
Abstract
The National Survey on Drug Abuse and Health reported the prevalence of alcohol use, cigarette smoking and illicit drug use among pregnant women in the United States as 11%, 16% and 4%, respectively, in 2009 (Behnke et al., 2013). Since the recognition of fetal alcohol syndrome in 1973, alcohol has received more scientific attention compared to the other two (Clarke & Gibbard, 2003), probably because the evidence for harm at low levels (approximately two drinks/week) is weak (Mamluk et al., 2017; McCallum & Holland, 2018).
Fetal exposure to all three substances has overlapping effects including low birth weight, lower brain volumes and cognitive deficits (Ekblad et al., 2010; Rivkin et al., 2008; Treit et al., 2016). That alcohol and tobacco are legal does not mean that they are safer than illicit drugs (Ross et al., 2015). Substance use in pregnancy is influenced by women's perceptions of their safety. For example, some believed that cannabis was helpful for morning sickness (Mark et al., 2017) and considered it safe (Jarlenski et al., 2017).
There is a broad consensus that binge drinking causes adverse birth and neurodevelopmental outcomes (Flak et al., 2014). Because alcohol crosses the placenta, maternal and fetal alcohol levels equalise within 2 h of alcohol intake (Dejong et al., 2019). This makes binge drinking particularly harmful to the fetal central nervous system (Lange et al., 2017). In contrast, the evidence regarding low alcohol use in pregnancy (<32 g per week) is patchy and equivocal (Mamluk et al., 2017). For example, a Danish study reported that maternal consumption of 1–4 drinks per week did not impair IQ, attention and executive function of children at the age of 5 years (Kesmodel et al., 2012; Skogerbo et al., 2012). This agrees with a meta-analysis that found no association with cognition for low-to-moderate levels of alcohol intake (Flak et al., 2014). Other researchers reported higher cognitive abilities in mothers who were light drinkers (<2 units per week) (Kelly et al., 2012). In addition, no behavioural difficulties were found in children of light-drinking mothers (Kelly et al., 2012; Robinson et al., 2010).
Tobacco is more commonly used by pregnant women compared to alcohol and illicit drug use. Like alcohol, smoking metabolites pass through the placenta, reducing uterine blood flow and retarding fetal growth (Law et al., 2003). Compared to alcohol and illicit drugs, tobacco use in pregnancy was the strongest predictor of low birth weight (Hemingway et al., 2020). Infants of smoking mothers experience nicotine withdrawal about 10 h after birth and show greater need for handling (Stroud et al., 2009). In childhood, greater irritability, inattention and externalising behaviour were associated with tobacco exposure in pregnancy (Cornelius & Day, 2009).
The effect of illicit drugs on fetal neurodevelopment is subtle and varies by drug. Animal studies showed that cocaine disrupts the coupling of the D1 receptor to its G protein (Thompson et al., 2009). With decreased dopamine, the proliferation and migration of neurons to cortical areas is inhibited (Crandall et al., 2007; Lidow & Song, 2001). This may account for the attention-deficit hyperactive disorder (ADHD)-like symptoms of cocaine-exposed offspring (Thompson et al., 2009). Amphetamines (including MDMA) tend to accumulate in the fetal striatum and brainstem and disrupt monoamine transport (Won et al., 2001). Swedish and American cohort studies reported that children prenatally exposed to amphetamine were more aggressive or volatile emotionally (Billing et al., 1994; Smith et al., 2015). However, deficiencies in cognitive and academic outcomes were not consistently observed.
Since alcohol is a teratogen, the finding that low intake is associated with a positive outcome (in some studies) is surprising. The lack of precise measures of prenatal alcohol exposure may conceal its harm. Sood and colleagues mitigated recall bias by asking pregnant mothers to report alcohol consumption in the past 2 weeks (Sood et al., 2001). They reported a dose-response relation of alcohol consumption and child behaviour problems at the ages of 6 and 7 years. Unlike observational human studies, animal models of fetal alcohol exposure enable causal inference. Experiments in macaques by Clarren and colleagues showed that macaques develop similar facial deformities as humans prenatally exposed to alcohol (Clarren & Bowden, 1982). Macaques exposed for longer durations in gestation had difficulties walking and learning and worse performance in a cognitive task (Clarren & Astley, 1992). For a review of animal studies of fetal alcohol exposure, see Schneider et al. (2011).
