
Abstract
Keywords
Introduction
Recovery
Consensus on the meaning of recovery has not been fully reached in spite of many attempts to define recovery from substance use disorders (SUD) (Ashford et al. 2019; Inanlou et al. 2020). The definition of recovery and its outcomes measures vary significantly, with discussions emphasizing that merely achieving abstinence does not automatically align with improvements in areas such as criminal behaviour, health, employment, income or stable housing (Bacchus et al., 2000; Maddux & Desmond, 1986). The latest UK Drugs Strategy “From harm to hope” (UK Government, 2022) sees recovery as a process over time which required efforts to maintain and broadened access to meaningful activities, housing and a support system within the community. The key consensus areas around recovery are that it is (1) a process of (2) stopping, reducing or gaining control over substance use, at the same time as (3) making positive changes, with a goal to enhance health and wellbeing, and (4) fostering an environment conducive to increased community activism and citizenship (Ashford et al., 2019; Betty Ford Institute Consensus Group, 2007; Dekkers et al., 2020; Sheedy & Whitter, 2009; UK Drug Policy Commission, 2008).
Recovery as a process over time
Recognizing recovery as a process underscores the understanding that overcoming SUDs extends beyond a singular moment, with the initiation and the continued sustaining of recovery seen as different phases, each with its unique characteristics (Humphreys et al., 1995; Snow et al., 1994). The Betty Ford Institute Consensus Panel (2007) has indentified three distinct recovery stages: early (<1 year), sustained (1–5 years) and stable recovery (>5 years), after which a person reaches a point where the risk of relapse plateaus (Best et al., 2010). This progression aligns with findings from longitudinal research conducted by Dennis et al. (2014), who asserted that, until this juncture, individuals often require external support to sustain their recovery. Additionally, the Harvard Grant Study on alcoholism (Vaillant, 2003, 2012) and a 33-year follow-up study on heroin addiction (Hser, 2007), suggest that a 5-year period of abstinence markedly increases the chances of stable recovery. It is noteworthy that the majority of individuals can and ultimately do achieve recovery (Kelly et al., 2017; Sheedy & Whitter, 2009; White, 2012). At the same time, research indicates that addiction careers are often long and complex, lasting an average of 28 years and involving four to five treatment episodes over approximately 8 years (Dennis et al., 2007). These findings highlight that, although recovery is achievable, it is frequently a prolonged and non-linear process.
Meaningful activities and well-being
Recovery research has evidenced that well-being and quality of life of individuals in recovery are significantly influenced by social connections and active engagement in meaningful activities. Dame Carol Black's review of the evidence for the UK Government (Black, 2016) emphasized that, in addition to treatment, engaging in meaningful activities plays a significant role in maintaining recovery. There is substantial evidence that employment can enhance quality of life (Eddie et al., 2020), improve treatment results, diminish both the frequency and intensity of relapses, and build recovery capital (Laudet & White, 2010; Lynch et al., 2022; Manuel et al., 2017).
Leamy et al. (2011) introduced the CHIME framework (Connectedness, Hope, Identity, Meaning, Empowerment), claiming that it is essential for supporting mental health recovery. Best et al. (2012) also reflected this sentiment in the context of addiction recovery, asserting that positive Connections instill a sense of Hope, reinforcing the belief that change is attainable. Hope serves as a catalyst of change which inspires people to engage in Meaningful activities that foster a positive Identity and culminates in an internal sense of Empowerment. Studies in Birmingham and Glasgow by Best et al. (2011) found that spending time with others in recovery and engaging in meaningful activities, including child care, group involvement, volunteering, education, training and employment, significantly improves well-being, and correlates with improved outcomes in recovery. A 2013 follow-up study (Best et al., 2013) further established a direct link and correlation between engagement in meaningful activities and improvements in quality of life and well-being measures. Challenging the idea that well-being improvement must precede the initiation of meaningful activities, they reported that, on the contrary, continuous engagement in meaningful activities significantly enhances well-being of participants. They also found that stopping these activities over the course of 1 year caused their well-being to decline.
Meaningful activities are closely linked with the idea of citizenship and its critical role in the recovery process, highlighted in recovery definitions. This is particularly significant as addiction frequently results in individuals losing their sense of connection and commitment towards their community. That disconnection can manifest as a withdrawal of personal contributions to community life or, in some cases, as a danger or direct harm to the community and its members, and is linked to legal status, education, employment, community participation and volunteering. White et al. (2010) have created an extensive list of examples of the “Core Acts of Citizenship in Recovery”, and claim that recovery-grounded values can inform daily activities in family (e.g., Engaging in family rituals and activities), social (e.g., Joining social support groups), economic (Pursuing employment or educational development), and political participation (e.g., Public speaking about recovery), as well as shared life meaning and purpose (Being part of or engaging in spiritual, religious or community service work). This is also linked with the notion of community recovery capital.
Recovery capital, Life in Recovery (LiR) survey and Strengths And Barriers Recovery Scale (SABRS)
Recognizing the significance of societal responses, the concept of ‘recovery capital’ has emerged in past decades and assumes a pivotal role in understanding the dynamics of recovery from substance use disorders (Best & Laudet, 2010; Cloud & Granfield, 2008; Granfield & Cloud, 2001). It includes a spectrum of resources available and instrumental for initiating, maintaining, and sustaining recovery (Cloud & Granfield, 2008). The crucial role of recovery capital is emphasized by its strong connection to the severity of the issue and the overall process of recovery (Best & Laudet, 2010; Hennessy, 2017; White & Cloud, 2008). The dimensions of recovery capital have been classified as:
Personal Recovery Capital (qualities and skills such as communication skills and resilience) Social Recovery Capital (positive social support and networks) Community Recovery Capital (available and accessible resources in the community, such as employment and education),
Recovery capital provides a comprehensive framework for evaluating the multifaceted resources contributing to the recovery journey (Best & Laudet, 2010; White & Cloud, 2008). Furthermore, a paradigm shift towards acknowledging and utilizing community recovery capital underlines the significance of a broad spectrum of community resources. It also encompasses, among other peer-delivered interventions, mutual aid groups, and a variety of community engagement opportunities, such as volunteering, which can be instrumental in initiating and sustaining recovery. Humphreys and Lembke (2014) supported this idea and highlighted the strong evidence base for these interventions, alongside the assertion of Evans et al. (2013) that community recovery transcends the personal recovery of its members by fostering connections and enhancing the quality of community life. This facilitates access to community resources, thereby expanding individuals’ capacities to forge positive networks and build social capital (Best & Savic, 2015; Putnam, 2000). Research indicates that Peer-Based Recovery Support Services are beneficial for individuals by effectively reducing alcohol and drug use, lowering relapse rates, enhancing engagement and satisfaction with treatment, securing stable housing, and increasing recovery capital (Bassuk et al., 2016; Eddie et al., 2019). However, the accumulation of recovery capital does not follow a straightforward or consistently positive trajectory (Cano et al., 2017; Kaskutas et al., 2009). Cloud and Granfield (2008) emphasized that recovery capital includes not only positive resources that support recovery, but also negative elements, often referred to as “recovery barriers” or “negative recovery capital”, which can undermine progress. These include factors such as stigma, untreated mental health issues, unstable housing, poverty and lack of social support, all of which may actively hinder an individual's ability to sustain long-term recovery. Factors such as (female) gender or incarceration have been identified as impediments to the recovery process (Cloud and Granfield, 2008).
Understanding the dynamics of recovery is connected with recognizing the role and influence of gender and the significance of societal responses. Gender's relevance extends beyond its impact on the initiation of substance use, addiction onset and treatment engagement, and plays a pivotal role in shaping post-treatment outcomes and the recovery journey (Grella et al., 2008). Despite these findings, there remains a scarcity of research pinpointing specific features of recovery capital that exhibit marked gender differences across settings and recovery journeys. A significant gender disparity underscores the existence of unique barriers that women encounter in accessing treatment, such as specific needs related to mental health and care giving responsibilities, compared to men who have disclosed greater unmet needs concerning physical health (Andersson et al., 2021; Public Health England, 2020; Schamp et al., 2021).
