
Abstract
Background
Denmark and Sweden have similar welfare systems, but different drug policies. Denmark has historically a more liberal and more harm reduction-oriented drug policy than Sweden. On this background, we present a study of risks and use of formal and informal resources among structurally vulnerable people who use drugs in Copenhagen in Denmark and Malmö in Sweden.
Methods
The study reports from research projects in each city that investigated the everyday lives and risks- and enabling environments of structurally vulnerable people who use drugs. Both projects involved the same survey. Participants were recruited at treatment and low-threshold services in Copenhagen (n = 243) and Malmö (n = 231).
Results
The participants in the two cities used many different resources provided by the welfare system, but participants from Copenhagen made more use of available harm reduction services. The participants from Malmö used drugs in more risky settings and relied more on other people who use drugs for resources and had more concerns regarding overdoses and other drug-related harms and about being arrested by the police.
Conclusions
In both cities, the Nordic welfare state plays a large role in providing resources, but drug policy can influence access to harm reduction resources and the experience of criminalization. These differences can play a role in shaping the local risk environments, although the patterns identified should be interpreted with caution given the exploratory nature of the study. More comparative research is needed to explore how drug policy shape risk environments.
Introduction
Denmark and Sweden, separated only by the narrow Öresund strait and connected by the Öresund bridge, offer a unique opportunity to compare drug policies. Despite their geographical proximity, the two countries have historically divergent approaches to drug policy. In 2014, Swedish researcher Bengt Svensson highlighted that while a mere strait separates Denmark and Sweden, the distance between their policies is more like an ocean (Svensson, 2014). This study examines whether this disparity persists and its implications for the risks and resource accessibility for people who use drugs.
As Nordic welfare states, Denmark and Sweden provide extensive benefits and services to their citizens. However, their drug policies have differed significantly. Denmark has traditionally adopted a lenient drug control policy and emphasized harm reduction (Houborg & Møller, 2021). By contrast, Sweden has maintained strict drug control policies, with harm reduction playing a lesser role. Recent years have seen some convergence in their policies, yet notable differences remain (Bjerge et al., 2016; Holeksa, 2024).
Drug policy is often shaped at the local level, where stakeholders directly confront drug-related issues (Wodak, 2006; Kübler & Wälti, 2001). In Denmark and Sweden, municipalities play a crucial role in implementing drug policies, leading to variations in service availability and quality. This local dimension complicates the comparison of national drug policies.
The present study explores how drug control and harm reduction measures may shape perceived risks and access to resources for people who use drugs in Copenhagen and Malmö. By examining perceived risks, drug use practices and access to support, some of which we interpret as indicators of risk based on prior research, we aim to explore how policy implementation in two similar welfare systems with different drug policies may affect local risk environments and lived experiences. The research is based on structured interviews with 474 people who use drugs in Copenhagen (n = 243) and Malmö (n = 231).
The Political Economy of Drug-Related Harms
To understand vulnerability to drug-related risks and social harms, it is important to apply a perspective that considers socioeconomic conditions and access to social and healthcare provisions, rather than focusing solely on specific drug policies (Stevens, 2011; Currie, 1994; Waterston, 1997; Rhodes et al., 2012). While drug use is widespread, the most harmful patterns and severe consequences are concentrated among socioeconomically disadvantaged groups (Stevens, 2011). For example, Bourgois (2003) argues that the crack epidemic in the USA during the 1980s was driven not by the pharmacology of crack, but by socioeconomic inequality. Rhodes et al. (2012) highlights how social, political and economic structures create and perpetuate vulnerability to HIV among marginalized groups. Therefore, drug policy should be understood within the context of the political economy and broader social policies that distribute resources and risks within society (Waterston, 1997; Stevens, 2011; Currie, 1994; Jauffret-Roustide et al., 2022). This does not suggest that drug policy is insignificant; rather, it should be viewed as part of the broader management of social, economic and health risks, which it can both complement and contradict (Benoît, 2003; Stevens, 2011).
Risk Environments and Drug-Related Harm
To understand the vulnerability to drug-related harm, a heuristic framework has been developed that positions individuals and groups within risk environments. These environments both generate and mitigate harm (Rhodes, 2002, 2009; Moore & Dietze, 2005; Duff, 2010). The framework emphasizes the role of structural and social factors in shaping risks related to health and social harms associated with drug use. It shifts focus away from individual behavioral change as the primary driver for preventing harm and instead examines the interaction between individuals and their social, cultural, political and economic environments.
A risk environment comprises two dimensions: types and levels of environmental influence (Rhodes et al., 2005). Types of environmental influence include physical, social, economic and policy factors. Levels of influence are categorized as micro, meso and macro: Micro-level factors pertain to interpersonal relationships among people who use drugs and how these relationships affect exposure to risks. Meso-level factors relate to social and group-level factors, such as group norms influencing risk behavior, as well as institutional and organizational responses such as local implementation of harm reduction services and policing strategies. Macro-level factors encompass legislation, policies and economic conditions that shape meso- and micro-level influences. Rhodes et al. (2005) emphasize that macro-structural factors do not necessarily correlate with harm in a linear fashion. Therefore, it is crucial to consider how local risk environments are structured when aiming to reduce drug-related harm, rather than assuming universal applicability of strategies effective in one setting.
Drawing inspiration from the risk-environment framework, this study discusses how welfare and drug policy in Copenhagen and Malmö play a part in structuring the risk- and enabling environments of structurally vulnerable people with lived experience of substance use in the two cities.
Similar Welfare States
Denmark and Sweden are similar Nordic welfare states characterized by a high degree of decommodification of socioeconomic risks (Esping-Andersen, 1990) achieved through comprehensive, tax-based social insurance systems that provide citizens with free social and health services and benefits. The tax-based welfare model also facilitates economic redistribution, resulting in relatively low levels of social and economic inequality compared to many other countries. While both countries have structures and policies that can be expected to minimize the populations’ vulnerability to drug problems and drug related harm, it does not mean that there are not groups who are vulnerable to drug-related harm due to poverty, homelessness, social exclusion, discrimination and stigmatization. The group of concern in this study comprises people who are in such a structurally and socially vulnerable position.
