
Abstract
Illicit drug use is a considerable health problem worldwide, especially the illicit use of opioids (Degenhardt et al., 2013; United Nations Office on Drugs and Crime, 2023). In 2021, an estimated 60 million people worldwide used illicit opioids (United Nations Office on Drugs and Crime, 2023). In Germany, 0.31% of the population aged 15–64 years were estimated to consume illegal opioids (Kraus et al., 2019).
Opioid addiction is overrepresented in the prison setting. In Germany, an estimated 8% of incarcerated persons experience opioid addiction (Länderarbeitsgruppe “Bundeseinheitliche Erhebung zur stoffgebundenen Suchtproblematik im Justizvollzug”, 2022).
Incarceration can lead to drug-related risk behaviour, e.g., syringe sharing (Milloy et al., 2009). Given the spiral of addiction, crime and incarceration, evidence-based and effective treatment for incarcerated individuals with opioid addiction is particularly important. This is especially true as people who are freshly released from prison are at extreme risk of relapse and overdose during re-entry into the community (Farrell & Marsden, 2008; Krinsky et al., 2009; Merrall et al., 2010).
Opioid substitution treatment
Opioid substitution treatment (OST), which involves replacing illicit opioids with medically prescribed opioids, is considered the standard treatment for opioid addiction in many parts of the world (European Monitoring Centre for Drugs and Drug Addiction, 2022). In addition to reducing the use of illicit opioids, OST aims to improve the health of those affected, reduce involvement in criminal activity and reduce the use of other illicit substances (Bundesärztekammer, 2023). There are numerous studies on OST for opioid addiction that have demonstrated positive effects on illicit opioid use, health status and social integration (MacArthur et al., 2012; Pierce et al., 2016; Wittchen et al., 2011).
OST is now also offered in prisons in most European countries (European Monitoring Centre for Drugs and Drug Addiction, 2022). This also applies to German prisons, where the number of incarcerated persons in OST has increased from 24% in 2018 (Drogenbeauftragte der Bundesregierung, 2019) to 46% in 2022 (Länderarbeitsgruppe “Bundeseinheitliche Erhebung zur stoffgebundenen Suchtproblematik im Justizvollzug”, 2022).
Research on OST
Illicit use of opioids and other substances
Reducing illicit opioid use is one of the main objectives of OST. Some studies confirm a reduction in heroin use with substitution treatment in non-prison populations (Amato et al., 2005; Gossop et al., 2003; Johansson et al., 2007; Mattick et al., 2009). Corresponding results can be shown for the situation during imprisonment. Two reviews report reductions in illicit opioid and injecting drug use among incarcerated individuals in OST (Hedrich et al., 2012; Sharma et al., 2016). Two meta-analyses report similar results for the period after release from prison. (Boksán et al., 2023; Moore et al., 2019). However, the study base in both meta-analyses was small and the results heterogeneous.
OST may also help reduce benzodiazepine or crack cocaine use (Boksán et al., 2023; Gossop et al., 2003). Nevertheless, there are several studies that show no differences between OST-receivers and non-receivers regarding other illicit drug use, both in the community (Betts et al., 2016; Gjersing & Bretteville-Jensen, 2013) and in prison or after release (Brinkley-Rubinstein et al., 2018; Hedrich et al., 2012).
In addition to the illicit substances mentioned above, prescription drugs, particularly substitution drugs such as methadone or buprenorphine, are also misused, in freedom (Bretteville-Jensen et al., 2015; Johnson & Richert, 2019; Piispa et al., 2022; Prami et al., 2023; Roche et al., 2008; Vlahov et al., 2007) as well as in prison (Franchetti et al., 2023). Some studies report a decrease in non-prescription use of opioid substitution medication by OST (Gossop et al., 2003; Roche et al., 2008; Schulte et al., 2016). However, further studies showed an increased use of non-prescribed methadone and buprenorphine during OST (Aitken et al., 2008; Best et al., 2000).
The studies on non-prescription use of opioid substitution medication during OST only consider the community situation; there are no results for the prison context. In addition, due to weak study designs (i.e., lack of control group), the evidence is limited and the research situation remains unclear.
Craving and opioid withdrawal symptoms
OST is expected to reduce opioid withdrawal symptoms and opioid craving (European Monitoring Centre for Drugs and Drug Addiction, 2022; Havnes et al., 2013; Kastelic et al., 2009; Moratti et al., 2010). Two studies reported reduced opioid withdrawal symptoms and reduced craving as benefits of OST in prison (Johnson et al., 2001; Sindicich et al., 2016), but there have been few studies on this topic.