The Life in Recovery (LiR) surveys offer illuminating findings on the transformative impact of recovery and advancements across various life domains of people in recovery highlight the potential positive effects of transitioning from active addiction to recovery. The impact of the LiR survey, initially conducted in the USA (Laudet, 2013), extended beyond the USA, first in Australia (Best, 2015), followed by the UK (Best et al., 2015), Canada (McQuaid et al., 2017) and Belgium, The Netherlands, Scotland and England (Best et al., 2019). The last wave was supplemented with nine additional European countries which further contributed to the growing body of international research. It involved 44 items which encompassed five core domains: health, work, finances, legal and criminal justice, and social and family dynamics, and covered two time windows: once to capture experiences during the phase of “active addiction” and again to assess changes “since entering recovery”. Despite overall similar patterns of improvement across the five domains, each country exhibited unique differences in participant characteristics and the specific social and cultural contexts surrounding recovery (Best et al., 2015, 2018).
The work on the European dataset has also resulted in the creation of Strengths And Barriers Recovery Scale (SABRS; Best et al., 2020) from the Life In Recovery instrument to create composite scoring with the goal of assessing positive and negative recovery capital in individuals with addiction and those in recovery, resulting in a score for total Recovery Strengths and total Recovery Barriers for both Active Addiction and in Recovery. The SABRS scale revealed an intriguing shift in the dynamics of reported recovery strengths between males and females. This demonstrated significantly more recovery strengths during active addiction among males, and a reversal and greater growth in strengths from addiction to recovery for females (Best et al., 2020). In a related study (Best et al., 2021), the significance of the association between living with dependent children and increased gains in recovery capital was found to be more pronounced in females than males, underscoring noteworthy gender differences in the recovery trajectory.
In Sweden, the concept of Recovery Capital and its practical and theoretical applications have gained recognition (Skogens and von Greiff, 2016; Skogens et al., 2017; Topor et al., 2018). These studies suggest that an recovery capital based assessment tool could be effectively integrated into Swedish treatment settings, reflecting successful applications in various other countries (Best et al., 2016; Burns and Marks, 2013; Groshkova et al., 2013). The capacity of recovery capital to pinpoint key elements of a person's recovery journey, identifying both obstacles and strengths, aligns with the fundamental principles of evidence-based practice, particularly the growing requirement for documentation and evaluation. The National Board of Health and Welfare (NBHW) in Sweden emphasizes the need for assessment tools to comprehend and meet client treatment requirements, analyze outcomes, bolster client relationships, and motivate change through progress tracking (NBHW, 2019). Furthermore, there is an increasing need for detailed documentation within social work agencies (Björk, 2017). In response, the NBHW has been proactive in advocating for the adoption of such tools in social work, especially within agencies dealing with alcohol and other drugs treatment (NBHW, 2019).
Although existing studies provide a broad view of and evidence for recovery, the current research delves into the experience of the recovery community in Sweden, a non-English-speaking country under-represented in recovery research. By focusing on Sweden, we contribute to a more global understanding of recovery, challenging the applicability of findings and key recovery ingredients from Anglophone world to different cultural and social settings. This setting allows us to examine how societal infrastructure supports individuals in recovery to engage in both meaningful and activities and determine whether that is influenced by gender and time in recovery. The present study adopts a broad definition of recovery as a process of making positive changes and achieving well-being through community engagement and citizenship over time (Betty Ford Institute Consensus, 2007; UK Government, 2022). To test this, the present study specifically aims to:
Investigate gender differences in recovery capital the recovery population in Sweden; Explore the impact of time in recovery on engagement in meaningful activities among the recovery population in Sweden; and Assess whether harmful activities decrease over time in recovery. We hypothesize that time in recovery significantly predicts community engagement and prevalence of meaningful activities among recovering population, and decrease in activities with detrimental effects, with notable differences between genders.
Methods
Instrument
Our analysis is framed by the concepts of recovery outlined above. Our LIR study builds on an already established research methodology (Best, 2015; Best et al., 2015; Laudet, 2013; McQuaid et al., 2017, McQuaid & Dell, 2018). The LIR scale assesses self-reported experiences in both active addiction and in recovery in five domains: health, work, finances, legal and criminal justice, and social and family dynamics. The same questions are asked for two time windows covering “in active addiction” and “since entering recovery”.
The LIR survey served as the primary data collection instrument in this study. It includes items covering five domains: health, legal, finances, employment and social/family life, each measured both during active addiction and in recovery. From this survey, the SABRS was developed (Best et al., 2020) to quantitatively assess changes in recovery capital across stages of recovery. The SABRS includes a range of recovery “strengths” (e.g., engaging in meaningful activities, volunteering, improved physical health) and “barriers” (e.g., homelessness, involvement in crime, untreated mental health issues).
In the present study, we used two approaches to present change data. First, we calculated an overall SABRS change score based on the total number of strengths and barriers reported during active addiction and in recovery. Second, we analyzed a subset of SABRS items focused on meaningful and detrimental activities, selected for their particular relevance to gendered aspects of recovery and comparability across groups. These items were drawn directly from the SABRS but were reported separately to explore specific dimensions of recovery experience. The rationale for this selective analysis was to focus on activities most associated with social integration, mental health and personal growth, which have been shown to differ by gender in previous studies (Best et al., 2021).
A slightly adapted version of the instrument was circulated through Swedish networks. The LiR instrument was supplemented with some additional measures: lifetime treatment for mental health disorders, Adverse Childhood Experience scale (Wingenfeld et al., 2011) and stigma scales (which will not be discussed here).
Finally, we created a composite score of overall “SABRS Change”, calculated as increase in strengths minus reduction in barriers, which has not previously been used as a metric (Best et al., 2020).
Recruitment
Recruitment was conducted through social media, key recovery agencies and treatment services (a range of residential and outpatient institutions, community treatment providers, recovery groups, therapeutic communities, communes and institutions providing various supports to people affected by drugs and those in recovery across Sweden), and through word-of-mouth (we actively encouraged a snowballing approach). Additionally, people in recovery played a critical role in the distribution of the survey and circulated the survey amongst family members, friends and other individuals in recovery amongst their networks (to boost ‘snowball sampling’) providing information about the study and the link to the screening questionnaire.
The surveys were completed by individuals who were ≥18 years old, in self-reported recovery for ≥3 months, irrespective of how they understand recovery and what stage they are at on this journey.
