
Abstract
Aim
This long-term follow-up study assessed substance related mortality by sex and compared it with the age-matched general population, with the aim of informing the development of treatment services.
Methods
Data included 10,891 former patients who had sought treatment for substance use between 1990 and 2009, and a special group of 1,076 children who had accompanied their parent(s) to family treatment. Treatment data were linked to national register data concerning education, hospitalizations and death by 2019. Age-specific death rates, standardized mortality ratios and causes of death were compared with the Finnish general population.
Results
By 2019, a larger proportion of the 7,334 treatment-seeking men (42.6%) than of the 3,557 women (27.4%) had died. The underlying cause of death was alcohol and/or drug related in one-third of the deaths and two-thirds when further causes were included. Age-specific comparisons with the general population revealed that the studied men and women had markedly higher death rates and the difference increased decade by decade, being highest among the youngest age-groups (standardized mortality ratios were 9.8 for men and 13.8 for women born in the 1980s). Out of the 1,076 children, 15 boys (2.8%) and four girls (0.7%) had died, mostly due to substance use or violence related causes.
Conclusions
Mortality was significantly increased for several years after treatment highlighting the need for long-term follow-up, as well as after-care and easy re-entry to treatment. Special attention should be paid to the relatively higher increase in mortality risk among women.
Introduction
Heavy alcohol and other substance use (SU) are known to be associated with various adverse outcomes, such as a heightened risk for educational drop-out (Townsend et al., 2007), familial problems (Mardani et al., 2023) and premature death (Pitkänen et al., 2020). SU disorders (SUD) are considered chronic relapsing-remitting disorders and thus treatment should also be sufficiently long lasting (Ravndal et al., 2005). Long-term follow-up research on the life-course of people who have recognized the need for substance use treatment and sought help for themselves and/or their families is needed as feedback for service providers and for developing the service system. National register data enable comparison with age-matched population data and long-term follow-up. Research is needed to deepen our understanding of the special needs of these vulnerable groups.
SUDs are one of the mental disorders with highest mortality rates not only for specific-death causes (due to self-harm and overdoses among others), but also because of their contribution to all-cause mortality due to the connections that SUDs have with other physical diseases (Chesney et al., 2014). When studying substance related mortality, it is important to consider both underlying and further causes of death. The World Health Organization (2025) has defined the underlying cause of death as “the disease or injury which initiated the train of morbid events leading directly to death, or the circumstances of the accident or violence which produced the fatal injury”. Additionally, there can be substance related further causes of death that are contributing (adversely affect the development of the condition leading to death), immediate (the disease, failure or injury whose symptoms cause the person to die) or intermediate (the condition that leads from the underlying cause of death to the immediate cause of death) (Official Statistics of Finland, 2018).
Treatment record data in combination with data from other registers enable long-term pseudonymized follow-up. High quality ethical procedures have been developed in Finland to enable research use of data sets that are exceptional due to the unique personal number assigned to each person at birth. Especially the death certification practices and cause of death validation have produced high quality data also on both underlying and further causes of death for several decades (Lahti & Penttilä, 2001; Ylijoki-Sørensen et al., 2014).
Generally, women live longer than men in Finland; for example, the average life expectancy is 74.2 years for women and 65.9 years for men born in 1971 (Official Statistics Finland, 2025). Differences in causes of death have been found between sexes, such as suicide rates being generally higher among men than among women (Statistics Finland, 2018). Based on previous knowledge, there are sex differences with regards to SU and the harms related to SUDs (McHugh et al., 2018; Pitkänen, 2006), as well as in mortality and causes of death (Kendler et al., 2017; Laine et al., 2022). In research, sex is often treated as a confounding factor; however, when studying substance related mortality, separate analyses for men and women can reveal differences across the life course.
Children born into disadvantaged circumstances and who experience cumulative childhood adversities are at risk for long-term harms, such as poor educational attainment (Machin, 2006) and increased mortality (Fang et al., 2018; Kauhanen et al., 2006; Landberg et al., 2018; Rod et al., 2020). SU related problems are often intergenerational, and the multidimensional cycle of genetic, environmental and socio-economic burden is difficult to break, with the adverse familial effects starting already prior to conception and birth and continuing throughout pregnancy into childhood and adolescence. Parental SUD increases the risk of children subsequently developing a SUD (Jääskeläinen et al., 2016; Merikangas, 2002; Merikangas & McClair, 2012) and strong support for this phenomenon has been found across multiple substances (Knight et al., 2014). It is plausible that the children of parents with SUDs could also have an increased risk of premature death because they themselves are more likely to develop an SUD and have often encountered various adversities in childhood (Enoch, 2011). The effect of parental SU on children has been mostly investigated with regards to perinatal SU and adversities in early childhood. However, a large population-based study in Denmark found an increased long-term risk of all-cause and alcohol related mortality among individuals born to parents with alcohol use disorders (Holst et al., 2022). Another study found that experiencing childhood adversities seems to be an important mediator of the association between parental education and offspring mortality in early adulthood and postulated that interventions reducing the exposure to childhood adversities may reduce the socio-economic background gradient associated with early adult mortality (Elsenburg et al., 2022).
The current register-based long-term follow-up study focused on assessing the proportion, timing and causes of death of former patients who had sought SU treatment and children who had accompanied their parent(s) to the family unit, with special attention paid to substance related deaths. There were four research questions.
How many and what kind of deaths occurred after SU treatment? Did mortality of individuals who had sought treatment for SU differ by sex and in comparison with the same aged general population? What was the timing of the deaths after SU treatment? How did the mortality of the children who had accompanied their parents to inpatient care differ compared to the general population and to same aged patients who had sought treatment for SU?
Methods
Data included 10,891 in- and outpatients who had sought treatment for SU (there after patients/men/women with SU) and the special group of 1,076 children who had accompanied their parent(s) to an inpatient family treatment unit (there after children/boy/girl) (Figure 1). Data were retrieved from our larger Register-based Follow-up Study on Criminality, Health and Taxation of Inpatients and Outpatients entered into Treatment for Substance Use in Finland (Pitkänen et al., 2020). Data include treatment records of three units of the A-Clinic Foundation between 1990 and 2009 that have been linked to national register data. Data have been pseudonymized.
