
Abstract
Keywords
Background
Excessive alcohol use causes a wide range of illnesses that have consequences both at a personal and societal level (WHO, 2018b). In Denmark, new estimates show that nearly 10% (n = 401,682) of the adult population has moderate alcohol problems and approximately 67,000 people are estimated to have severe alcohol problems (SIF, 2023). Approximately 2% of all Danish hospital contacts are alcohol related (SST & SSI, 2015). In 2013, there were 131,264 alcohol-related contacts registered in the hospitals (SSI & SST, 2015) and it has been found that 17% of patients in somatic wards scored >8 with the AUDIT screening tool (equivalent to hazardous use or above) (Schwarz et al., 2019). The prevalence of alcohol use in Danish emergency departments (EDs) is unknown, but a study from the UK has shown that 40.1% of patients exceeded this limit (Drummond et al., 2014). In 2018, 17,583 people were in public treatment for alcohol dependency (Sundhedsdatastyrelsen, 2020), and 20% were referred from either a somatic or psychiatric hospital (Schwarz et al., 2018). These numbers leave a considerable treatment gap. Furthermore, it is known that the time lapse between onset of the alcohol problem and treatment is 10–18 years (Chapman et al., 2015; Kessler et al., 2001); therefore, it is crucial to shorten this period and explore possibilities for better cross-sector collaborations and referral practices to ensure more people enter treatment earlier. Of admitted patients in an ED, 68% are discharged directly to their home without being hospitalised to a specialty ward (AHH). This means that ED settings play a key role in the cross-sectoral collaboration and are an important venue for preventive measures in at-risk patient groups.
Screening, Brief Intervention and Referral to Treatment (SBIRT) is one of the most examined preventive public health models intending to bridge the detection of alcohol problems in non-treatment seeking populations to specialty treatment services (SAMHSA, 2011). For a successful implementation, the literature calls for “seamless transitions” and strong referral networks in the “Referral to Treatment” (RT) component of SBIRT (Del Boca et al., 2017; Madras et al., 2009; SAMHSA, 2011, 2013). However, evidence is lacking that the BI component is effective in linking individuals to specialty treatment (Glass et al., 2015; Kim et al., 2017; Schwarz et al., 2019). In addition, the RT component itself is also understudied (Berger et al., 2017; Cucciare & Timko, 2015; Glass et al., 2017), as it is often not the primary outcome in randomised controlled trials (RCTs) within this field (Glass et al., 2015). Thus, its effectiveness is therefore questionable (Glass et al., 2015; Saitz, 2015). Barriers to SBIRT have been reported at patient, provider and system levels (Broyles et al., 2012; Cucciare & Timko, 2015; Gargaritano et al., 2020; Johnson et al., 2011). Although patient barriers mainly are connected to shame and stigma entering treatment (Farhoudian et al., 2022; Finn et al., 2023), a review of provider barriers in-hospital found personal discomfort, lack of knowledge, and time and resources being some of the most frequent barriers (Gargaritano et al., 2020). Further, the responsibility for addressing problematic alcohol use has been problematised by nurses, suggesting other specialised professionals to intervene and handle alcohol problems (Broyles et al., 2012). However, many of these studies reflect either the setting of primary care or different somatic hospital wards, are focused on all SBIRT components (with minor focus on the “RT” part) or consist of surveys.
At the system level, cross-sector collaborations and continuity in patient trajectories have been pivotal topics in healthcare for decades, but the complex nature of the required coordination to accomplish this still causes numerous challenges and is found inadequate (Seemann & Gustafsson, 2016; WHO, 2018a). In general, literature on cross-sector collaborations in other areas of healthcare has shown difficulties in transitions and communication, and the supposedly two collaborative sectors have been described as “two worlds” (Coleman & Berenson, 2004; Petersen et al., 2019) with their different culture, including goals and motivators. Further, the conditions for collaboration are not always supported by the underlying organisational structures (Høgsgaard, 2016; Kousgaard et al., 2019). Knowledge of integrated care and collaborative models supporting a cross-sector trajectory are comprehensive and diverse (WHO, 2016). However, it is not always possible to transfer a collaborative model that works in one setting into another (VIVE, 2018). This could be due to contextual factors and the fact that interventions need to be adapted or tailored to the local context (Kirk et al., 2021; Waltz et al., 2019; Wensing et al., 2011). In implementation science, examining context from micro to macro levels in a pre-implementation phase is highlighted in determinant frameworks, since it impacts implementation outcomes and degree of success, and can generate more implementable solutions to a long-standing problem (Nilsen & Bernhardsson, 2019).
To sum up, only few patients who need treatment are referred from hospitals to alcohol treatment. Further, the referral-to-treatment (RT) component of SBIRT is the least studied, and cross-sector collaborations and contextual factors as determinants for implementation are understudied qualitatively between EDs and municipalities. Seemingly, alcohol treatment pathways are challenged, and the aim of the present study was to examine both sector perspectives mutually to get a better understanding to improve and design sustainable cross-sector collaborations.
Aim
The aim of the present study was to examine perceptions of existing cross-sectoral collaborations regarding patients with alcohol problems from healthcare professionals’ perspectives in an ED and two associated municipalities. With this approach we can explore possibilities for future cross-sectoral interventions aimed at patients with alcohol problems.
Research questions
How are cross-sector collaborations regarding patients with alcohol problems experienced in an ED and in municipal alcohol treatment centres, respectively?
Which challenges occur – and how are they managed – in the cross-sectoral work?