Procedure
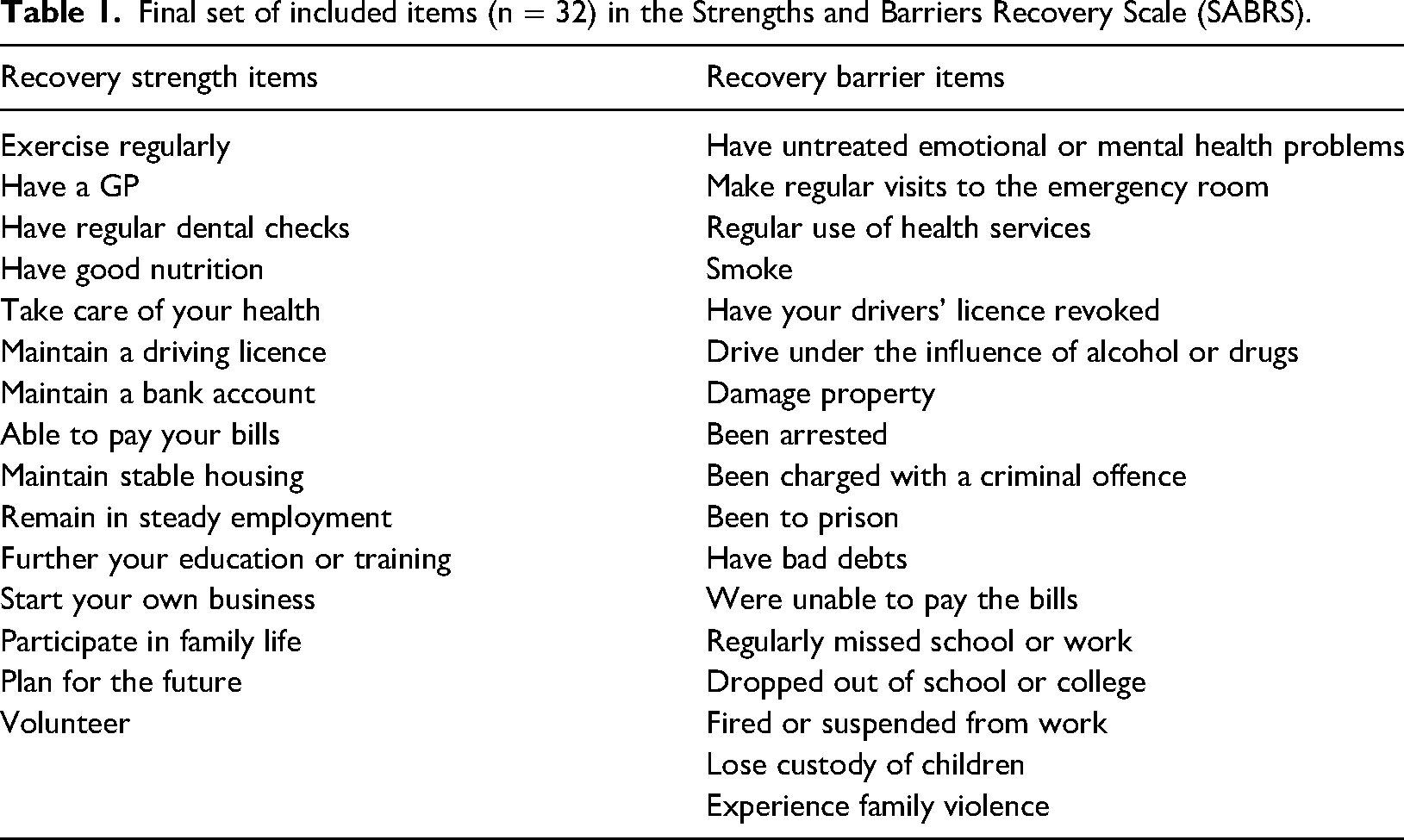
The survey has been translated into the Swedish language following a process of back-translation to ensure both consistency and that it was meaningful to potential participants. It ran between 30 September 2022 and 1 June 2023. The survey was available online and it was promoted via recovery and treatment organizations, social media, websites and other partner agencies. The aim (as with other LiR surveys) was to start from known recovery groups and then snowball out to a more diverse group of potential participants. The survey collected a range of background information, including participants’ age, gender, employment status, living situation and mental health history. In addition, respondents were asked about the types of substances they had used problematically and for which respondents reported a range of substances for which they had sought help. The most common were amphetamines (24.8%), followed by alcohol (19.3%), heroin (22.0%), cocaine (9.2%), cannabis (5.5%) and prescription drugs (4.6%). A notable 11.9% reported polydrug use as their primary problem substance, whereas no participants listed crack cocaine as their main issue. The rationale for the LiR is based on a series of indicators that the participant endorses for two different stages of their life – as they are currently (“in recovery”) and at the peak of their substance use (“in active addiction”) in five domains: Health, Legal, Finances, Employment, and Social and Family Dynamics, enabling us to observe the change in life domains as individuals progressed from addiction to recovery. Additional clarification of the key variables included in analyses is in Table 1.
Final set of included items (n = 32) in the Strengths and Barriers Recovery Scale (SABRS).
Analysis
The survey data underwent processing and analysis using SPSS (IBM Corp.). First, we provide sample characteristics grouped by gender. Analyses were performed for meaningful activities and participation in detrimental activities which can pose barriers to recovery, in addiction by gender, and in recovery by both gender and stage: early (<1 year), sustained (1–5 years) and stable recovery (>5 years) (Betty Ford Institute Consensus Group, 2007). Chi-squared tests, Independent sample t-tests, one-way analyses of variance and Spearman's rho tests were performed to test differences in sample characteristics. The SABRS scale (Best et al., 2020) was then used to estimate change score in overall recovery wellbeing.
Results
Sample characteristics by gender
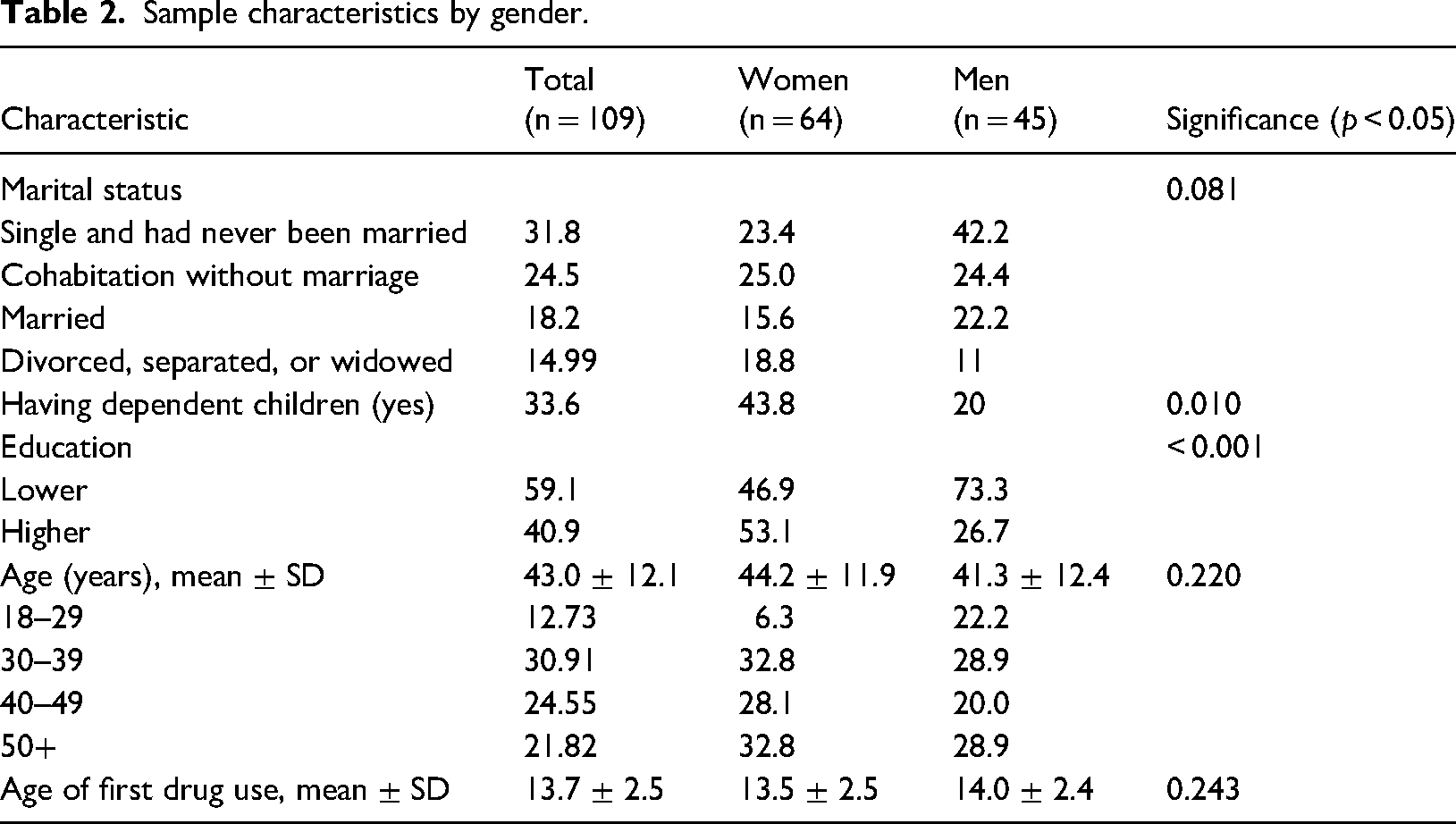
The sample comprised 110 individuals, 58.2% of whom were female, one person self-identified as “queer” and was excluded from the analysis. Women were significantly more educated (53.1/26.7%, p < 0.001), less likely to be single (23.4%/42.2%) or married (15.6%/22.2%), but reported having significantly more dependent children (43.8%/20%, p = 0.027) than men.
The mean ± SD age of the participants was 42.8 ± 12.2 years (range = 18–77 years), with more women being in the 30–39 years and ≥50 years age groups (32.8%/28.9%, p = 0.055) than men. Participants typically started using any drug between the age of 12 and 16 years of age. The demographic characteristics of the sample, split by gender, are provided in Table 2.
Sample characteristics by gender.
