
Abstract
Keywords
Introduction
In comparison to other European countries, Sweden has a low prevalence of illicit drug use among both adults and adolescents (European Monitoring Centre for Drugs and Drug Addiction, 2022). Self-reported lifetime use of cannabis (i.e., the most prevalent drug, among 15–16-year-olds) ranges from 8% to 28%, where Sweden is at the lower end and Czechia is at the highest. However, a recent study applying new methodology found Swedish estimations of cannabis use among young adults may need to be increased by a factor of two to three to give an accurate prevalence (Andersson et al., 2023).
Swedish drug legislation has traditionally been strict in international comparison, where the Act on Penal Law on Narcotics (SFS 1968:64) criminalizes all types of illegal possession and personal use of narcotics (i.e., drug offences). The rationale is to prevent young people from trying drugs, and the combination with easy access to care and support it is supposed to reach young drug users at an early stage. The policy is hereby expected to work through a positive penal power scheme (i.e., facilitating support and rehabilitation) (Garland, 2013), and where the target groups, in line with general European policy, are primarily understood as victims of addiction, requiring medical and social support (Protais, 2016). This article explores how the Swedish system functions in relation to what characterizes adolescents convicted of drug offences and the extent and content of legal responses and the rehabilitative measures they receive. Rehabilitative measures is used as a broader categorizing term of social interventions, e.g. outpatient care, institutional care, initiated and provided by social services.
The Swedish system
In Sweden, criminal responsibility begins at the age of 15 years. Children who commit offences before this age cannot be subject to legal penalties. In such instances, the primary responsibility for assessing the need for care and support and taking measures lies with social services. However, under specific conditions, the police and prosecutors may still investigate the circumstances surrounding the crime. After a child welfare investigation has been conducted, social services can suggest decisions on various measures, for example rehabilitative measures. However, if the adolescent is of criminally responsible age, social services assess young people's offending behaviour, drug problem and other personal circumstances within the framework of the legal system for adolescents to suggest an appropriate legal response including possible service responses. Accordingly, two different legal processes are initiated: one according to criminal law and the other according to social law. These processes are parallel but are at the same time closely connected.
The social services’ assessment contains an estimation of needs of care and support as well as a plan for the extent and duration of the rehabilitative measures considered. Relying (partly) on the social services assessment, the prosecutor can waive prosecution for 15–17-year-olds who plead guilty if adequate support is given outside the court system. In some cases, the court may sentence adolescents to rehabilitative measures within the framework of a legal response for young persons, known as youth care. This can occur if the social services’ measures, as outlined in the care plan, are deemed sufficiently intrusive in light of the penal value, the nature of the crime and any previous criminality. Additionally, this response requires the adolescent to have a specific need for care or support, as defined by the Social Services Act (2001:453), SoL or the Act with Special Provisions on the Care of Young Persons (1990:52), LVU.
In sum, the Swedish system put great trust in that the connection between the judicial system and the social services will result in adequate support for drug using/criminal young people. Keeping drug use as an offence in the penal code places Sweden in a group of few exceptions from international policy standards. This underlines the importance of studies on how the systems works and if it provides support at earlier stages. This study will examine this by analysing who are offered and undergo rehabilitative measures, as well as results in terms of recidivism in drug offences. One way to assess how well founded the policy intention of having the justice system “deliver” young people with drug problems to the social services for care and support is to see whether it identifies individuals not already known by the support system and whether they receive the support they need.
Aim and research questions
The purpose of this study was to examine how the judiciary and social services succeed in identifying and providing support to adolescents convicted of offences against the Act on Penal Law on Narcotics (PLN). Furthermore, the analysis covered the adolescents’ recidivism, psychiatric and drug-related healthcare contacts over a period of three years. The study was guided by the following research questions:
What characterized adolescents convicted of drug offences in terms of criminal and socioeconomic background? What legal responses followed the drug offence and to what extent did they include rehabilitative measures from social services? What was the reconviction rate in new drug offences with respect to legal response at the index offence, and to what extent did they receive health care (psychiatric and drug-related diagnosis) during the follow-up period (after the index offence until 2020)?
Theory and previous research
Punishment or rehabilitation
A substantial percentage of youth crime in Sweden is related to drug use (Egnell et al., 2019) and Swedish drug policy focus on minor drug violations and personal use (Anderberg et al., 2022; Lenke & Olsson, 2002). However, criminalization of personal use has been criticized, where some argue that it is contra-productive and impedes both motivation to seek treatment and society's ability to provide drug abuse treatment (SOU 2023:62). Others have raised ethical concerns regarding coerced treatment following conviction (Caulkins et al., 2021) questioning whether compulsory drug treatments are beneficial (Werb et al., 2016).
Pro and contra arguments for the involvement of drug-using adolescents in the criminal justice system entail two competing theoretical perspectives: deterrence and labelling. The former predicts that sanctions will reduce offending, and the latter that sanctions may increase subsequent offending (Liberman et al., 2014; Lopes et al., 2012; Motz et al., 2020). Labelling theory seems to gain most support from research literature (McAra & McVie, 2010; Sandøy et al., 2022) and the effect of sanctions seems to vary by age and crime (Huizinga & Henry, 2008; Sandøy et al., 2022), indicating that sanctions increase offending in high-risk youth, while having negligible effects among youth with lower risk (Morris & Piquero, 2013).
An argument for criminalization of personal use is that greater force can be used to connect offenders to support and treatment via the court system (Petrosino et al., 2010; SOU 2023:62). However, available statistics provide little evidence to suggest that the criminalization of minor drug offences significantly improved the reach of rehabilitation measures for drug users (Estrada et al., 2023). Something that needs to be addressed when preventing further drug use among adolescents in rapidly developing/deteriorating processes (Hartnett et al., 2017) is that the average age of onset for cannabis use in European Union population was 16 years, while the average for first-time help seeking was 25 years (European Monitoring Centre for Drugs and Drug Addiction, 2022). This late entry in treatment is often prompted by multiple negative consequences and being pressured from family, friends, or employers (Tucker, 2001).
Early interventions (i.e., measures offered before abuse or dependence criteria are met) have shown positive effects on both criminality and drug use (Carney & Myers, 2012). Adolescent drug use prevention is also stressed in longitudinal studies (Nilsson et al., 2014; Stenbacka & Stattin, 2007), which indicates that illicit drug use is a significant predictor for adult criminality. The Swedish National Council for Crime Prevention further concludes that drug use and convictions at an early age (often for minor drug offences, such as personal use) is associated with greater recidivism (Westlund & Öberg, 2021).
Programs that redirect individuals to treatment instead of criminal sanctions (Albert et al., 2011; Caulkins et al., 2021) has shown limited but promising outcomes on recidivism, drug use and psychosocial health (Lindquist-Grantz et al., 2021). Bernard et al. (2020) found that such programs for low-level drug offenders are likely to be cost-effective, avoid overdose deaths and improve quality of life. The most promising seem to be programs delivered in an individual format over multiple sessions (Carney & Myers, 2012). In particular for young offenders, provisions by healthcare and social services are likely to be more helpful than fining (Cullen, 2005; Sandøy et al., 2022).
Swedish follow-up studies on adolescents with alcohol and drug problems are scarce. Anderberg et al. (2021) found that two-thirds of adolescents who start outpatient treatment for drug use problems had no indication of drug use one year later. Further, when investigating criminality among adolescents with drug use, Anderberg et al. (2022) found that about one-quarter of the adolescents who begin outpatient treatment had been convicted of crimes at 1-year follow-up. Of the reconvicted adolescents, 84% had indications of continued drug or alcohol use and 74% had been charged for drug-related offence within the 1-year follow-up time. However, concerns have been raised on evaluating the justice system based on reconvictions due to selection bias, i.e., already identified young people are more likely to be suspected again (Bateman & Wigzell, 2019; McAra & McVie, 2010).
Risk factors for drug use
Research on risk and protective factors specific to drug use and related problems indicates that there are risk factors across various domains and levels: societal, familial, group and individual (Folkhälsomyndigheten, 2021). Typically, a combination of (cumulative) risk factors increases the likelihood of drug usage among adolescents (Socialstyrelsen, 2020). Poor school attachment and performance as well as having friends who use drugs, lack of leisure activities and drug availability in different combinations increase the risk of drug use (Aston, 2015; Cleveland et al., 2008; Fergusson et al., 2008; Hoeben et al., 2016; Kristjansson et al., 2021; Stone et al., 2012; von Sydow et al., 2002). Furthermore, the risk of dependence is higher among those who have ever had a psychiatric diagnosis (Lopez-Quintero et al., 2011). Other mental health-related risk factors include poor coping ability and low self-esteem (von Sydow et al., 2002).