Treatment and overdoses after release
Release from prison is associated with increased risk of fatal overdose (Farrell & Marsden, 2008; Kalsås et al., 2023; Krinsky et al., 2009; Merrall et al., 2010). Two systematic reviews report lower post-release mortality rates in individuals who received pre-release OST (Crowley & van Hout, 2017; Malta et al., 2019), whereas Hedrich et al. (2012) showed no clear evidence of a reduction in fatal post-release overdoses for persons receiving OST in prison. Bird et al. (2015) showed a reduction in drug-related deaths in the first 12 weeks after release with OST in prison, but no differences were seen in the first 14 days after release. OST may also reduce non-fatal overdoses after release from custody (Betts et al., 2016; Malta et al., 2019), although the results are inconsistent. Crowley and van Hout (2017) concluded in their systematic review that there is insufficient evidence for a reduction of non-fatal overdoses in individuals receiving OST.
Continuity in OST appears to be an important factor in health status, illicit opioid use, re-incarceration and social integration (Dolan et al., 2005; Hedrich et al., 2012; Malta et al., 2019; Stallwitz & Stöver, 2007). People experiencing opioid addiction who receive OST in prison are more likely to be in treatment after their release (Boksán et al., 2023; Brinkley-Rubinstein et al., 2018; Crowley & van Hout, 2017; Hedrich et al., 2012; Malta et al., 2019; Moore et al., 2019; Sharma et al., 2016).
Current study
Most studies, so far, come from the USA or other English-speaking countries. A systematic database search as part of a research project yielded 15 studies of people who are incarcerated undergoing OST that evaluated and reported data on drug use after prison release. Of these 15 studies, only three were conducted outside the USA (one in Australia (Dolan et al., 2003), one in Canada (Johnson, 2001) and one in Norway (Lobmaier et al., 2010) (Boksán et al., 2023)). The dominance of US studies raises the question of the extent to which the results are transferable to Europe, and to Germany in particular, given the differences in the justice system, social welfare and health insurance.
The aim of this article was to compare data on individuals with opioid addiction receiving intramural OST with those not receiving OST in the German federal state of Bavaria. In this longitudinal study, we evaluated intramural OST in prison and after release. Our hypotheses are:
Prison-based OST reduces illicit opioid use, overall illicit drug use, opioid craving and opioid withdrawal symptoms during prison sentence. Prison-based OST reduces illicit opioid use, overall illicit drug use, opioid craving, opioid withdrawal symptoms and drug overdoses up to 6 months after release from prison. Prison-based OST increases likelihood of post-release treatment.
Materials and methods
Design and procedures
This article is part of a multicentre observational study conducted in Bavarian state prisons funded by the Bavarian Ministry of Justice. The overall aim of this multicentre study was to examine the effects of OST versus no OST for incarcerated individuals experiencing opioid addiction on their behaviour in prison, as well as health status, addiction relapse, legal probation and social integration after release. This article focuses on substance relapse and substance-related variables.
Diagnosing opioid addiction (according to ICD-10) was the responsibility of prison hospital departments. The treatment decision (OST/no OST) was made by the medical staff at the beginning of the sentence in consultation with the incarcerated individuals. This happened completely independently of participation in the study. The assignment to the treatment or control group (OST vs. no OST) in the study was based on the treatment decision made in advance; the research team consisting of psychologists had no influence on the treatment. Randomisation of participants to different treatments was not ethically justifiable, as the refusal of substitution treatment by prisons constitutes a violation of Article 3 of the European Convention on Human Rights (prohibition of torture, see European Court of Human Rights in the case Wenner versus Germany from 1 September 2016).
Participants in the control group had access to the same medical and social services as those in the treatment group (e.g., addiction counselling) but did not receive OST (they received an abstinence-oriented treatment instead).
All incarcerated persons who were aged at least 18 years and who had spent at least 3 months in Bavarian penal sentence and were due to be released shortly (time between interview and release: M = 8.96 weeks, SD = 13.59), were eligible to participate in the study. In addition, opioid addiction had to have been medically diagnosed. Multiple drug use was not an exclusion criterion if an opioid addiction was diagnosed. Another participation criterion was a sufficient ability to speak and understand the German language to participate in an interview, as no interpreter was available.
Participants were interviewed at four measurement times: T0 took place in prison, shortly before release; T1 followed approximately 1 month after release (M = 5.57 weeks, SD = 2.63); T2 3–6 months (M = 16.83 weeks, SD = 6.54); and T3 12 months after release (M = 54.73 weeks, SD = 13.29). In the present study, data from T0, T1 and T2 were used.
Participation was voluntary, but incentives were given in the form of a packet of coffee (in prison) or supermarket vouchers after release (T1: €50 voucher value, T2 and T3: €100 voucher value each).