There may be other unmeasured confounders in human studies. It is possible that light drinkers (vs. abstainers) in pregnancy have genetic, socioeconomic and psychological characteristics that mask or offset the detrimental effect of alcohol (Barefoot et al., 2002). It is also difficult to tease apart the contribution of gestational smoking and illicit drugs from the effects of family upbringing, genetic predispositions and co-morbidity among disorders (Boden et al., 2010; Kuja-Halkola et al., 2014). In this work, we considered the possibility that differential attrition in mother–child dyads make the observed samples different from the baseline cohort. In longitudinal studies, it is common for participants with lower income, poorer health and lower social status to drop out in follow-up (Young et al., 2006). This motivated our use of weights to make the composition of surviving participants similar to the starting cohort.
We hypothesised that: (1) prenatal exposure to alcohol, tobacco and illicit drugs predicts deviant behaviours (threatening others, truancy and cruelty to animals) in early adolescence; and (2) these deviant behaviours are preceded by psychological deficits (in IQ, social cognition, working memory and inhibition) that are themselves predicted by those substances.
Methods
Sample data and variables
This is a secondary data analysis of the Avon Longitudinal Study of Parents and Children (ALSPAC), a cohort of the offspring of pregnant women resident in southwest England born in 1991 and 1992. ALSPAC was designed to study how genetic and environmental factors influence human development (Golding et al., 2001). Parental information was assessed with questionnaires at multiple points in pregnancy, when the average age of the mothers was 28 years (age range = 16–44 years). The children's physical characteristics, biological measures, education, health and social outcomes were repeatedly measured from birth to adulthood (Fraser et al., 2013). Since the offspring are now adults with their own children, ALSPAC has become a three-generation study (Northstone et al., 2019). The data for this study ended when the offspring were aged approximately 12 years.
Our sample consisted of 7,769 children who were alive 1 year after birth and whose parents had complete data in alcohol, substance use and socioeconomic variables (Table 1). Among the children, 3,767 (48%) were female and 4,002 (52%) were male. If the birth consisted of multiple infants, only one was included.
Descriptive statistics of parental variables at pregnancy (n = 7,769). a
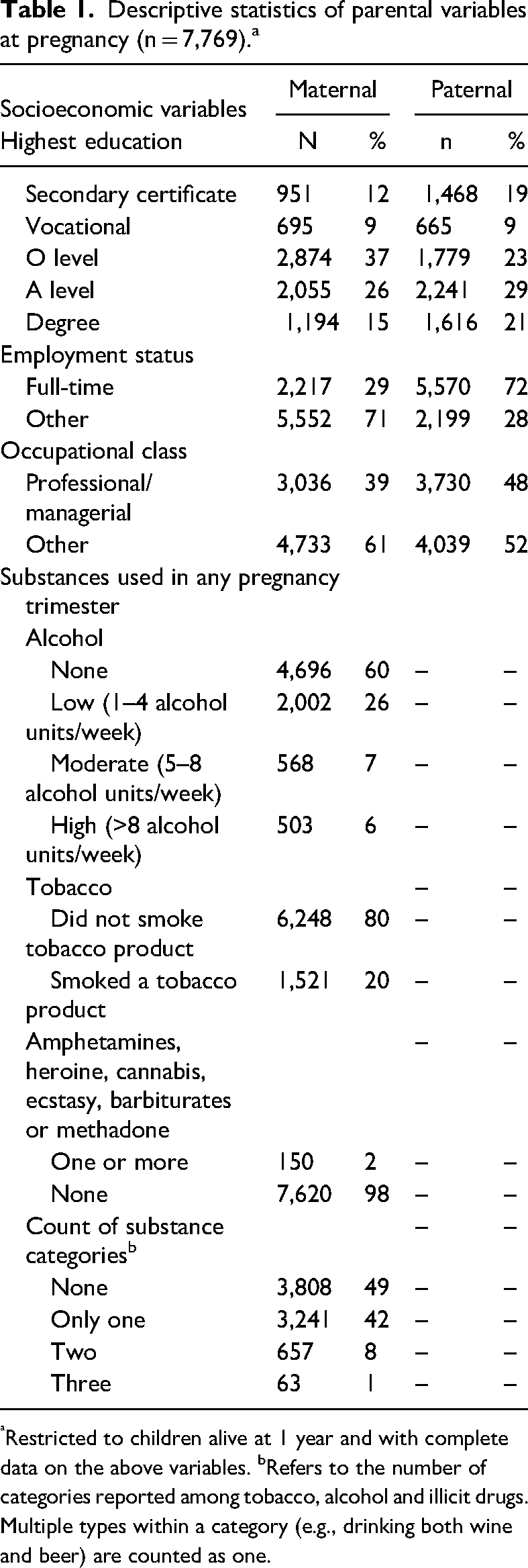
Restricted to children alive at 1 year and with complete data on the above variables. bRefers to the number of categories reported among tobacco, alcohol and illicit drugs. Multiple types within a category (e.g., drinking both wine and beer) are counted as one.