Drug use and comorbid mental health problems
A review of adolescent drug use studies found that 60% had comorbid diagnoses, most common conduct disorder and oppositional defiant disorder. Child psychopathology, especially conduct disorder, was linked to early onset of drug use in later adolescence (Armstrong & Costello, 2002). A study of self-reported mental health problems among young people in Swedish outpatient clinics found that 34–54% had concentration difficulties, sleep problems, anxiety and depression, while around 20% were diagnosed with mental health disorders (Richert et al., 2020). Treatment for adolescents with drug use and comorbid mental health problems have in different studies shown varying results (Anderberg et al., 2021).
Data and methods
Population
The population consists of all adolescents, 15–17 years, convicted in Sweden for offences against the Act on Penal Law on Narcotics, PLN, (i.e., drug offences) in 2017 (N = 2017). After removal of 170 individuals without valid identification number, the study population contains 1847 individuals. Data on convictions were drawn from the National Conviction Register (NCR) at the Swedish National Council for Crime Prevention. To enable the study of a range of social background variables, different data sources from national registers were linked at individual level by unique identification number given to all Swedish residents at birth or during the immigration process. The excluded participants were primarily asylum seekers, for whom a lack of personal identification numbers hindered data integration from national registers, preventing comparison with the remaining study population. During the study period, a significant number of unaccompanied asylum-seeking minors arrived in Sweden, most of whom resided in out-of-home care and maintained regular contact with social services.
To analyse the assessment process rendering different legal responses, a subsample of 189 adolescents from 29 cities were selected using a stratified sampling procedure. Selection criteria was that all seven geographical public prosecution areas in Sweden were to be represented, as well as regions of different population density and individuals with different types of legal response. The subsample was made proportional according to age, while girls were made slightly over-represented to gain a sufficient large number. The subsample covered 10% of the study population, 17% of girls and 9% of boys (Table 1).
Population.
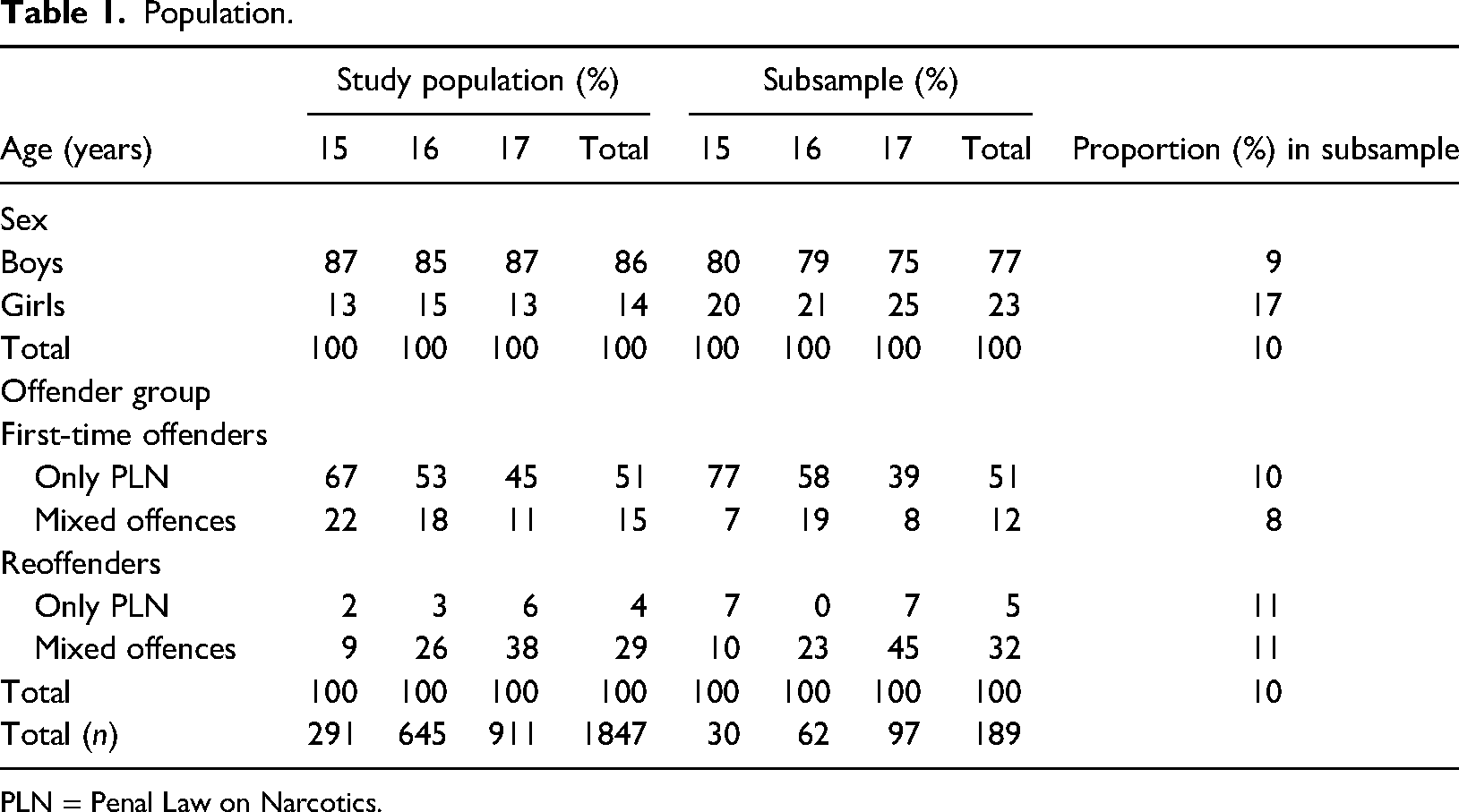
PLN = Penal Law on Narcotics.
Index offence & follow-up period
The first conviction for a drug offence in 2017 constitutes the index offence and the follow-up period starts immediately after the conviction date, and stretches until the end of 2020, or until emigration or death.
Study groups/offender groups
The population was divided into four mutually exclusive offender groups to render more homogenous groups in terms of criminal history:
First-time offenders, only PLN (n = 945). First-time offenders, mixed offences (n = 285). Reoffenders, only PLN (n = 82). Reoffenders, mixed offences (n = 535).
Outcomes
(1) Legal response at index offence (waiver of prosecution with formal caution, fine, youth services, youth care and other).
(2) Recidivism (at least one drug offence after the conviction date of index offence)
(3) Healthcare contacts for psychiatric or drug-related diagnosis, a composite measure: Measures health care (inpatient or specialized outpatient care) with psychiatric diagnosis according to the Swedish version of the International system of Classification of Diseases, ICD-10: F1–F9 (including care at psychiatric clinic without diagnosis, MVO = 9), including mental and behavioural disorders due to use of drugs (psychoactive substances) and/or use of psychotropic drugs according to The Anatomical Therapeutic Chemical Classification code, ATC: N03, N05A excl. N05AN, N05B, N05C excl. N05CH01, N06A, N06BA excl. N06BA07, C02AC02. Psychotropic drug use is considered a proxy for outpatient care (other than specialized outpatient care) due to psychiatric disorders because there are no national register data on primary health care in Sweden.
Background factors
The choice of background factors was guided by prior research (see section Risk factors for drug use) and available data. The socioeconomic background factors relate to the birth mother only, in order to reduce missing values. The following background factors were used (descriptive statistics are provided in Table 2):
Research data, registers and data retrieved for variables.

(a) Administered jointly by the Swedish School Authority and Statistics Sweden. (b) ICD-10: F1–F9. Inpatient care or specialized outpatient care without diagnosis at psychiatric clinics (MVO = 9). (c) ATC: N03, N05A excl. N05AN, N05B, N05C excl. N05CH01, N06A, N06BA excl. N06BA07, C02AC02.
Sex: Females and males.
Migrant background: Swedish background refers to at least one parent born in Sweden. Foreign background refers to both parents born abroad (including missing information on parents’ birth country).
Qualified for upper secondary education: A dichotomous variable was used indicating qualification (or not) for upper secondary education at exit from primary school (aged 15–16 years). 12 percent were missing in The Primary School Register, which could either be a result of frequent truancy or attending a school for students with special education needs or institutions that do not report to the register.
Out-of-home care (<13 years of age): Foster family care or residential care at any time before the age of 13 years because of parental neglect, maltreatment or abuse in family or own disruptive behaviour.
Mother's social assistance: Birth mother receiving any level of social assistance from the last-resort minimum income scheme when the study subject was 12–14 years, number of years (0–3 years).