Recruitment took place in the prison. Contact persons informed eligible individuals about the study and, if interested, arranged an interview appointment. Written informed consent was obtained before the first interview. The participants were assured of the confidentiality of the project team towards the correctional facilities. Participants were asked to provide reliable contact details for follow-up interviews after release from prison. At T0, interviews were conducted either in person in prison, or, due to the COVID-19 pandemic, by telephone. The interviews were generally conducted in rooms without acoustic monitoring. Follow-up interviews were conducted by telephone.
The study protocol was assessed positively by the ethics committee of the Friedrich-Alexander-Universität Erlangen-Nürnberg, the data protection concept was approved by the data protection officer of the Friedrich-Alexander-Universität Erlangen-Nürnberg.
Survey instrument
A validated standardised interview procedure, the European Addiction Severity Index (EuropASI) (Gsellhofer et al., 1997; McLellan et al., 1992) was used to collect self-reports. A version adapted to the prison conditions was used for the incarceration interview (T0); a shortened but otherwise largely unchanged version of the EuropASI was adapted for the post-release follow-up interviews (T1, T2). The adapted semi-structured interview collects data from persons with addiction problems in seven independent problem areas: general information; physical condition; work situation; alcohol and drug use; legal situation; family and social relationships; and mental status.
Data included in this paper were part of the “alcohol and drug use” section of the EuropASI, which examines age at first drug use, years of usage and current use for various substances by asking “What drugs/substances have you ever used/since the last interview?” Questions about opioid craving, opioid withdrawal symptoms (physical complaints, e.g., nausea, sweating), overdoses and substitution treatment were included in this section. Questions about OST were also added (e.g., “Are you currently receiving OST?”).
For each domain, there were dichotomous questions (e.g., “Are you currently receiving OST?”) and rating questions, each addressing the distress or impairment caused by problems in that domain (e.g., “How much have your drug problems bothered or affected you in the last 30 days?”). These rating questions were answered by the participants using a 5-point Likert scale.
All incarceration information (T0) referred to outcomes like drug use, craving and opioid withdrawal symptoms during the incarceration period in which the first interview took place. The data from follow-up points T1 and T2 refer to outcomes (drug use, craving, opioid withdrawal symptoms, overdoses) since the previous interview and to the current substitution status at the time of the interview.
Sample description