Methods
Setting
The healthcare system in Denmark is tax-financed with free and, in principle, equal access for all citizens. The healthcare system works at three levels: national; regional (n = 5); and municipal (n = 98). Hospitals are governed by the regions and are responsible for somatic and psychiatric hospital treatment and care. The municipalities are responsible for preventive healthcare initiatives (such as dental services for all children aged <18 years, healthcare centres/clinics, family nursing, etc.), rehabilitation, home care services and nursing homes. In relation to alcohol, since 2007 according to §141 of the Danish Health Act (Indenrigs- og sundhedsministeriet, 2019), the treatment and prevention of alcohol problems are overall a responsibility of the municipalities, while hospitals are responsible for the acute alcohol-related hospitalisations, such as severe detoxifications, withdrawal symptoms and alcohol-related co-morbidity. With the responsibility distributed among multiple municipalities, national quality standards for treatment have been called for, since a huge variation in provided quality and staff competences was found in a recent comparison (SST, 2019).
The present study was conducted in an ED at a university hospital in the Capital Region and in two municipalities. The hospital covers an area of approximately 500,000 citizens and collaborates with 10 municipalities in the uptake area. The ED receives nearly 200 patients daily and almost 70% of them are discharged directly from the ED, without entering a specialised inpatient unit (AHH).
A function relevant for this study is the “social nurse”, originating in Denmark in 2006, and currently 1–2 social nurses are employed at each hospital in the Capital Region (Dideriksen et al., 2019). Social nurses are registered nurses (BA level, 3.5 years) with preferably more than 5 years of experience with the target group. They are considered specialists and the majority also hold a higher academic degree, such as a Master's degree. Social nursing is based on the principles of harm reduction with a holistic and health-related approach (Dideriksen et al., 2019). The aim of social nursing is to reduce inequalities for socially marginalised patients with diverse health-related problems, such as homelessness, multi-morbidity, severe alcohol dependency, drug addiction or psychiatric disorders. A central part of the job is to provide professional guidance to healthcare professionals (HCPs) regarding treatment of alcohol and substance use (Dideriksen et al., 2019). Hence, social nurses are usually present in the different wards several times per week, but they are not part of frontline staff, and a referral is needed.
The two participating municipalities in this study have <40,000 inhabitants (Muni A) and >500,000 inhabitants (Muni B). Both municipalities are a part of the hospital's uptake area and operate their own alcohol treatment facilities, in contrast to other municipalities in the Capital Region that buy services from external private alcohol treatment providers. Thus, both municipalities have their own facilities and provide a broad range of therapeutic sessions (individual and group), medical treatment, detoxifications and a variety of social support. They provide an individual treatment plan, often consisting of a combination of medical and psychosocial treatment. The treatment facilities are interdisciplinary, with psychologists, nurses, doctors, physiotherapists and social workers.
Study design
This study is a qualitative exploratory study examining the context determinant in cross-sectoral collaborations regarding patients with alcohol problems in an ED and two municipal alcohol treatment centres. With this qualitative approach, it is possible to draw attention to those elements in the cross-sectoral collaboration that work as barriers or enablers in future implementation efforts (Green & Thorogood, 2009; Nilsen & Bernhardsson, 2019).
Participants and data collection
Semi-structured single interviews (Kvale & Brinkmann, 2014) with ED nurses and medical secretaries (n = 21) were held in January and February 2020. Sampling for interviews was purposive and subsets of interview data have been used in previous studies in combination with other data material (Sivertsen et al., 2021, 2023), while data for this paper have not been used previously. Ward managers of nurses and medical secretaries acted as gatekeepers (Green & Thorogood, 2009) and on scheduled days, the interviewer was placed in a room near the ED during working hours in the data collection period. The HCPs on duty on those given days were asked to participate in the study and were interviewed in turns. Nurses (n = 11) had 5.8 years of seniority in the ED (range 1–16), whereas medical secretaries (n = 10) had 12.9 years (range 1–33). Interviews varied in length with a mean time of 31 min (range 21–60 min). Every participant received written and oral information about the study and signed consent forms.
Two group interviews (Green & Thorogood, 2009) with healthcare professionals from municipalities were conducted in their respective municipal alcohol treatment facilities in August 2020. Conducting interviews in pre-existing groups of colleagues is suitable for examining common experiences, opinions and social group norms (Kitzinger, 1995). In collaboration with treatment facility managers, participant sampling was purposive. Participants all worked in the alcohol treatment facilities and had experiences with ED collaboration. Three persons participated in Municipality A: the manager of the treatment facility; a doctor; and a nurse. In Municipality B, a manager, one doctor and two nurses participated. Both interviews had a duration of 2 h.
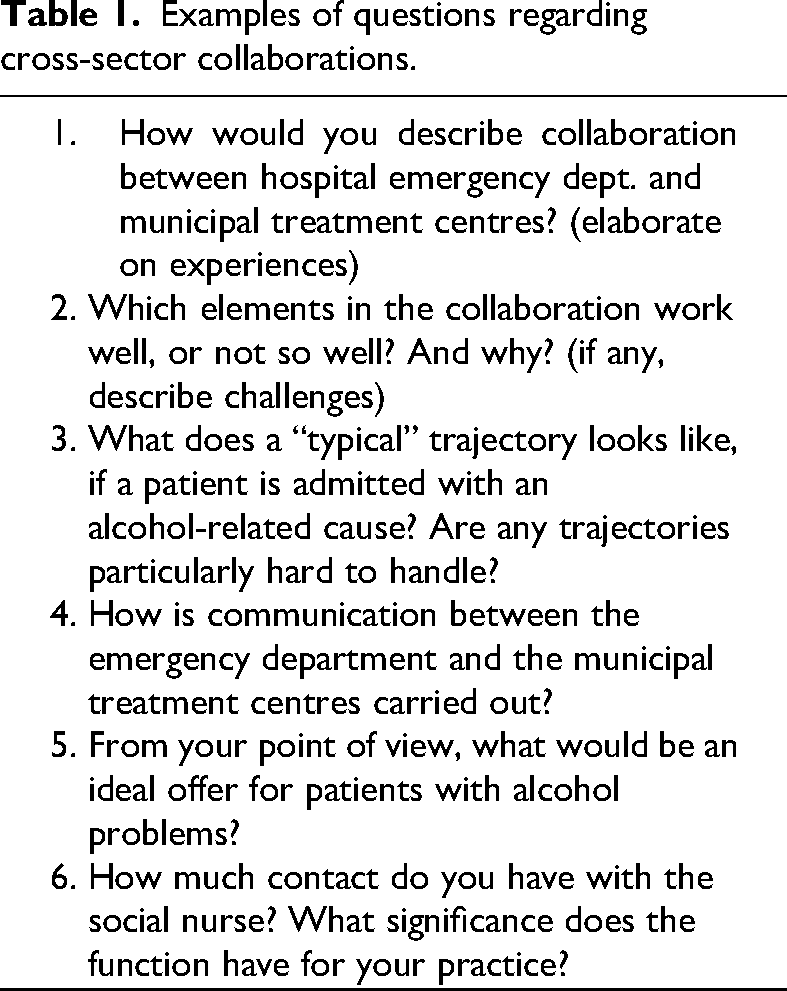
Interview guides were developed for the two sectors based on previous findings from an ethnographic study with 150 h of observation from an ED (Sivertsen et al., 2021). Here, it was found that cross-sector collaborations and HCP possibilities for actions ought to be explored further. Examples of questions are shown in Table 1.
