
Abstract
There are multiple conceptualisations of how to understand substance use among adolescents. A prominent one is the public health model for prevention of disease and disorder, which asserts that there is a greater likelihood of substance use among people exposed to specific risk factors, compared to among those randomly selected from the general population (Arthur et al., 2002). This study attempts to assess the relevance of this model and its various domains in predicting substance use in Swedish adolescents, considering cigarette use, binge-drinking and illegal substance use at different time points (9th and 11th school grade). While the public health model has had a great influence on policy and prevention interventions, surprisingly few studies have assessed how well it fares across different substances during different periods in adolescents’ lives. There is an obvious need for a comprehensive understanding of how risk factors may vary over time (Mak et al., 2020) and across substances (del Palacio-Gonzalez & Pedersen, 2022). Without a thorough understanding of what drives young people's substance use, resources aimed to prevent harm may be poorly allocated.
The public health model for prevention of disease and disorder
Conceptualisations of adolescent substance use can broadly be divided into two main categories: the normalisation thesis, which claims that substance use is an integral part of youth culture (Parker et al., 1998), and a series of risk factor approaches. A key conceptualisation within the risk factor approach is the public health model for prevention of disease and disorder (Arthur et al., 2007; Arthur et al., 2002). The risk factor approach typically underpins prevention interventions in this area, such as school-based drug education (Karlsson, 2006). In this study, we focus on the public health model for prevention of disease and disorder due to its major impact on policy and prevention.
One of its main assumptions is that substance users have specific characteristics (typically “deficits”) that distinguish them from non-users (Hawkins et al., 1992). By identifying and targeting the risk factors with the strongest impact on substance use, it is assumed that negative outcomes can be reduced (Arthur et al., 2002; Hawkins et al., 2002). Numerous studies have highlighted risk factors as key for understanding what drives substance use (Anderberg & Dahlberg, 2018; Cleveland et al., 2008; del Palacio-Gonzalez & Pedersen, 2022; Diseth & Samdal, 2015; Elliot et al., 1989; Epstein et al., 2017; Flory & Lynam, 2003; Gauffin et al., 2013; Hawkins et al., 1992; Jones et al., 2012; Joseph et al., 2021; Kellam et al., 1982; Mak et al., 2020; Shedler & Block, 1990; Sher et al., 1991). Some researchers, however, suggest that the predictive strength of the risk factors may vary during different periods of life. A strong predictor at one point can be a weak predictor later on, and vice versa (Cleveland et al., 2012; del Palacio-Gonzalez & Pedersen, 2022; Epstein et al., 2017; Hawkins et al., 1992; Mak et al., 2020). Also, the associations may vary by substance (del Palacio-Gonzalez & Pedersen, 2022; Mak et al., 2020) or by different domains that are assumed to hold specific risk factors (Cleveland et al., 2012).
Although the bulk of this research has addressed individual level factors, some researchers have explored risk factors at higher levels (Cleveland et al., 2012; Hawkins et al., 1992; Jones et al., 2012). Arthur and colleagues, for example, identified risk factors across four overarching domains: family, school, individual/peer and community (Arthur et al., 2007). The strength of the associations between various domains and substance use is inconsistent in the literature (Epstein et al., 2017) and these domains may be differently linked with substance use throughout the period of adolescence. For example, whereas the family domain may be important in the early teenage years, school and individual/peer factors may play a greater role later on (Cleveland et al., 2008).
Previous research is also inconsistent regarding the association between gender and substance use. Some research suggests that gender does not predict use of tobacco and alcohol (Van Ryzin et al., 2012) or illegal substances (Van Ryzin et al., 2012; Wilkhu, 2021). Other studies indicate that males and females may be affected differently by specific domains during specific periods of their lives (Epstein et al., 2017).
Within the family domain, poor family management has been linked to various kinds, and degrees of, problem behaviour (Arthur et al., 2002; Epstein et al., 2017; Hoeve et al., 2009; Lac & Crano, 2009; Van Ryzin et al., 2012). Cleveland and colleagues found that the family domain did predict substance use, but less so than other domains (Cleveland et al., 2008). Other research, however, suggests the domain has a stable association with substance use (Epstein et al., 2017).