Mother's educational level: Birth mother's highest educational level when the adolescent were 12–14 years of age categorized into three groups, (i) primary education (no ISCED level 3); (ii) upper secondary education (ISCED level 3 and 4); and (iii) post-secondary education (ISCED level 5 or higher). A fourth category for missing information was included.
Mother's/father's conviction: Criminal offences settled by a public prosecutor or a court when study subject aged 0–14 years.
Statistical analysis
Analyses were made with the SAS software package (SAS Institute Inc., Cary, NC, USA) (procedure given in brackets). Descriptive statistics are presented in Tables 1, 3 and Figures 1–5 (PROC FREQ). In Figures 4 and 5, the study population was restricted to individuals born in 2000–2002 due to comparability with the general population.
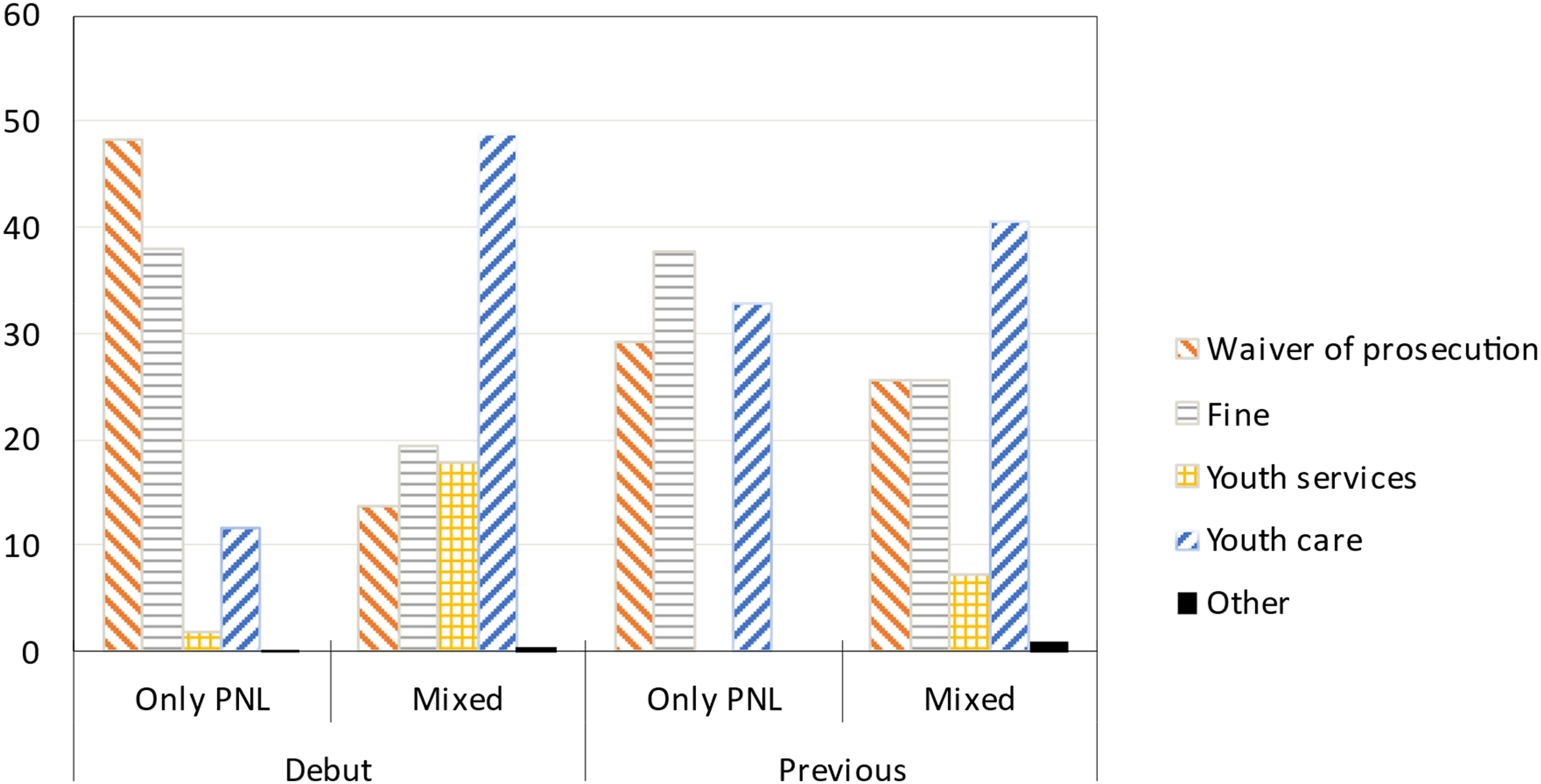
Legal response by offender group. Percent.
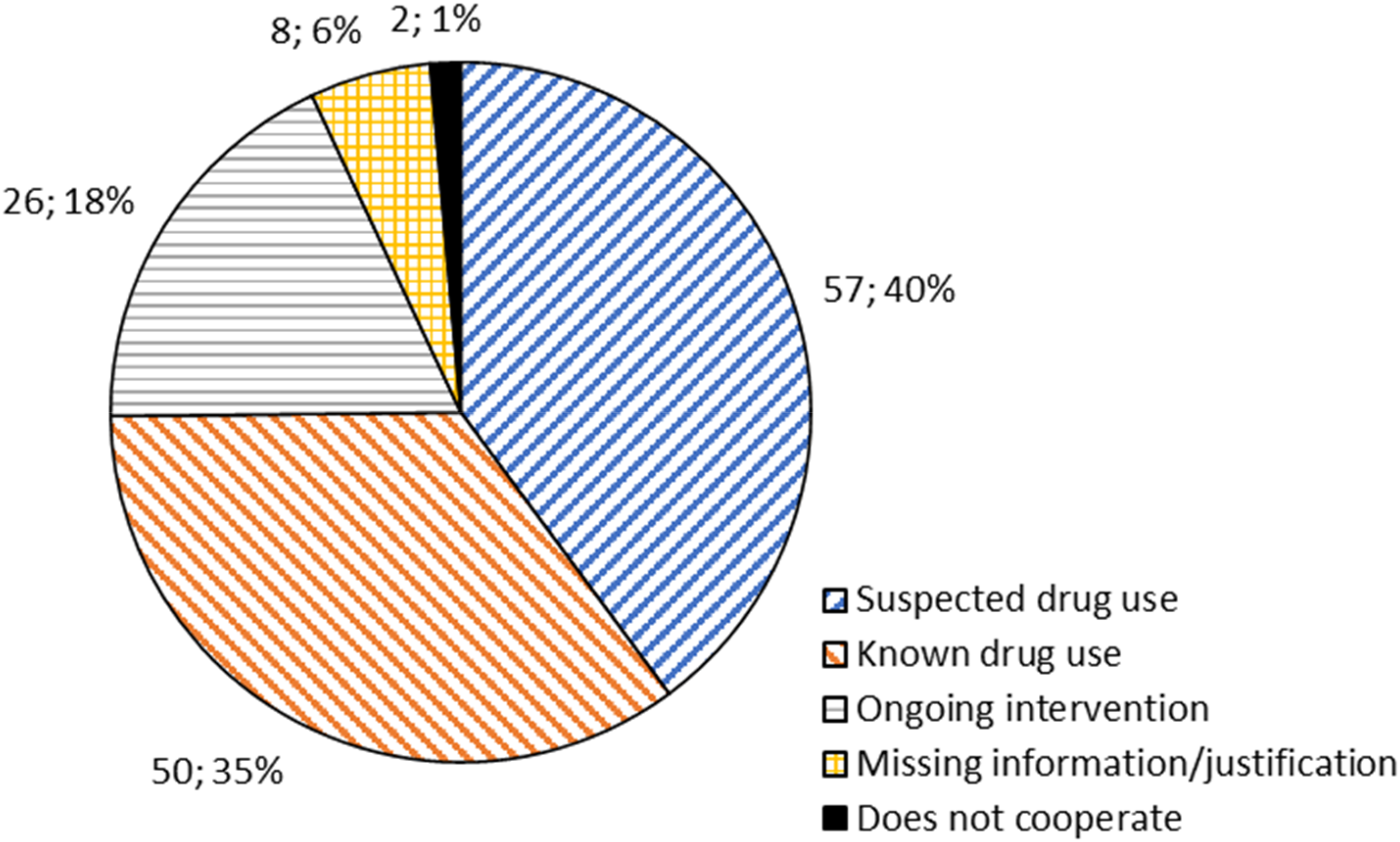
Need for rehabilitative measures, justification by social services. Number, Percent.