Recovery status, recovery stage and life-time help seeking
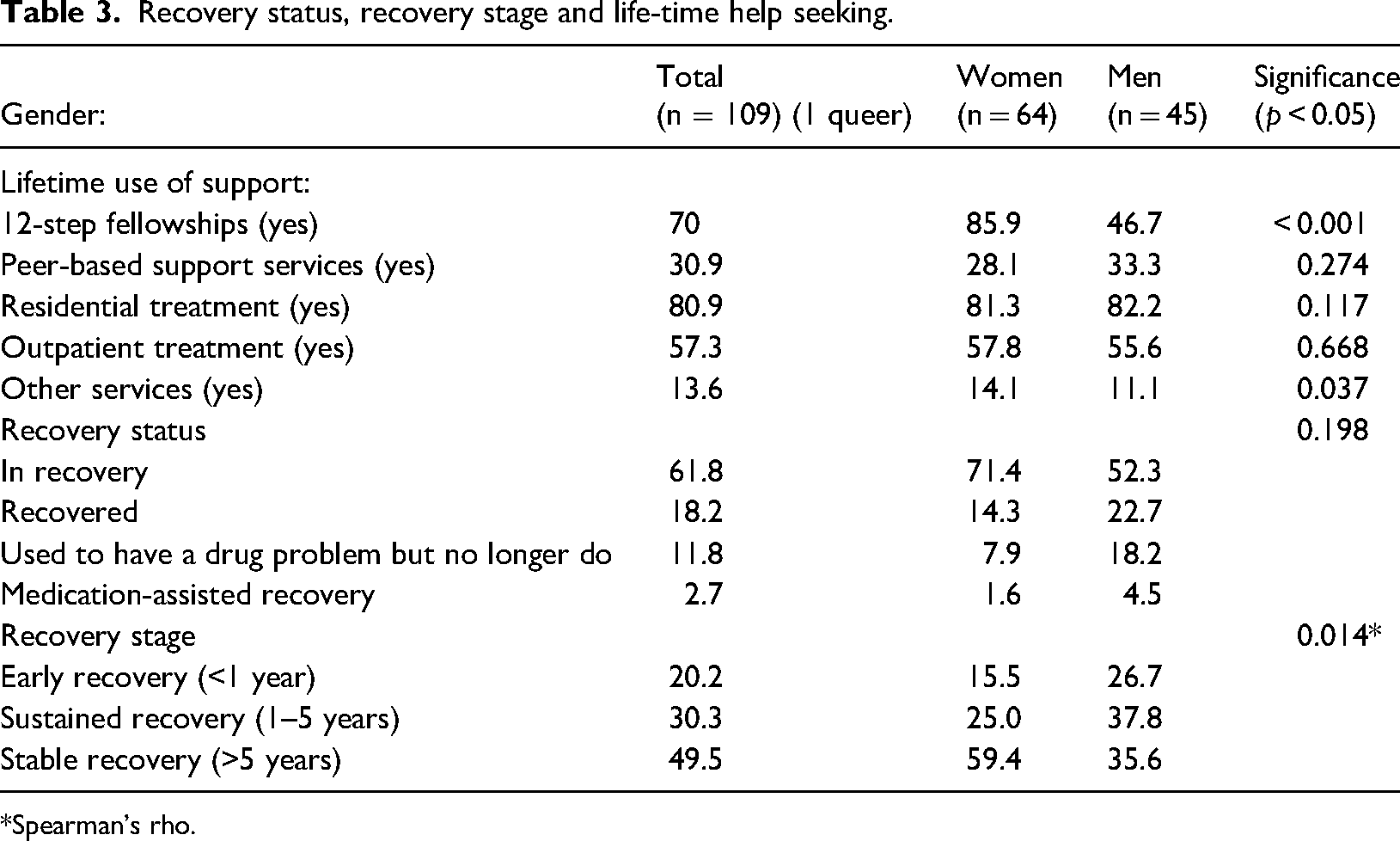
Reported lifetime 12-step fellowship participation (85.9%/46.7%, p < 0.001) and the use of other support services like churches were significantly higher among women than men (14.1%/11.1%, p = 0.037) (Table 3). Utilization of other examined support services was similar across both genders. As part of the survey, participants were asked to self-identify their recovery status by choosing from one of four categories: (1) Medically Assisted Recovery (MAR), (2) In recovery, (3) Recovered and (4) Used to have a drug or alcohol problem but no longer do. These categories were not predefined or explained in the survey but were instead based on participants’ own interpretations of their recovery journey. “In recovery” typically reflects an active engagement in the recovery process, often involving support groups or treatment. “Recovered” may indicate a sense of having completed that journey and no longer needing active support. The category “Used to have a drug or alcohol problem but no longer do” may be chosen by individuals who do not identify with the recovery movement or who view their substance use problems as resolved without formal recovery processes. The MAR category refers to those currently using medication (e.g., methadone or buprenorphine) as part of their recovery strategy. These distinctions, although self-defined, provide insight into participants’ perceptions of their recovery status and allow for exploratory analysis across different identity-based recovery pathways. The largest proportion of both genders saw themselves as being “in recovery”, with a smaller percentage identifying themselves as being in medication-assisted recovery. Significant differences (p = 0.049) were found between recovery stages, with the largest proportion of female participants in “stable recovery” (49.4%/35.6%), whereas more male participants were in “sustained recovery” (respectively 25% and 37.8%). A relatively larger proportion of persons in “early recovery” (26.7%) was among male participants (15.5%).
Recovery status, recovery stage and life-time help seeking.
Spearman's rho.
Meaningful and detrimental activities in active addiction and recovery
The LiR survey asked participants about a series of meaningful activities (positive)and activities that could be regarded as harmful to the individual, family or community, first during the period of their addiction and again as they experience them at the time of completing the survey. The transition from addiction to recovery is marked by a notable increase in engagement with meaningful activities across all categories and a significant decrease in detrimental behaviours, illustrating the profound positive impact of recovery on individuals (Table 4).
Meaningful and detrimental activities in active addiction and recovery.
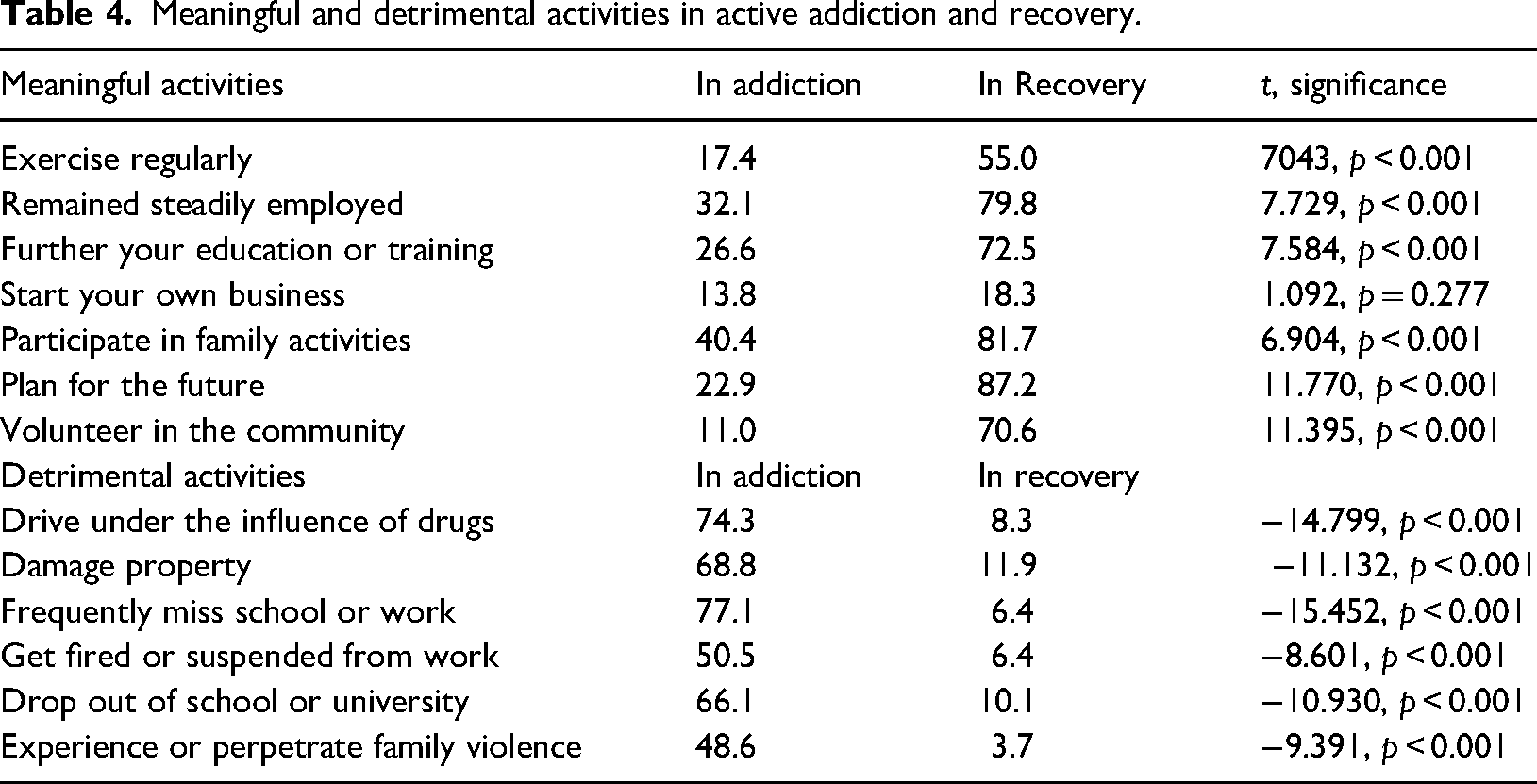
During active addiction, the highest rates of meaningful activities were reported for steady employment and participation in family activities across both genders. Although gender differences did not reach significance, males reported more engagement in every investigated meaningful activity when they were in addiction. In addition, males reported significantly higher rates of driving under the influence of drugs (84.4%/67.2%), whereas experiencing family violence was more commonly reported by females (60.9%/31.1%).