The survey period was scheduled between February 2020 and May 2022. Prisoners from 20 Bavarian correctional facilities participated. For the baseline interview (T0, in custody), the sample consisted of 247 participants. In the baseline sample, nOST = 139 (56%) were in OST, while nnoOST = 108 (44%) were not receiving OST at the time of the first interview. Additional sample characteristics are listed in Table 1.
Baseline data.
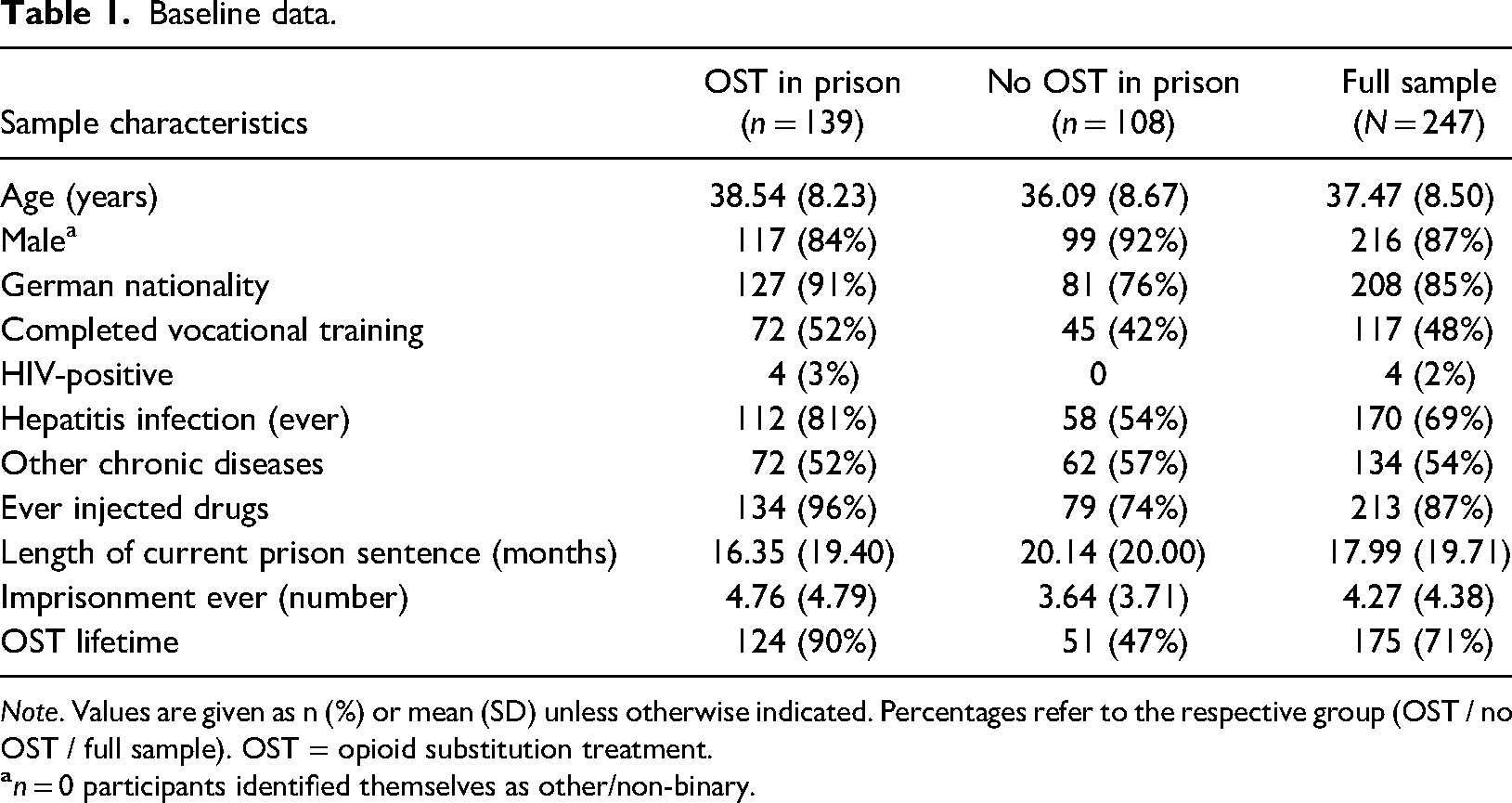
Note. Values are given as n (%) or mean (SD) unless otherwise indicated. Percentages refer to the respective group (OST / no OST / full sample). OST = opioid substitution treatment.
The most often prescribed substitute in prison was levomethadone (27% of OST patients), followed by methadone (16%), buprenorphine depot (10%) and buprenorphine (7%). Morphine (2%) and a combination of buprenorphine and naloxone (1%) were rarely used.
After release, we obtained information from 72% of the baseline sample. There was no systematic dropout in the grouping variable (dropout rate 25% of the participants in the OST group (n = 35) and 32% of the participants in the non-OST group (n = 34); χ²(1) = 1.20, p = .274). For more information about the participants at each follow-up point, see Table 2. Most participants who dropped out of the study could not be contacted again because they did not provide enough contact information in prison or the contact information was incorrect (e.g., invalid mobile phone number, email address or postal address). Only five participants actively refused further participation after release.
Sample sizes at follow-up T1 and T2.

Note. Values are given as n (%). Percentages refer to the respective group (OST at baseline in prison / no OST at baseline in prison / full sample at baseline in prison). OST = opioid substitution treatment.
Statistical analysis
Data were analysed using SPSS 29. Due to the level of the data, group comparisons were calculated using χ² tests or the Fisher–Yates test. The effect size is indicated by odds ratio (OR), whereby an OR >1 indicates a benefit for the treatment group.
Intent-to-treat vs. as treated
After release from prison, not all participants continued the OST they had started in prison, and others began the OST after their release even though no OST was started in prison. Therefore, there were some “changeovers” between the groups. To account for this, both intent-to-treat and as-treated analyses were performed (Shrier et al., 2014).
For the as-treated analyses, individuals were investigated as part of the group to which they belonged at the time of the respective follow-up. For example, a participant who had not received OST in custody but had started treatment after release before follow-up time point T1 was considered part of the OST group at follow-up point T1. Although this reflects the actual treatment situation, distortions are possible (Endres et al., 2016; Hollis & Campbell, 1999). Therefore, intent-to-treat analyses were also conducted, taking into account the distribution of participants in prison at the first measurement time point, regardless of whether treatment was discontinued or restarted after release. This corresponds more to the practical care situation, even though an underestimation of treatment effects is possible (Endres et al., 2016).