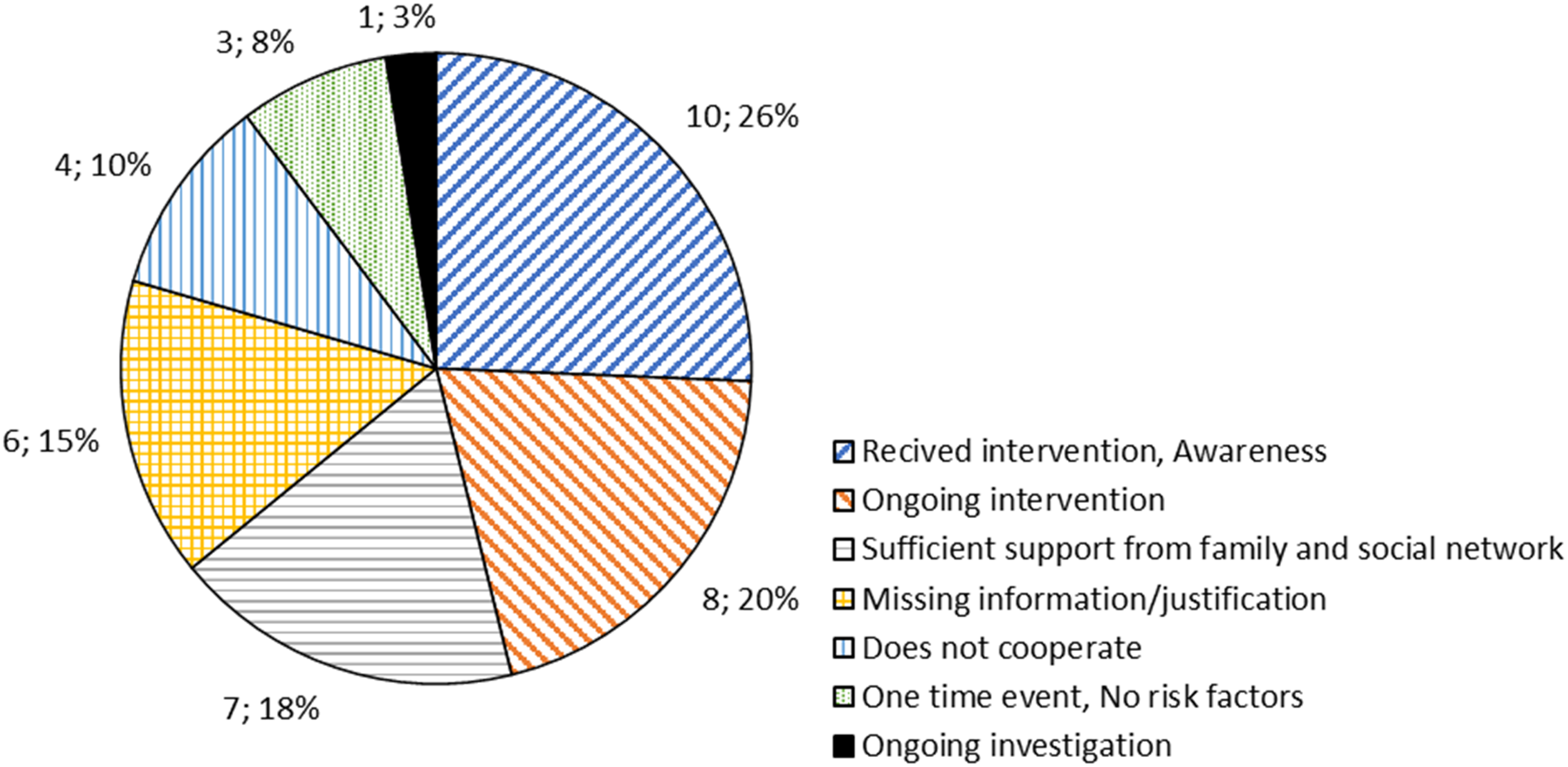
No need for rehabilitative measures, justification by social services. Number, Percent.
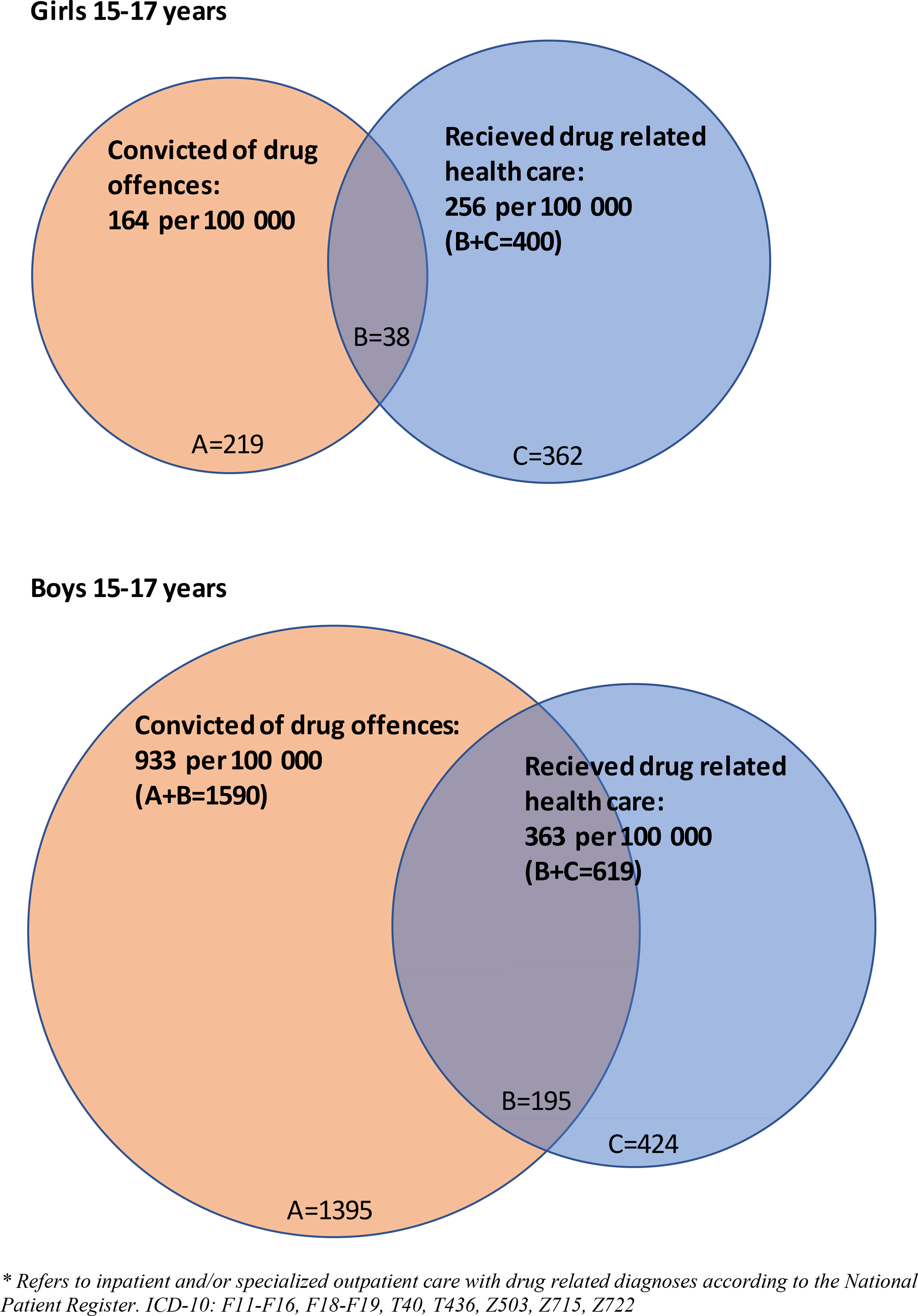
Adolescents in the general population who received drug related health care* and/or were convicted of drug offences (PLN). Boys and girls 15–17 years of age in 2017. Total number (A, B, C) and number per 100 000 inhabitants. *Refers to inpatient and/or specialized outpatient care with drug related diagnoses according to the National Patient Register. ICD-10: F11–F16, F18–F19, T40, T436, Z503, Z715, Z722.