Further analysis was performed to determine the impact of time in recovery on engagement in meaningful activities and assess how their engagement in detrimental activities decreases over time.
Meaningful activities
Although some trends remain the same among both genders, the time in recovery for females was associated with increase in exercising more (20.0% in early, 50% in sustained, to 63.2% in stable recovery), more participation in family activities (60.0% in early, 93.8% in sustained and 92.1% in stable recovery), and planning for the future (70.0% in early, 100% in sustained and 94.7% in stable recovery), whereas these activities have not significantly grown in men. On the other hand, males engaged more in starting their own business (from 0.0% in early, 5.9% in sustained, to 43.8% in stable recovery). Further differences between recovery stages were found for volunteering in the community (25.0% in early, 52.9% in sustained and 81.3% in stable) which has not shown significant growth for women although they have higher prevalence of volunteering.
Table 5 shows the extent to which meaningful activities were prevalent at different stages of recovery. The analysis of meaningful activities during recovery illustrates a progressive increase in positive engagement as individuals move through stages of recovery, with significant associations (p < 0.05) observed in several domains.
Meaningful activities by recovery stage.
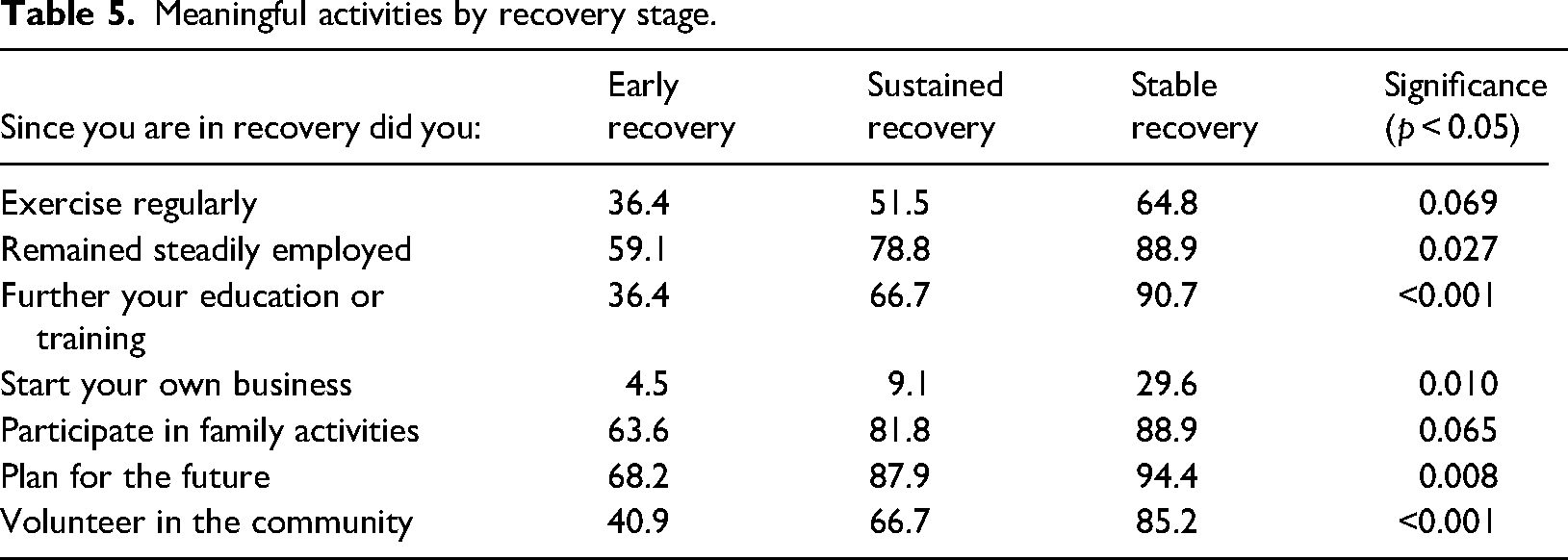
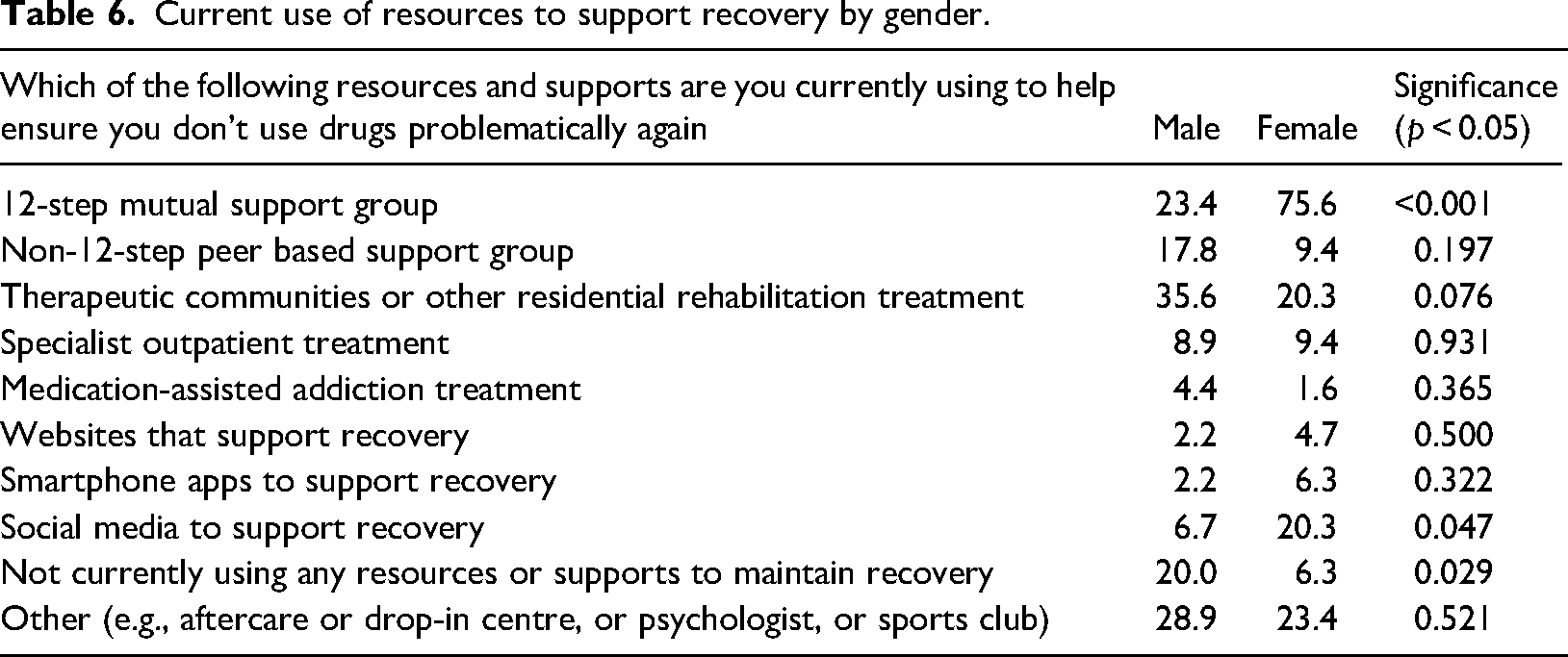
Table 6 shows meaningful engagements in terms of the extent resources to support recovery were currently used at the time of the survey, by gender. The use of 12-step mutual support groups was three times more common among females than males (75.6% vs. 23.4%), as well as the use of social media to support recovery (20.3% vs. 6.7%). Males, on the other hand, reported not using any resource or support to maintain recovery compared to females (20.0% vs. 6.3%).