Different Drug Policies
Denmark and Sweden have historically differed in their drug policies, although some convergence has occurred in recent decades. Since the 1960s, both countries have viewed “the drug problem” as a “social problem” rather than a medical one, but their drug policies have evolved differently based on how drug use is perceived and different policy goals. In Denmark, drug use is generally seen as an inherent part of society, with policies aimed at reducing the harms it causes. In Sweden, drug use has been viewed as alien to society and the drug policy strives for a drug-free society (Bjerge et al., 2016; Houborg, 2008; Edman, 2013). Against this background, we focus on two key policy areas, namely drug control policy and harm reduction policy, where there a several differences between the two countries. Most importantly, Sweden criminalizes both drug possession and use, whereas Denmark only criminalizes possession. This distinction allows Swedish law enforcement to intervene more directly in the lives of people suspected of drug use (Richert & Nordgren, 2025). Another key difference is that Denmark has introduced different forms of decriminalization over the years. From 1969 to 2004, personal drug possession was de facto decriminalized (Houborg, 2010; Storgaard, 2000; Jepsen, 2008). In 2004, this was replaced by a zero-tolerance policy, but economically disadvantaged people dependent on other drugs than cannabis were decriminalized for possession of illegal drugs for personal use. Furthermore, in 2012, legislation on drug consumption rooms (DCRs) involved further decriminalization of possession of drugs for use inside DCRs and in immediate vicinity of such services. This means that, for the group that is the subject of this study, there is a wide difference between the drug control regimes they live under in the two countries.
Harm reduction is also an area where there have historically been large differences between Denmark and Sweden, although there has been a trend towards convergence in recent years. In both Denmark and Sweden, early experiments with opioid substitution treatment (OST) were abandoned in favor of an abstinence-based treatment approach. However, in the mid-1980s, a principle of “graduated goals” was introduced in Danish drug treatment, where harm reduction became a legitimate goal (Narkotikarådet, 1984; Houborg, 2006), which led to abandoning restrictions on OST (Ege, 1997). With other harm reduction measures, Denmark has had earlier and more comprehensive rollout than Sweden. Needle exchange programs (NEP) were introduced in the 1980s, heroin-assisted treatment (HAT) in 2008, DCRs in 2012 and naloxone in 2019. Historically, Sweden has seen significant resistance to harm reduction leading to delays in implementing some services, and to strict regulations and high thresholds for OST and NEP. Therefore, access to harm reduction services has been limited, and has varied widely across different regions (Richert et al., 2023; Holeksa & Richert, 2024). In Sweden, the wider implementation of OST came later than in Denmark but is comprehensive today. Until recently, there were only a few NEPs in Sweden, one of them in Malmö, established in the 1980s. Take-home naloxone programs began to be implemented in some regions from 2019, but access to interventions varies in different regions. Sweden does not have HAT or DCRs.
Local Drug Policy in Copenhagen and Malmö
Copenhagen offers a comprehensive array of services. It has a long tradition for low-threshold OST where harm reduction is a key goal. Injection and smoking equipment are widely available at OST centers, drop-in centers, shelters, health clinics and other places without control or registration. Naloxone sprays and naloxone training are offered by various municipal and private organizations. At the Vesterbro open drug scene in central Copenhagen, there are two drug consumption rooms (DCRs), with a third exclusively for women opened after data collection. The municipality also offers HAT. At three of the main shelters for the homeless in the city, drug use is permitted. Additionally, low-threshold social and health services are accessible to people who use drugs, particularly near the open drug scene. There are two user-led organizations in Copenhagen, Brugernes Akademi and Brugerforeningen, who offer harm reduction and support such as clean drug consumption equipment, food and access to other resources. Concerning drug law enforcement, the whole area where the open drug scene and the DCRs are located is decriminalized for people who use the DCRs and the police should not confiscate their drugs. In the rest of the city, the national policy of decriminalization of economically disadvantaged people who are dependent on hard drugs applies, but, in these areas, the police can confiscate their drugs.
Malmö has driven harm reduction further than other municipalities in Sweden (Richert et al., 2023). OST is provided by both public and private clinics with easy access and no waiting time, but with somewhat stricter control and regulations than to most OST clinics in Copenhagen. Malmö has one NEP with a comprehensive range of services. However, the program has an age limit of 18 years, as well as requirements for identification and regular testing for hepatitis, which may discourage some people from visiting it (Nordstedt, 2023). A pilot project with take-home naloxone was implemented during the time of data collection. This project has now been made permanent, and naloxone kits are distributed via OST and the NEP (Håkansson et al., 2024). Malmö offers other services for people who use drugs, including outpatient clinics for youth and adults, open support programs and outreach work. In addition, several voluntary organizations like the Swedish Church and the City Mission offer low threshold help and support (mainly food, clothing and places to rest), but few user-led harm reduction initiatives. There is a low-threshold residential service called Sigtunaboendet, which is unique in Sweden in its harm reduction approach. It accepts homeless people with active drug use and allows the use of drugs in the apartments. Additionally, Housing First is provided by the social services to some adults with long-term homelessness and psychiatric comorbidity. There is no HAT or DCRs available in Malmö. The police in Malmö have generally been positive toward harm reduction initiatives (Nordgren et al., 2022). Although the focus of drug law enforcement is directed at young persons who use drugs or first-time offenders, people with extensive drug problems also risk being punished for drug possession or use (Richert & Nordgren, 2025).
Methods
The present study is based on surveys of people who use drugs in Copenhagen and Malmö where the same questionnaire was used in face-to-face interviews in the two cities. In total, 474 interviews were conducted: 243 in Denmark and 231 in Sweden. In Malmö, the study was conducted between August 2019 and October 2020, and in Copenhagen between October 2018 and July 2019.
In Malmö, respondents were recruited at seven services for people who use drugs: the NEP, a civil society café service for people experiencing homelessness and drug problems, a supported accommodation for women who use drugs, two different low threshold supported accommodations, and two different OST clinics. The inclusion criteria were self-reported illicit drug use and being a visitor at the services where recruitment took place. As such, recruitment was based on an opportunistic strategy. The interviews were conducted by two trained research assistants who filled out the survey based on the answers of the respondents. The interviews were conducted in separate secluded rooms at the services. The respondents were reimbursed with a 200 SEK food retail store and pharmacy voucher for their participation.
In Copenhagen, a similar approach was used. Visitors at 12 services for people who use drugs in three areas of Copenhagen were interviewed: four OAT services, two DCRs, three shelters for homeless people and three drop-in centers. Interviews were conducted by a team of researchers and research assistants. Before interviews were initiated, interviewers made sure that respondents were using or had been using other drugs than cannabis, such as heroin, cocaine, crack or illegal methadone. The Danish respondents were reimbursed with a 200 DKK voucher for food retail stores. The interviews lasted between 40–120 min in both cities.
It is important to emphasize that the samples were opportunistic and service-based, meaning they do not represent all people who use drugs in Copenhagen and Malmö. Differences in recruitment strategies e.g., more participants via OST in Copenhagen (54% compared to 16% in Malmö) may also influence results (see limitations).
Research Ethics
The respondents were informed about the study and their right to withdraw from it at any time, before agreeing to participate. They gave their informed consent by either a written signature on an informed consent document, or orally. The Swedish part of the study was approved by the Swedish Ethical Review Authority (Dnr. 2019-06509). The Danish part was approved by the Danish Data Protection Agency via Aarhus University (journal number 2016-051-000001, serial number 883).