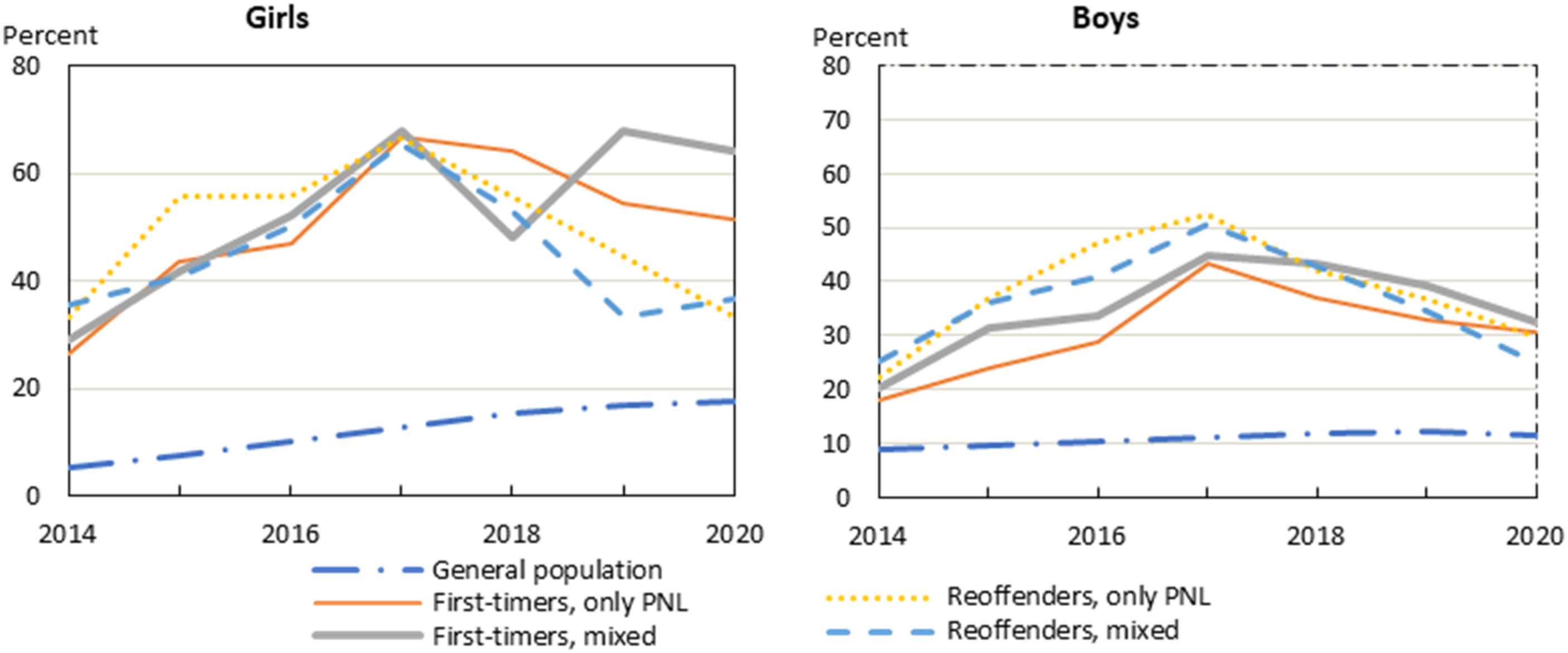
Health care contacts for psychiatric or drug-related diagnosis, a composite measure: (1) Inpatient or specialized outpatient care for psychiatric disorders ((including mental health problems and behavioral problems caused by narcotics (ICD-10: F1–F9, incl. care without diagnosis at psychiatric clinics MVO = 9)), (2) or use of psychotropic drugs 2014-2020 by sex and offender group (ATC: N03, N05A excl. N05AN, N05B, N05C excl. N05CH01, N06A, N06BA excl. N06BA07, C02AC02). Individuals born in 2000–2002. Percent.
Background factors
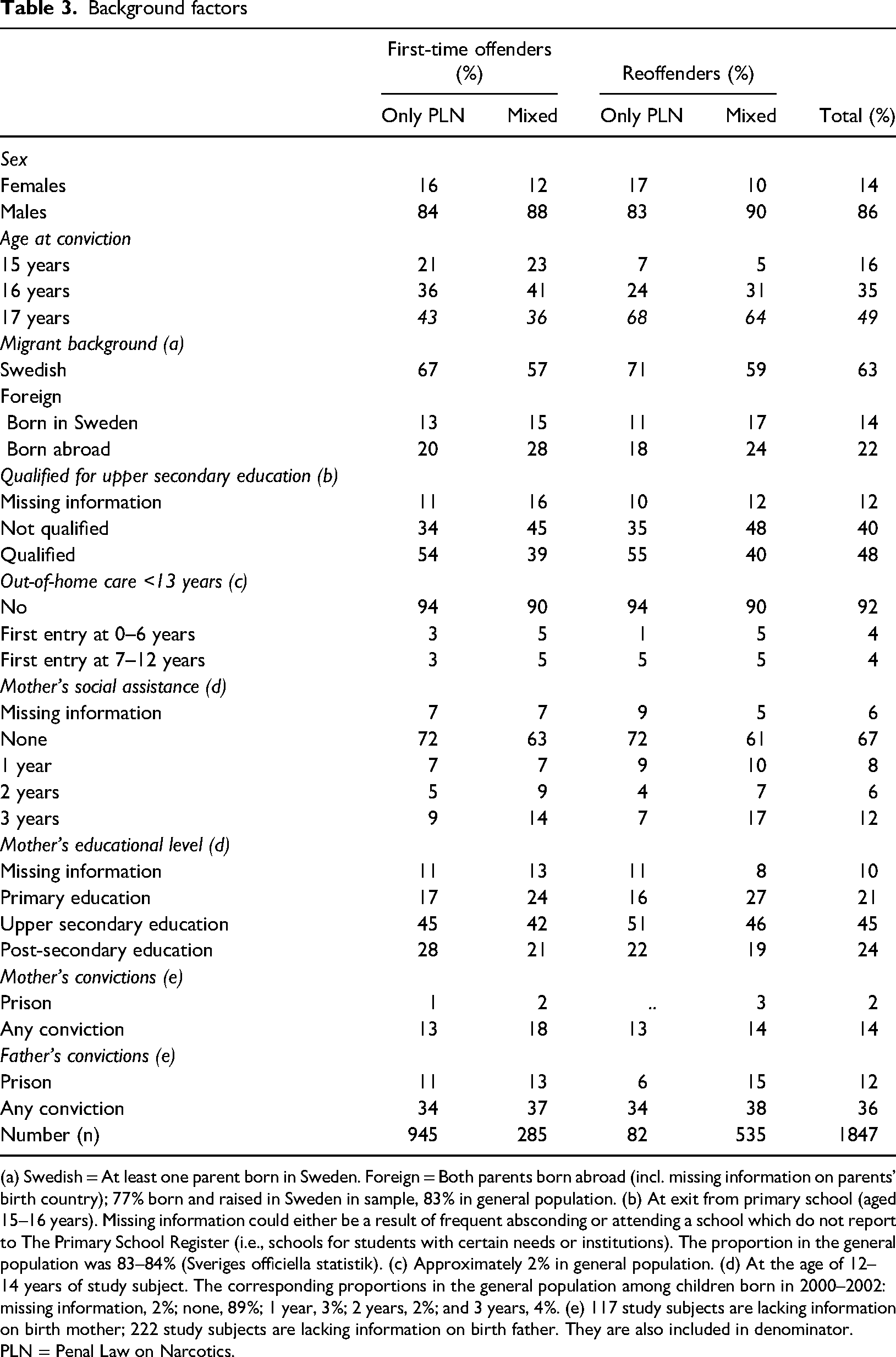
(a) Swedish = At least one parent born in Sweden. Foreign = Both parents born abroad (incl. missing information on parents’ birth country); 77% born and raised in Sweden in sample, 83% in general population. (b) At exit from primary school (aged 15–16 years). Missing information could either be a result of frequent absconding or attending a school which do not report to The Primary School Register (i.e., schools for students with certain needs or institutions). The proportion in the general population was 83–84% (Sveriges officiella statistik). (c) Approximately 2% in general population. (d) At the age of 12–14 years of study subject. The corresponding proportions in the general population among children born in 2000–2002: missing information, 2%; none, 89%; 1 year, 3%; 2 years, 2%; and 3 years, 4%. (e) 117 study subjects are lacking information on birth mother; 222 study subjects are lacking information on birth father. They are also included in denominator.
PLN = Penal Law on Narcotics.
Recidivism in drug offence (Figure 6a,b) was estimated using survival functions with the life-table method (PROC LIFETEST) and refers to the percentage in the study population who had had at least one drug offence settled by a public prosecutor or a court within 3 years after index offence. Time (person-days) was calculated with entry date defined as the day after the conviction date of index offence, and the exit date defined as the first conviction date of a new drug offence (event), or date of death or emigration (censored), or end of follow-up (December, 2020). Information on date of death was collected from the Swedish Cause of Death Register and date of emigration from the Total Population Register. Figure 6a refers to recidivism in drug offences by sex and offender group. Figure 6b refers to recidivism in drug offences among boys who were convicted of their first drug offence in 2017 (i.e., boys in the offender group: “first-timers, only PLN”) by age at index offence and legal response (with or without rehabilitative measures).