Low academic achievement and commitment have been identified as the strongest risk factors in the school domain, albeit only showing a moderate association with problem behaviour (Arthur et al., 2002). In contrast, a Swedish study found low academic achievement to be strongly associated with illegal substance use later in life (Gauffin et al., 2013). Also, while academic ambition was not analysed separately, it has been included in school-related indexes in previous research, with lower scores associated with legal substance use (Diseth & Samdal, 2015), as well as substance use in general (Bond et al., 2007; Catalano et al., 2004). Truancy has also been strongly associated with substance use (Henry & Huizinga, 2007; Karlsson et al., 2018; Rocque et al., 2017), although the exact causal relationships may be difficult to establish (Henry & Huizinga, 2007; Rocque et al., 2017).
The literature has also paid considerable attention to the role of what can be referred to as “deviant behaviour”. Various measures have been used in the studies, such as committing crimes, problem behaviour, delinquency and anti-social behaviour. All of these are part of the individual/peer domain, and are sometimes also treated as outcome variables along with substance use, rather than as risk factors in their own right (Arthur et al., 2002). Deviant behaviour seems to be a consistent predictor of substance use from early to late adolescence (Cleveland et al., 2008; Cleveland et al., 2012; Pape & Rossow, 2021) and may, in combination with other risk factors, increase the likelihood of substance use (Epstein et al., 2017).
It has also been concluded that deviant behaviour may be caused by attention-deficit/hyperactivity disorder (ADHD) (Flory & Lynam, 2003), which potentially makes the former a mediator rather than a risk factor for substance use (Klein et al., 2012; Sibley et al., 2014). In line with this, there has been extensive research on the link between ADHD and substance use. ADHD is associated with lifetime use of cigarettes and illegal substances, but there is no evidence for any association with alcohol (Lee et al., 2011). Other psychiatric conditions, such as poor mental health, have also been associated with use of cigarettes (Mathers et al., 2006) and alcohol (Pape & Rossow, 2021), but little evidence supports a specific association between depression and later cannabis use (Degenhardt et al., 2003). Thus, in Sweden, we can expect that a traditional risk factor approach would be more relevant to explain what is considered marginalised, atypical and of low prevalence, such as use of illegal substances. It may be less relevant in explaining use of alcohol and cigarettes, which are within the cultural boundaries of normality.
Aims and research questions
The aim of the present study was to test the validity of the public health model for prevention of disease and disorder for both legal and illegal substance use among young Swedes, and at different periods of their adolescence, using data from a nationally representative sample born in 2001 (Futura01). The study will contribute with up-to-date findings to inform discussions on how best to conceptualise adolescent substance use in a low-prevalence country. Given that profound changes in adolescent substance use have taken place during the past decades (Englund, 2019), understanding how established conceptualisations fare in relation to contemporary Swedish data is fundamental. Additionally, different conceptualisations are linked to different definitions of the problem, but also to how different preventive strategies and legal frameworks are articulated and implemented.
Research questions:
To what extent do risk factors in different domains (family, school and individual/peer) predict adolescent substance use? Do the associations vary between different substances and between school years 9 and 11?
Methods
Data and participants
The purpose of the overarching Futura01 project is to understand substance use and how it may affect adolescents’ paths into adulthood. The participants in this nationally representative sample were born in 2001 and the first wave of data was collected during 2017 when participants attended 9th grade at age 15–16 years (n = 5576). Across Sweden, 500 schools were randomly selected and 344 of these schools participated (68.8% of eligible school classes; we have no data on the characteristics of the schools that did not participate). The questionnaires were distributed manually on paper in the classrooms. The response rate was 82.3% among the students who were invited to participate, also excluding surveys with incomplete ID numbers. Participants (then aged 17–18 years) were free to choose whether to fill out the questionnaire on paper or electronically, with the vast majority choosing the latter. Only those who participated in both waves were included in the present study (n = 4013). Of these, individuals with complete values on all variables considered in this study were included (n = 3303, 82.3%).