Three dependent variables were deviant behaviours at 12 years old: truancy; threatening to hurt others; and cruelty to animals, all of which were dichotomous variables. These were selected because they represent different aspects of deviant behaviour. Truancy reflects non-conformity but not aggression, while the other two distinguish between aggressive words and behaviours.
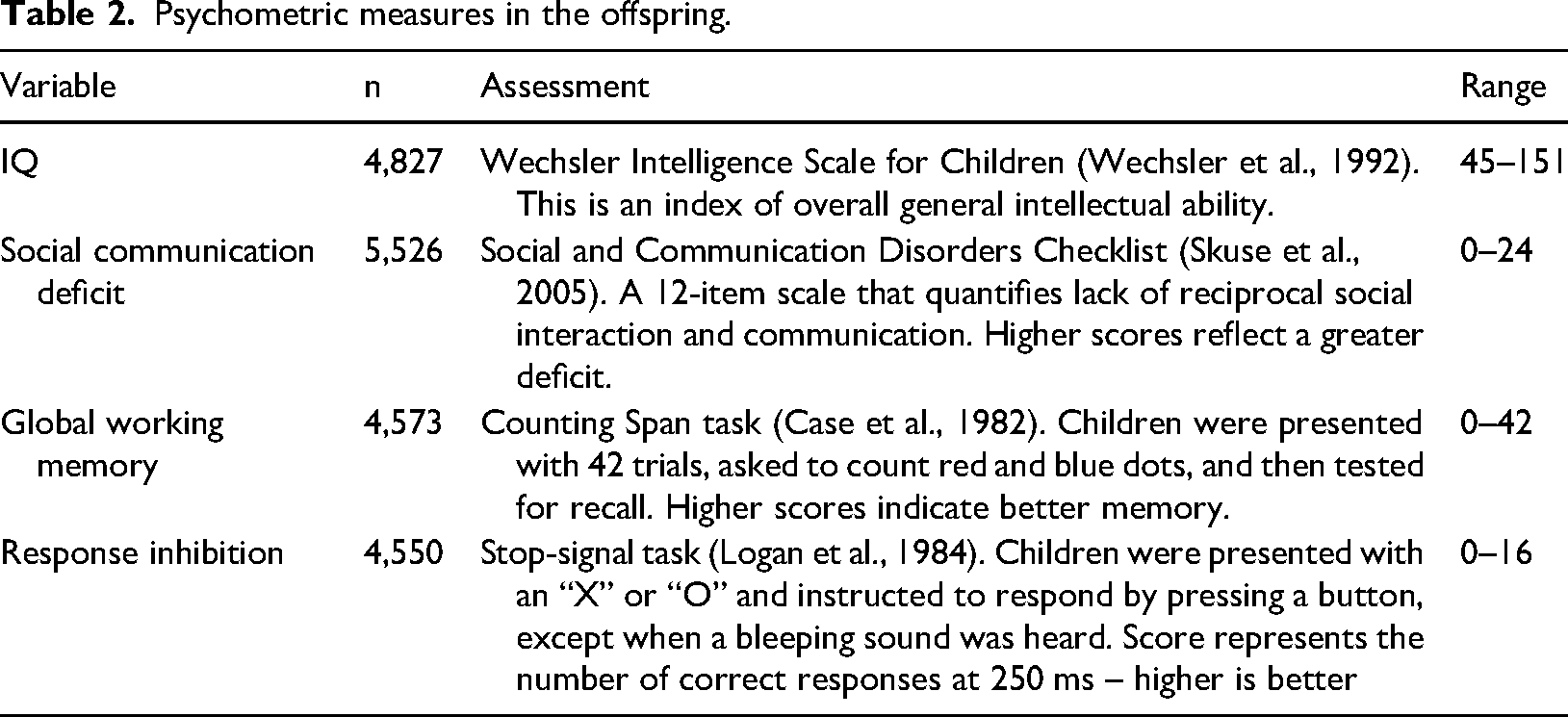
In addition, we selected four psychological dependent variables assessed at earlier ages. These were IQ and social communication deficit (both measured at 8 years of age) and working memory and response inhibition, which were measured at 10 years of age (Figure 1). These four psychological variables (Table 2) served dual roles as dependent variables and predictors of the outcomes at the age of 12 years.
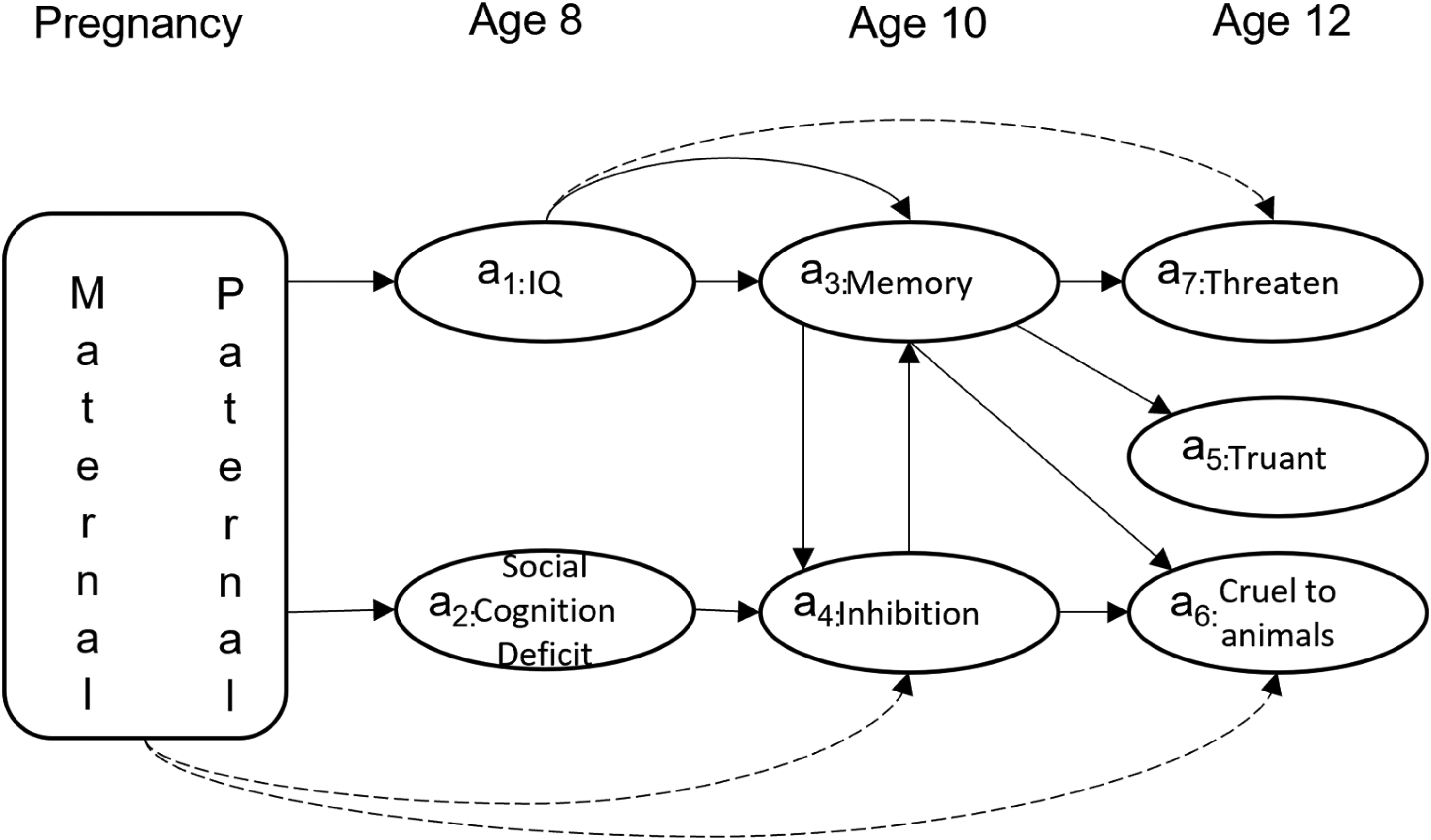
Weighting scheme. For IQ (assessment 1) and social cognition deficit (assessment 2), the observed and unobserved samples are weighted to achieve balance based on maternal and paternal characteristics. Attending the other assessment(s) during the same age is also entered as a predictor. Double-adjustment was used when balance was not achieved with inverse-probability weights alone (dashed arrows). Other dashed arrows are omitted for clarity.
Psychometric measures in the offspring.
The exposures of interest were maternal alcohol, tobacco and illicit drug use at any point in pregnancy. Mothers were asked about the quantity of beer, wine, spirits and other alcoholic drinks in the first, second and third trimesters. For the first and third trimesters, ALSPAC