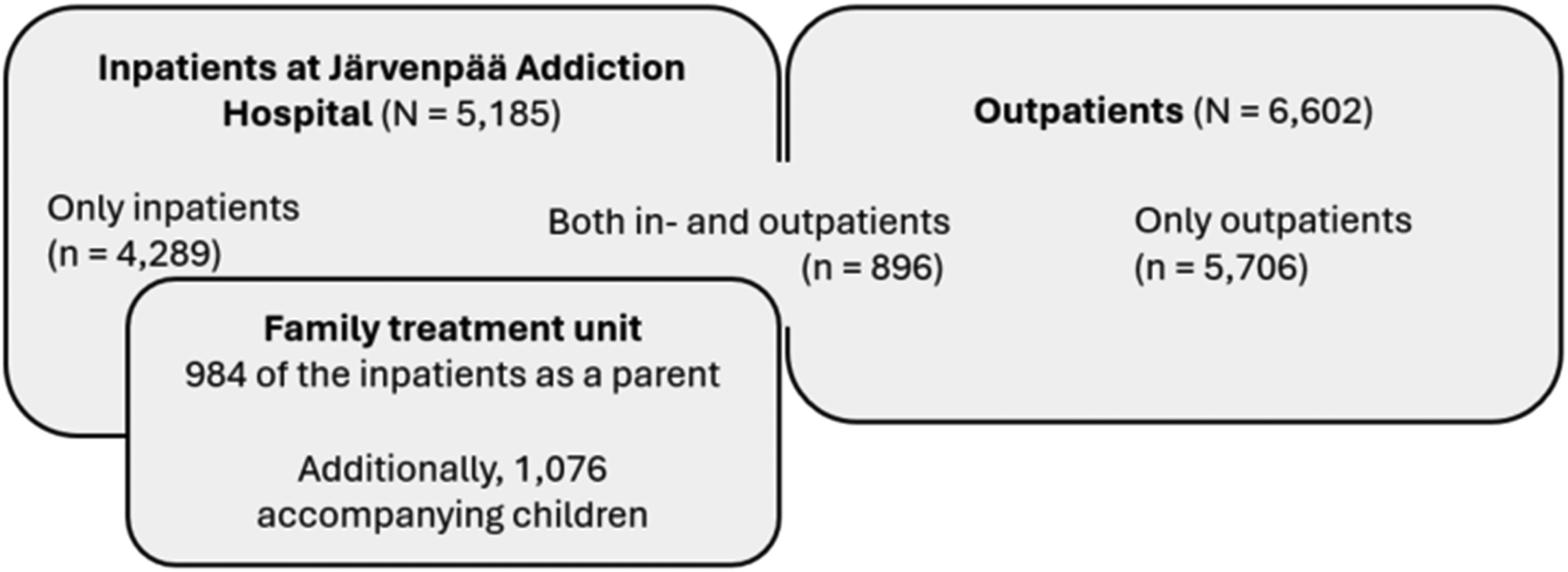
The Proportion of Inpatients and Outpatients and the Relation of the Family Unit to the Data Set.
Treatment Units in 1990–2009
The A-Clinic Foundation is a nationwide non-profit non-governmental organization that provided specialized services for SU at the time of data collection. Järvenpää Addiction Hospital (JAH) has been the only hospital to specialize in the treatment of addictions in Finland since 1951. During the study period (1990–2009), JAH offered a variety of inpatient programs, including detoxification from alcohol and other substances, an opioid substitution treatment program, family treatment, and rehabilitation programs for men and women separately. Treatment was provided by multidisciplinary teams using cognitive behavioral theory-based approaches. Treatment was voluntary.
The data included 5,185 inpatients and a special group of 1,076 children who had attended family treatment in JAH. The data consisted of all adults and children in the electronic patient information system between March 1997 and September 2009. Additionally, inpatient data included 214 mothers and 125 fathers who had been at the family treatment unit with a child and those outpatients (81 women and 214 men) who had also been at JAH before the electronic documenting system was implemented (1990–1996). The data were complemented manually to include all accompanying children born between 1990 and 1997. Some personal identification numbers were missing or incorrect and it was not possible to estimate the exact number of missing data while the same person could have been included in the data via other treatment periods. According to the available data, every other patient (48%) had been admitted to the hospital more than once during the study period.
The data included also all outpatients (6,602) of two SU treatment units in Helsinki between 1990 and 2009. One of them provided special welfare services for individuals with alcohol and/or drug use and the other was started to complement it for providing opioid substitution treatment when it became accepted in Finland. Outpatient treatment consisted mostly of individual or group therapy and counselling with the overall aim of helping clients to stop or reduce SU and the associated harms and to enhance their quality of life. Some outpatients (8.3%) had also been inpatients at JAH. Three sons and two daughters emerged in the data later as adult patients, all alive throughout the follow-up.
Background Data
Background information to describe the characteristics and to study the sex differences was selected from the large data set that includes linked data from various registers for several research settings. Treatment data provided the sex, year of birth, the municipality of residence (grouped as Helsinki or other) and the treatment dates. For descriptive purposes a dummy variable was created to separate those in- and outpatients with a treatment length of 7 days or less (n = 1779) from those who had long or several contacts (mean ± SD time between the first and last contact: 962.2 ± 1,372.8 days; n = 9,112). The seven-day cut-off separated people with sustained treatment contact from those with a short or single visit to treatment.
Information on SUDs was extracted from treatment data and national hospital records between 1990 and 2009. The Hospital Discharge Register until 1993 and the Finland Care Register for Health Care since 1994 included the primary and two secondary diagnoses of each hospitalization recorded using International Classifications of Diseases (ICD) Ninth Revision and, after 1996, also ICD-10 codes (The World Health Organization, 1975, 2016). About half of the outpatients (n = 3,136) had received treatment but the SU had not been diagnosed by a medical doctor. A dummy variable was created for separating patients with only alcohol use disorder (AUD only) from those with other or several SUDs because drug use increased markedly during the studied period.
Data from the national Register of Completed Education and Degrees were provided by Statistics Finland up to 1 January 2019. A categorization into two groups according to completion of secondary education (approximately 12 years) was made.
Mortality
Data concerning date and causes of death were provided by Statistics Finland up to 1 January 2019. Follow-up time varied from 9.1 to 29.8 years after the first contact during the studied period; 10-year follow-up data were available for 96.5% and 15-year follow-up data for 46.6% of the adults with SU. The follow-up time for children was dependent on the year of birth.
A national time series classification into 54 groups of underlying causes of death enabled follow-up and comparison to the general population. The classification was started in 1969 and, thus, it does not comply with the grouping of the current ICD; however, a linking key is provided for the ICD codes (Statistics Finland, 2021). In addition to the underlying cause of death, also data on further causes including immediate, intermediate and contributing causes of death were obtained from the death certificates (Official Statistics of Finland, 2018), enabling in-depth analyses on drug related deaths (DRD). A grouping of all alcohol related deaths (ARD) was received from Statistics Finland.