Examples of questions regarding cross-sector collaborations.
Both single and group interviews were conducted by DMS. In group interviews, JWK acted as observer/co-interviewer. Interviews were recorded on a digital voice recorder and later transcribed verbatim.
Data analysis
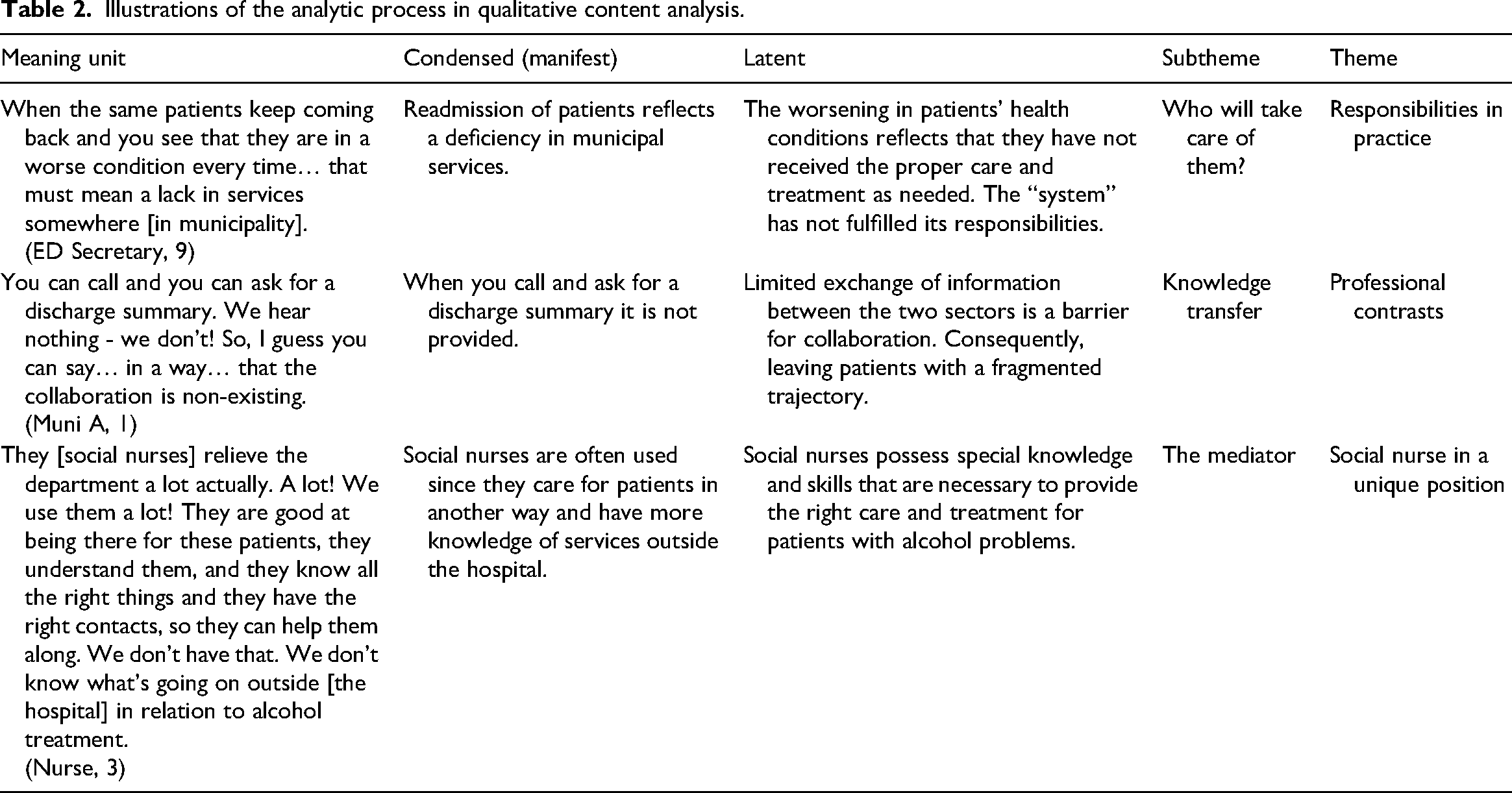
First, the material was read and re-read to gain an overall understanding of the content. All interviews were inductively coded using the Qualitative Content Analysis (Graneheim & Lundman, 2004). All transcriptions were divided into meaning units and subsequently the essence was condensed at a manifest level. Next, an interpretative and latent level was applied and codes that illuminated subthemes were provided. The first author coded the data material (207 pages) and JWK validated the work; discrepancies were discussed until reaching consensus. Finally, themes were developed in an iterative and interpretative process and discussed among authors until reaching consensus. This methodology provides insights at theoretical and latent levels and has a transparent analytical process that increases validity (Graneheim & Lundman, 2004). (Table 2)
Illustrations of the analytic process in qualitative content analysis.