Inverse probability of treatment weighting (IPTW)
For ethical reasons, randomisation to treatment and control group was not possible, so differences between the two groups at baseline may limit the interpretability of the results. To control for these potential confounding factors, inverse probability of treatment weighting (IPTW) was applied, which is recommended for non-randomised group assignment (Austin, 2011; Chesnaye et al., 2022). Possible differences between the treated and non-treated group have been identified in the literature (Chesnaye et al., 2022). Women appear to be more likely to receive treatment than men (European Monitoring Centre for Drugs and Drug Addiction, 2022; Länderarbeitsgruppe “Bundeseinheitliche Erhebung zur stoffgebundenen Suchtproblematik im Justizvollzug”, 2022; von Bernuth et al., 2020). Furthermore, OST participants appear to be older (von Bernuth et al., 2020) and to have a more severe addiction history, e.g., more intravenous drug use (Weiss et al., 2022). These differences were similar in our sample (gender: χ²(1) = 3.11, p = .078; age: t(245) = −2.26, p = .024; intravenous drug use: χ²(1) = 26.52, p < .001) (see Table 1), whereas no group differences were found for other variables (e.g., nationality, completed vocational training, chronic diseases other than hepatitis, number of previous prison sentences). The variables “gender”, “age” and “intravenous drug use” were entered into a logistic regression model as predictors. This was used to calculate propensity scores, i.e., the probability of a study participant being included in the treatment group. OST participants who had a low probability of being included in the treatment group were given a higher weighting, and vice versa. To prevent extreme weighting values from inflating the confidence intervals and the variance of the effect estimate, weight stabilisation was performed (Chesnaye et al., 2022). Both outcomes, unweighted and weighted, are reported for the intent-to-treat analysis and are labelled accordingly.
Results
Descriptive statistics
Drug use in prison
Of the sample, 48% used at least one illicit substance during their current incarceration. The most frequently used illicit substances were cannabis (19% of the sample reported having used it at least once), synthetic cannabinoids (16%), opioids (except heroin, methadone or buprenorphine; mostly fentanyl, 16%), heroin and buprenorphine (14% each), benzodiazepines (13%) and cocaine (6%).
Drug use after release
Of the sample, 88% reported illicit use of at least one substance throughout the follow-up period. The most frequently used illicit substances were cannabis (63% of the sample reported having used it at least once), heroin (59%), cocaine (36%), benzodiazepines (28%) and crystal meth (24%).