Current use of resources to support recovery by gender.
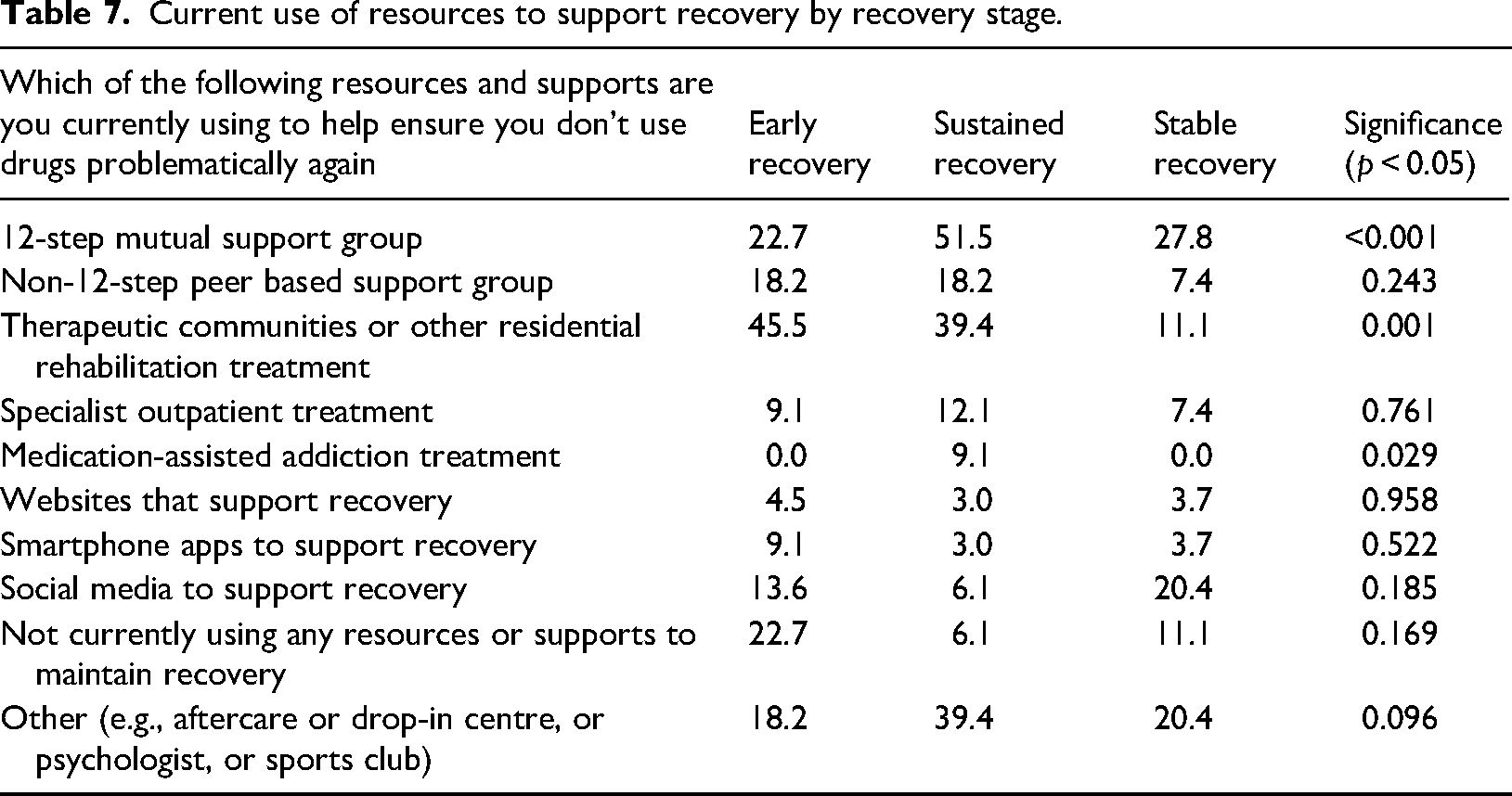
When considering recovery stages (Table 7), 12-step mutual support groups are most utilized during sustained recovery (51.5%) but see a reduction in stable recovery (27.8%). Therapeutic Communities or other Residential Rehabilitation treatment usage declines markedly from early recovery (45.5%) to stable recovery (11.1%). Interestingly, medication-assisted addiction treatment is only noted during sustained recovery (9.1%), with no reported usage in early or stable recovery stages.
Current use of resources to support recovery by recovery stage.
Barriers to recovery in terms of detrimental activities
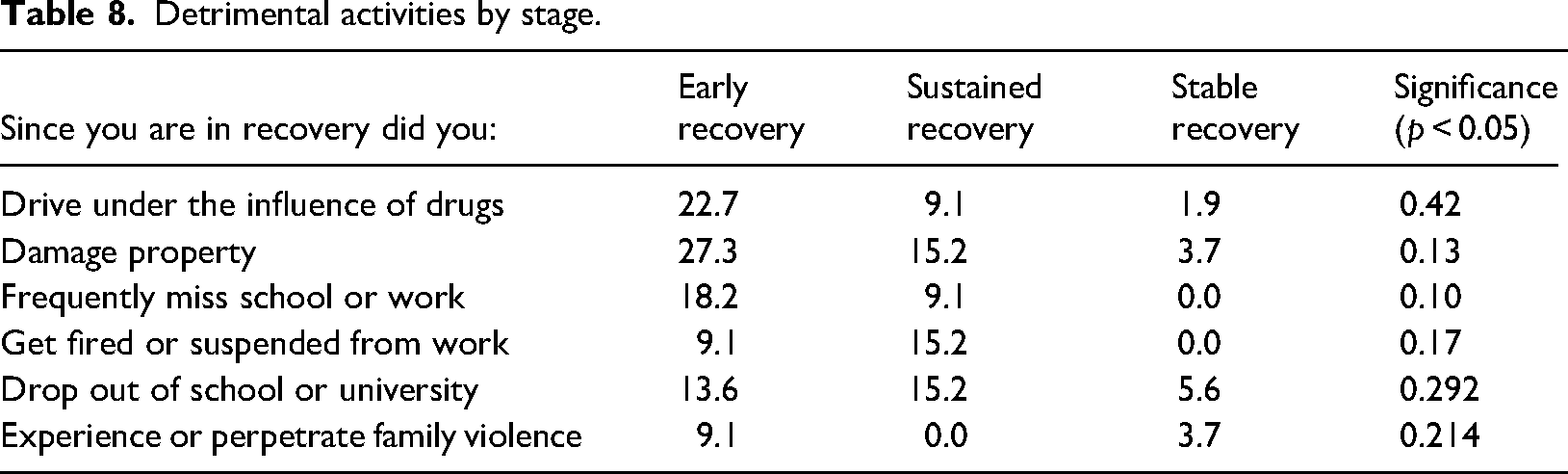
Further analysis was performed to examine the extent to which activities that could pose a barrier to recovery were prevalent in different stages of recovery (Table 8). During the course of recovery, a significant decline is observed in harmful behaviours such as driving under the influence of drugs, which drops from 22.7% in early recovery to 1.9% in stable recovery and damaging property, decreasing from 27.3% to 3.7%. Similarly, there is a reduction in frequently missing school or work, with rates falling to 0% in stable recovery. Getting fired or suspended from work initially increased in sustained recovery to 15.2% but dropped to 0% in stable recovery. The trend for dropping out of school or university and for experiencing or perpetrating family violence, however, does not show significant changes across the recovery stages.
Detrimental activities by stage.
Other addictive behaviours among individuals at various stages of recovery revealed a statistically significant reduction in tobacco use from early recovery (77.3%) to stable recovery (40.7%). Excessive working was almost three times more common in stable recovery (61.1%) than early recovery (22.7%). For the other behaviours examined, although some trends are notable, no significant differences between the recovery stages were found in gaming, gambling, sports, excessive shopping or engagement in sex. However, excessive food intake shows a huge upward trend from early recovery (22.7%) reaching almost half of the sample in stable recovery (44.4%), although without statistical significance across recovery stages.