Variables and Analysis
For the analyses presented in this study, we selected variables that can inform about the everyday lives and risk- and enabling environments of the two populations that can then be discussed considering our presentation of the drug policies in the two cities. The variables included for analysis are:
Sociodemographics
Age, gender, citizenship, housing and income.
Drug Use
Types of drugs used and the locations where drugs are consumed.
Marginalization and Entrenchment
The social relations and networks of the respondents with people who use drugs and people who do not use drugs as well as how different relations are valued.
Use of Formal Resources
Includes social, health, and security services provided by public or private organizations in the two cities.
Informal Resources
Includes drug-related and non-drug-related resources provided through the social networks and relationships of the respondents.
Everyday Concerns
Includes different kinds of concerns regarding, for example drugs, economy, health and relationships.
Some of the variables in our analysis, such as everyday concerns, reflect the participants self-reported perceptions of risk. Others, such as drug use settings, are interpreted in the studies as risk indicators, based on prior literature on structural vulnerability and harm reduction (Rhodes, 2002; Bourgois & Schonberg, 2009; Small et al., 2007). We distinguish between these where relevant in the analysis but use the broader term “risk environments” to encompass both perceived and interpreted dimensions of risk.
Measures and Analytical Approach
For each item in the questionnaire, a positive response was coded as present (e.g. if a respondent reported that they injected drugs, a code of “Yes” was assigned). In comparing the two cities, we used Pearson’s chi-squared test for nominal variables and t-tests for continuous variables. P < .05 was considered statistically significant.
Results
When comparing the results from the two cities, the results should be interpreted with caution. Although several statistically significant differences are observed between the two cities, many differences are modest, and some results were not significant. Moreover, due to the non-random sampling strategy, these findings are not generalizable. However the results may nonetheless offer useful insights into how local policy contexts intersect with risk environments.
Demographic and Socioeconomic Status
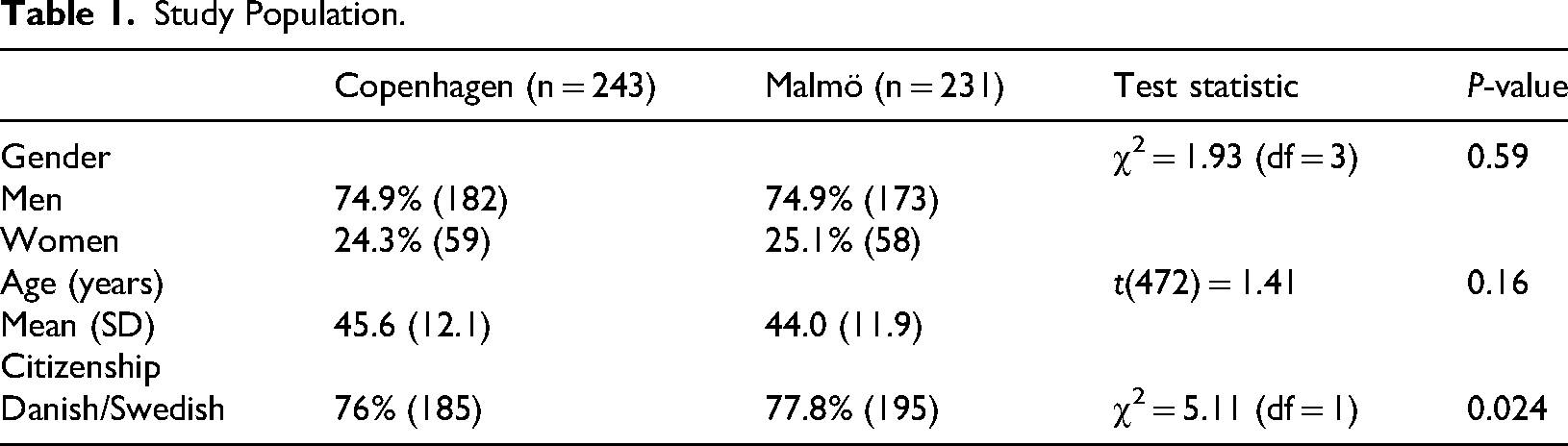
The study populations in Copenhagen and Malmö are similar in terms of basic demographic characteristics and socioeconomic status. Three-quarters of the participants are men, the average age is in the mid-forties and three-quarters hold Danish or Swedish citizenship (see Table 1).
Socioeconomically, very few participants had full-time employment: three (1%) in Copenhagen and seven (3%) in Malmö. The vast majority received social assistance (50% in Copenhagen and 58% in Malmö) or early retirement pension (21% in Copenhagen and 15% in Malmö). The very low employment rate and dependence on public benefits indicate significant economic vulnerability, which for many is exacerbated by the need to purchase drugs.
Housing
In terms of housing, the two populations are similar with no significant differences. Around half in both cities had their own homes, while a quarter in Copenhagen and almost a third in Malmö lived in housing services. A little under a quarter in both cities had unstable housing, such as temporarily staying with friends or sleeping outdoors. The near quarter of participants in each city with unstable housing indicates structural vulnerability related to housing, which can exacerbate health issues, including drug-related harms, social issues such as violence and difficulties in accessing necessary services (Koo et al., 2008; Lee & Schreck, 2005).
Drug Use
Most participants in both cities are poly-drug users who often supplement drug use with heavy alcohol consumption. While there are similarities in the types of drugs used, there are also notable differences. Heroin is popular in both populations, with around 40% in each city having used the drug within the past year. Stimulants are the most popular type of drug in both cities, but the types of stimulants used differed. Reflecting Sweden's long history of amphetamine use, a significantly larger proportion in Malmö than in Copenhagen had used amphetamine (57% vs. 18%) and methamphetamine (23% vs. 6%). In Copenhagen, cocaine is the most popular stimulant, with a significantly larger proportion of the population having used this drug than in Malmö (64% vs. 41%). This reflects a shift in Copenhagen starting around twenty years ago, where cocaine began to replace heroin as the most popular drug (Olsen et al., 2011). Additionally, a significantly larger proportion of participants from Copenhagen than from Malmö had used illegal methadone (42% vs. 16%), which may reflect a more liberal methadone prescription policy in Copenhagen. Conversely, a significantly larger proportion of participants from Malmö had used benzodiazepines (54% vs. 43%), which may reflect differences in prescription practices. In Denmark, efforts have been made to reduce benzodiazepine prescriptions and to prescribe less potent ones.