Mortality
One death was known in the entire sample at T2.
Hypothesis testing
Intent-to-treat analyses
Participants who received OST in prison were less likely to use illicit opioids and illicit substitution medication (T0 and T2), they reported less craving (T0, T1 and T2) and were more likely to be in treatment after release (T1 and T2) than participants who did not receive OST (see Table 3).
Intent-to-treat analyses.
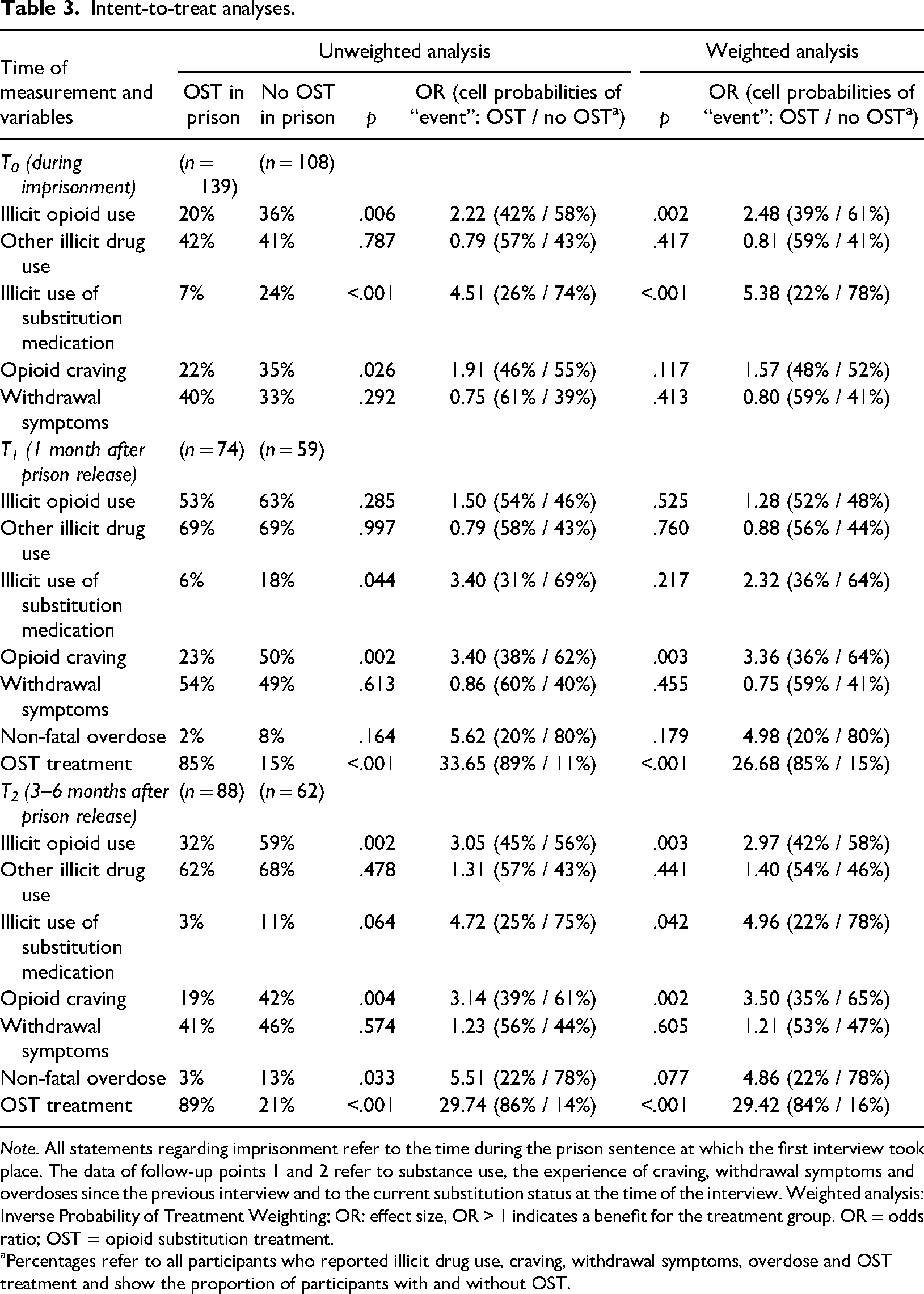
Note. All statements regarding imprisonment refer to the time during the prison sentence at which the first interview took place. The data of follow-up points 1 and 2 refer to substance use, the experience of craving, withdrawal symptoms and overdoses since the previous interview and to the current substitution status at the time of the interview. Weighted analysis: Inverse Probability of Treatment Weighting; OR: effect size, OR > 1 indicates a benefit for the treatment group. OR = odds ratio; OST = opioid substitution treatment.
Percentages refer to all participants who reported illicit drug use, craving, withdrawal symptoms, overdose and OST treatment and show the proportion of participants with and without OST.
As-treated analysis for follow-ups 1 and 2
Again, participants receiving OST were less likely to use illicit opioids (T2) and substitution medication (T1 and T2) and reported less craving (T1 and T2) than participants who did not receive OST (see Table 4).
As-treated analyses.
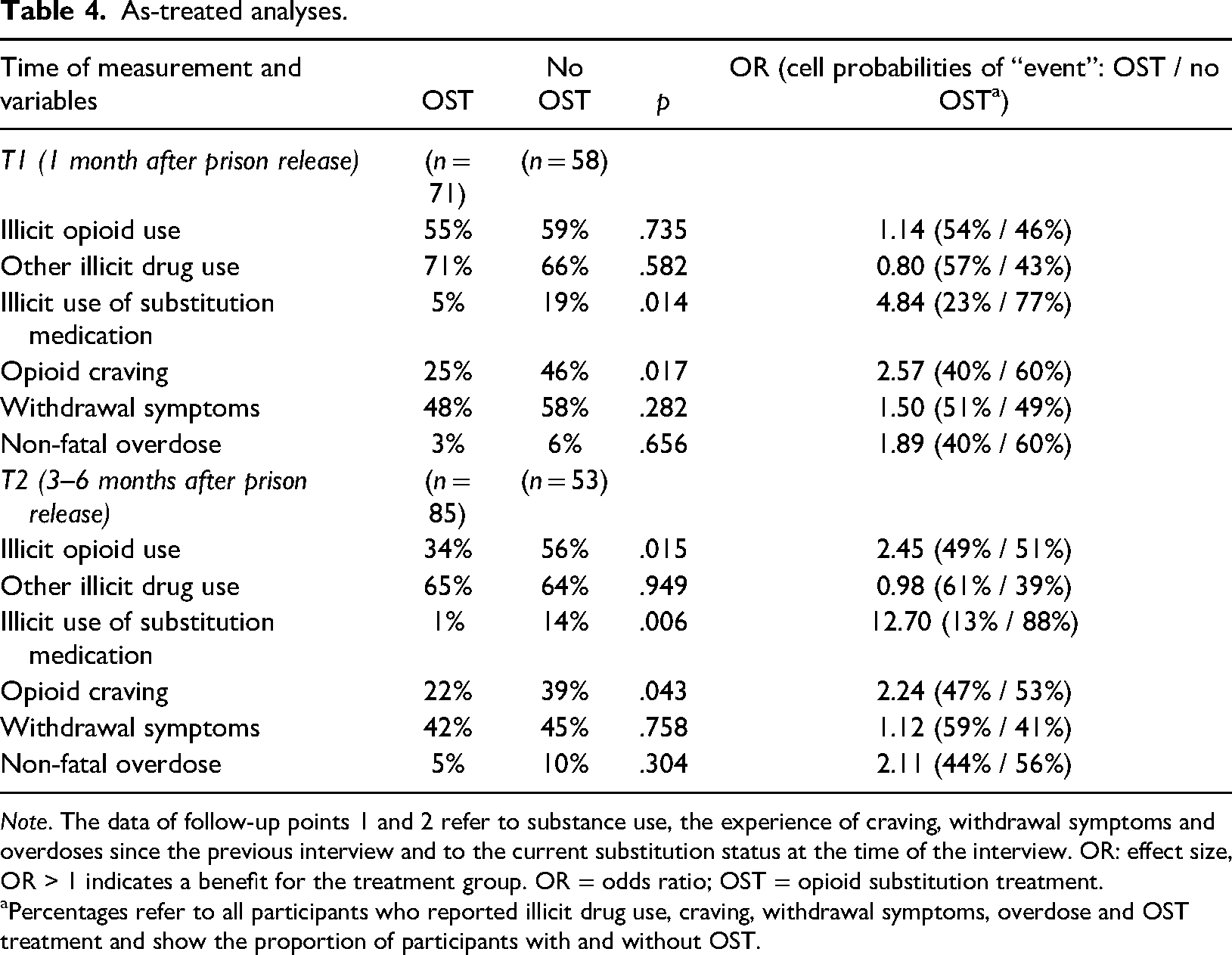
Note. The data of follow-up points 1 and 2 refer to substance use, the experience of craving, withdrawal symptoms and overdoses since the previous interview and to the current substitution status at the time of the interview. OR: effect size, OR > 1 indicates a benefit for the treatment group. OR = odds ratio; OST = opioid substitution treatment.
Percentages refer to all participants who reported illicit drug use, craving, withdrawal symptoms, overdose and OST treatment and show the proportion of participants with and without OST.
Discussion
Summary and integration of the results
During incarceration (T0), participants who received OST reported using less illicit opioids and less illicit substitution medication than those who did not receive OST.
One month after prison release (T1), the intent-to-treat analysis showed less opioid craving and higher treatment rates for the group that received OST in prison. In the as-treated analysis, participants who received OST used less illicit substitution medications and reported less opioid craving than those who did not receive OST.