For comparison, general population data was downloaded from Statistics Finland (retrieved 30.7.2020, licensed under CC BY 4.0). Life table by age and sex, 1986–2018 included survival rates of the Finnish general population (approximately 5.5 million people; Statistics Finland, 2020a). Additionally, information on deaths by underlying cause of death (54 groups), age and sex were retrieved including data on all Finnish people who had died between 1990 and 2018 (Statistics Finland, 2020b). Altogether 229,179 Finnish men and 95,295 women had died between age 15 and 64 years between 1990 and 2018, also including the studied men (2,687; 1.2%) and women (816; 0.9%). In the age group ≥64 years, the proportion of the study population was lower (0.11% of men and 0.02% of women).
Statistical Analysis
In the crosstabulations, percentages with 95% confidence intervals (CI) were calculated, and their differences were analyzed with Fisher's exact test or a chi-squared test. Differences in means of the continuous variables were tested with a t-test or Levene's test whenever equal variances could not be assumed. The effect sizes were estimated with mean absolute difference (MAD) and Cramer's V.
For comparison of age-specific mortality, the number of deaths and percentages with 95% CI by sex and decade of birth were calculated up to 1.1.2019 for the study population. The mean number of non-survivors in the general population for each birth decade was computed by compiling the yearly data and subtracting the mean survivor rate from 100,000. Age-specific death rates (ASDR) were calculated for the study and general populations by dividing the number of deaths at each age interval with the population of the age interval (Curtin & Klein, 1995). Standardized mortality ratios (SMR) were calculated by dividing the ASDR of the study population by the ASDR of the general population. Similarly, the SMRs for sex differences were calculated by dividing the ASDRs. To facilitate the comparison of the death rates, the expected numbers of deaths based on the mortality in the general population were calculated for comparison with the actual numbers of deaths (95% CI) in the study population.
Ethical Considerations
The ethical committee of the A-Clinic Foundation approved the study protocol. Permission was granted for retrieving data from registers regarding treatment, education, hospitalizations and mortality from each respective registry. The National Institute for Health and Welfare gave permission to combine the datasets.
Results
The 10,891 patients with SU were born mainly between 1933 and 1984 (97.0%; mean ± SD: 1,961.5 ± 13.4). At the time of the contact to the studied treatment unit between 1990 and 2009, the mean ± SD age was 37.5 ± 12.1 years; range 12–86 years). By 2019, more than one-third of the patients had died (n = 4,099; 37.6%). The mean ± SD time between death and the last known treatment contact was 7.9 ± 6.3 years (range 0–28.0 years).
Substance-Related Underlying and Further Causes of Death
Data on underlying and further causes of death were available for 4,012 deaths (97.9%). The underlying cause was substance related in 1,512 (37.7%) cases and, when further causes of death were added, the number increased to 2,684 (66.9%) substance-related deaths.
Out of the 4,012 deaths 1,828 (45.6%) were ARDs and the mean time of death after entering treatment was 9.3 years. Altogether, the proportion of ARDs was larger among those who had died between age 35 and 64 years (n = 1,512, 52.7%) than among the younger (18–34 years; n = 105, 23.0%) and older (≥64 years; n = 211, 30.6%) adults (χ2 = 214.8, df = 2, p < 0.001; Cramer's V = 0.245). The underlying cause of death was coded as alcohol related diseases or poisoning in 997 deaths (24.9%). The most common diagnoses were alcoholic liver diseases (481; 48.2%), alcohol intoxication (230; 23.1%), alcohol dependence (86; 8.6%) and alcoholic cardiomyopathy (52; 5.2%). Additionally, alcohol as a further cause was registered in 831 deaths (20.7%): the largest proportion in events of undetermined intent (in 27 out of 47; 57.4%) followed by accidents (195/350; 55.7%), homicides (35/66; 53.0%), suicides (112/409; 27.4%), other diseases (393/1,628; 24.1%), poisonings (63/414; 15.2%) and DRDs (6/101; 5.9%).
Altogether, there were 1,026 DRDs (25.6% of the 4,012 deaths) and the mean time for death was 7.6 years after entering treatment. Altogether, the proportion of DRDs was markedly higher among those who had died by age 35 (328; 70.5%) than among those aged 35–64 years (683; 23.8%) and ≥64 years (15; 1.5%; χ2 = 717.6, df = 2, p < 0.001; Cramer's V = 0.423). The underlying cause was drug related in 515 deaths (12.8% of all deaths), including 414 poisonings other than alcohol and 101 other drug-use related diagnoses, with 67 mental and behavioral disorders due to multiple drug use and use of other psychoactive substances and 21 opioid related disorders. Drug use as a further cause was registered in 511 deaths (12.7% of all deaths). In these cases, the underlying cause of death was most often suicide (in 281 out of 409; 68.7%), homicide (15/66; 22.7%), event of undetermined intent (10/47; 21.3%) or accident (72/764; 9.4%), but rarely alcohol-related (31/997; 3.1%) or other disease (102/1,728; 5.9%).
One-third (33.1%) of the 4,012 deaths were not registered to be substance related. The most common underlying cause among these 1,328 deaths were diseases of the circulatory system (33.4%, excluding alcohol-related causes), followed by malignant neoplasm of larynx, trachea, bronchus and lung (8.4%), other malignant neoplasms (18.8%), accidents (7.9%), diseases of the respiratory system (7.6%), suicides (4.7%), homicides (1.7%), and events of undetermined intent (1.2%).
There were some background related differences concerning substance related deaths. Not having secondary education was common; however, it was associated somewhat more often with DRDs than ARDs (58.2% vs. 50.2% respectively). Every other individual of those who had sought help for AUD only (n = 1,773/3,326; 53.3%) had died, and over half of these deaths (n = 998; 56.3%) were ARDs. One-quarter of those who had sought help for other or multiple SUDs (n = 1,276/4,429; 28.8%) had died and half of these were DRDs (n = 643; 50.4%), summing up to three-quarters (n = 961; 75.3%) when all ARDs and DRDs were considered. Death causes by sex and age are presented in detail in the sections below.