The study was granted permission by the Swedish Ethical Review Authority, reference number 2020-01272. The Futura01 project holds a separate permission, reference number 2017/5.2. The data were stored on locked units with no access to identification keys. The collection of the Futura01 data was not conducted by the authors of this article, but we complied with all relevant study protocols to ensure protection of the data.
Measures
The measures used cover risk factors from several domains, and use of both legal and illegal substances. Three out of Arthur and colleagues’ four domains were examined (family, school and individual/peer) (Arthur et al., 2007; Arthur et al., 2002). Community, the fourth domain, was left out due to lack of relevant variables in the data.
We used data from baseline and first follow-up. Identical questions were used for measuring the variables included in this study (see below) on both occasions, besides gender which was only measured at baseline, but deducted from baseline to follow-up.
Dependent variables
The three dependent variables captured use of cigarettes, binge-drinking and illegal substance use. For the questions “Have you ever smoked cigarettes?” and “Have you ever used narcotics? (Narcotics include, e.g., hashish, marijuana, amphetamine, cocaine, heroin)”, four responses were available: “No”, “Yes, during the past 30 days”, “Yes, during the past 12 months” and “Yes, more than 12 months ago”. For cigarettes, we concentrated on those who had used during the past month. For narcotics, that is, illegal substances, we looked at lifetime use. For alcohol, we used a binge-drinking variable: “How often do you drink six or more units per occasion” and decided upon a cut-off point of monthly binge-drinking. Each of these were coded as binary variables. Individuals who had experience were coded as 1 and those who had no such experience were coded as 0.
Independent variables
We elaborated with different independent variables to capture key risk factors from the three domains (see Table 1). We had at our disposal only a limited number of variables which corresponded with the risk factors outlined by Arthur and colleagues (Arthur et al., 2007; Arthur et al., 2002), but these should work as reasonable indicators.
Variables included in this study.
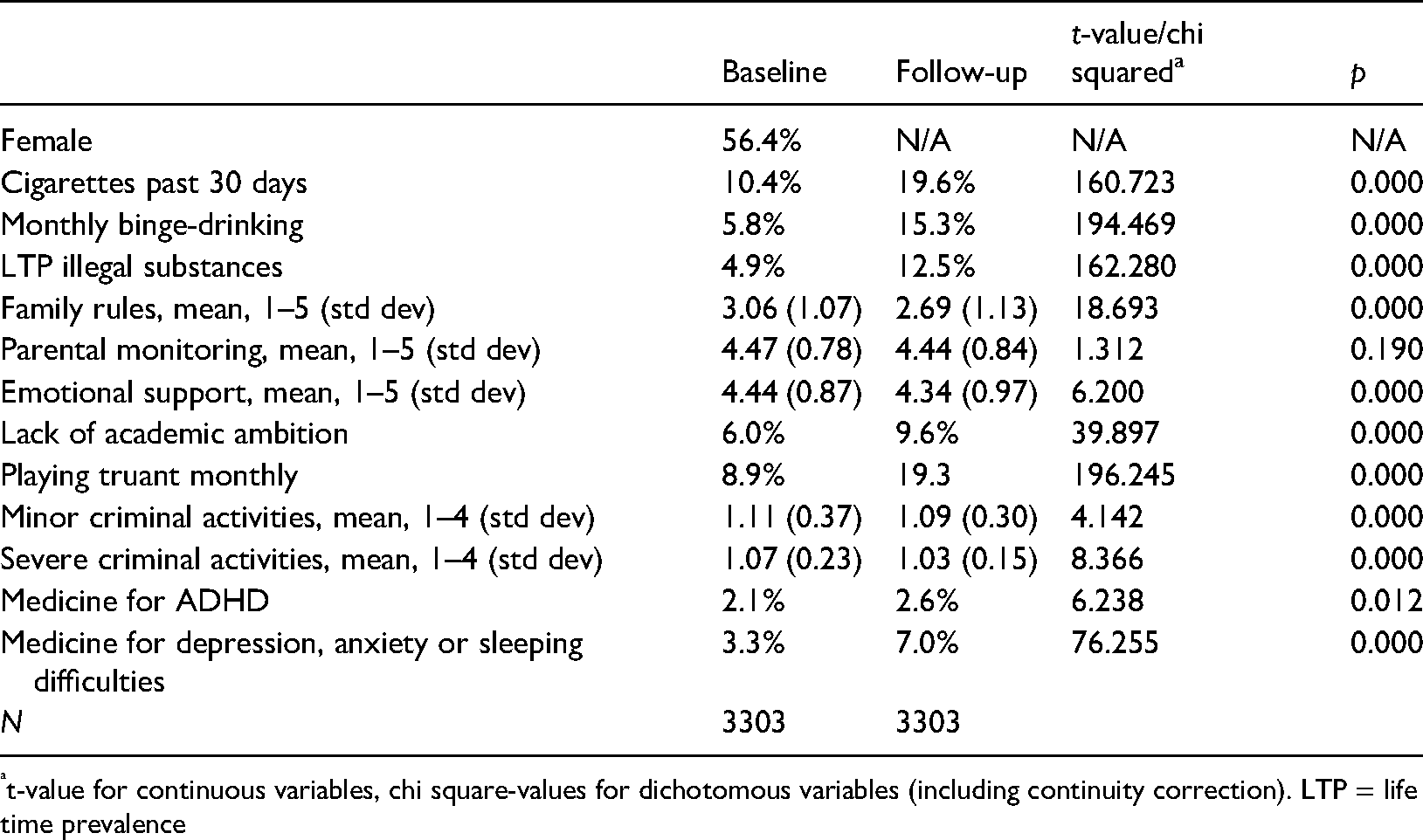
t-value for continuous variables, chi square-values for dichotomous variables (including continuity correction). LTP = life time prevalence