The second-order analysis is inspired by the analytical concept of “boundary object” (Star & Griesemer, 1989) to explain and nuance the findings further. After re-reading the coded data material, the results were interpreted in an iterative process with this analytic perspective. The concept originates from the work of Star & Griesemer studying the collaboration of different actors and their divergent perspectives of flora and fauna species in a Museum of Zoology (Star & Griesemer, 1989). Here a boundary object is described as: “objects which are both plastic enough to adapt to local needs and the constraints of the several parties employing them, yet robust enough to maintain a common identity across sites […] They have different meanings in different social worlds but their structure is common enough […] to make them recognizable” (Star & Griesemer, 1989). Further, the term boundary should be understood as “a shared space” rather than an edge or a border (Leigh Star, 2010). Thereby, a boundary object has taken various forms in different studies and is not necessarily described as a material object, a “thing”, such as fieldnotes, specimens or maps (Star & Griesemer, 1989), but can also be a practice, e.g., care pathway (Haland et al., 2015), an idea or theory (Fox, 2011), or even a patient or human body (Bishop & Waring, 2019; Kirk et al., 2024; Mol, 2002). Further, boundary objects are often most relevant to study from an organisational level (Leigh Star, 2010). In this study, “the patient with an alcohol problem” is considered the boundary object, since the patient is present in both social worlds (EDs and municipal treatment centre), adapts to these worlds and is perceived differently in these places due to different representations of “identity”. The patient thereby constitutes a shared entity that crosses boundaries, further accounted for in the analysis.
Ethical considerations
The present study was approved by the Data Protection Agency in the Capital Region of Denmark (2012–58-0004 and VD-2018-229, I-Suite: 6471). According to the Danish National Committee on Health Research Ethics, there is no need for ethical approval in interview studies. The study was conducted according to the Helsinki Declaration (WMA, 2013) as all participants received written and oral information regarding the purpose of the study, confidentiality, voluntary participation, the right to withdraw and anonymity before they gave their written consent. The results are presented according to Consolidated criteria for reporting qualitative research (COREQ) (Tong et al., 2007).
Results
The overarching and unifying topic, corresponding to the aim of the study, is the cross-sector collaboration between the ED and the two municipalities. Based on the qualitative content analysis, three themes and seven subthemes emerged (see Figure 1), describing and explaining the existing collaboration from different perspectives. The main themes are: 1) Responsibilities in practice; 2) Professional contrasts; and 3) The social nurse in a unique position. In the following, we analyse these themes by illustrating how “the patient with an alcohol problem” can be interpreted as a boundary object (Star & Griesemer, 1989) across sectors, and further how this boundary object, as a shared object, can be used to understand the collaboration of these distinct social worlds.
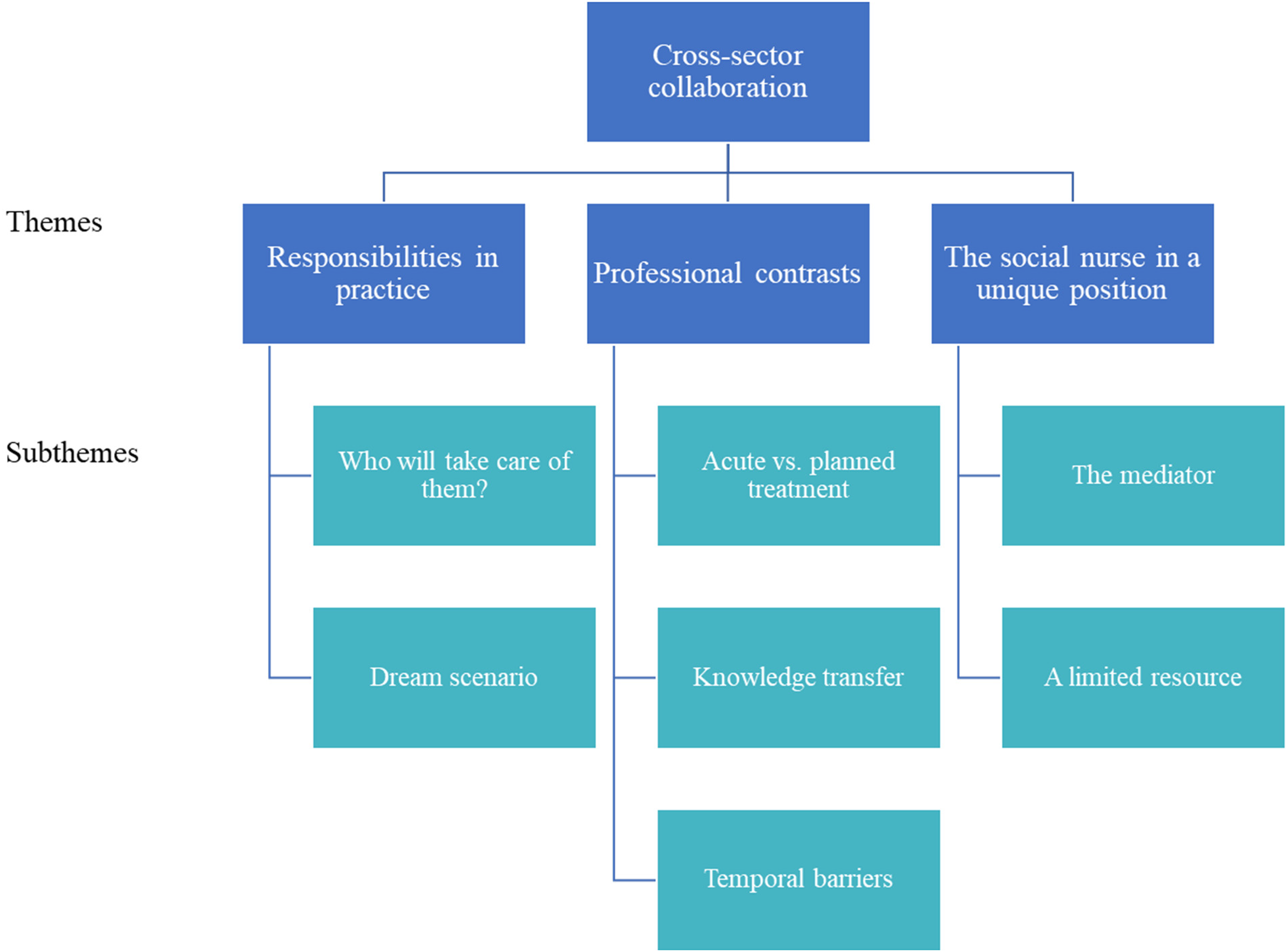
Themes and subthemes in the cross-sector collaborations between emergency departments and municipal alcohol treatment centres regarding patients with alcohol problems.