Comparison Between Men and Women
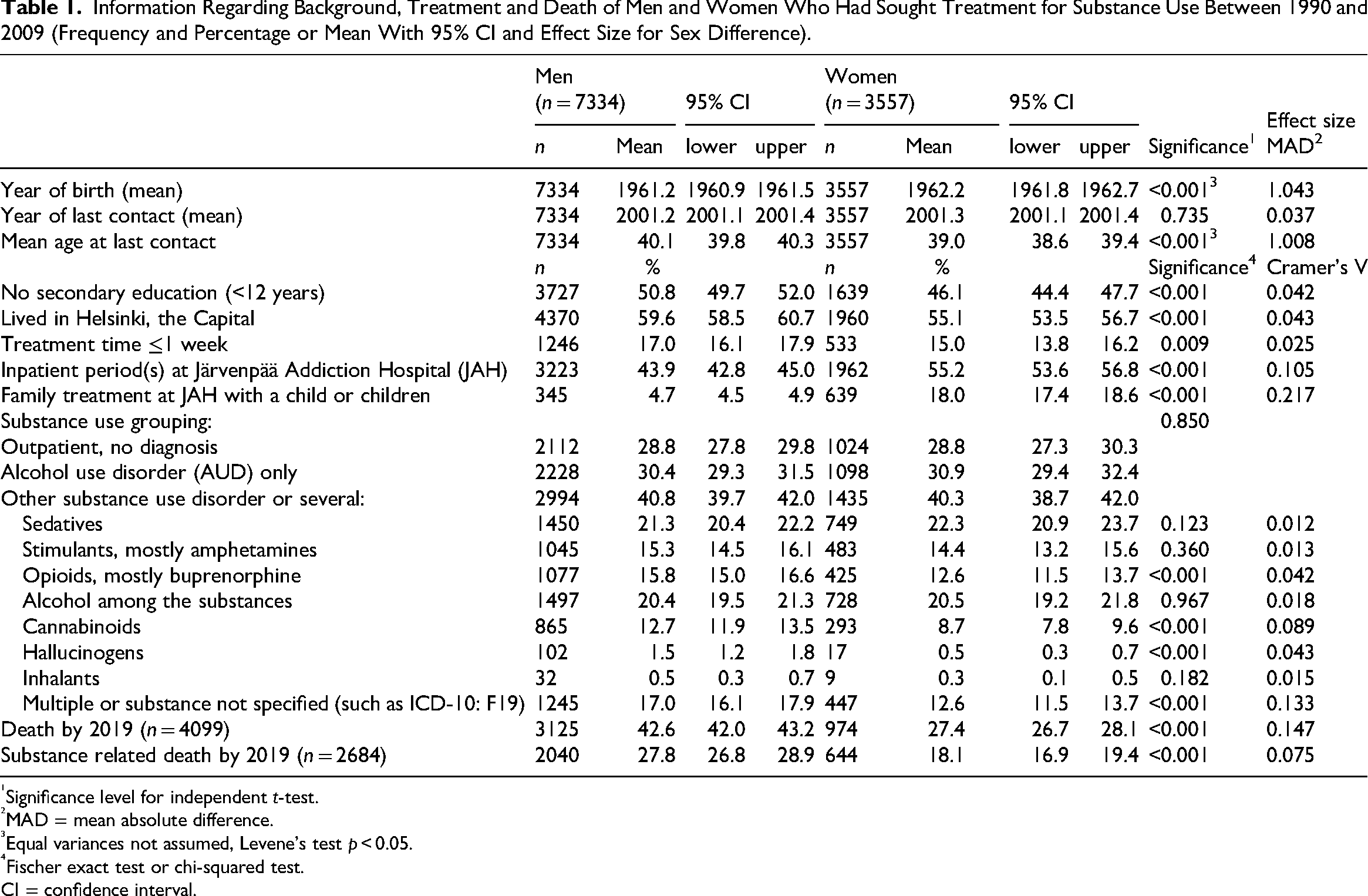
One third (32.7%) of the patients with SU were women. Table 1 provides an overview of the background of the men (n = 7,334) and women (n = 3,557). Proportionally more women had been inpatients at JAH and especially at the family treatment than men. A slightly larger proportion of the men were older, less educated or used several drugs compared to the women.
Information Regarding Background, Treatment and Death of Men and Women Who Had Sought Treatment for Substance Use Between 1990 and 2009 (Frequency and Percentage or Mean With 95% CI and Effect Size for Sex Difference).
Significance level for independent t-test.
MAD = mean absolute difference.
Equal variances not assumed, Levene's test p < 0.05.
Fischer exact test or chi-squared test.
CI = confidence interval.
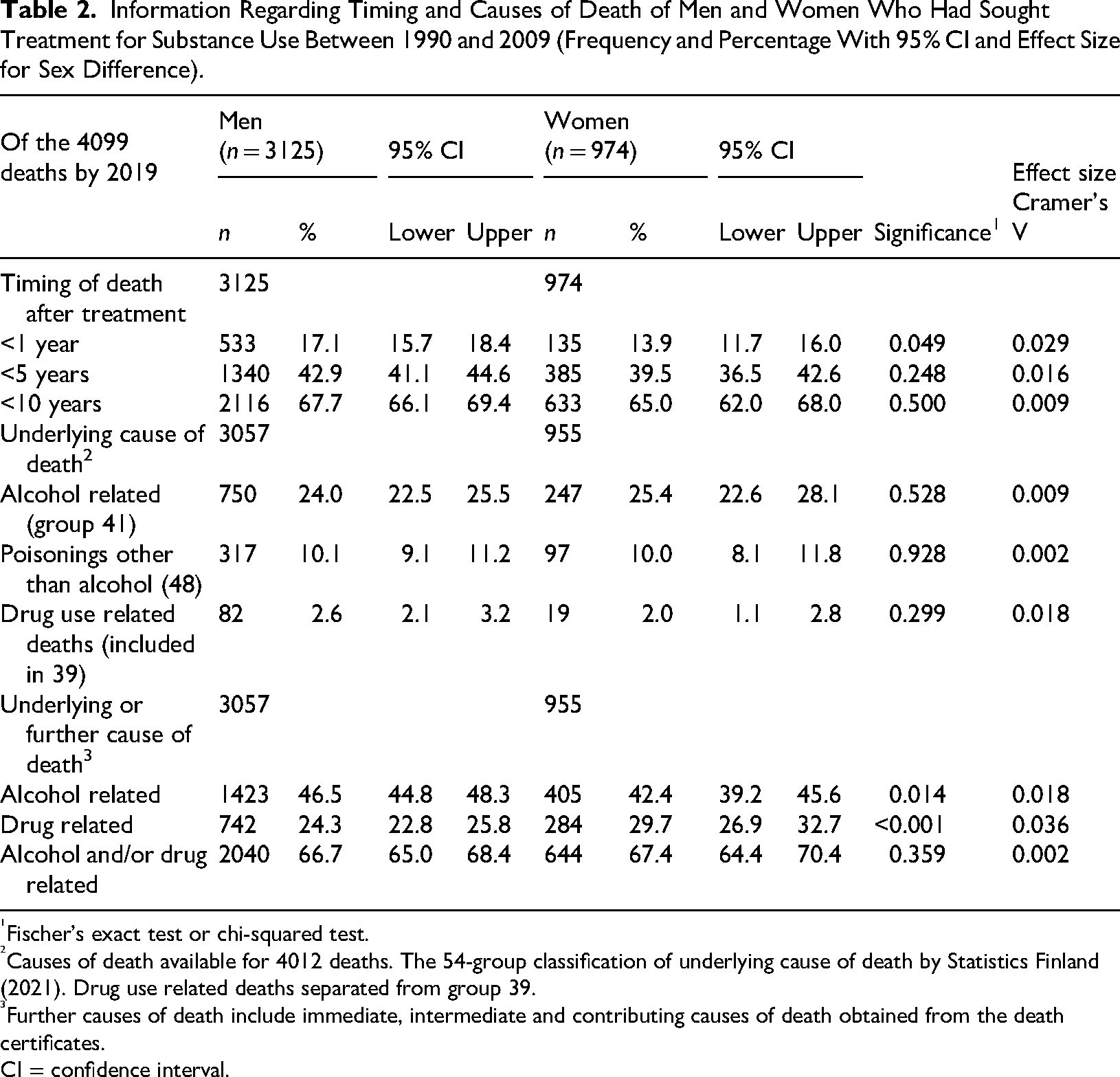
By 2019, markedly more men than women had died; however, there were few sex differences concerning those who had died. Even though the proportion of men who had died during the first year after treatment was slightly larger, the difference decreased by time (Table 2). There were no differences concerning substance related underlying causes of death, but, after adding further causes, the proportion of ARDs became larger among men but DRDs among women. The mean ± SD age at death was 51.5 ± 4.2 years for both sexes. For both men and women who had died between age 25 and 64 years, the proportion of not having secondary education was high (53.3% of 1509 men and 54.1% of 525 women).