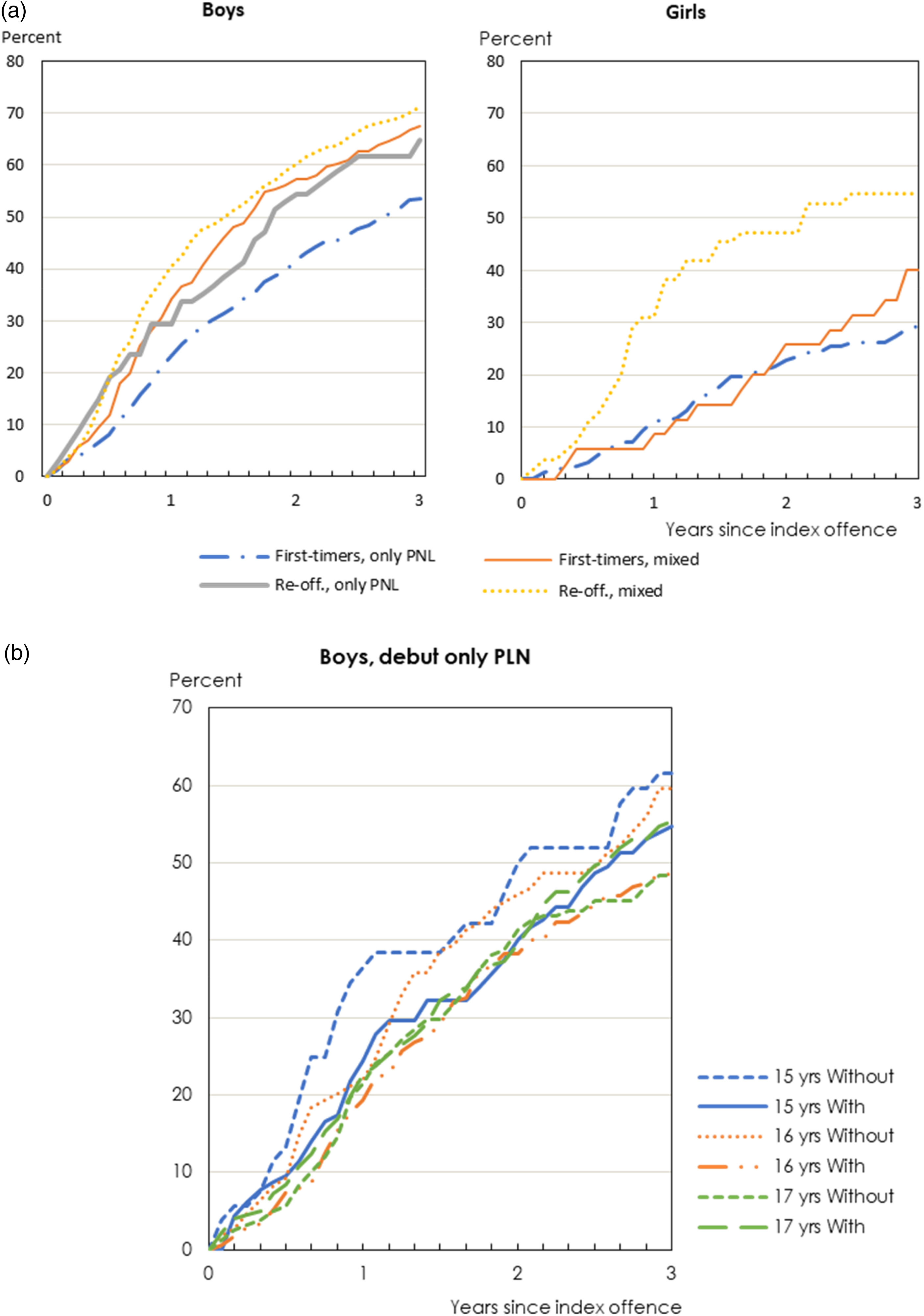
(a) Proportion who reoffended in PLN offences after index offence in 2017, by duration (years since index offence), sex and offender group. Percent. (b) Proportion who reoffended in drug offences among boys who were first-time offenders, only PLN, by duration (years since index offence), age and legal response (with or without rehabilitative measures) at index offence in 2017. Percent.
Results
Index offence
The vast majority (97%) of the study population were convicted of minor drug offences (the index offence) concerning use or possession for own use. In 61% of the cases, the conviction involved the index offence alone (i.e., one drug offence). In 21% of the cases, the conviction covered two offences and, in 18% of the cases, three or more offences. For a small group of adolescents (1%), the conviction involved ten or more offences.
Crimes other than drug offences were common when the conviction included more than one offence (the index offence). When the conviction included two offences, almost half were convicted for other types of crimes together with the drug offence; when three or four offences were included, it applied in close to 90% of the cases; and, when five or more offences were included, it applied to all. When these other offences were of a more serious nature than the drug index offence, it was mainly offences under the Criminal Code (SFS 1962:700), where theft, robbery and assault were most common, followed by violent crimes.
There is a significant variation in the proportion of convicted individuals across different counties. The rate was approximately three times higher in counties with the highest proportions of convictions for drug offences compared to those with the lowest rate. Nationally, 617 per 100,000 15–17-year-olds (0.6%) were convicted, with the highest observation in the Gotland (906 per 100,000 inhabitants) and the lowest in Kronoberg (301 per 100,000 inhabitants).
Background factors
Girls constituted 14% in the study population. At the time of the conviction, 49% of the population were 17 years old, 35% were 16 years and 16% were 15 years (Table 1). On average, the index offence occurred 3-4 months prior to conviction.
Two-thirds were first-time offenders, and most had no other offences beside drug offences. First-time offenders with only PLN offences were the largest offender group in the study (51%). The second largest offender group (29%) was reoffenders who had been convicted of other offences beside drug offences (i.e., mixed offences), either prior to or together with the index offence. The remaining fifth of the study population were divided into two additional offender groups: first time offenders with mixed offences (15%), and reoffenders with only PLN offences (4%). The distribution between offender groups were similar in the subsample (Table 1). Offender groups with only PLN offences had a higher proportion of females (first-timers 16% and reoffenders 17%) compared to offender groups with mixed offences (12% and 10%) (Table 3).
The differences in socioeconomic background factors between offender groups were associated with number of offences (PLN only versus mixed offences) rather than past criminal history (first-timers versus reoffenders). Migrant background was somewhat more common in the mixed-offender groups. Among first-time offenders, 43% had migrant background in the mixed offences group compared to 33% in the PLN only group. Qualification for upper secondary education was less common in the mixed-offender groups than in the PLN only groups (39–40% versus 54–55% (Table 3). Birth mothers of adolescents in the mixed-offender groups had lower educational level on average compared to adolescents in the PLN only offender groups (Table 3).
Furthermore, out-of-home care before age 13 was more common in the mixed offence groups than in the PLN only groups (10% versus 6%). Birth mothers’ social assistance was more prevalent in the mixed offender groups, 17% of adolescents in the mixed reoffender group had mothers who received yearly social assistance when they were between 12 and 14 years old compared to 7% in the PLN only reoffender group. Fifteen percent in the mixed reoffenders group had birth fathers who had been sentenced to prison compared to 6% among PLN only reoffenders (Table 3). Overall, these differences in socioeconomic background factors between offender groups were slightly more pronounced among girls than among boys.
Legal responses
The majority (68%) of the adolescents received legal responses consisting of rehabilitative measures (i.e., waiver of prosecution with formal caution or youth care). A waiver of prosecution with formal caution and fines (by court or by prosecutor) were the two most common legal responses (36% and 32%, respectively). Just over one-quarter were sentenced to youth care (27%), while youth services occurred less often (6%). A small proportion of adolescents (0,4%) received other sanctions (probation, suspended sentence, community service and prison). Waiver of prosecution was more often used for girls (girls 47%, boys 34%) and other legal responses more often for boys. Rehabilitative measures were more prevalent among younger adolescents, 75% of those aged 15 years, 71% of those aged 16 years and 64% of those aged 17 years.
Legal responses are determined in regard to the penalty value of the (drug) offence and with account taken of previous offences. Figure 1 shows that rehabilitative measures were more common in the two mixed-offender groups, 81% among first-timers and 74% among reoffenders, compared to 62% among the PLN only offender groups. Waiver of prosecution with formal caution was most prevalent among first-timers with PLN only offences (48%). Fine was most common in the PLN only offender groups (38%). Only 19% among first-timers with mixed offences received fine as a legal response. Youth care was more common among the mixed offender groups (first-timers: 49%; reoffenders: 41%). The results show that the more severe the situation (measured in differentiated and repeated offences), the more rehabilitative measures are included in the sentence.