Three to six months after release (T2), the intent-to-treat analysis showed group differences in illicit opioid use, use of illicit opioid substitution medications, opioid craving and treatment rates, with more positive results for the OST group. In the as-treated analysis, lower illicit opioid use, illicit substitution drug use and less opioid craving were observed in the OST group.
Opioid use
The lower rates of illicit opioid use reported by the OST group compared to the non-OST group in the present study are consistent with the existing literature for the prison setting (Hedrich et al., 2012; Sharma et al., 2016) and after release (Boksán et al., 2023; Brinkley-Rubinstein et al., 2018; Moore et al., 2019). After prison release, this effect only became apparent at the 3–6-month follow-ups. Release from prison and thus the transition from a structured daily routine to a self-determined daily life in the community is a particularly vulnerable and difficult time (Jamin et al., 2021), which can promote a relapse in the period up to 1 month after release. Stabilisation of living conditions in freedom combined with stable OST could have a positive impact on reducing opioid use over time (T2, 3–6 months after release).
Another factor influencing illicit opioid use is the dosage of the substitution medication (Amato et al., 2005; Hedrich et al., 2012; Mielau et al., 2021; Ward et al., 1999), which may vary during substitution treatment, leading to illicit opioid use despite OST. Unfortunately, we did not obtain reliable information about medication dosage in our study. Future studies should pay attention to assess medication dosage more precisely.
Other illicit drug use
The results of the present study are not consistent with those of Boksán et al. (2023) and Gossop et al. (2003), who reported a decrease in illicit use of other substances during OST. In the present study, the OST group was as likely to use illicit non-opioid drugs as the non-OST group. This supports the results of previous research on the situation in freedom (Betts et al., 2016; Gjersing & Bretteville-Jensen, 2013), in prison or after release (Brinkley-Rubinstein et al., 2018; Hedrich et al., 2012).
Overall, it remains questionable whether a decrease in the use of non-opioid substances can be expected through OST, although some guidelines suggest this (Bundesärztekammer, 2023). Substitution drugs are intended to activate opioid receptors, preventing the effects of illegally taken opioids and opioid withdrawal symptoms (Veilleux et al., 2010). This does not directly target the addiction of other substances. Although opioid addiction is often associated with comorbid disorders and addiction on other substances (Strain, 2002), from a pharmacodynamic perspective it seems questionable whether OST will lead to a reduction in the use of other illicit substances.