Information Regarding Timing and Causes of Death of Men and Women Who Had Sought Treatment for Substance Use Between 1990 and 2009 (Frequency and Percentage With 95% CI and Effect Size for Sex Difference).
Fischer’s exact test or chi-squared test.
Causes of death available for 4012 deaths. The 54-group classification of underlying cause of death by Statistics Finland (2021). Drug use related deaths separated from group 39.
Further causes of death include immediate, intermediate and contributing causes of death obtained from the death certificates.
CI = confidence interval.
Underlying Causes of Death in Comparison to the General Population
General population data concerning underlying causes of death was available for comparison by sex in three age groups. Table 3 presents the comparisons for both men and women. Alcohol related diseases were more common among the men and women with SU than among the general population in all age groups and other poisonings up to age 64 years. Unfortunately, other drug-related causes than poisonings were included into the group “Other diseases” and thus not comparable.
Underlying Causes of Death in Three Age Groups Among Men and Women Who Had Sought Treatment for Substance Use in Comparison to the General Population Between 1990 and 2018.
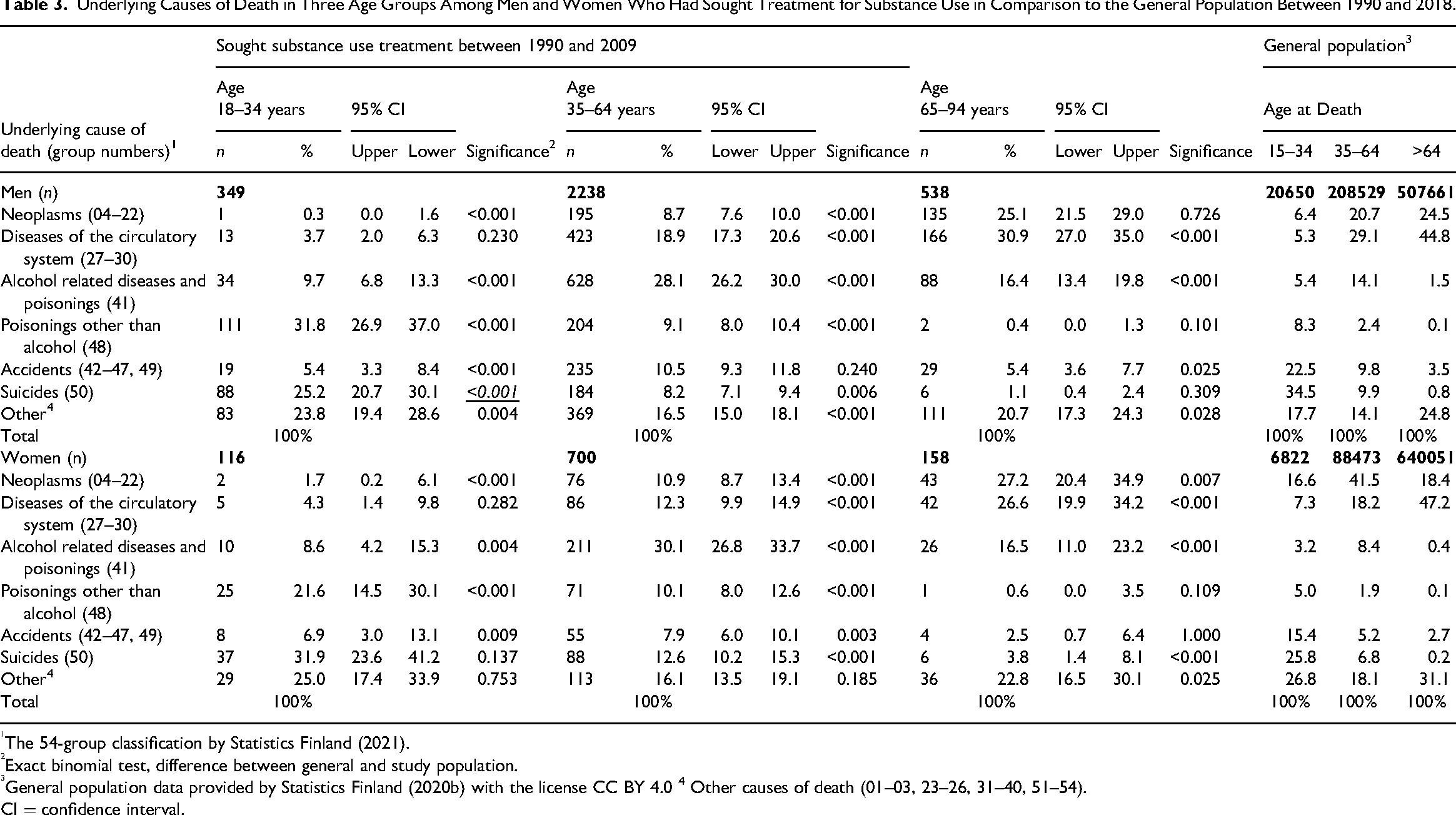
The 54-group classification by Statistics Finland (2021).