Six questions were recoded into three variables to capture the family domain. Each of these had the same response alternatives, ranging from 1 (almost never) to 5 (almost always). The statements: “My parent(s) have set rules about what I can do at home” and “My parent(s) have set rules about what I can do outside home” were combined into the variable “parental rules”. The statements: “My parent(s) know(s) whom I spend time with during evenings” and “My parent(s) know(s) where I am during evenings” were combined into the variable “parental monitoring”. The third variable, “emotional support”, was derived from the statements: “I can easily get affection and support from my mother and/or father” and “I can easily get emotional support from my mother and/or father”. Mean values were calculated for each of the family variables, thus keeping the original scale for each question (i.e., 1–5).
Academic ambition and playing truant were used as indicators of the school domain. To capture lack of academic ambition the students were asked to what extent the statement “It is important for me to do well in school” applied to them. Four options were given, and they were coded into a binary variable where the responses “Not at all” and “Not agreeing to some extent”, were coded as 1 and “Agree to some extent” and “Agree completely” were coded as 0. Playing truant was measured with the question “Are you prone to skip classes?” with response alternatives ranging from “No” (coded as 0) to “Yes, several times a week”. In this study, we used a binary variable for monthly, or more frequent truancy (coded as 1).
Two indicators were used to capture the individual/peer domain: criminal behaviours and use of prescribed medicines. Criminal behaviour was measured by the question “How many times have you done the following during the past 12 months?” followed by six criminal activities, each with response alternatives ranging from “Never” to “More than five times”. These six activities were coded into two variables, each variable then divided by the number of questions included to reflect the original scale of the question for each of the six criminal activities (i.e., 1–4). The minor criminality variable included “Shoplifted or stolen something from a store” and/or “Stolen a bicycle”. The severe criminality variable included: “Broken something that did not belong to you (e.g., bus stop, window, someone's bicycle or similar)”, “Trespassed in someone's home or other buildings”, “Set something valuable on fire (e.g., a car, building or a forest)” and finally “Left your house with a weapon (e.g., knife, brass knuckles or baton)”.