Theme 1: responsibilities in practice
This theme concerns the HCPs’ reflections on their own and their collaborators’ responsibilities in connection to alcohol treatment and how they interpret and practise this daily. The results showcase some of the discrepancies in perceptions of HCPs working in the two sectors, but also provides a picture of HCPs’ visions for treating patients with alcohol problems in a shared responsibility.
Subtheme: who will take care of them?
This subtheme concerns the HCPs’ perspective on responsibility for the patients between municipalities and hospitals. Most ED nurses express that patients do not have sufficient health literacy or are motivated to seek help on their own after discharge, and they are uncertain of what the patients are discharged to and who “catches them” outside the hospital. When they are discharged, I often wonder what are we sending them home to? […] Who will take care of them? (ED nurse, 7)
Between professions in the ED, some nurses problematise that they sometimes can feel left alone with the responsibility for the patients’ trajectories and call for secretaries and doctors to take part in this responsibility as well. Between sectors, a doctor in the municipality raises some issues regarding the professional responsibility of ED doctors, in terms of referring to municipal follow-up treatment if this is a possibility. My point is that the Hippocratic oath also applies to doctors who treat “addicts”. If the patient shows signs of a tumour, the doctor needs to deal with it. One cannot say: “I can’t deal with that”. It's a no-go! (Muni A, 1)
Subtheme: dream scenario
This subtheme contains the HCPs’ ideas for changes in structures and new opportunities for care and treatment for patients with alcohol problems, reflecting inadequacies in the current system. Many participants used expressions like “I wish…” or “I hope…” when they elaborated on this topic. A recurring topic was that patients with alcohol problems should not be in an ED. HCPs feel that they have no time for them, that the care given is not appropriate and that they are misplaced in the ED. They shouldn’t be here. They should be in a place where someone could take much better care of them and could follow up on it. This is just a revolving door – you are in and then you are out. So maybe they should go somewhere else. That would be the best. (ED nurse, 2)
This view can both be interpreted as self-reflection from a professional expressing concern of a patient group, but on the other hand it represents a reality where patients are objectified and “moved around” as the system demands. In contrast, according to the municipalities, the patients with the most severe alcohol problems do not want to be in the ED and they describe how these patients have an aversion of being admitted and how municipal HCPs try to avoid a hospitalisation by using close monitoring and relational work in the municipalities. Even though preventing an admission is overall beneficial, supporting patients’ aversions may expand the gap between sectors and potentially create distrust among them.
Many HCPs are aware of this gap and suggests that some in-hospital reorganisation should be done to optimise alcohol treatment. Several ED nurses have a dream of a specialised hospital unit only for patients with substance use, staffed with dedicated doctors, nurses and social workers. Some suggest a kind of hybrid between a somatic and a psychiatric unit, responsible for the complex treatment, which could be placed in either a somatic hospital ward with therapeutic treatment available or at a psychiatric ward with competences in acute somatic conditions.
The municipalities highlight the benefits of an outreach program where employees from the alcohol treatment centre could visit the hospitalised patient and make an agreement of entering treatment after discharge. We can help more people into treatment by meeting them in the ward, hand them a leaflet and say: it is me you will meet next Monday. I believe that would be the best-case scenario. (Muni A, 2)
Accordingly, this approach can provide the patient with a feeling of safety and ensure that the patient is not lost between hospital and municipalities – a shared responsibility. With these more integrated initiatives the boundary object would be described as positive, since the positive boundary object enables exchange of ideas between collaborative groups and yield a common language and enhanced knowledge and can even bring harmony to a previous dispute (Fox, 2011).
Theme 2: professional contrasts
This theme concerns the HCPs’ perception of their own professional roles and their core tasks. It further showcases boundary challenges and how barriers for collaboration exist due to assumptions about each other, lack of knowledge exchange and temporal structures.