Social services
Results from the social services file study (n = 189) showed that in 85% of the cases the police sent a report to social service adjacent to the time of the offence. Later in the legal process, the police or prosecutor sent a request in 98% of the cases asking for an opinion regarding the choice of rehabilitative measure from the social services.
The majority (n = 146) of the adolescents were already known to the social services before they were reported in relation to the index offence, girls to a higher degree than boys (84% compared to 75%). Three-quarters (75%) of the known adolescents had previously received, or were currently receiving, rehabilitative measures through social services, most often due to norm-breaking or antisocial behaviour, such as drug use (54%), criminality (44%) or school problems (39%). Girls had to a higher extent received rehabilitative measures than boys (82% versus 73%). All adolescents who had previously been convicted for criminal offences (n = 70) were known to social services. For one-quarter (25%), social services only knew about the adolescent based on previous notifications of concern.
For just over three-quarters of the adolescents (n = 143), the social services reported in its statement to the police or prosecutor that there was need of rehabilitative measures from the social service as a result of the index offence. Boys were more frequently reported in need of rehabilitative measures than girls (78% versus 67%). In just over 20% of the cases (n = 39), the assessment did not show a special need of rehabilitative measures, and for a few cases (n = 7), the implication of the assessment was unclear.
The most common justification for rehabilitative measures was that social services expressed concern about drug use, and where subsequent provision included further investigation of the extent of drug use and information about the risks associated with drug use. When the social services were more aware of the adolescent's drug use and other risk behaviours, the proposed intervention contained drug treatment or support. In 18% of the cases, the justification was that the adolescent already had ongoing rehabilitative measures (Figure 2).
One-fifth (n = 39) of the adolescent were assessed as not having further need of rehabilitative measures and more than half (n = 23) were previously known to social services. Almost all (n = 22) of the previously known adolescents had been notified due to their own behaviour, almost half due to drug use. At the time of the index offence, 20% (n = 8) had some type of ongoing rehabilitative measures, of which three received support for drug use (Figure 3).
The measure most often suggested was drug use assessment with brief intervention. This can be described as a time-limited intervention focusing on the adolescent's risk behaviour and drug use, with included drug tests, six to eight occasions within the same number of weeks. This was usually provided by a specialized outpatient clinic for young people with drug problems. More unusual were various types of programs or group activities that were focused on, for example, criminality or self-control. Every fifth measure proposed by social services in relation to the index offence was residential care.
A high percentage, almost four out of five adolescents, completed the rehabilitative measure described in the youth contract or in the care plan. The most common reason when dropping out was misbehaviour.
Intersection of conviction and health care
The justification for a judicial system that identify and ‘deliver’ young people to the social services could partly be assessed based on whether it detects individuals not already receiving adequate support elsewhere.
Figure 4 shows that only a small group of individuals convicted of drug offences in 2017 received drug-related health care the same year (girls 15%, boys 12%). However, 46% among boys who received drug-related health care in 2017 were convicted of drug offences the same year, thus more than four times the same proportion among girls (10%). This result probably mirrors gender differences in respect to number of drug convicts but could also indicate differences in help seeking behaviour. The proportion among boys convicted of drug offences were almost six times as high compared to girls (933 versus 164 per 100,000 inhabitants), while the proportion who received drug-related health care were about 1.4 times as high (363 compared to 256 per 100,000 inhabitants). Furthermore, girls had more often received drug-related health care than being convicted of drug offences (256 versus 164 per 100,000) while boys had more often been convicted of drug offences than received care (933 versus 363 per 100,000). There is no information on whether the interaction between drug-related health care and drug offences (the overlap between circles in Figure 4) is a result of the same event, either in connection with police intervention or rehabilitative measures from the social services after conviction. Of adolescents (15–17 years of age) receiving drug related health care in 2017 (blue circles in Figure 4), more than half (56%) were admitted due to harmful use of one or more types of psychoactive substances, while one fourth (25%) were admitted due to acute intoxication. The single most common diagnosis (41%) was harmful use of cannabinoids (F12.1). Less than 5 percent were admitted for drug rehabilitation and/or drug abuse counselling (Z50.3, Z71.5, Z72.2). Cannabinoids (F12) were more common among boys than girls (60% vs. 44%), multiple drugs (F19) were more common among girls than boys (29% vs. 19%) as well as sedatives or hypnotics (F13) (10% vs. 3%). Girls were more often than boys admitted due to acute intoxication (35% vs. 16%). Boys were more often admitted due to harmful use (57% vs. 43%). Approximately 8–9% of both girls and boys were admitted due to dependence syndrome.
Healthcare contacts with psychiatry and/or drug-related diagnosis
Figure 5 display the aggregated proportion of adolescents being in contact with the health care for assessment and/or treatment for mental, (neuro-) psychiatric or drug-related problems during the period 2014–2020. It is a composite measure based on (1) psychiatric diagnoses within inpatient or specialized outpatient care including care at psychiatric clinics without a diagnosis and/or (2) retrieval of prescribed psychotropic drugs. The psychiatric diagnoses also include drug-related diagnoses i.e., mental and behavioural disorders due to use of psychoactive substances (International Classification of Diseases [ICD]-10: F10–F19).
According to the composite measure, healthcare contacts with psychiatric and/or drug-related diagnosis were considerably more common in the study population compared to peers in the general population, both in the years before the index offence and in the years after the index offence, and especially among girls (Figure 5). Compared to the general population, the prevalence among girls in the offender groups were 4.9–6.6 times as high 3 years before the index offence (2014), 5.1–5.3 times as high in the year of the index offence (2017) and 1.9–3.6 times as high three years after the index offence (2020). The corresponding ratios among boys were 2.0–2.8 in 2014, 3.9–4.7 in 2017 and 2.2–2.9 times as high in 2020. Healthcare contacts among boys in the study population were more common in the reoffender groups compared to the first-timer groups in the years up to and including the year of the index offence. The difference between offender groups among girls were larger in the years after the index offence, where healthcare contacts with psychiatric and/or drug-related diagnosis were more common among the first-timer groups compared to the reoffender groups.
To some extent, the prevalence of healthcare contacts in the study population might have been a result of being caught by the police for a drug offence (e.g., health care in association with the arrest, or the social services referring to different types of health care assessments or treatments as a result of the arrest). This is also evident from the peak in the year of the index offence among all offender groups, and the somewhat higher rate with respect to healthcare contacts among reoffenders compared to first-timers in the years prior to the year of the index offence (Figure 5).
Over one-fifth (22%) of the girls had, before their first drug offence, a healthcare contact related to anxiety disorders and 10% had a healthcare contact for depression. Among boys, the proportions were substantially lower: 4% had a healthcare contact related to depression, and 5% for anxiety disorders.
Neuropsychiatric disorders were considerably more common in the study population than among comparable peers. About 35% of the girls had, before their first drug offence ever, a healthcare contact related to ADHD. The corresponding proportion was about 23% of the boys.
Recidivism
Within the follow-up period, 61% of the adolescents were reconvicted for new drug offences; more specifically, 64% of the boys and 39% of the girls.
Figure 6a displays the rate of reconviction of new drug offences within the follow-up period in the offender groups by sex. The rate of new drug offences was highest among boys convicted for mixed offences, especially among reoffenders. In the latter study group, half of the population was reconvicted for new drug offences within 18 months and, by the end of the follow-up period, 71% were reconvicted. The largest group, first-timer boys with only PLN, had the lowest reconviction rate for new drug offences: 33% were reconvicted after 18 months and 54% by the end of the follow-up period.
The reconviction rate for girls were lower than for boys in all offender groups. However, the offender groups of girls display the same pattern as for boys in that reoffender girls with mixed offences had the highest rate of reconvictions of new drug offences (55%) and debutants with only PLN with the lowest (29%). The offender group reoffender girls with only PLN is not shown in the figure due to low numbers.
Figure 6b takes a closer look at the largest offender group (i.e., first-timer boys with only PLN, where recidivism is studied in regards to age and legal response at index offence). Younger boys, aged 15 and 16 years, who received rehabilitative measures as legal response had lower reconviction rate compared to peers who received legal responses without such measures. However, the pattern differed among older boys (17 years old). During the first 2 years, there were no or small differences in reconviction rate, while the rate was reversed at end of follow-up (the third year) (i.e., the rate was higher among those who received rehabilitative measures compared to those who did not). The pattern remains and strengthens when adjusting for background factors; however, the differences were not significant at the 5% level. Among the background factors, “birth parents in- and/or outpatient care with drug related diagnosis” (hazard ratio = 1.55) and “not qualified for upper secondary education at exit from primary school” (hazard ratio = 1.54) had the strongest effect on recidivism among boys convicted of their first drug offence in 2017. Details are provided in supplemental Table S1.