derived the sum of alcohol units per week (variables a261 and c373, respectively). ALSPAC did not provide a derived variable for the second trimester, so we created a variable that represented the maximum number of alcohol drinks weekly, which had a range of 0–121 alcohol drinks. Mothers were then classified by the maximum amount of alcohol units (or drinks) in any trimester. These categories were as follows: none; low (1–4 alcohol units); moderate (5–8 alcohol units); and high (>8 alcohol units) (Centers for Disease Control and Prevention, 2021). To illustrate, a woman who reported 1 unit/week in the first trimester, 12 drinks/week in the second trimester, and 2 units/week in the third trimester would be assigned to the highest category. If there was no information for a given trimester, a woman was classified based on the higher number in the other two trimesters.
Tobacco use was assessed with two questions asked approximately 18 weeks into pregnancy. These inquired if the mother smoked cigarettes, cigars or any tobacco product at any time in the first 3 months of pregnancy or in the previous 2 weeks. An affirmative response to either question indicated tobacco exposure. Illicit drug exposure was indicated if the mother reported taking one or more of the following: amphetamines; heroine; cannabis; ecstasy; barbiturates; and methadone.
In adjusting for confounders, we chose variables that are known contributors or risk factors for an outcome. For example, taking illicit drugs may reflect maternal stress or poor maternal mental state and these factors are associated with lower IQ in the