Exact binomial test, difference between general and study population.
General population data provided by Statistics Finland (2020b) with the license CC BY 4.0 4 Other causes of death (01–03, 23–26, 31–40, 51–54).
CI = confidence interval.
The proportion of suicides was higher among men than women in all age groups in the general population; however, the proportion of suicides was higher among women than men with SU (13.5% vs. 9.0% p < 0.001). Suicide was generally a common cause of death among the youngest age group and the proportion decreased by age. The proportion of suicides was higher among women with SU than in the general population after age 35 years.
Substance related underlying causes of death were more common among young adults with SU, whereas accidents were common among the general population of the same age. However, the proportion of accidents as a cause of death was higher among women with SU for age group 35–64 years and among men with SU in the oldest age group (>64 years) than among the general population. The proportion of neoplasm was lower among the women with SU until age 64 years but higher in the oldest age group in comparison to general population. It is to be noted that, although the study focused on substance-related deaths and their commonness in different age groups, the proportions concerning other types of deaths should not be interpreted as independent results.
Mortality in Relation to the General Population
The death rates of the men and women with SU were compared with those of the general population by decade of birth (Table 4). The SMRs showed that the sex differences were smaller and mortality higher among those with SU than in the general population. The difference to the general population increased decade by decade, and more among women than men; the SMRs showed an increase from 5.4 to 13.8 among women and from 4.0 to 9.8 among men from the birth decade 1950s to the 1980s.
Deaths by 2019 of Men and Women After Substance Use Treatment Between 1990 and 2009 and of the Accompanying Boys and Girls in Comparison to the General Population1 by Decade of Birth and Gender.
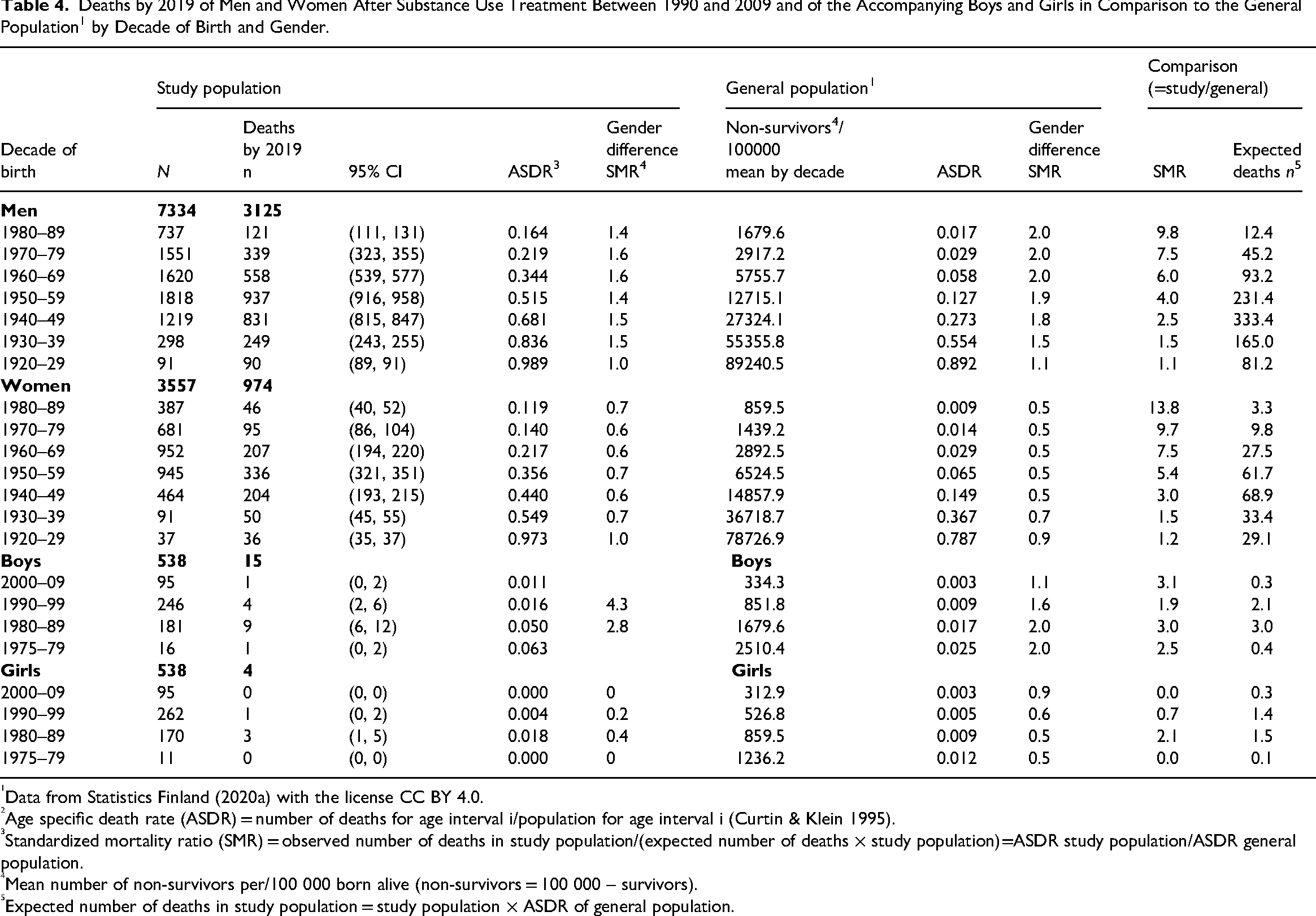
Data from Statistics Finland (2020a) with the license CC BY 4.0.
Age specific death rate (ASDR) = number of deaths for age interval i/population for age interval i (Curtin & Klein 1995).
Standardized mortality ratio (SMR) = observed number of deaths in study population/(expected number of deaths × study population)=ASDR study population/ASDR general population.
Mean number of non-survivors per/100 000 born alive (non-survivors = 100 000 – survivors).
Expected number of deaths in study population = study population × ASDR of general population.