Discussion
Minor drug offences at a young age may be an indication of a drug problem and a general criminalization of drug possession, including personal use, is thought to counter development of drug use in Sweden. This study investigated how the judiciary and social services succeed in identifying and providing support to adolescents convicted of offences against the Act on Penal Law on Narcotics (SFS 1968:64). Characteristics of 15–17-year-olds convicted in 2017 were examined using longitudinal register data, as well as those who receive rehabilitative measures as a legal response, and how these programs affect recidivism compared to other legal responses.
A first question to ask is whether adolescents reported to the social services need rehabilitative measures; if not, the need to identify them within the social services would be less legitimate. Proponents of the current policy might be calmed by the fact that just one-quarter of those assessed were considered as not in need. Adolescents who do not plead guilty or consent to participate are likely to be fined since compulsory measures are only relevant in the most serious cases, and this result is further strengthened by how the group convicted of drug offences distinguish in terms of vulnerability. In line with previous research (Anderberg et al., 2022), adolescents convicted of drug offences displayed a pronounced vulnerability compared to the general population. For example, only 48% of the sample qualified for upper secondary education compared to 83–84% in the general population. Out-of-home care before age 13 years was twice as common and mothers receiving social assistance when the child was 12–14 years old was almost three times as common compared to that in the general population
Next, even if adolescents convicted of drug offences are in more troublesome life situations, facilitating support from the social services via the judicial system would be more adequate if those reported were previously unknown to the system, at least regarding suspected drug use. Looking comprehensively at all those who are convicted, the great majority consists of those already known to the social services not only regarding drug use, but also because of other risk behaviours or difficulties (e.g., in school and/or their families). Nevertheless, the assessments initiated by the reports from the judicial system might provide an opportunity to reach groups with incipient or problematic drug use. The current findings reveal that social services to a large extent investigated and assessed the drug offences as serious risk factors for negative development and recidivism. More than three-quarters of adolescents were deemed in need of rehabilitative measures, typically targeting drug use, and a substantial group had not received a targeted drug intervention before.
Analysing healthcare data for the convicted group indicates that a potential new way forward for a large proportion of individuals would incorporate social and mental health support. A significantly higher percentage of the convicted adolescents had a healthcare contact related to mental health problems and/or neuropsychiatric disorders compared to their peers. This is in line with previous research indicating that a substantial percentage (50–90%) of young individuals facing drug and alcohol issues also encounter significant mental health challenges (Richert et al., 2020). These levels correspond to the composite measure presented in this study (Figure 5). Accordingly, many of the adolescents need rehabilitative measures from both social services and healthcare. In the present study, a notable peak in 2017 is evident in the composite measure, suggesting that convictions did result in an upswing in healthcare contact, followed by a decline in subsequent years. But there are differences between boys and girls, indicating that boys’ healthcare is more often linked to convictions, while girls seem to be more proactively seeking healthcare. Girls were also less frequently convicted of new offences compared to boys, despite exhibiting more risk factors. This discrepancy may be attributed to social services and healthcare being more adept at recognizing and addressing girls’ needs for support, particularly in cases of norm-breaking behaviour (Estrada et al., 2022).
For the system to work effectively, rehabilitative measures might have to merge even better with the healthcare system. However, there is limited knowledge on what constitute effective community-based outpatient treatment for drug using adolescents, especially in Swedish follow-up studies. Anderberg et al. (2021) show that two-thirds who start outpatient treatment for drug use problems had no indications of drug use 1 year later. This type of outpatient treatment, integrating social services and health care was the most common rehabilitative measure provided to adolescents in the present study. Sandøy et al. (2022) showed, in their study on first-time drug offenders in Norway, that rehabilitative measures provided by social services or health care, were more successful in preventing recidivism than fines. Around half of the population reoffended within 5 years.
Despite the fact that the vast majority of adolescents in the present study had no prior criminal convictions and received a rehabilitative measure as legal response, a considerable majority (61%) of the adolescents were reconvicted for new drug offences during the 3-year follow-up period. How can such a large proportion of recidivism be understood?
A general explanation for the rate of recidivism could be borrowed from labelling and biases in police practice. Drug offences involve police surveillance and intervention, and the adolescents convicted have been in an environment or situation noted by the police, and those once identified will more likely be observed more closely (Luthman, 2023). In the present study, being convicted for other crimes was almost as common as being convicted for drug offences only. A combination of criminal activities probably increases the likelihood of detection, impacting the legal response and subsequent outcomes; this is a group within the focus of society's surveillance lens. This suggests that adolescents convicted of drug offences do not necessarily represent the broader population of adolescents using narcotics.
Another explanation for the elevated recidivism rate among adolescents, especially among boys, may be linked to their heightened need for rehabilitative measures, a need not always adequately addressed within the legal system or through referrals. However, rehabilitative measures involving risk assessments or brief interventions may suffice for certain subgroups (e.g., first-time offenders with only a drug-related offence). This study indicates that younger boys, aged 15 and 16 years, who received rehabilitative measures had lower reconviction rate compared to peers who received legal responses without such measures. The finding is significant because it indicates that early interventions work (Carney & Myers, 2012), which is important since studies suggest that early drug use increases the risk of continued drug use and negative development (Rioux et al., 2018; Tillson et al., 2019; Trujillo et al., 2019).
The contrasting interests of proportionality and need are not easily reconciled. Our study reveals that the rehabilitative measures proposed by social services as a legal response have been adjusted in line with the penal law principle of proportionality. The design of rehabilitative measures cannot be overly extensive regarding time and complexity, especially for minor drug offences, which is a pecuniary penalty. In some cases, the penal value determines the limits of the rehabilitative measures given within the framework of a legal response, not corresponding to the possibly more comprehensive needs of the adolescents. The idea behind the system is that the legal response can serve as a pathway to necessary care (Albert et al., 2011; Caulkins et al., 2021), enabling the young person to be referred to more comprehensive measures outside the legal response. However, the system is far from perfect. It reasonably its intended group well reaches, but the high recidivism rate calls for that substantial improvements are needed, both in terms of follow-up upon treatment results and forming holistic support merging social and healthcare needs among adolescents at risk.
The strengths of the current study include the use of longitudinal register data covering all adolescents convicted of drug offences in 2017 and their parents, together with additional case file data from the social services. However, the case file data only cover a subsample of the adolescents (10%), which limits the possibility of generalizing on the decision process rendering different legal responses. In addition, the exclusive use of case file data on the decision process omitted other perspectives beside the social services. In the context of this research, ethical considerations focused on balancing individual privacy with the societal benefit of improved legal and social interventions. Although participants might feel uneasy about their data being used, the study's goal is to enhance knowledge about the target group, ultimately contributing to better rehabilitative measures and legal processes.
Conclusions
The findings underscore the interaction between the judicial system, social services and healthcare in addressing adolescent drug offences. While the current approach aims to provide rehabilitative measures proportional to the offence, high recidivism rates suggest a need for more tailored interventions. Despite efforts to identify and support at-risk adolescents, challenges remain in effectively addressing underlying mental health issues and coordinating holistic support. Motivating adolescents to engage in rehabilitative measures before they experience negative consequences of drug use can be challenging, given the early stage and that drug abuse has not yet developed. Moving forward, there is a critical need for improved follow-up procedures and a more integrated approach that bridges social and healthcare services. Ultimately, addressing the underlying factors contributing to adolescent drug offences requires a multifaceted approach that prioritizes early intervention, personalized support and collaboration across systems to promote positive outcomes and reduce recidivism rates.
Supplemental Material
sj-docx-1-nad-10.1177_14550725241295469 - Supplemental material for Rehabilitative measures as a legal response for adolescents convicted for drug offences: The Swedish system
Supplemental material, sj-docx-1-nad-10.1177_14550725241295469 for Rehabilitative measures as a legal response for adolescents convicted for drug offences: The Swedish system by Johan Glad, Marie Berlin, Olof Bäckman, Torbjörn Forkby and Gunnel Hedman Wallin in Nordic Studies on Alcohol and Drugs
Footnotes
Acknowledgements
We are grateful to all representatives of the social services in the included municipalities for their help to retrieve the substantial amount of documentation used in this study.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Ethical approval
The study was approved by the Swedish Ethical Review Authority 2019-05810 and 2021-03549.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Swedish National Board of Health and Welfare and the Swedish Ministry of Health and Social Affairs.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.