Composite effects
The mean ± SD total number of strengths reported (based on the SABRS strength measure, ranging from 0–15) was 4.4 ± 3.14 in active addiction. By contrast, in recovery, the mean ± SD number of strengths was 10.2 ± 2.85. The total number of recovery barriers reported in active addiction (range = 0–17) was 9.6 ± 2.23, whereas, in recovery, the mean ± SD number of barriers was 2.9 ± 3.07. For the whole sample, this meant a mean decrease in barriers of −6.7 ± 3.73 and an increase in strengths of 5.8 ± 4.27.
However, we are also able to create a composite score of overall “SABRS Change” calculated as increase in strengths minus reduction in barriers. This composite SABRS change score averaged a change of 12.6 ± 7.09, indicating a marked change in overall recovery wellbeing. Each of these differences is compared across the two gender groups in Table 9.
Strengths And Barriers Recovery Scale (SABRS) change score by gender.
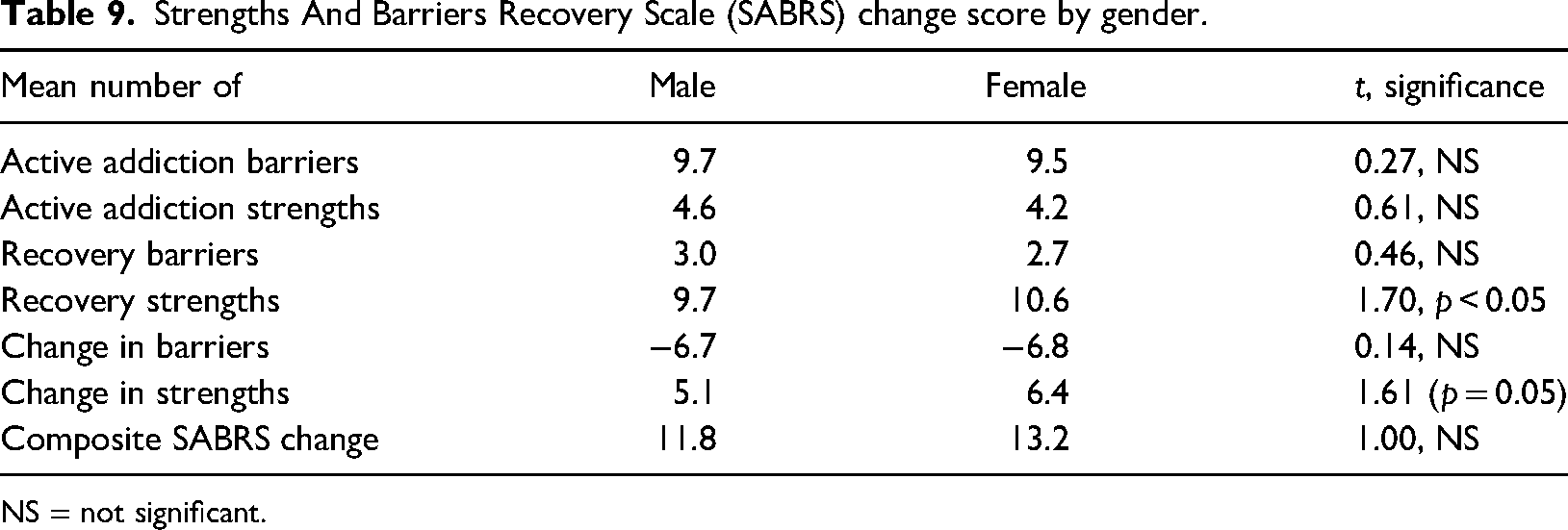
NS = not significant.
Although there is an overall mean increase in strengths and reductions in barriers, women reported a significantly greater increase in strengths and a greater composite level of change (although non-significant).
Table 10 makes a similar comparison by recovery stage at the time the survey was completed. Recovery stage matters not for the barriers experienced in active addiction (although surprisingly for the strengths in active addiction), but the differences are clear for barriers in recovery (where the significant difference lies between early and stable groups) and for strengths in recovery (where there are significant differences between all three groups. This is then reflected in the change scores with overall change significantly greater at the stable stage compared to the other two groups.
Strengths And Barriers Recovery Scale (SABRS) change score by recovery stage.
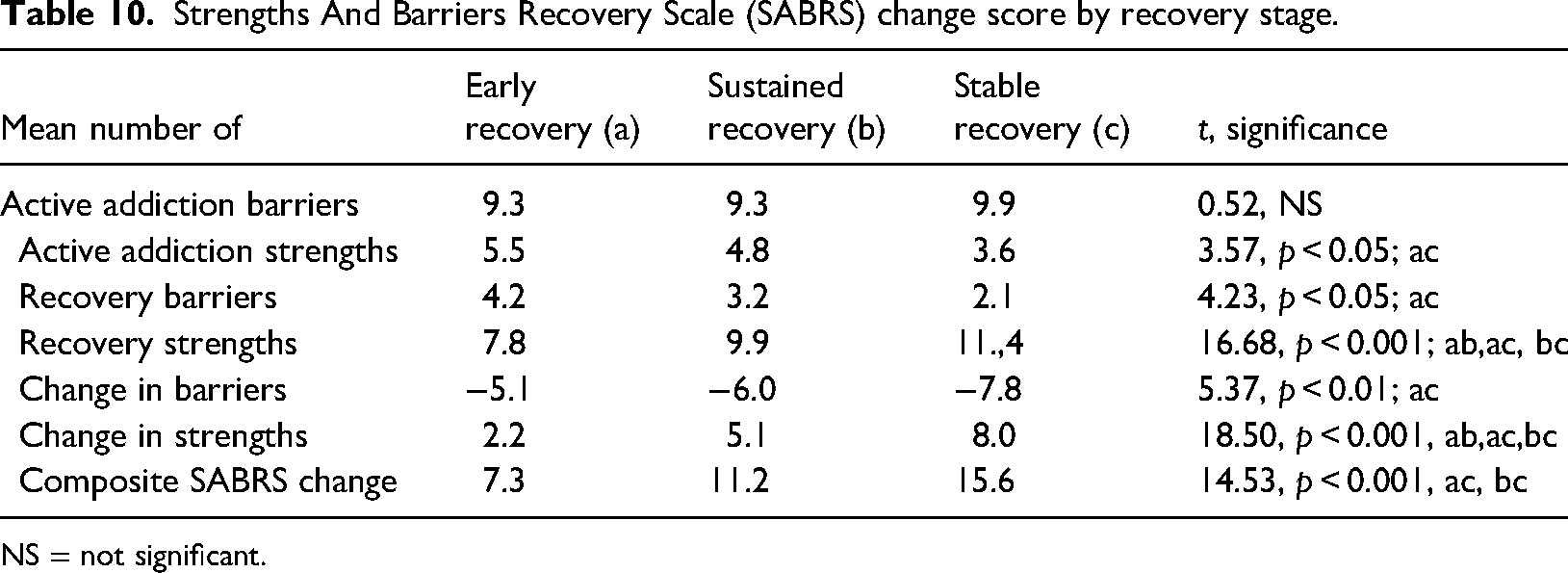
NS = not significant.
Although there are no differences in barriers at either point or in the change score, women participants reported more strengths in recovery and a greater change in recovery strengths from active addiction to recovery.
Discussion
The present study explores experiences of diverse sample of 109 individuals in recovery from Sweden to tests the progressive character of recovery in relation to meaningful and detrimental activities, as well as to measures strengths and barriers in addiction and recovery. The findings reveal significant improvements in individuals’ well-being as they transition from active addiction to recovery, evidenced by a notable increase in strengths and a decrease in recovery barriers (SABRS; Best et al., 2020). We also created a new measure for SABRS of composite change which shows that there are stepwise changes over the course of the recovery journey with the reduction in barriers greatest in the first year, and then increases in strengths happening more gradually after that. it is also evident that there are slightly greater changes in strengths for women than for men.
Furthermore, we reconfirmed that time matters in recovery – the more time people spend in recovery, the more they are engaged in meaningful activities and the less in those activities that might hinder recovery and act as barriers, such as driving under the influence of drugs, and that could harm both the individual and the public safety (Best, 2015; Best et al., 2015; McQuaid et al., 2017). These aspects also align with five of ten performance domains outlined by SAMHSA's National Outcome Measures, including abstinence, employment or educational engagement, reduced criminal justice involvement, social connectedness and perception of care (Substance Abuse and Mental Health Services Administration, Office of Applied Studies, 2002).
