significantly influenced the parameter CIUS-5 (1.1; p = 0.009). Moreover, a participant's age was found to significantly affect the duration of single gaming session (−0.03; p = 0.025), while occupation status exerted significant effects on the parameters CORE-OM (4.5; p = 0.031), proportion of problematic gaming time (6.4; p = 0.003), number of single gaming sessions per day (0.2; p = 0.025) and mental health (−0.2; p = 0.007).
Discussion
The aim of this study was to assess the preliminary outcomes of the Restart program on gaming behaviour and well-being among a group of Finnish problematic digital gamers. The study focused on clarifying how the online training and individual coaching provided via the Restart program were associated with changes in gaming control, gaming behaviour, and the well-being of gamers. The effects of the intervention were assessed by comparing results collected at three different time points: before the program (baseline), immediately after the program (post-program) and 3 months after the program (follow-up). The results revealed that participation in the Restart program was associated with changes in participants’ gaming behaviour and well-being. Statistically significant differences were observed in all measures examined in this study between the baseline and post-program measurements. Although statistically significant differences were only observed for a few of the included measures between the post-program and 3-month follow-up time points, it is important to note that no deterioration was observed for any of the measures relevant to problematic gaming. In other words, a measure either followed the trend observed between the baseline and post-program measurements or remained stable in the period between the end of the program and the follow-up measurement.
In terms of time spent gaming and perceived gaming problems, participating in the Restart program may be associated with improved control over their gaming. A statistically significant decrease in the time spent gaming, as measured by number of days per week spent gaming, was observed over the entire study period. A statistically significant reduction in the number of single gaming sessions per day and the duration of a single gaming session was also observed between the baseline and post-program measurements. Although no significant decrease in the number of single gaming sessions per day or the duration of a single gaming session was noted between the post-program and three-month follow-up time points, the trend in both metrics continued to decrease or had reached a plateau. Therefore, an individual who participates in the Restart program can expect an improvement in the time they spend gaming within three months of completing the intervention. Furthermore, the metrics of perceived problems with time spent gaming and proportion of problematic gaming time demonstrated statistically significant decreases across the entire study period. In other words, although significant differences in all aspects of problematic gaming were not observed between the post-program and 3-month follow-up time points, participants reported lower levels of problematic gaming 3 months after the program had finished. These findings suggest that participation in the program may be associated with sustained changes in problematic gaming, although causal conclusions cannot be drawn without a control group.
Changes in the IGDT-10 and POGQ scores, both of which measure problematic gaming, also suggest that the intervention may be associated with potential benefits. However, it should be stated that the average baseline scores for these two measures did not exceed the cut-off points for problematic gaming. Even though the prerequisite for participating in the Restart program was set as a subjective experience of problematic gaming rather than a diagnosis of IGD, this result may nevertheless partly reflect the level of severity of gaming problems among those who apply to the program. This result was similar to what was reported by Starcevic et al. (2020) (i.e., 39% of those seeking treatment for problematic digital gaming did not meet the diagnostic criteria for IGD); instead, gamers sought treatment because of personal experiences and/or feedback from family members. It should be noted that this may not be a large factor because IGD can be diagnosed based on different criteria (e.g., identification of problematic gaming or overall time spent gamin)g (Pontes et al., 2022).
The results of the present study support prior views that online interventions are suitable for treating problematic digital gaming (Kim et al., 2022b; Lo et al., 2023). The present study's findings also support the view reported by Baumeister et al. (2014) in their review paper, which indicated that guided internet-based interventions were superior to unguided ones. Specifically, guided interventions showed greater reductions in symptom severity and higher completion rates of intervention modules. In the present study, the participants were assigned a coach with whom they had weekly phone sessions where the content of the conversations progressed based on the weekly theme. However, although initial studies on this type of therapy orientation or technique have shown promising results in addressing problematic gaming, more rigorous research is needed to fully support the development of evidence-based treatment methods (King et al., 2017; Mestre-Bach et al., 2022; Zajac et al., 2017). According to a meta-analysis conducted by Lo et al. (2023), the theoretical orientation used in an intervention or therapeutic approach had no significant effect on the effectiveness of the intervention; instead, the format of the intervention was found to be relevant for effectiveness. The results showed that interventions with a group-based format are currently the most effective (Lo et al., 2023). There are also differing views on the significance of the applied theoretical approach because Kim et al. (2022b) reported that interventions combining different therapy methods are more effective than those using a single therapeutic orientation. Nevertheless, the results of this study support the view that web-based interventions or treatments for problematic gaming may be promising approaches (Andersson & Titov, 2014; Boumparis et al., 2022; Gorowska et al., 2022).