Drug Consumption Settings
From a risk-environment and harm reduction perspective, the setting where drugs are consumed is crucial because it affects exposure to risk. We asked participants about the settings where they had used drugs in the past week, which provided insights into both the physical and social environments of drug use. Given the instability that likely characterizes many of these participants’ lives, their substance use in the past week may not accurately reflect their typical patterns of consumption but gives a cross sectional view of the recent pattern.
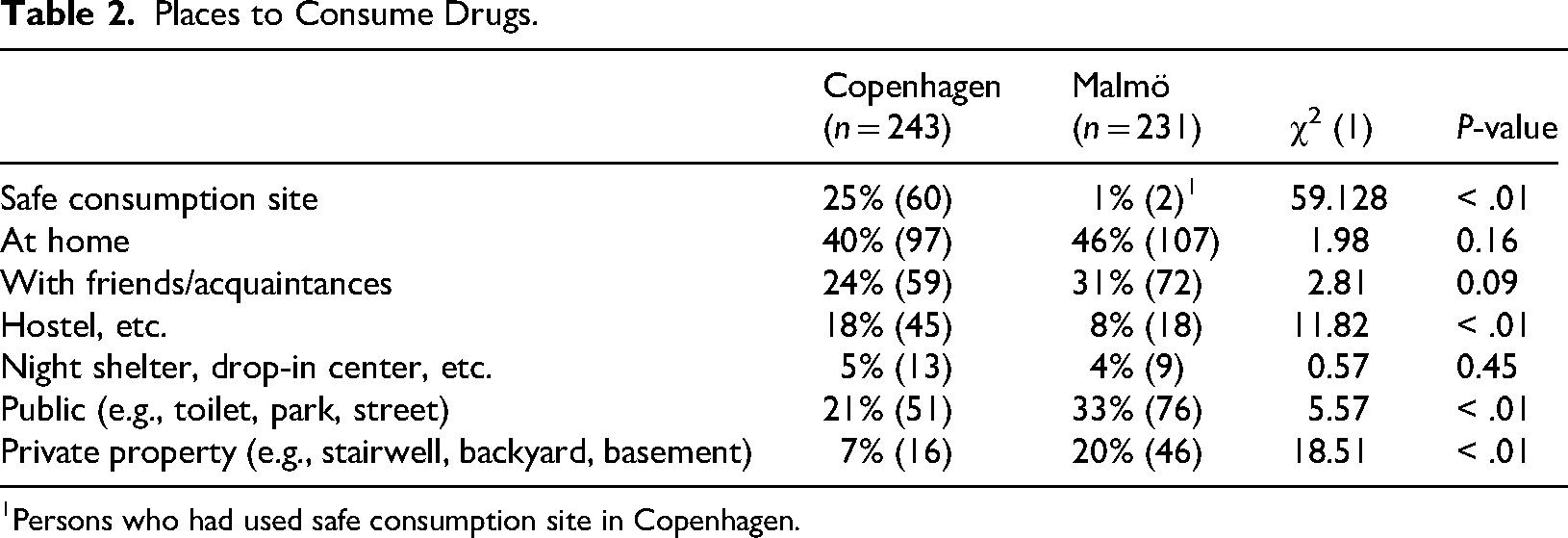
There were several significant differences in the drug use settings, reflecting differences in the risk environments (Table 2).
First, a significantly larger proportion of participants from Copenhagen had used DCRs (25% vs. 1%), reflecting the availability of two DCRs in Copenhagen, while Malmö has none. This is a crucial difference, as DCRs provide a clean and supervised drug use environment to reduce harm.
A significantly larger proportion of participants from Copenhagen had used drugs in hostels and other housing services (18% vs. 8%). Hostels may be high-risk environments, particularly if drugs are consumed alone in a room, but may also be enabling environments if harm reduction services and approaches are implemented by staff.
Public places like toilets, parks and streets, as well as private places such as stairwells, backyards and basements, are known to be high-risk settings for drug use, both in terms of transmission of infectious diseases, other health risks and overdoses. In Malmö, a significantly larger proportion of participants reported using drugs in such public (33% vs. 21%) and private places (20% vs. 7%), indicating a more precarious risk environment for participants in Malmö than for participants in Copenhagen.
There was no statistically significant difference between the proportion of participants who used drugs at home in the two cities (46% in Malmö and 40% in Copenhagen). Using drugs at home can be both protective and risky. It not only can provide privacy, comfort, safety and better hygiene than outdoors, but also can lack supervision, increasing the risk of fatal overdoses.
Participants were therefore asked whether they used drugs with friends and acquaintances. Here, we saw a small non-significant difference between Malmö (31%) and Copenhagen (24%). Consuming drugs with others can provide support in case of overdoses but can also increase the risk of sharing drug paraphernalia and spreading infectious diseases, particularly if drug-use equipment is not readily available.
Personal Relations and Entrenchment in Drug Scenes
Social relationships and networks are important for understanding the social context of drug use and participation in drug scenes, with the associated risks. They are also important for understanding inclusion in non-drug-related social relations, which can provide protective resources. To investigate this several questions were asked about social and affective relationships. The participants were asked who they spent time with during their everyday lives with multiple response options. No reply could both mean that they did not spend time with anyone or that they did not want to reply. Using a Likert scale, the participants were also asked about to which extent several sentences were correct for them, including: “I have good friends I can trust who do not use drugs” and “I have good friends I can trust who use drugs.”