Two dichotomous variables in the individual/peer domain measured whether participants had ever been prescribed ADHD medicine and/or medicine for depression, anxiety or sleeping difficulties. Individuals who reported ever having been prescribed ADHD medicine were coded as 1, and those who had not were coded as 0. Individuals who reported having been prescribed medicine for either depression, anxiety or sleeping difficulties received a value of 1 and those who did not were coded 0. The third option “Not sure” was coded as “missing” for both these variables.
Statistical analyses
Differences in the distribution of the independent and dependent variables at baseline compared to follow-up were tested using McNemar's test (for dichotomous variables) and paired t-test (for continuous variables) (see Table 1). The cross-sectional associations between the independent and the dependent variables at baseline and first follow-up, respectively, were analysed using both unadjusted (Tables 2a and 2b) and adjusted modified Poisson regression analysis (Tables 3a and 3b) (Zou, 2004). This modified approach entails running a Poisson regression on a binary outcome, using robust standard errors (Zou, 2004). P-values <0.05 were considered statistically significant. We created an analytical sample across all substances and both time points resulting in 3303 complete cases (i.e., using listwise deletion of missing values). Statistical analyses were run using IBM SPSS statistics 26.
Cross-sectional modified Poisson regressions at baseline (unadjusted).
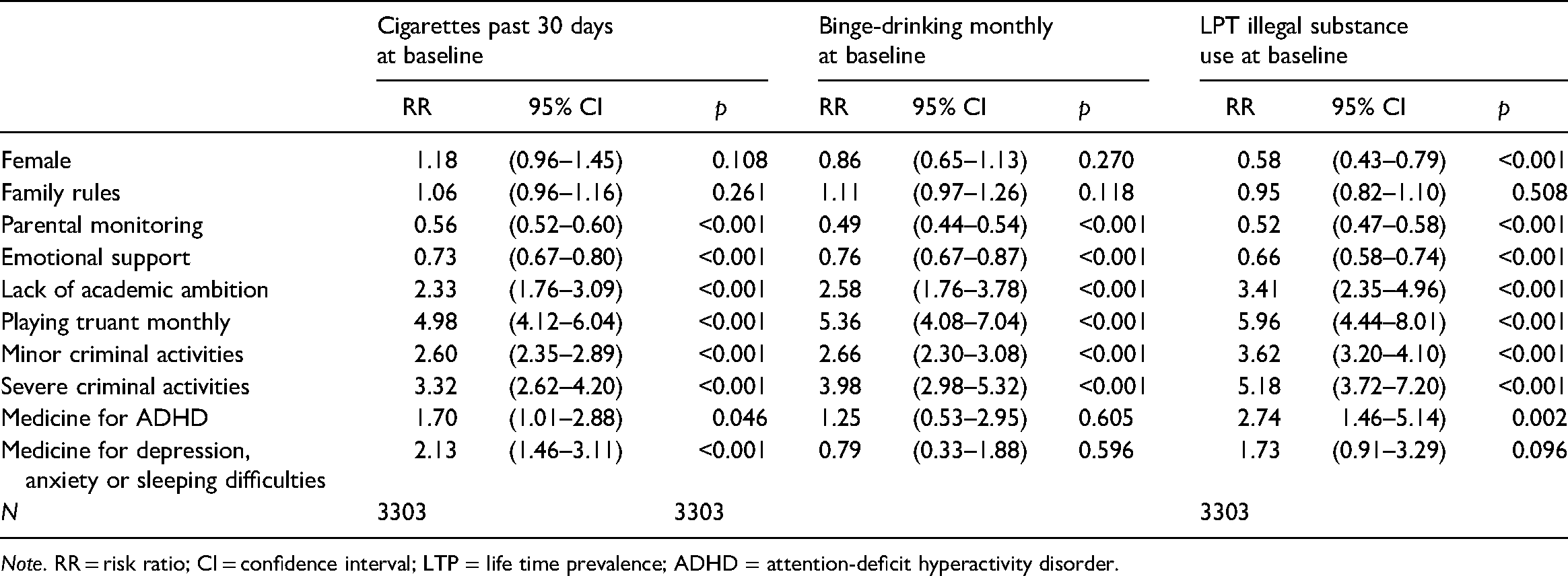
Note. RR = risk ratio; CI = confidence interval; LTP = life time prevalence; ADHD = attention-deficit hyperactivity disorder.