The mean time between death and the last known treatment for SU was 7.5 years for men and 8.1 years for women, indicating the need for a long follow-up time when studying substance related mortality. Figure 2 shows the proportions of deaths and the timing in relation to the last known treatment contact by decade of birth and sex. Despite the overall higher mortality among men, similar patterns of mortality post-treatment are observed for both sexes, with slightly under one-fifth of deaths occurring during the first year after treatment, and two thirds during the first decade post-treatment.
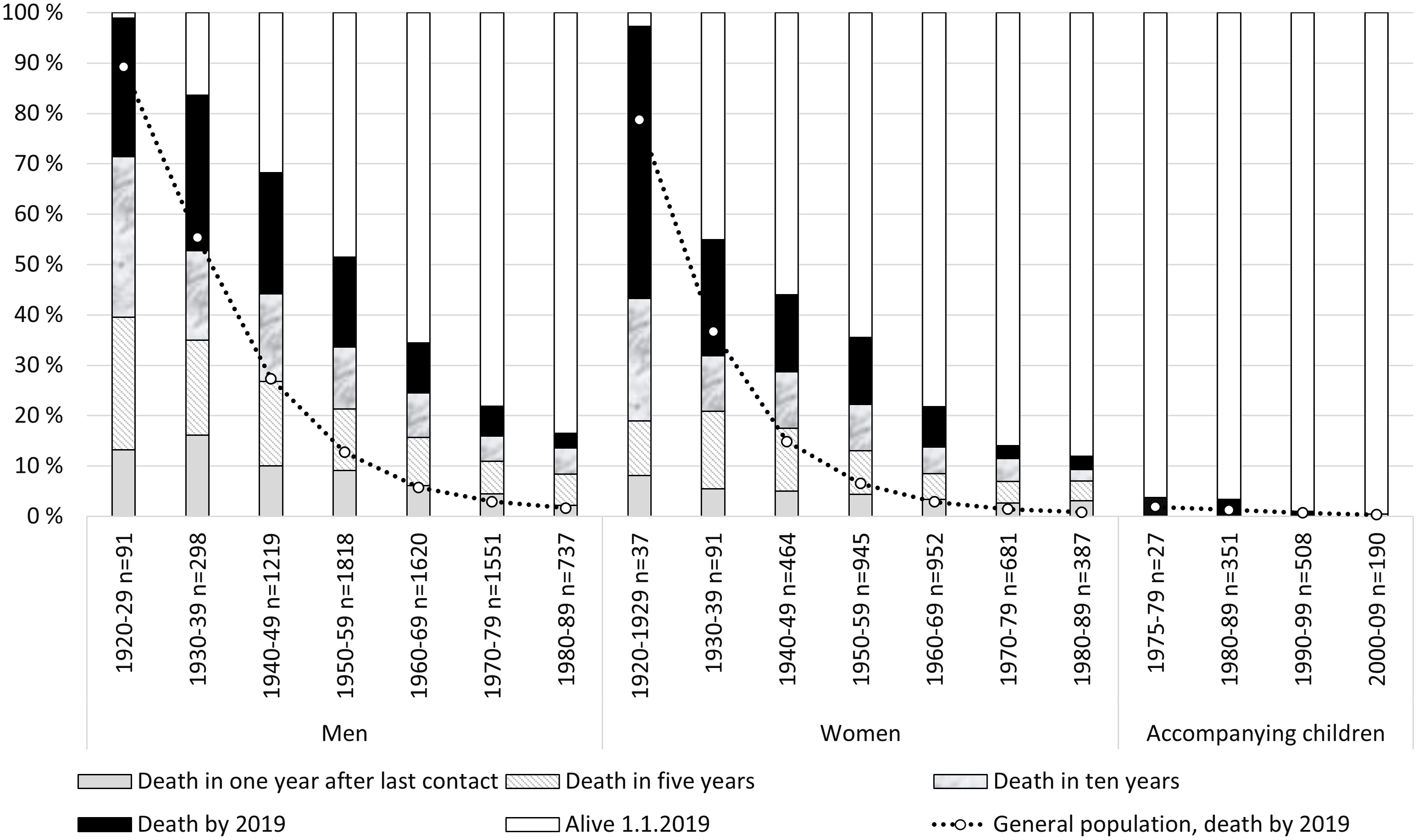
Death in 1, 5 and 10 Years After Last Contact to the Studied Substance Use Treatment Units Between 1990 and 2009 and All Deaths by 2019 of Men, Women and Accompanying Children by Decade of Birth in Comparison With the General Population. Note: General Population Data Retrieved from Statistics Finland (2021) With the License CC BY 4.0; Approximate Percentages Based on Survival Rates by 100,000 Calculated by Decade of Birth.
Mortality of the Accompanying Children
The treatment data included a special group of children who had accompanied their parent(s) to the family treatment unit of JAH between 1990 and 2009. These 538 girls and 538 boys were born between 1975 and 2009 and thus their age varied from 9 to 35 years at the end of the follow-up. By 2019, slightly more boys (15; 2.8%) than girls (4; 0.7%) had died (Fisher's exact test, p = 0.009). The time and the causes of deaths were studied to better understand the mortality of these children. Out of the 1,076 children, two had died by age 5 years within 2 years after having been in family treatment and 17 children had died between age 16 and 35 years, two of them within 10 years and the rest between 14 and 25 years after the family treatment. The underlying cause of death was categorized as suicide, assault or event of undetermined intent for seven children, as disease for six children and as accident for another six children. When information on further causes of death was also utilized, 12 out of the 19 deaths were reported to be substance related and only three deaths were neither violence nor substance related. For 17 children, death record data was available also for some of their family members. Eight families had lost the parent who had sought family treatment for SU (6/14 mothers and 2/9 fathers); however, none of the accompanying nine siblings had died. Three parents had died before the child and in two cases the parent and the adult child had died in the same accident.
The SMRs of these children who had been raised in a family with parent(s) who had sought treatment for SU did not differ significantly from the SMRs of the age-matched general population, except for boys born in the 1980s (Table 4); however, the death rates of the children were lower than the death rates of the age-matched men and women with SU.
Discussion
In this follow-up study, every one-third of those who had sought treatment for SU had died and two-thirds of the deaths were substance related. The death rates were markedly higher in comparison to the age-matched general population. The difference in mortality increased decade by decade, being the highest among the youngest age groups where most life-years are lost. A small number of children who had accompanied their parent(s) to family treatment had died; however, most of these deaths were substance or violence related.