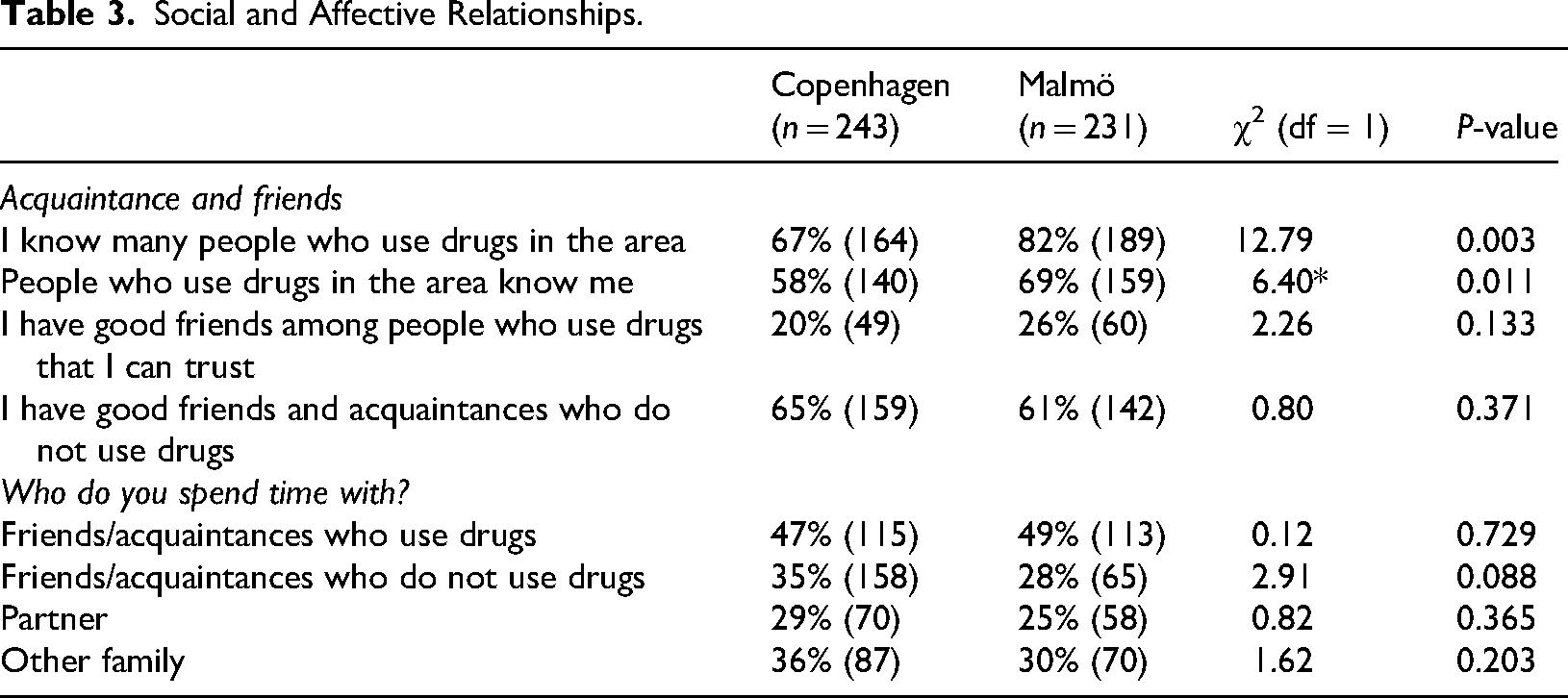
A large proportion of participants from both cities stated that they knew other people who use drugs and that other people who use drugs knew them in the research areas, and it was more common in both cities to spend time with people who used drugs (47% in Copenhagen and 49% in Malmö) than with people who did not use drugs (35% in Copenhagen and 28% in Malmö). This indicates entrenchment in the local drug scene in both cities. However, participants from Malmö appeared to be more entrenched than those from Copenhagen because a significantly larger proportion reported knowing other people who use drugs (82% vs. 67%) and being known by other people who use drugs (69% vs. 58%) in the area. This suggests a denser social network of drug users in Malmö, which can influence norms, behaviors and access to information and resources (Table 3).
Other questions about social relations did not reveal statistically significant differences. In Copenhagen, 20% reported having trustworthy friends who use drugs compared to 26% in Malmö. Additionally, 65% of participants in Copenhagen reported having good friends who do not use drugs compared to 61% in Malmö. These results indicate that a large proportion of participants from both cities had valuable social relationships outside the drug scenes. This may also be reflected in the fact that letting people they care about down was the most frequent everyday concern mentioned by the participants in both cities: 61% in Copenhagen and 58% in Malmö. However, we also found that large proportions of the participants in both Copenhagen (41%) and Malmö (56%) were concerned about loneliness, which could reflect lack of social relations with people who do not use drugs (data not included in Table 6; but see Houborg et al., 2022a). In the qualitative parts of the research project particularly older participants who had reduced or stopped their active participation in the drug scenes expressed loneliness because they found it difficult to establish social relations that were not drug-related (Houborg et al., 2022a).
Study Population.
Places to Consume Drugs.
Persons who had used safe consumption site in Copenhagen.
Social and Affective Relationships.
Access to Formal Resources.
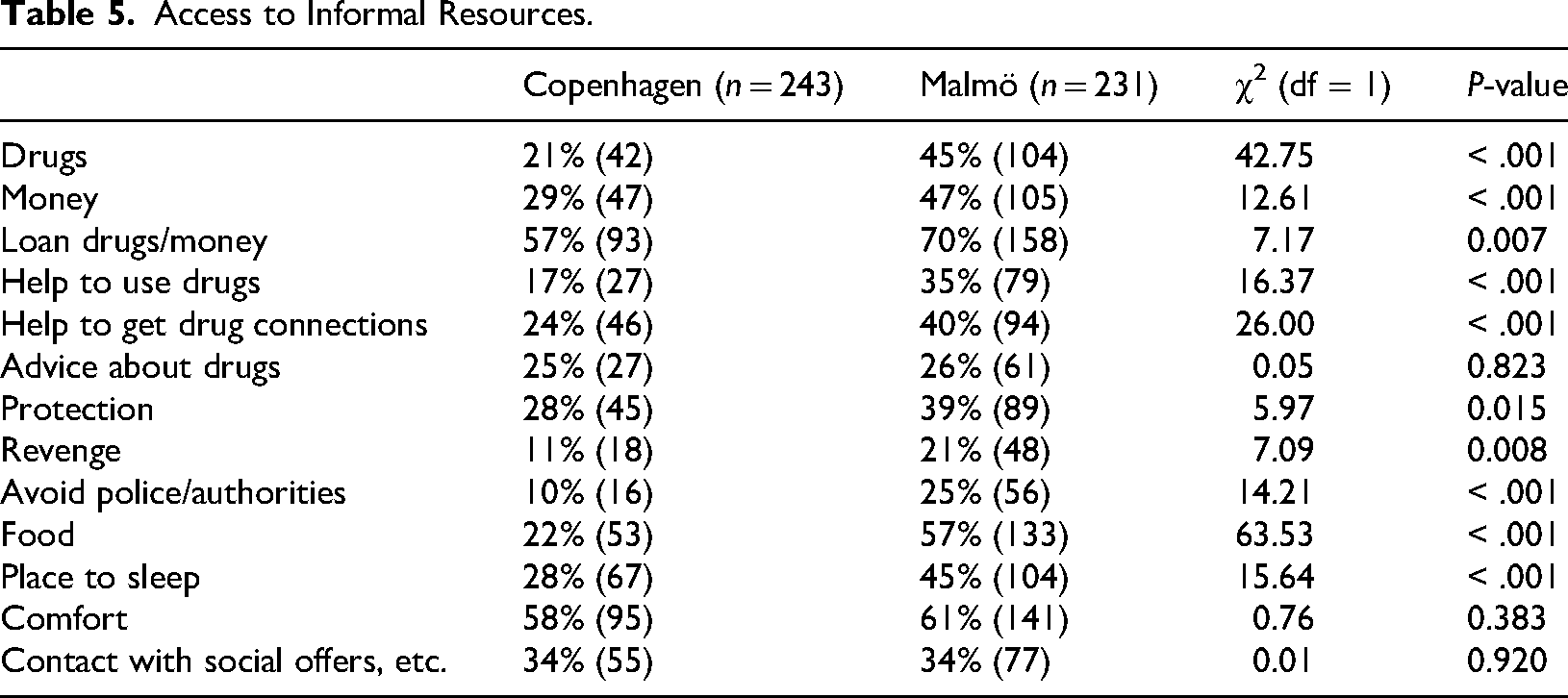
Access to Informal Resources.