Cross-sectional modified Poisson regressions at follow-up (unadjusted).
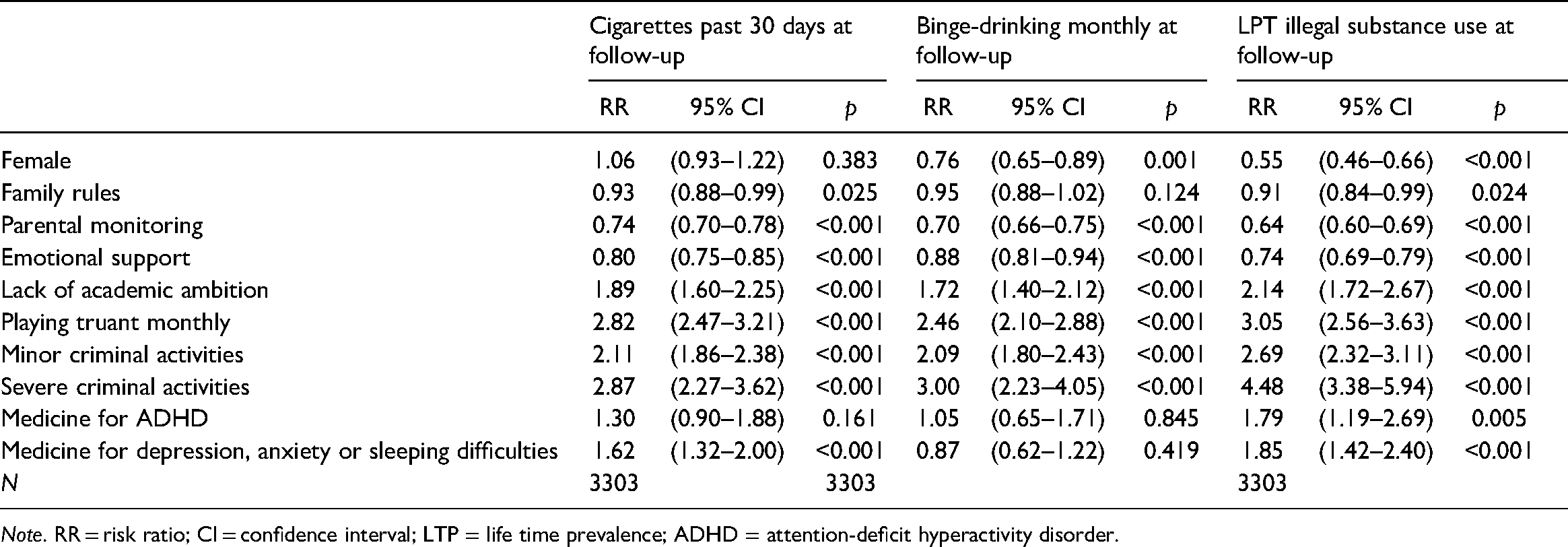
Note. RR = risk ratio; CI = confidence interval; LTP = life time prevalence; ADHD = attention-deficit hyperactivity disorder.
Cross-sectional modified Poisson regressions at baseline (adjusted).