offspring (Baird et al., 2023). Accordingly, we entered maternal mental health indicators. We used the single question, “did the mother seek counselling or a psychiatrist as a child”. Maternal depression status during pregnancy (at 21 months) was assessed using the Crown Crisp—Depression subscale (Birtchnell et al., 1988; Ross & Hafner, 1990). This consisted of eight questions with scores in the range of 0–16 (Ross & Hafner, 1990).
Engaging in deviant behaviours in adolescence can result from various environmental factors. These include parental education and occupation, which reflect socioeconomic status. A meta-analysis of 133 studies showed that low socioeconomic status was associated with child and adolescent antisocial behaviours (Piotrowska et al., 2015). To tease apart the influence of substances, we adjusted for maternal and paternal socio-demographic characteristics during pregnancy. These were as follows: age at first pregnancy; educational qualification; employment status; and type of occupation. Following previous studies (Melotti et al., 2011; Taylor et al., 2013), qualifications had five categories: certificate of secondary education (CSE); vocational; O level; A level; and degree. The British educational system emphasises “sorting” to restrict entry to the universities. Even though holders of CSE, vocational, O-level and A-level certificates are all high school graduates, only those with A-level qualifications can be admitted to university (Kerckhoff et al., 2001). Parental occupations were dichotomised into professional/managerial (classes I and II) and others (classes III–V).