Previous studies on causes of death in the context of SUD have reported overdose as the most common cause of death (Bartu et al., 2004; Bauer et al., 2008; Mathers et al., 2013; Nyhlén et al., 2011; Ravndal et al., 2015) followed by suicide and external causes (Degenhardt et al., 2009). We also found poisonings due to other substances than alcohol and suicides to be most prominent underlying causes of death among youngest age group. In comparison with earlier studies, our observation period was long, and the data consisted of people seeking help for variety of substance use problems. In the present study, alcohol related causes of death were common among the older age groups that used mainly alcohol. Altogether, two-thirds of the deaths were substance related, implying that SU played a role in the lives of the patients after treatment and that only looking at the underlying causes could underestimate this relationship. The information about further causes provided important additional insight to the mechanisms relating to the cause of death.
Generally, less women than men with SU had died during the follow-up. In comparison with the general population, the highest mortality was observed for young women with SU, which is in line with previous findings that the mortality hazard ratio due to SU has been stronger for women compared to men (Kendler et al., 2016; Kendler et al., 2017). The proportion of suicides was high among older women with SU, as were drug related further causes of death, whereas alcohol related further causes were more prominent among men with SU. Overall, there were markable sex differences between those who had sought help, but less among those of them who had died. Also, the sex difference between Finnish men and women who had sought treatment for SU was shown to be smaller in subgroups with the history of imprisonment (Kaskela & Pitkänen, 2018) and psychiatric in-patient care (Levola et al., 2022).
A personal history of SU was associated with higher mortality than being raised in a family with parent(s) who had sought treatment for SU. A small number of accompanying children had died. In comparison with the general population, the death rate was significantly increased only for sons in young adulthood, still being much lower than death rates of same aged men who had sought treatment for SU for themselves.
Because the overall death rate after seeking treatment for SU was much higher than in the general population, it seems that there is a high risk for premature mortality for many years after the treatment. Most of the deaths occurred several years after seeking help but still being premature. These results were in line with previous studies with shorter follow-up times, where a risk of death has been found to be higher among people who have received treatment for SUD compared to the general population (Gossop et al., 2002; Lindblad et al., 2016). A long follow-up was needed for studying the variation in timing of deaths and for an in-depth understanding of the causes of death related to SU, as well as the life-course of the children. In the future, increased follow-up time will provide new possibilities for analyzing the current data; for example, hospitalizations, criminality and the child-parent dyads, as well as provide valuable knowledge on the life-course and needs of the children of parent(s) with SUD.
Strengths and Limitations
This study has several strengths. A large, real-life sample including former in- and outpatients and accompanying children was available for use. The use of several nationwide registers enabled comparisons with the general population and a long follow-up time with very little missing information. However, when interpreting these results, it has to be taken into consideration that the follow-up time varied between 9 and 28 years according to the time of entering into the data and the year of birth. During the period covered by this study, numerous changes occurred concerning the used substances, treatment practices, as well as sex differences and characteristics of people who seek treatment for SU (Pitkänen et al., 2017). In the 1990s, treatment for alcohol use and long inpatient periods were common and, in JAH, even daycare and school were available for accompanying children. By 2009, treatment for drug use as well as DRDs had become more common, the treatment periods were shorter, the proportion of treatment seeking women had grown and most of the accompanying children were newborns or toddlers.
A socially disadvantaged childhood and parental SU have been associated with increased mortality in offspring (Kauhanen et al., 2006; Landberg et al., 2018). However, over-generational cycles and accumulation of problems are multifaceted and complicated issues. Typically, families engaging in family treatment have also been intensively involved with child welfare services with the long-term aim of promoting the health and well-being of these children, who often have met various adversities early in life. It is possible that the risk of premature death is associated with the received support, such as family treatment and other interventions as speculated also by Elsenburg et al. (2022). In the current sample, it can be expected that the accompanying children were mostly very young, even unborn, when the treatment seeking family had started to receive social or other special services. Unfortunately, there was no access to data on other specialized services, and further studies are needed. However, entering the family treatment path might be beneficial and thus affect the generalizability of the results.
When studying the proximity of deaths to treatment, it is to be noted that, even though we had data on all hospitalizations during a specific time period, we did not have information on all other possible treatment options. In most cases, when a person is discharged from inpatient treatment, treatment does not end but continues in an outpatient setting. The number of studied outpatient clinics was small and included urban residents only. Therefore, because JAH offers treatment nationally and inpatient treatment at this unit is typically reflective of a severe course of SUD, the results regarding these patients are not generalizable to all individuals seeking treatment for SU. Further studies are needed for different types of treatment settings.
Conclusions
The risk of death is increased for a long time after seeking SU treatment, especially for substance related deaths, indicating the need for sufficiently sustained after care and easy treatment re-entry. In comparison with the general population, the risk was highest among young adults but remained high until old age for both men and women with SU. Sex differences typically exist in connection to SU and mortality rates; however the deaths of the studied men and women resembled each other, indicating a more detrimental impact of SUD for some women. The high proportion of suicides as well as drug-related further causes of death among women with SU yield attention. The personal history of seeking help for SU was associated with higher mortality than that of those who had been raised in a family with parent(s) who had sought treatment. This pioneer study on accompanying children shows the need for further long-term follow-up studies with modern structured treatment data.
Footnotes
Author Contributions
TP, TK and JL were responsible for conceptualization; TP, TK and RL were responsible for formal analysis; TP, TK and VU were responsible for investigation; TP was responsible for methodology; TP and JL were responsible for writing – original draft; RL, TK and & VU were responsible for writing – review & editing; All authors approved the final version of the manuscript submitted for publication.
Funding
The data collection has been funded by the Finnish Ministry of Justice and the Finland's Slot Machine Association (RAY). Finalization of this article was undertaken as part of the Out of Despair project, funded by the Strategic Research Council established within the Academy of Finland under a grant for the Out of Despair project (352600), Finnish Youth Research Society (352603), and A-Clinic Foundation (353249). We gratefully acknowledge the resources made available by the Alli Paasikivi Foundation, the Finnish Foundation for Alcohol Studies, the Yrjö Jahnsson Foundation, and the International Max Planck Research School for Population, Health and Data Science (IMPRS-PHDS).
Declaration of Conflicting Interests
All authors have worked as independent researchers and JL as a medical doctor at the A-Clinic Foundation, where TK is also currently working. The A-Clinic Foundation is a non-profit, non-governmental organization in the field of addictions for which the daughter company A-Clinic Ltd offers treatment and rehabilitation services.
Data Availability
The treatment and register data are not publicly available due to their containing information that could compromise the privacy of research participants. General population data by Statistics Finland is freely available, licensed under CC BY 4.0.