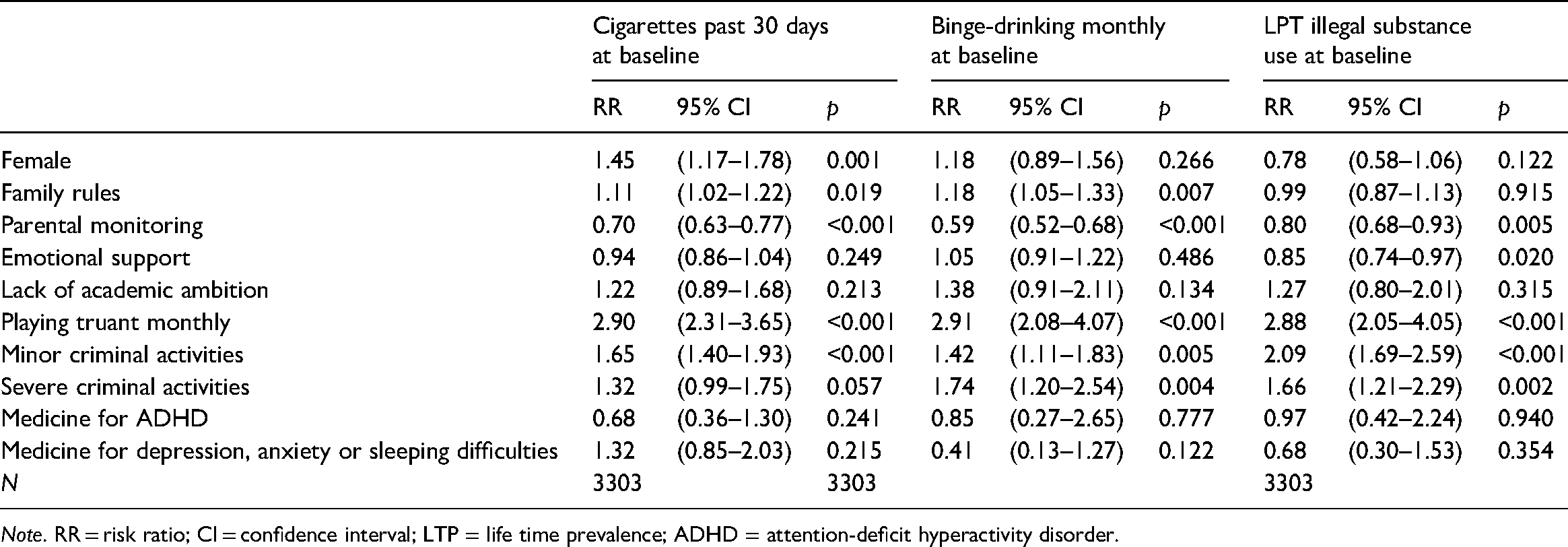
Note. RR = risk ratio; CI = confidence interval; LTP = life time prevalence; ADHD = attention-deficit hyperactivity disorder.
Cross-sectional modified Poisson regressions at follow-up (adjusted).
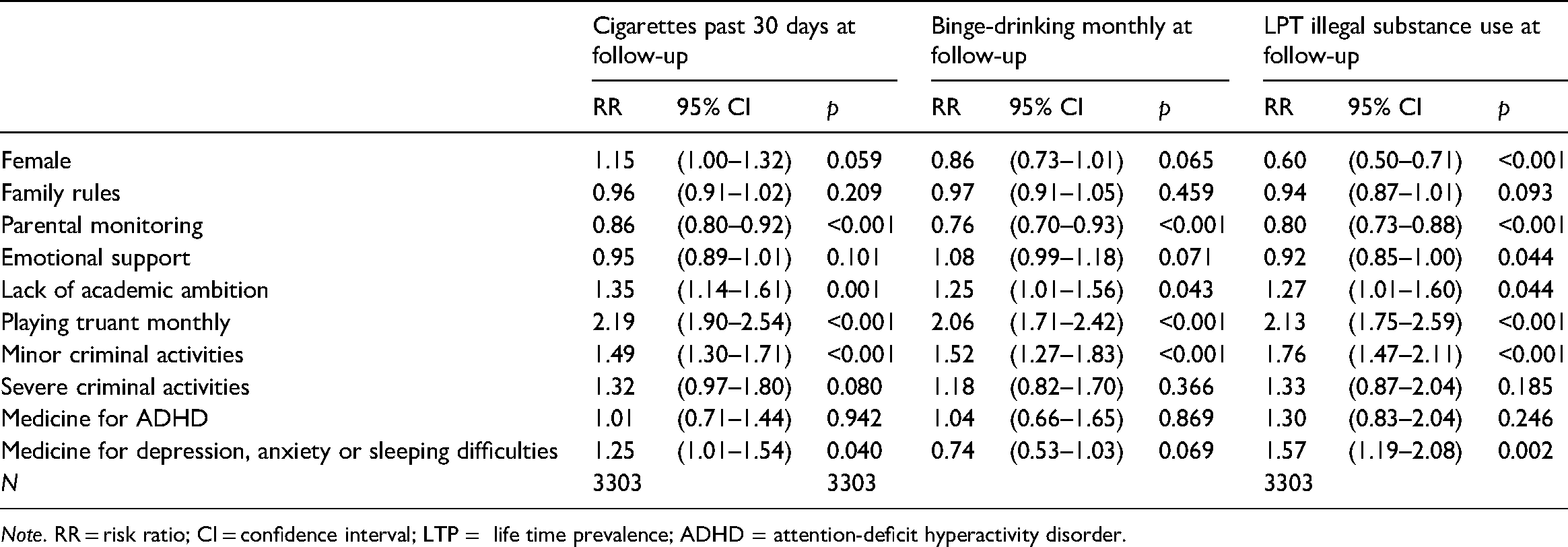
Note. RR = risk ratio; CI = confidence interval; LTP = life time prevalence; ADHD = attention-deficit hyperactivity disorder.
Results
Descriptive statistics
Table 1 presents descriptive statistics for the dependent and independent variables, separately for baseline and follow-up. Besides parental monitoring, all differences in the distribution of the independent variables were statistically significant. In addition to showing quite stable values between time points on some variables (e.g., parental monitoring, criminal activities and medicine for ADHD), the participants reported somewhat decreasing levels of rules and support within the family domain, and increasing levels of truancy and lack of academic ambition. The use of medicines for depression, anxiety and sleeping difficulties doubled between time points.
While not shown in Table 1, it can be noted that only minor gender differences could be seen as regards cigarette use over time and binge-drinking at baseline. Males were more likely to have engaged in binge-drinking at follow-up. Males were also more likely to have used illegal substances at both time points.
As expected, the participants had more experience of legal substances than illegal substances, though it should be noted that the different variables had different time frames. Also, the prevalence of use roughly doubled between baseline and follow-up for all three types of substances. Differences in the distribution of the dependent variables were statistically significant. At follow-up, 19.6% had used cigarettes