We found that time in recovery improves chances of finding meaning in life (and eventually improved wellbeing) through engaging in meaningful activities, personal growth, stable employment, volunteering and family activities, as well as utilization of community resources like peer based support services to boost community recovery capital (Betty Ford Institute Consensus Panel, 2007; Laudet, 2007; UK Government, 2022; White, 2007). The findings show that the odds of having more recovery community capital are higher among those in sustained recovery than among those in early recovery, and higher for those in stable recovery than those in sustained recovery. Although the levels of employment in addiction are higher in Sweden than in some of the other LiR surveys, there are clear improvements in productivity, reliability and commitment to education and employment. Furthermore, there is almost an sevenfold increase in volunteering and community participation, suggesting the importance and levels of benefits of recovery for community engagement (Best & Nisic, 2022).
What this clearly indicates is that recovery is a complex phenomenon whose many aspects are closely linked with improvements in overall citizenship and community recovery capital. However, the ongoing utilization of current support in stable recovery among females is not in line with findings from longitudinal research conducted by Dennis et al. (2014). These researchers assert that, after approximately 5 years of abstinence, considered a turning point toward stable recovery, individuals often no longer require external support to maintain recovery. Notably, their research, similar to much of the existing recovery literature, was based primarily on male samples. There were marked differences in levels of the utilization of current support, and females reported using 12-step fellowships and social media more than men, whereas men more commonly reported using Residential rehab and therapeutic communities and not using any services to support their recovery at the time of the survey. It is interesting, and merits further exploration that females in recovery are more likely to use ongoing recovery supports (such as 12-step groups and online resources), whereas males are more likely to have used discrete and time-limited intensive recovery supports such as therapeutic communities.
Potentially detrimental activities that could impede recovery, such as job loss, or engaging in activities which pose risks to both the individual and public safety, were found to diminish over time in recovery. The rates of people getting fired have dropped from around 50% to around 0% in stable recovery and school drop-out has reduced from 66% to 6%. These findings underscore the overall positive impact of recovery on reducing harmful activities, with some gender-specific differences. From a public health and safety perspective, there are marked reductions in driving under the influence and damaging property for men, whereas females show significant improvements in areas like school or work attendance and workplace stability. There are marked changes in family functioning with 60.9% of females reported committing or experiencing family violence during active addiction, whereas only 2.6% reported this event during stable recovery. We found statistically significant reduction in tobacco use from early recovery (77.3%) to stable recovery (40.7%), indicating a positive trend towards healthier habits as recovery progresses, although these rates are still relatively high. We also investigated whether people in recovery are engaged in various excessive activities that potentially can be detrimental and act as “substitute” addiction. Excessive working was almost three times more common in stable recovery (61.1%) than early recivery (22.7%), suggesting a potential shift towards workaholism, but more research is needed to determine whether work is used as a coping mechanism in later stages of recovery. However, for almost all of these effects, it is not an overnight process and the pattern of change varies across genders and groups but consistently grows over at least the first five years of the recovery journey (Betty Ford Consensus Group, 2007).
One noteworthy trend observed in the data, although not statistically significant, was the marked increase in self-reported excessive food intake, rising from 22.7% in early recovery to 44.4% in stable recovery, and excessive working, almost three times more common in stable recovery (61.1%) than early recovery (22.7%). Although this pattern may initially seem counterintuitive, it aligns with previous research suggesting that individuals in recovery may shift from one coping behaviour to another as they manage emotional regulation and reward sensitivity (Vaillant, 1966)). This finding suggests a need for holistic recovery support that also considers nutrition, emotional wellbeing, and the potential for cross-addiction or behavioural substitutions.
The composite SABRS change score, averaging a 12.6 change, has shown this marked improvement in overall recovery well-being. Furthermore, the data indicate variations in recovery experiences across genders and stages of recovery, with women participants reporting more strengths in recovery and a greater change in recovery strengths from active addiction to recovery. These insights underscore the importance of personalized support and interventions tailored to individual recovery journeys, acknowledging the influence of gender and time in recovery on the challenges and strengths experienced during the recovery process. The key messages from this are that, even in stable recovery, there are still clear barriers to live through, and that barriers reduce to their minimum typically earlier in the recovery journey than strengths grow. Similarly, although stage is the stronger predictor of net recovery growth, gender does play a role with women in recovery generally showing greater accrual of strengths, and the present study further provides evidence that women's and men's recovery journeys are typically not the same.
Building upon the findings from previous LiR studies (Best, 2015; Best et al., 2015; Laudet, 2013; Mcquaid et al., 2017; McQuaid & Dell, 2018) that highlighted the significant role of gender, we confirmed the existence of a number of gender differences. The findings reveal significant gender differences in recovery stages of the sample, with women more likely to be in stable recovery, whereas men are more often in sustained or early recovery, suggesting potential variations in recovery experiences, motivations or the effectiveness of support systems between genders. The findings could imply that individuals in different recovery stages have varying levels of willingness or ability to participate in research. For example, those in stable recovery might feel more secure in their recovery process and therefore more willing to share their experiences, or they might see more value in contributing to research that could benefit others in similar situations. Conversely, individuals in early recovery might be less likely to participate due to the challenges they are currently facing.
Additionally, the present study adds to the evidence that a transition must be done from a deficit to a strengths-based model which has created an agenda in restorative justice and therapeutic jurisprudence, as well as an emerging evidence base around mental health and addiction recovery founded in the core values of CHIME: Connectedness, Hope, Identity, Meaning and Empowerment (Leamy et al., 2011). What is clear is that recovery is a process and not an event, given that, although there are some immediate improvements within the first year (referred to as early recovery), others take much longer. The findings are in line with the international evidence and provide strong support for the suggestion that recovery oriented treatment will only produce significant benefits for people and communities where support goes beyond acute clinical care to support people throughout their recovery pathways, and that continuity of care and support is an essential part of sustaining change (McKay, 2021). These findings highlight the necessity for gender-sensitive approaches in both research and practice. Understanding the specific needs, barriers and facilitators to recovery for different genders can inform targeted interventions. Future research should explore the reasons behind these differences, including societal roles, stigma, access to and types of treatment and recovery support services, and personal networks, to better support individuals through their recovery journey
Limitations
The present study has several noteworthy limitations, typical to previous LiR surveys. The selection process for participants was not within our control, and the broader group from which these participants were drawn remains unknown. Consequently, it's difficult to assert the representativeness of our sample. The reliance on self-reported information for both when the participants of the study were in addiction and in recovery must be taken into account because it could have potentially led to an overemphasis of the negative impacts of addiction and an overvaluation of recovery benefits, and has depended on participants’ self-identification with recovery for inclusion.
The observed differences in changes over time and gender-specific experiences indicate distinct areas requiring further investigation. Moreover, although the present study illuminates that people do have recovery capital in addiction, as well as ongoing barriers to recovery, this survey may not fully capture the diverse challenges and facilitators of recovery. Future analysis should aim to delve deeper into cultural differences in recovery journeys and conduct more thorough comparative analyses across countries, which we plan to do.
Despite these challenges, the present study questions prevailing gender-specific beliefs and support in both addiction and recovery and significantly contributes to the body of research by introducing a focus on measuring positive and negative elements of community recovery capital domains of both the current scores and changes over time.
Conclusions
The present study expands the scope of how recovery is defined, supporting a view that emphasizes the broad benefits of recovery beyond abstinence (Betty Ford Institute Consensus Panel, 2007; UK Drug Policy Commission, 2008). It offers a more inclusive understanding of recovery. These insights support a reevaluation of long-term recovery outcomes, reflecting the enduring nature of recovery, as seen in earlier studies (Dennis et al., 2014; Laudet & White, 2008). They also highlight the need for gender-specific support strategies to better understand different recovery processes.
The findings show that many individuals in recovery report living meaningful lives and contributing to their families and communities. Our results affirm the progressive nature of recovery: as time in recovery increases, barriers tend to decrease, whereas strengths increase. This is a hopeful message for individuals and families affected by addiction. It supports the idea that initiating recovery improves life circumstances, which in turn helps sustain recovery (Best & Laudet, 2010; Best, 2015; Laudet, 2013; McQuaid et al.,2017).
These findings suggest that addiction treatment should go beyond clinical interventions (Simpson, 2004). We propose a rethinking of how recovery outcomes are evaluated. This includes a shift from institution-based measures to those rooted in families, neighborhoods and communities – focusing on recovery capital in areas such as family life, education, employment and community involvement.
Footnotes
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The authors received no financial support for the research, authorship and/or publication of this article.