Subtheme: acute versus planned treatment
Reflecting on their possibilities for action, the HCPs in the ED explain that besides services offered by the social nurse (see Theme 3), they lack opportunities and knowledge of what can be done. As one says: “I see it as fire extinguishing, then they [patients] come again, then we put out the fire again” (ED secretary, 2). Some of the HCPs in the ED are questioning what can be expected in an acute setting, other than their usual offers: detoxification; monitoring of withdrawal symptoms; and medication. In addition, many refer to a leaflet with contact information to a local alcohol treatment clinic, which is occasionally given to the patients. The presence of the leaflet in the ED, highlights the awareness of a shared space and the implicit potential of the leaflet to change the patient trajectory and lead the patient (the boundary object) in the intended direction of a planned treatment. Thereby, it represents a concrete artefact symbolising the pathway between sectors. I have just handed out a leaflet with a telephone number on it. I don’t know of any other options besides that. (ED nurse, 5) It says Substance Abuse Centre on our leaflets, but when Mr. Smith who drinks too much red wine is admitted, he does not feel that he belongs in a centre like that with all the drug abusers […] It is a lost cause […] what the hell have they been thinking! (ED nurse, 6) Well, you can say that I’m supposed to provide the basic nursing and check for withdrawal symptoms and all those things… But we’re in an acute situation and they are often in a very bad condition. (ED nurse, 2) If I assess that a patient cannot be discharged, then even if the doctor believes that no more can be done, we can still try to keep them for a couple of days […] It is not because we want to ‘throw them out the door’, but we sometimes have to. If we cannot argue why they should stay hospitalised, they’ll be discharged. (ED nurse, 3)
In opposition to the HCPs in the ED, municipalities are more optimistic about treatment, they work with long-term goals and have faith that the patient eventually will succeed, even after several relapses. Professionally, they would prefer to see patients at a much earlier stage than is usually the case. The municipalities call for earlier detection in hospitals and closer collaboration; this way they can intervene earlier and prevent a patient's personal deterioration. Here, the patient is spoken of in a more active role, if it is possible to arrive at an earlier stage than they usually do. We welcome those who are not on the ropes, so we can work with the family dynamics, and the children and the employment. (Muni B, 3)
Subtheme: knowledge transfer
This subtheme deals with barriers for cross-sectoral communication experienced by the two sectors. Several HCPs from the ED call for more simplified communication pathways and supportive IT solutions to deliver brief notices, instead of long and detailed care schedules (da. plejeforløbsplan), which is the existing tool, although not frequently used. I know, we can make a care schedule and send it to the municipality in agreement with the patient telling the municipality to visit [name]. But I don’t think we really do that (…) I think most of them are left undone. (ED nurse, 1) We are almost never notified when our patients are discharged. We have no idea. We have no idea what medicine they have been given, and we rarely can see it in the database. If he got 400 mg last time and I give him 100 mg, the treatment fails. The patient cannot tell me what he got. “I got some little round pills” – they have no idea. And it’s such a shame, since we really want to cooperate. (Muni B, 3)
A care schedule is very seldom used, even though it is the agreed tool for exchanging information. As mentioned in methods, a boundary object can also be a “thing”, and if a care schedule is perceived flexible enough to adapt to both sectors while simultaneously being robust enough to keep a common identity (Star & Griesemer, 1989), then it can be interpreted as such. However, in opposition to the earlier mentioned positive boundary object, the inability to create knowledge exchange would categorise it as an ineffective boundary object (Fox, 2011).
Subtheme: temporal barriers
This subtheme relates to the temporal barriers and availability as experienced by the healthcare professionals. ED HCPs call for increased accessibility to the municipalities, such as expanded opening hours and a 24-h phone, not only a few hours on weekdays. They describe how municipal treatment facilities are not open when patients need them the most, and from an ED perspective these opening hours are experienced as problematic. Consequently, patients will end up in the ED if help is not provided in the municipalities, since they are open around the clock. Many alcohol units are closed on holidays and weekends when people are most vulnerable and maybe are having a bottle of vodka during Easter or Christmas, then there is no one to help them. I think it's a shame if somebody is sad on Christmas Eve and only the emergency department is there to take care of them. (ED secretary, 9) It is a practical question because rounds often take place around noon where they agree to discharge, but our telephone hours end at noon. The patients have lunch [at the hospital] between 12 and 1 pm and then they are ready to leave, but then we are closed. It's incoherent. (Muni B, 2)
Consequently, these temporal barriers are disruptions in the patient trajectory and there seems to be a lack in the choreography of their work regarding their common boundary object (the patient). Instead, they work in parallels. Further, as presented in the subtheme “acute vs. planned treatment”, the perspectives for treatment are different in the two sectors, while EDs work in short-term perspectives and the municipalities have a long-term perspective in their approach to the patient.
Theme 3: the social nurse in a unique position
This theme concerns the function of the social nurse since this particular service played a dominant part in the dataset. The theme is divided into two subthemes: “The mediator” and “A limited resource”, describing the HCPs’ need for a function like this, but also the potential pitfalls of this function and how it may affect the patient (as the boundary object).
Subtheme: the mediator
The importance of the social nurse function is emphasised in most interviews. The social nurse clearly fulfils a need in the ED providing specialist knowledge and care. This function is mentioned in very positive terms and is believed to be an almost certain guarantor of a good discharge. They are damn good. They are SO good because they know who to call if problems occur after discharge. And they have such good contact with these patients. And often, they know them already, which is extremely important. (ED nurse, 10) I appreciate the social nurses who can provide patients with the relevant offers. I think it's a jungle, knowing what is relevant and where to find it. They try to teach us, but I still consider it a jungle. (ED nurse, 1) The social nurses are a big help regarding the interdisciplinary work and what to offer the patients after discharge. They are always updated with recent changes and know which offers exist and how to send the patients on their way. I always use her for those things. (ED nurse, 2) I try to use the social nurses as often as I can. I call in and say: “now Peter is here again”. [Imitating social nurse]: “Great, I will check on him”. I think it works fine! (Muni B, 3)
Subtheme: a limited resource
Even though the social nurse is highly appreciated in both sectors, several participants point to the fact that even though the social nurse tries to see as many patients as possible, she cannot see all patients with alcohol problems. Some suggest that she primarily treat or take care of patients with the most severe and obvious problems. If somebody is really far out, they can talk to a social nurse – and they are in demand! They are very busy. So, we only use them in very, very severe cases. (ED secretary, 5) The social nurses take care of the most vulnerable or homeless, those who have the biggest problems. But not necessarily those who are admitted because they drink and have problems because of that. They end up getting help for 2 days [detoxification] and then they are left to their own devices. (ED nurse, 3) I don’t want to paternalise [name] in room 9.3 to talk to the social nurse because he drinks six beers a day and has mild withdrawal symptoms. The social nurse is an offer for those who want it. But I do not want to impose anything on anyone. (ED nurse, 1)
As shown in the previous subtheme, all participants mentioned the function of the social nurse in very positive terms, but both municipalities highlighted the fragility of this position. Usually, there is one social nurse (sometimes two) covering an entire hospital, which means that if the social nurse has a day off, is on a course or on vacation, the collaborative work is likely to fail. …and then she may be gone on a Friday, but the patients get discharged anyhow and then collaboration is ruined immediately. If she isn’t present just once, then there is no cooperation. It is sad, since they are good when at work. (Muni A, 3)