In addition to parental variables, adolescents who engage in deviant behaviours are influenced by their peer group (Kendler et al., 2015). We therefore adjusted deviance outcomes for peer influences. By peer influence meant whether the child's friends (peers) engaged in behaviours related to the outcome. For truancy, this was having friends who were truant; for threatening others, this was whether friends were seen punching somebody; and for cruelty to animals, it was seeing friends being cruel to animals.
Analysis
Our overall analytical strategy consisted of the following three steps: (1) calculating weights to deal with attrition; (2) creating weighted logistic regression models for deviance; and (3) creating weighted linear regression models for psychological outcomes. As an aid to understanding, Figure 1 shows the temporal sequence of assessments, with the results of later outcomes predicted by earlier outcomes.
Calculation of weights for covariate balancing
Inspection of the data revealed that missing values in the outcomes were associated with behaviours in pregnancy and parental characteristics. For example, children of mothers who took illicit substances in pregnancy were less likely to attend an IQ assessment, leading to missing IQ scores. When outcomes are systematically related to exposures of interest, a complete-case analysis can lead to biased results and wrong conclusions. Accordingly, we used inverse probability of treatment weighting (iptw) as implemented in the twang package (Cefalu et al., 2021) in R (R Core Team, 2022). The iptw function in twang assigns a weight to each child based on parental characteristics and attendance in previous or contemporaneous assessments.
We designed our analysis to include only parents who had non-missing values at baseline but allowed children to have missing values in one or more of the assessments. After the inverse probability weights were calculated, the balance of observed and unobserved samples with respect to the covariates were re-examined. If balance was not achieved with respect to a covariate, we used double adjustment by entering the same variable to predict an outcome, following a recommended procedure (Nguyen et al., 2017). Inadequate balance was defined as a standardised difference in proportions of 0.10 or higher between observed and unobserved samples (Nguyen et al., 2017).
Weighted regression models
Using weights created in the previous step, regression models were created for psychological and deviance outcomes, entering residual imbalance covariates if necessary. Truancy, threatening others and cruelty to animals were all dichotomous variables; therefore, logistic regression models were created. These models were adjusted for peer influences.
We used weighted linear regression for the psychological outcomes at the ages of 8 and 10 years. Unlike with deviance outcomes, we did not include peer influences for IQ, social cognition working memory and inhibition because these were laboratory-based tasks.
This project received approval from the university ethics board.
Results
Social deviance at age 12+ years
All three deviance outcomes were significantly predicted by peer influences. High prenatal alcohol exposure (>8 drinks per week) predicted truancy (odds ratio [OR]: 1.60, 95% confidence interval [CI] 1.03–2.47) and cruelty to animals (OR: 2.29, 95% CI: 1.11–4.70). Tobacco exposure predicted truancy (OR: 1.45, 95% CI: 1.06–1.98) and threatening others (OR: 1.28, 95% CI: 1.01–1.61). Illicit drug exposure predicted truancy (OR: 2.02, 95% CI: 1.05–3.88). In general, deviant behaviours were predicted more strongly by peer influences, with all three deviant behaviours having significant associations with at least one substance. Please refer to Supplement 1, Supplement 2 and Supplement 3 for statistical tables with alcohol, tobacco and illicit drugs as predictors, respectively.
Psychological outcomes at ages 8–10 years
IQ was inversely related to tobacco exposure (B = −3.49, 95% CI: −4.77 to −2.21) and unrelated to illicit drug use. Surprisingly, low prenatal alcohol exposure (1–4 alcohol units per week) was associated with higher child IQ compared to no alcohol exposure. The offspring of mothers who belonged in higher drinking categories (moderate or high) did not differ significantly from counterparts with non-drinking mothers.