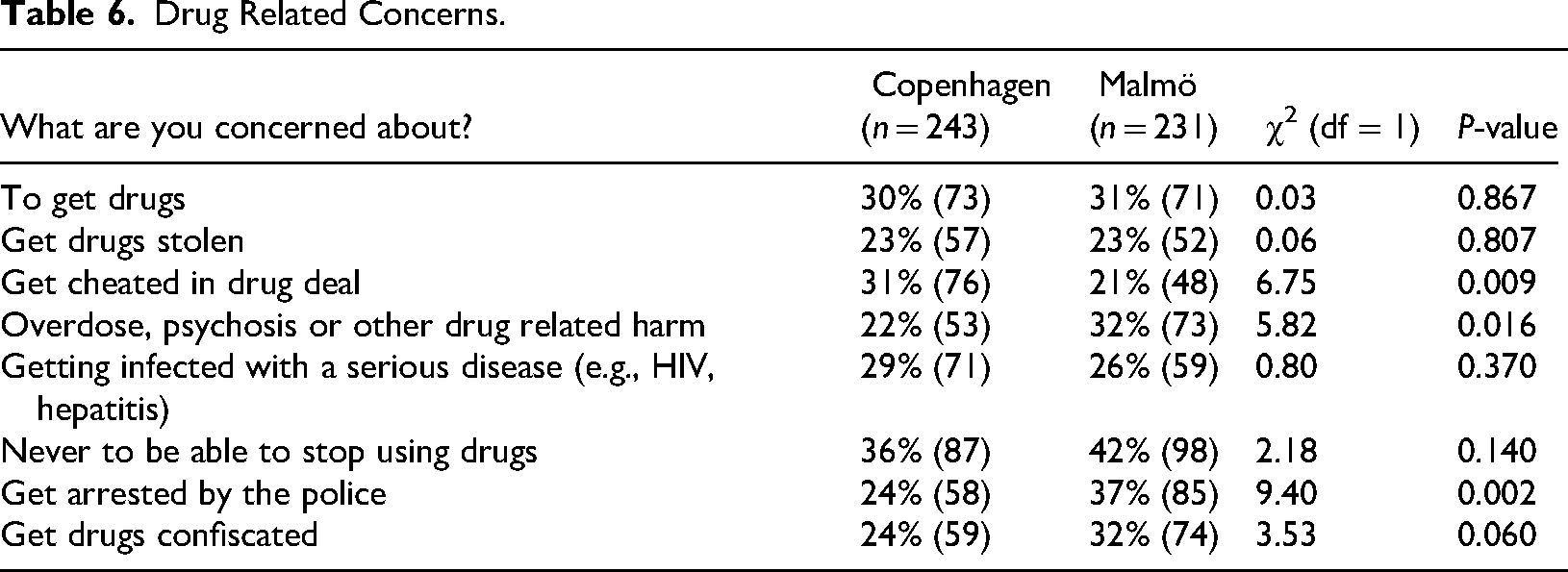
Drug Related Concerns.
Formal and Informal Resources
Both formal resources provided by public or private organizations and informal resources available through social networks can play a crucial role in reducing vulnerability to drug-related and other harms, as well as improving well-being.
Formal Resources
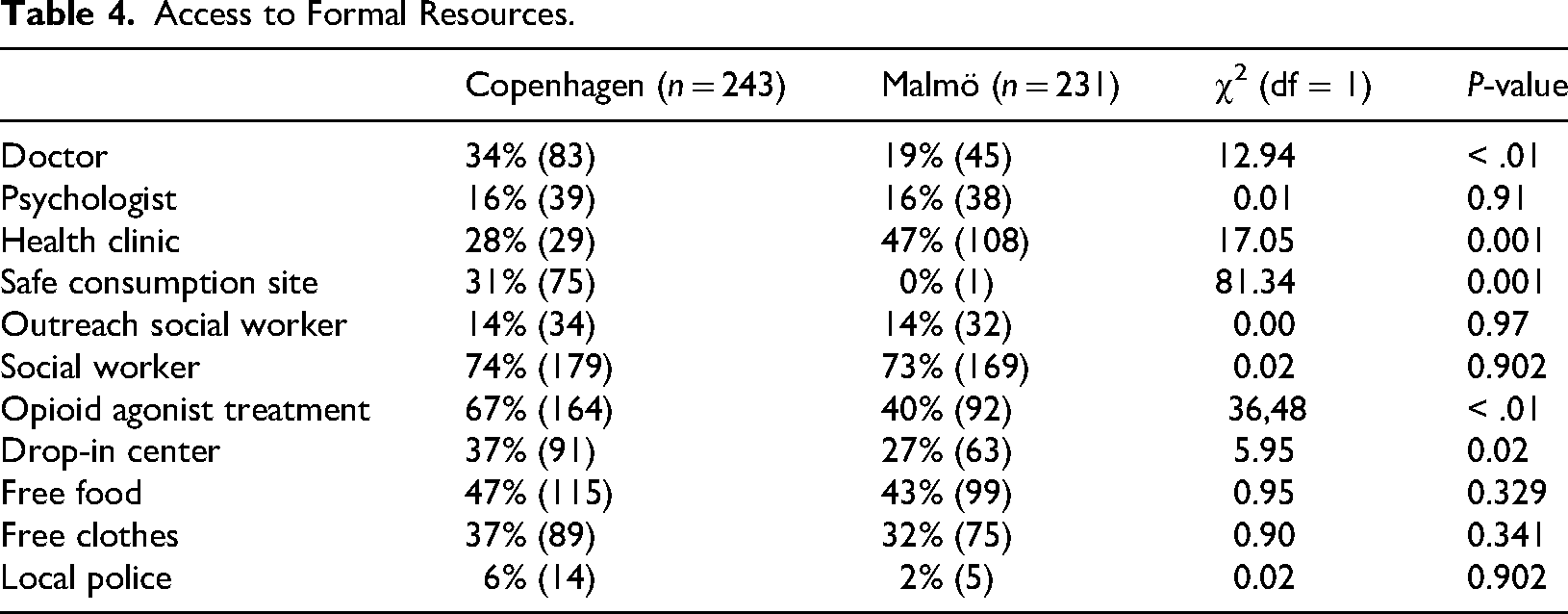
The participants utilize many different types of services available through public and private providers, reflecting the important role of the welfare state in their lives (Table 4). This pattern is evident in both cities, but there are also differences, some of which may relate to drug policy, while others may relate to other factors, such as Copenhagen being a larger city than Malmö.