Discussion
This explorative study presented three themes, describing the collaboration between the two sectors in relation to patients with alcohol problems as inadequate. A lack of opportunities and clarity in the division of responsibilities was experienced by staff in EDs and municipalities. ED HCPs, in particular, were uncertain of possibilities and structures in the municipal alcohol treatment facilities. Both sectors faced barriers complicating the intersectoral work, such as temporal aspects, professional approaches and organisational structures in acute versus long-term treatment. One of the main findings in this study was that the cross-sectoral collaboration was largely linked to one highly appreciated function – the social nurse. We found that the social nurse had a significant role as a mediator in the intersectoral collaboration in relation to patients with alcohol problems, since this function fulfils a need of the HCPs in providing specialist knowledge and taking over responsibility. However, results also showed that not all patients with alcohol problems are referred to the social nurse. HCPs assess which patients could benefit most from this type of help, based on the core focus of the function: socially marginalised patients (Dideriksen et al., 2019). With this core focus, the social nurse is entitled to assess and prioritise if patients (as boundary objects) are within the target group. In the results, we described how the social nurse is positioned as a mediator and a passage point to further services. In addition to this, Cramer et al. describes how “boundary work” and “boundary actors” occur constantly in organisations (Cramer et al., 2018). The boundary term is used to indicate a difference between and within professions, but it can be used as a strategy to connect units, or as a barrier protecting autonomy, status and the control of resources (Cramer et al., 2018; Gieryn, 1983). In other words, these boundaries are negotiable, and the boundary actor acts as a mediator connecting two worlds, but with a strong position to include or exclude patients according to certain patient group categories (Cramer et al., 2018). From this perspective, the social nurse could be described as a “boundary actor” being highly appreciated and bridging the acute disease-focused and flow-driven environment of an ED with the holistic approach that governs the social nurse's work. An ethnographic study examining the handling of patients with alcohol problems in an ED showed that HCPs tend to not recognise the broad spectrum of alcohol problems and mainly focused on patients with severe substance dependency often in combination with psychiatric disorders and social problems, since they demand extra time and energy from staff with their “inappropriate” behaviour (Sivertsen et al., 2021). Hence, these patients are likely the same as those referred to the social nurse, since the social nurse, as the boundary actor, takes over responsibility for the trajectory of the “hard-to-treat” patients. As shown in the results, a patient who drinks six beers a day and shows mild withdrawal symptoms may not necessarily be referred. This decision may be due to a subjective assessment by the nurse or based on prior experiences of negotiating if a patient was in the target group of a social nurse. The “minor” alcohol problems of patients not perceived as “hard-to-treat” may fulfil criteria for dependency, but this category of patients may only receive treatment for the cause of their admission, not their alcohol problem. When this happens for patients with dependency, this will most likely be the case for the less identifiable patients with hazardous and harmful use as well (Sivertsen et al., 2021). In case the social nurse is the primary link between hospitals and municipalities in relation to patients with alcohol problems, patients referred from hospital to treatment centres will be skewed towards socially marginalised patients. This was also an observation point from the municipalities, where there was a wish that citizens could enter treatment at an earlier stage of their alcohol misuse. Broadening the target group and incorporating preventive aspects to this function would remediate this. Internationally, social workers and social service providers in the ED fulfil some of the same tasks as the social nurse (Craig & Muskat, 2013; Gehring et al., 2022; Moore et al., 2017). There is a considerate overlap in practice roles such as case manager, counsellor and problem-solver (Moore et al., 2017). However, in Denmark, social nurses and social workers differ in terms of educational background and work under different legislations – the Health Act and the Act of Social Services, respectively. Moreover, the number of social workers in hospital have decreased drastically over decades (Harsløf et al., 2016). In the results, it was suggested that a person from the alcohol treatment facility could visit the hospital on a regular basis and plan with eligible patients to enter treatment. This has been done in a Danish RCT study (the Relay Model), where a therapist from a municipal alcohol treatment centre showed up at four different somatic in-hospital wards and met patients screened to be at risk, offered Brief Intervention and provided information about available treatment options after discharge (Schwarz et al., 2019). With the aim of improving referrals from hospital to municipal alcohol treatment, they found a significantly higher probability of treatment attendance 18 months after discharge in those patients who had received the intervention. However, even though the Relay Model had tried to overcome known provider-level barriers towards SBIRT, the study concluded that the overall number of people attending was relatively small and the considerable efforts of this intervention did not add up to outcomes and recommended to rethink if general hospitals are suitable for SBIRT (Schwarz et al., 2019). Results like this highlight the importance of separating intervention outcomes from implementation outcomes (Proctor et al., 2011).
Leaflets are another way to inform of possibilities for entering treatment. We found that besides the social nurse, ED HCPs felt that they lacked opportunities to help patients with alcohol problems. However, leaflets were occasionally given to patients, but the wording was experienced as creating barriers, since patients associated the word “abuse” with “drug abuse”. Such an experience could prevent a nurse from ever delivering such a leaflet. The terms used in relation to severe alcohol use (or substance use), which are highly stigmatised health conditions, affect the likelihood of people seeking help (Volkow et al., 2021). Hence, if leaflets are not aimed directly at their target group and the wording stops people from entering treatment, HCPs might feel that they have done something when delivering the leaflet, but if the effect of it is questionable, at least changing the wording would be a starting point and an “easy picking”. However, it is still not known if patients would enter municipal treatment even if wording was different and despite the “open door policy”, since alcohol treatment is heavily stigmatised and only few patients have the confidence and motivation needed to navigate the system (Andreasson et al., 2013; Gilburt et al., 2015; May et al., 2019). Further, a Cochrane review showed that the effect on printed educational material is low in order to change practices and outcomes (Giguere et al., 2020). In our study, HCPs from both sectors agreed that patients should not be responsible for seeking help themselves. Municipalities meant that the ED should be responsible for establishing connections to alcohol treatment facilities, but to the contrary ED HCPs suggested that, ideally, general practitioners should be responsible. In a Consolidated Framework for Collaboration Research, having a shared vision is one of the main constructs (Calancie et al., 2021); therefore, future implementation efforts for cross-sectoral alcohol initiatives should initially focus on strategies to attain a common goal. Further, we found challenges in the existing collaboration due to different approaches to the patients and knowledge transfer, both in terms of temporal barriers but also in electronic medical records for medicine (da. Fælles Medicin Kort, FMK), in which municipalities were rarely able to see which medicine was given during a hospitalisation and potentially updated medicine status. In SBIRT literature, cross-organisational communication and the necessity of integration with the electronic medical health record are highlighted as important facilitators for continuous referral to treatment processes (Broyles et al., 2012; Vendetti et al., 2017).