We performed a sensitivity analysis among 503 offspring exposed to the highest alcohol category (>8 drinks per week in at least one trimester) and treated alcohol units as a continuous variable (range: 9–121 drinks per week). With IQ as a dependent variable, we performed a weighted linear regression as before. We found that each additional drink over nine drinks per week predicted about one-fifth of a point decrease in child IQ (B = −0.19, 95% CI: −0.37 to 0.00, p = .05).
A greater social communication deficit was predicted by tobacco exposure (B = 0.73, 95% CI: 0.43–1.04) and illicit drug exposure (B = 1.04, 95% CI: 0.14–1.93). Working memory was inversely related to tobacco exposure (B = −1.39, 95% CI: −2.00 to −0.77). Response inhibition was not predicted by any substance or parental characteristic.
Discussion
We examined prenatal exposure to psychoactive substances and child outcomes. After accounting for attrition, parental and peer influences, we found that all three deviant behaviours were associated with at least one substance. Truancy was predicted by all three substances, cruelty to animals was predicted by high alcohol drinking and threatening others was predicted by tobacco.
These deviant behaviours in early adolescence were preceded by associations of tobacco with deficits in IQ, social communication and working memory in childhood. Social communication deficit was also associated with illicit drug exposure. That tobacco exposure had broad and enduring associations is consistent with previous studies. During infancy, tobacco exposure predicted lower self-regulation, lower attention, negative affect and increased startle (Barros et al., 2011; Fried et al., 1987). The underlying pathology may persist into childhood and adolescence, presenting as oppositional defiant disorder and delinquency (Wakschlag et al., 2006).
That tobacco exposure predicts lower IQ has been reported previously (Mortensen et al., 2005; Naeye, 1992). Mortensen et al. (2005) reported a dose-response relation between number of cigarettes smoked daily and child IQ at the age of 18 years. They reported a 6-point difference in IQ between children of non-smoking mothers and the heaviest smokers. Our finding regarding tobacco and IQ agrees with these studies, even though our variable was dichotomous. In contrast, Breslau and colleagues reported that after adjusting for maternal IQ and education, tobacco exposure was not associated with offspring IQ (Breslau et al., 2005). The interpretation offered in that study is that tobacco is not causally related to IQ. Another study using the Collaborative Perinatal Project did not find a relation between maternal smoking and child IQ (Gilman et al., 2008). We agree with the authors that it is difficult to separate smoking per se from other familial and environmental factors. Gene-environment studies are needed to apportion the relevant weight to the different contributory factors predicting deviance outcome (Chung et al., 2021).
Illicit drugs predicted truancy and a social communication deficit. The adolescent children of mothers who used opioids were more likely to engage in fighting, carry a handgun and steal valuables (Feder et al., 2020). Our own result suggests that a deficit in recognising emotions could be a factor in antisocial behaviours. Cannabis-dependent adult patients were reported to have impaired detection of facial emotions, which can lead to interpersonal problems (Bayrakci et al., 2015). Just as with smoking, it is difficult to pry apart the biological effect and family environment. Flykt and colleagues found that severe maternal substance use disorder predicted impaired emotion recognition in offspring (Flykt et al., 2021). However, this deficit was moderated by the quality of the mother–child relationship in infancy (Flykt et al., 2021). Our finding that the father's post-secondary qualification is protective against threatening others suggests that both parent relationships are important.
The finding that low levels of alcohol drinking were associated with higher IQ (compared to abstainers) is surprising, but not entirely new. An earlier ALSPAC study did not find lower academic scores at the age of 11 years with up to one drink per day in pregnancy (Alati et al., 2013). They found, however, that the offspring of binge-drinking mothers had lower educational attainment. Jacobson and colleagues meta-analysed six cohort studies in the United States that studied prenatal alcohol exposure and IQ at different ages (Jacobson et al., 2021). They detected an inverse association with IQ in young adulthood, but not at earlier ages. This partly confirms the unexpected relation of low alcohol exposure and IQ at the age of 8 years. The finding that each alcoholic drink over nine per week is harmful to child IQ is consistent with a previous study (Streissguth et al., 1990). These findings support the dose-response quality of the teratogenic effect of prenatal substance exposure and begs the question about the mediating effects of environmental factors and intervention support (Subramoney et al., 2018).