Healthcare: Looked at separately, there are significant differences in the use of health services such as doctors. These differences likely reflect variations in the institutional landscape and recruitment methods in the two cities. The larger proportion in Copenhagen that visit doctors may reflect that more participants there were recruited at OST centers and their visits to doctors may include regular consultations with doctors there. A larger proportion of participants from Malmö visited health clinics, which may reflect use of the health services at the NEP where a large proportion of the interviews where conducted. In Copenhagen, similar healthcare is available at shelters, drug consumption rooms and drop-in centers. Participants may not consider such places as health clinics but may still use the services they provide. When considering healthcare services together (doctors and health clinics), 62% of participants in Copenhagen and 66% in Malmö used such services. Looked at in that way, the difference in use of health care is minor. What is notable is that so large a proportion in both cities use health services.
Social Workers: Includes professionals who handle social benefits, access to social services, case management, etc., and who may be placed in various public institutions. In both cities, most participants were in contact with social workers, with no significant differences (74% in Copenhagen and 73% in Malmö). This, along with the high proportion of participants who used healthcare services, indicates a high need for care and support and underscores the importance of welfare services and provisions in the participants’ lives.
Opioid Substitution Treatment: The significant differences here, with a larger proportion of participants in Copenhagen undergoing such treatment may reflect lower thresholds of OST in Copenhagen but may also be an artifact of data collection methods (see limitations).
Regarding outreach and support services like free food and clothing, there is no significant difference between participants in the two cities and we see that such services play an important role for participants in both cities.
Drop-in centers can also be an important support for vulnerable people, and here we see a significant difference, with a larger proportion of participants from Copenhagen using such services. This may reflect the institutional landscape in the two cities. In Malmö, the NEP offers comprehensive services, including those of a drop-in center, but there are few alternatives to it. By contrast, Copenhagen has many different low-threshold services, including drop-in centers accessible to structurally vulnerable people who use drugs, just as there exist user-led services.
Overall, participants appear to make extensive use of and have access to a wide range of social and health services, including low-threshold services. The most important difference concerns DCRs, where around one-third had used DCRs in Copenhagen and only one Swedish participant had use one (probably in Copenhagen). This of course shows an important difference in the risk environments of the participants in the two cities and how drug policy affects this environment.
Informal Resources
Informal resources can play a critical role in meeting immediate needs and providing support, particularly if more formal resources are scarce.
In general, participants in Malmö reported receiving more support via private relationships than participants from Copenhagen, particularly regarding drug-related support, such as obtaining drugs, lending money for drugs, assistance with drug consumption and establishing drug connections (Table 5). Malmö participants also relied more heavily on informal support for safety, protection and basic needs such as food and shelter. The only types of informal resources where there was no significant difference were emotional comfort and help in contacting social services. The similarities in terms of informal affective resources (i.e., support and backing) also show up regarding who the participants experience as supportive in their lives. Family members, social workers and friends who did not use drugs were the three groups most participants in both cities reported as important supports in their lives. However, a significantly larger proportion in Copenhagen stated that doctors and social workers were important supports compared to Malmö.
Drug-related Concerns
The participants were asked a series of questions about everyday concerns relating to things like drugs, health, basic needs, social relations, and mental health. Here, we focus on drug-related concerns because they may relate to the different drug policies in the two countries (Table 6).
There were no significant differences in concerns about obtaining drugs or having drugs stolen. However, there was a significant difference regarding being cheated in a drug deal, with a larger proportion of participants in Copenhagen being concerned regarding this. This difference may reflect a different type of drug market in Copenhagen that is less influenced by a moral economy (Bourgois & Schonberg, 2009) and more by market transactions between people who do not have a personal relationship with each other (Houborg & Holt, 2018).
The only concerns where the two populations significantly differed were regarding overdoses, psychosis, or other drug-related harm, with a larger proportion of participants from Malmö being concerned.
Finally, we asked about legal concerns relating to drug control. Here, a significantly larger proportion of participants in Malmö were worried both about being arrested by the police and about having their drugs confiscated. This reflects a higher perceived risk of legal consequences in Malmö, likely related to Sweden's stricter drug control policy and police priorities.
Discussion
The findings from this exploratory study suggest a possible interplay between drug policy and the Nordic welfare state in shaping the risk environments and everyday lives of structurally vulnerable people who use drugs in Copenhagen and Malmö. However, due to the study's sample limitations and methodological constraints, such interpretations should be considered as indicative rather than conclusive. Despite differences, Denmark and Sweden both represent a type of dual track welfare state approach to drug use, in which both harm reduction and crime control approaches are extensive, in tandem with traditional drug treatment. This approach has also characterized drug policy in Finland and Norway (Hakkarainen et al., 2007; Tham, 2021; Larsson, 2021), in their attempts to balance public health and public order. While people who use drugs in both Malmö and Copenhagen benefit from comprehensive welfare systems that provide essential social and health services, the divergent drug policies of Denmark and Sweden create distinct risk environments that significantly impact the experiences and vulnerabilities of people who use drugs. This was reflected in the results.
The Nordic Welfare State: Addressing Structural Vulnerability
At a broad level, participants in the two cities shared many similarities, particularly in risks and vulnerabilities linked to a drug-related lifestyles and in their extensive use of support from the welfare state. As discussed earlier, socioeconomic conditions and social provisions play a pivotal role in producing and averting structural vulnerability to drug related harm (Stevens, 2011; Currie, 1994; Bourgois, 2003). The participants in our study are among the most vulnerable in the Danish and Swedish societies suffering from a host of different harms caused by the interplay between their structural position and their use of drugs. However, in our study, we have also seen that the Nordic welfare state plays a crucial role in addressing the vulnerability of people who use drugs in both cities. The comprehensive social and health services available in Denmark and Sweden ensure that people with lived experience of substance use who are structurally and socially vulnerable have access to essential resources, including healthcare, social benefits, social support and low-threshold services. This welfare provision is vital in mitigating the economic and social risks associated with drug use, as evidenced by the high utilization of formal resources by participants in both cities. However, the study also reveals that structural vulnerabilities persist, particularly in terms of housing instability and economic precariousness. The welfare state's role in providing supportive housing and financial assistance is essential but not sufficient to fully address these vulnerabilities. The reliance on informal resources, especially in Malmö, suggests that formal services do not fully meet the needs of people who use drugs, highlighting the importance of both formal and informal support systems.