Lack of time is frequently highlighted as a main barrier for implementing new interventions (Gargaritano et al., 2020; Geerligs et al., 2018; Vendetti et al., 2017), but different dimensions of time and temporality are often not described. We found that certain temporal structures characterised both sectors, and that participants experienced different temporal barriers in relation to this. Reddy et al. described temporality in work in three temporal features: trajectories; rhythms; and horizons (Reddy et al., 2006). Temporal trajectories are used to describe temporal logics following a “structured timeline” focusing on the sequence of work activities. An example of a temporal trajectory from this study is when patients are admitted for detoxification and are discharged as soon as they are stable. To be efficient, EDs must comply with requirements for length of stay and the maintenance of patient flow; therefore, they often use the term “fully treated” when the admission diagnosis is treated (Bendix Andersen et al., 2018; Kirk & Nilsen, 2015). Further, it can be argued that patients with alcohol problems may be perceived as “flow-stoppers” by ED staff (Kirk & Nilsen, 2016; Sivertsen et al., 2021). Several findings in this study can be related to temporal rhythms, which characterise work at a collective level and the repeated patterns of work. The HCPs in both sectors use their knowledge of these recurring patterns in the planning of care and treatment activities; for instance, in access to phone services, knowledge of rounds and discharge procedures or when municipalities try to advocate for a hospitalisation over the weekend, since they are closed for the weekend themselves. A place like an ED has multiple rhythms in relation to people, activities and interactions, which collectively form “a complex temporal fabric” (Reddy et al., 2006). This complexity becomes clear when the temporal activities of the two sectors are not aligned in, for example, opening hours, which has consequences for the patients who may experience feeling “lost” in a fragmented healthcare system. This leads to the question: Is the organisational structure designed for patients’ needs? Future cross-sector interventions aimed at people with alcohol problems should avoid siloing and work towards coordinated treatment. Further, findings should be incorporated in a process of tailoring the intervention and in selection of implementation strategies (Powell et al., 2015).
Strengths and limitations
A strength of the study is that it presents both the hospital sector and the primary care sector (alcohol treatment facilities in the municipalities) in a joint analysis to highlight attention points in the existing collaborations. Another strength is that no other peer-reviewed studies have, to our knowledge, described the use of the social nurse function from the HCPs’ perspectives in relation to everyday practice in an ED and specifically in relation to alcohol problems. Future studies on this function should focus on the referral practices (who, how, when and why), characteristics of the referred patients and potentially rejected patients, and examine the impact on HCPs’ feeling of responsibility, when the social nurse is involved in the patient trajectory. Even though it is a Danish concept, it can be compared to other “bridge building” functions, such as case managers, social workers, alcohol specialist nurses or alcohol liaison service. Therefore, results are likely transferable to those similar functions.
A limitation was that in group interviews, managers were present, which may have influenced the power balance in the group, possibly hindering someone from expressing his/her opinion (Kitzinger, 1995). However, managers were also part of the daily functions in the centres; therefore, they were also regular colleagues. Further, even though the two municipalities in this study varied in size, they had the same structure in terms of their own setup for alcohol treatment facilities implicit in the municipal organisation. Other municipalities buy services from external private facilities, and it is possible that results would have been different if those municipalities had been interviewed. Another limitation was that hospital doctors were not interviewed in relation to these cross-sectoral collaborations. We chose not to do so in this study, since they are mainly responsible for sending referrals, but the direct contact and coordination with municipalities is often a task for nurses or secretaries. However, future studies of ED collaborations should also include doctors’ perspectives, since a part of examining patients is to ask about alcohol and tobacco use and, as such, to deliver a platform for discussing issues related hereto. Finally, patients’ perspectives were not examined in this study, including their perceptions of the coherence and continuity in the intersectoral work and if they feel that they receive the needed help. These considerations would be of interest in future studies.
Conclusions
The existing collaboration between an ED and municipal alcohol treatment facilities is characterised by a lack of knowledge of each other's services and professional differences in their approach to the patient. HCPs in EDs describe a lack of possibilities and both sectors experience collaborations as influenced by temporal structures, which complicate the intersectoral work. The underlying organisational structures that govern their work counteracts a shared goal and responsibilities, which challenges collaborative work. Results show that besides the highly valued “social nurse”, there is a low strength in collaborative networks. This position has a unique status in supporting cross-sector collaborations; however, primarily socially marginalised patients with severe alcohol problems are referred to the social nurse. There are no current practices or collaborations aimed at the broad spectrum of alcohol use, besides a leaflet that is delivered occasionally. This means, that the present organisational structures and the way these structures are managed by HCPs is a co-producing factor for not handling a group of patients with “less severe” alcohol problems.
Footnotes
Acknowledgements
The authors would like to thank HCPs and managers from the participating ward and municipalities. We would also like to thank Andreas Schwander and Sascha Bjørnholdt for transcribing parts of the interviews.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received the following financial support for the research, authorship, and/or publication of this article: This research received funding from Tværspuljen, RegH (grant no. P-2018-2-14) and Amager Hvidovre Hospital strategic research funds (grant no. PSP: E-21835-14, PSP: E-21835-08 and 2021-518).