In addition to gaming behaviour and problematic gaming, this study also examined self-reported well-being in relation to participation in the intervention. Participants reported their subjective well-being at three different time points using the CORE-OM instrument; additionally, participants provided self-assessments of their mental and physical health. The baseline and post-program measurements were characterised by statistically significant differences across all three of the domains mentioned above; more specifically, a decrease in CORE-OM scores and an increase in mental and physical health parameters. Concerning the CORE-OM instrument, a decrease in total score is indicative of better subjectively perceived well-being (Barkham et al., 2001). Conversely, the values of the mental and physical health variables are positively correlated with perceived state of health, ranging from 1 (Very Bad) to 5 (Very Good). At the 3-month follow-up time point, the mean score results for CORE-OM and mental health remained stable, while physical health continued to show a statistically significant increase. The results of this study showed similar trends in well-being compared to the reported benefits of CBT interventions for the treatment of problematic gaming (Stevens et al., 2019; Torres-Rodríguez et al., 2018).
It is important to discuss the limitations of the presented research when considering the generalisability of the results. First, the study design was quasi-experimental (i.e., the study lacked a control group against which the effectiveness of the intervention could be compared). In this regard, individuals who self-select to participate in interventions like this may, on average, be more motivated to deal with their gaming problems, and some portion of their recovery could be due to this. Moreover, this study design is more vulnerable to the influence of confounding variables (e.g., external factors) that may impact the outcomes. This complexity can hinder the accurate assessment of the intervention's efficacy. Regarding the reliability of the study, it is also necessary to consider the attrition rate, which negatively impacted the sample sizes at the post-program and 3-month follow-up measurement points. A relatively short follow-up time (3 months) also makes it difficult to draw firm conclusions about the stability of the changes in study outcomes. Thus, the conclusions presented here are preliminary, and caution should be taken when generalising the findings. It is advisable to incorporate more extensive trials in subsequent studies to yield more generalisable conclusions. It is also worth noting that the open nature of the pre-phase program provided an opportunity to self-evaluate one's risk behaviour without being included in the intervention program. As a result, many initial evaluation participants did not participate in the actual intervention, which highlights the selective nature of the digital program's secondary prevention approach. Moreover, the data used in this study were based on self-assessments, which have been reported to be prone to bias. However, the reliability of the study was strengthened by using valid instruments.
The data analysis revealed that certain background variables exerted a statistically significant effect on the parameter estimates formed from the outcome variables. For example, occupational status was found to significantly influence several outcome variables. Notably, changing the value of occupational status increased the CORE-OM mean score by 5.1 units and the proportion of problematic time by 6.1 units, as well as the number of single gaming sessions per day by 0.2 units. This change in occupational status also decreased the mean values of the mental and physical health variables by 0.3 units. According to Lopez-Fernandez et al. (2019b) and Tullett-Prado et al. (2021), lower levels of education and increased leisure time (e.g., unemployment or full-time student status) are associated with higher measured scores of problematic gaming, which may also explain the findings observed in this study.
To conclude, participation in the Restart program was associated with observed changes in participants’ problematic gaming, gaming behaviour, and subjective well-being. However, due to the quasi-experimental design, these findings should be interpreted as preliminary and non-causal. The results suggest that the studied intervention, which combines online training and individual coaching, may be associated with improvements in addressing problematic gaming. Further research is needed to confirm the suitability of web-based interventions for this purpose. It would be useful for future research to include a more extended study period to ascertain whether online interventions for problematic gaming can lead to long-lasting improvements in gaming behaviour.
Footnotes
Ethical Statement
The study adhered to the principles outlined in the 1964 Helsinki Declaration and its later amendments. It adhered to the principles outlined in the Declaration of Helsinki and is consistent with the ethical standards for research within the Finnish Blue Ribbon, who manages this care service data. The study participants provided online consent and completed a voluntary online survey without providing identification data.
Funding
The authors received no financial support for the research, authorship and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Data Availability
The data are available from the Finnish Blue Ribbon upon reasonable request.