The Role of Drug Policy in Structuring Risk Environments
Drug policy can play a critical role by supplementing or contradicting wider policies that distribute risks and resources in society (Benoît, 2003). We have seen in this study that drug policy may be an important factor influencing access to harm reduction services and shaping risk environments in Copenhagen and Malmö. However, other contextual elements, such as differences in service infrastructures and cultures of care, may also contribute. Denmark's more liberal and harm reduction-oriented drug policy is evident in the greater availability and utilization of harm reduction services, including DCRs and HAT. This policy environment can reduce certain drug-related risks and could be one explanation for lower concerns about overdoses and drug-related harm among participants in Copenhagen. By contrast, the risk environment in Malmö seems more precarious, with higher reliance on informal resources and greater concerns about some forms of drug-related harm. At the same time, there were also similarities in concerns about contracting serious infections, having their drugs stolen, and not being able to stop using drugs, which indicates that many aspects of vulnerability may be common to people who use drugs across different policy contexts. Participants in Malmö were more concerned about legal consequences, reflecting Sweden's stricter drug control policies. It is well-documented that punitive policing is an important contributor to drug-related harm (Cooper et al., 2005; Friedman et al., 2006; Maher & Dixon, 1999; McNeil et al., 2015). Although police officers in Malmö have expressed that they support non-punitive approaches towards people with lived experience of substance use who are structurally and socially vulnerable (Richert & Nordgren, 2025), such discretionary attitudes among individual officers may not make up for more systemic repression under a punitive drug policy. In Denmark, a policy of decriminalization towards economically disadvantaged people who are dependent on other drugs than cannabis exists and, in Copenhagen, a harm reduction policy has been implemented (Houborg et al., 2014; Houborg & Møller, 2021), reducing the contribution of law enforcement to the risk-environment. However, despite this policy, some people who use drugs are still sceptical towards the police (Kammersgaard et al., 2024). The differences in drug consumption settings further highlight the impact of drug policy. One aspect of the enabling environment is the availability of DCRs in Copenhagen that can provide a safer environment for drug use, reducing the need to consume drugs in high-risk public spaces. In Malmö, the lack of such facilities may be one reason for to the high rates of drug use in public places and private properties, increasing the risk of health complications and overdoses (Rhodes et al., 2006; Ickowicz et al., 2017; Small et al., 2007). This disparity underscores the importance of harm reduction measures in creating safer environments for people with lived experience of substance use.
Social Relations and Entrenchment in Drug Scenes
The social networks and relationships of people who use drugs in Copenhagen and Malmö provide insights into their entrenchment in drug scenes and access to supportive resources. Overall, there were great similarities in social relations between the participants in the two cities. In both cities, the participants mainly socialized with other people who used drugs, while a majority also had good friends or acquaintances who did not use drugs. However, participants in Malmö appear to be more embedded in the local drug scene, knowing more people who use drugs, and being more reliant on support and protection from peers. This reliance on support from peers may help to manage a difficult life situation in the short term, and can also be a sign of community care within the local drug scene. Yet, it can also lead to a hardening of marginalization (Coumans et al., 2006) and entrenchment in the drug scene (Fast et al., 2009), which, in the long term, can reduce the possibility of reversing processes of marginalization and hinder social inclusion. Entrenchment in the drug scene can also increase the risk of sharing drug paraphernalia and spreading infectious diseases (Lovell, 2002; Prithwish et al., 2007). The strong reliance on informal support for participants in Malmö may also relate to less access to low-threshold or user led harm reduction services in comparison to participants in Copenhagen. The differences in social relations and entrenchment highlight the need for drug policies that address both the structural and social dimensions of drug-related harm, including the role that drug control policy can play in increasing harm (Rhodes, 2002; Burris et al., 2004; Bourgois & Schonberg, 2009).
Limitations
While this study provides valuable insights into the lives, resources and risk environments of structurally and socially vulnerable people who use drugs in Copenhagen and Malmö, several limitations must be acknowledged. First, the study is based on non-representative samples recruited through opportunistic sampling at selected services. This means that the findings cannot be generalized to all people who use drugs in the two cities or the two countries.
Second, although we used the same questionnaire and similar types of recruitment sites, there are differences in the institutional settings where the participants were interviewed. In Copenhagen, more participants were recruited through OST centers, whereas in Malmö, a larger share were recruited at the NEP. These differences in recruitment places may have influenced the observed patterns, particularly those related to service access and treatment. However, importantly, OST in Copenhagen is low-threshold where people are not excluded if they use illegal drugs and many of the participants in OST continue to use illegal drugs (Houborg et al., 2022b). Comparing the groups in the two cities with regards to background factors, we see that they are very similar in terms of background factors, which could also reduce possible problems with differences in recruitment places.
Third, the analyses are limited to descriptive statistics and basic group comparisons. We did not perform multivariate or regression analyses that could allow us to control for potentially confounding variables such as age, gender, housing status or type of service where recruitment took place. As such, we cannot clearly establish whether the observed differences are driven by policy context or by other underlying factors.
Finally, many of the observed differences were small in magnitude or not statistically significant, and some comparisons may be affected by limited statistical power due to the sample size. These limitations emphasize the exploratory nature of the study. The findings should therefore be interpreted as indicative patterns that warrant further investigation.
Conclusions
The present study underscores the complex interplay between drug policy and the Nordic welfare state in shaping the risk environments and everyday lives of structurally vulnerable people who use drugs in Copenhagen and Malmö. While the welfare state provides a critical safety net, drug policy plays a pivotal role in determining access to harm reduction services and structuring the overall risk environment. The findings point to the potential importance of tailored interventions that address both the structural and social dimensions of drug-related harm, ensuring that people who use drugs have access to the resources and support they need to mitigate risks and improve their well-being. Availability of harm reduction services and reducing negative consequences of punitive law enforcement is crucial in this regard. Moreover, the study highlights a trend toward convergence in the drug policies of Denmark and Sweden. Over recent decades, Denmark's drug control policy has become more restrictive, while Sweden has gradually adopted more harm reduction measures. There are however still significant differences. Denmark has accompanied a zero-tolerance policy with a policy that decriminalizes economically disadvantaged people who use drugs. Sweden, on the other hand, retains its strict drug control policy that includes criminalization of drug use, including of structurally and socially vulnerable people who use drugs. The tendency towards convergence suggests that the differences between the two countries’ drug policies are no longer as wide as an ocean but the persisting differences also means that they are not yet as narrow as a strait.
Footnotes
Funding
The authors disclosed receipt of the following financial support for the research, authorship and/or publication of this article: This work was supported by the Velux Fonden (grant number 18116).
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Correction (October 2025):
Article updated to correct the participants' proportions for Copenhagen (from 61% to 41%) and Malmö (from 58% to 56%) in the section “Personal Relations and Entrenchment in Drug Scenes”.