It is important to note that IQ is only one of many outcomes that can be adversely affected by alcohol exposure. Other studies found an association with antisociality. Disney and colleagues reported a higher risk for conduct disorder with even with low amounts of alcohol in pregnancy after adjusting for parental antisocial behaviour and a wide range of confounders. Moreover, the IQ of individuals with prenatal alcohol exposure varies greatly, in the range of 20–120 (Mattson et al., 2019). Similarly, a systematic review concluded that low to moderate alcohol use increases mental health problems in the offspring (Easey et al., 2019). Importantly, that review excluded studies of fetal alcohol syndrome.
Although peer influences were not the focus of the study, it is notable that these had the strongest predictive value for threatening others, cruelty to animals and truancy. Such outcomes of delinquency and the propensity for future offending are the byproduct of the interactions between negative and positive social factors (Walters, 2018). While parental factors such as income and education level positively protect from delinquency, their impact is limited to early childhood. Studies have demonstrated an inverse relationship between paternal education and delinquency (Demuth & Brown, 2004). On the other hand, peer influences were found to peak during adolescence and are less positive (Dishion & Dodge, 2005). Peer contagion, a process by which an individual's development is undermined, is the main mechanism by which this mutual process leads to negative and delinquent outcomes. Still, understanding these factors should have benefits for intervention.
The present study has some limitations. We did not have biological assays for the substances of interest. It has been shown by Ferraguti et al. (2017) that self-reported drinking underestimates actual consumption based on an ethanol metabolite in urine. The categorisation of alcohol intake is based on thresholds defined by the United States Centers for Disease Control and Prevention. These thresholds vary across countries (DeVido et al., 2015) and continue to evolve (Paradis et al., 2023). Self-reported substance use was assessed only in pregnancy. Maternal smoking after birth, second-hand smoke in childhood, and the effect of alcohol and drugs on breastfeeding are confounders that we did not control for. Our data are also limited by the absence of interventions in postnatal nutrition, social support and a supportive environment that could mitigate the effects of the substance exposures. It is possible that the associations (or lack thereof) that we found are mixed (or masked) by postnatal maternal and family behaviours.
Supplemental Material
sj-docx-1-nad-10.1177_14550725231206015 - Supplemental material for Parental factors predicting social deviance and psychological outcomes in offspring: Evidence from the Avon Longitudinal Study of Parents and Children (ALSPAC)
Supplemental material, sj-docx-1-nad-10.1177_14550725231206015 for Parental factors predicting social deviance and psychological outcomes in offspring: Evidence from the Avon Longitudinal Study of Parents and Children (ALSPAC) by Lloyd Balbuena, Mansfield Mela and AG Ahmed in Nordic Studies on Alcohol and Drugs
Supplemental Material
sj-docx-2-nad-10.1177_14550725231206015 - Supplemental material for Parental factors predicting social deviance and psychological outcomes in offspring: Evidence from the Avon Longitudinal Study of Parents and Children (ALSPAC)
Supplemental material, sj-docx-2-nad-10.1177_14550725231206015 for Parental factors predicting social deviance and psychological outcomes in offspring: Evidence from the Avon Longitudinal Study of Parents and Children (ALSPAC) by Lloyd Balbuena, Mansfield Mela and AG Ahmed in Nordic Studies on Alcohol and Drugs
Supplemental Material
sj-docx-3-nad-10.1177_14550725231206015 - Supplemental material for Parental factors predicting social deviance and psychological outcomes in offspring: Evidence from the Avon Longitudinal Study of Parents and Children (ALSPAC)
Supplemental material, sj-docx-3-nad-10.1177_14550725231206015 for Parental factors predicting social deviance and psychological outcomes in offspring: Evidence from the Avon Longitudinal Study of Parents and Children (ALSPAC) by Lloyd Balbuena, Mansfield Mela and AG Ahmed in Nordic Studies on Alcohol and Drugs
Footnotes
Acknowledgements
We are grateful to Dr David Petrishen and Dr Jenna Pylypow for their helpful suggestions and discussion.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work did not receive specific funding. LB received research funding from AA Pharma unrelated to the present work.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.