Illicit use of opioid substitution medication
To date, there are no known studies regarding the illicit use of substitution medication among incarcerated individuals. In the present study, participants receiving OST reported less illicit use while in prison and at T1 and T2, with differences between the unweighted and weighted analyses at T1 and T2. When analysed as treated, significant group differences were found for T1 and T2. This confirms the results of some studies in the extramural setting (Gossop et al., 2003; Roche et al., 2008; Schulte et al., 2016).
Opioid craving and withdrawal symptoms
Participants who received OST reported less opioid craving than those in the non-OST group at the first and second follow-ups, which is consistent with the findings by Johnson et al. (2001) and Sindicich et al. (2016). The doses administered in prison can sometimes be lower than in the community (Kastelic et al., 2009), which may account for the inconsistent results (unweighted vs. weighted analysis) regarding craving levels between the two groups during imprisonment.
In contrast to previous studies (Havnes et al., 2013; Moratti et al., 2010), the current study found no group differences in opioid withdrawal symptoms reported by participants. Again, the dose of the substitution medication may be relevant (Werner, 2007). For organisational reasons, our study neither recorded the exact doses of the opioid substitution medication nor differentiated between the different substitution medications. Therefore, the exact reasons for the withdrawal symptoms and opioid craving in the OST group remain unclear. However, the similar levels of opioid withdrawal symptoms in both groups suggest that the use of OST to treat opioid withdrawal symptoms (European Monitoring Centre for Drugs and Drug Addiction, 2022) is not yet fully successful.
Non-fatal overdoses and treatment at follow-up
In contrast to the findings of Betts et al. (2016) and Malta et al. (2019), in the current study there was only a trend towards fewer non-fatal overdoses in the prison OST group, but odds ratios greater than 1 indicate an advantage for the OST group at T1 and T2 (intent-to-treat analyses). Crowley and van Hout (2017) concluded in their systematic review that there was insufficient evidence of a reduction in non-fatal overdoses. As with opioid withdrawal symptoms, it is possible that the substitution drugs administered are relevant. In the study by Betts et al. (2016), most non-fatal overdoses occurred in the group of individuals who did not receive OST but were frequent methadone users. Other factors, such as age, education, homelessness or the use of other substances, also appear to be associated with non-fatal overdoses (Bretteville-Jensen et al., 2015).
The consistently higher treatment rates at follow-up in the prison OST group compared to the prison non-OST group in the present study at both follow-up time points are consistent with previous studies (Boksán et al., 2023; Brinkley-Rubinstein et al., 2018; Crowley & van Hout, 2017; Hedrich et al., 2012; Malta et al., 2019; Moore et al., 2019; Sharma et al., 2016).
Limitations
There are some limitations to the results described. Randomised assignment of the participants to the treatment and the control group was not possible. Although we adjusted for possible a priori group differences using IPT weighting, it cannot be ruled out that there are further group differences between the treatment and control groups.
Another limiting factor is the number of study dropouts at the follow-up times. Study dropout does not appear to be systematic and there are no differences between the treatment and control group. However, it is possible that there are differences in illicit drug use or other variables between those who dropped out and those who remained in the study.
In addition, all results described are based on self-reports by the participants. It is therefore conceivable that the given reports of drug use were not always completely true, even if there was no evidence of socially desirable answers and the participants did not have to fear negative consequences for their statements. The original plan was to objectify participants’ reports of drug use by collecting saliva samples at each measurement point, but this could not be done consistently due to the COVID-19 pandemic. Additionally, the research team did not verify information on overdose (e.g., by asking medical staff), instead asking participants to rate whether they had experienced a drug overdose since the last interview.
Conclusion
Opioid addiction in prison and after release is an important research topic because of the far-reaching consequences for those affected and for society. Future research should combine participants’ self-reports with objective data, such as drug screenings, and consider additional moderating factors of the opioid substitution treatment itself (drug substances, dosages) as well as other moderating variables (e.g., social integration, employment).
Prison-based OST appears to have a significant impact on illicit opioid use in prison and after release, and increases treatment rates after release, which may be a protective factor. Some results still remain unclear, especially for the first follow-up time point 1 month after release. The risk of overdose is particularly high during this period, which is why the high consumption rates in both the OST and the control group are worrying. In addition to OST, there appear to be other factors that lead to increased use regardless of treatment. These variables may be of particular relevance and should be identified in future research. Nevertheless, given the high risks associated with opioid addiction, any reduction, as shown in the current study for use in prison and 3–6 months after release, is positive – especially as there are no significant disadvantages for the OST group at any of the measurement points.
Footnotes
Data availability statement
Research data cannot be shared due to privacy or ethical restrictions.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Bayerisches Staatsministerium für Justiz.