during the past 30 days, 15.3% had experience of monthly binge-drinking, and 12.5% had lifetime experience of illegal substance use. Cannabis was the dominant illegal substance used and the majority reported having used five times or less in their lifetime (not in the table).
Regression analyses
The results from the unadjusted Poisson regression analyses are shown in Tables 2a and 2b for baseline and follow-up respectively and for all three substances. The majority of risk factors across domains showed clear associations with all substances, although some associations were not statistically significant. For instance, the association between family rules and illegal substances at baseline, and the association between ADHD medicine and legal substances at follow-up were not statistically significant. Strong significant associations with substance use were found within the school domain and criminal activities.
The associations between substance use and variables in the different domains were generally weaker at follow-up, compared to at baseline. The associations between use of different medicines and substance use were somewhat inconsistent, with some associations being more evident at baseline (e.g., ADHD medicine and cigarette use), and some being stronger at follow-up (e.g., medicine for depression, anxiety or sleeping difficulties and use of illegal substances). However, there were no changes in the direction of the associations with medicine use across time points, only in magnitude.
Tables 3a and 3b present the adjusted modified Poisson regression analyses for each substance at both time points. Taken as a whole, the family variables had inconsistent associations with substance use. In the adjusted models, higher level of family rules surprisingly predicted use of legal substances at baseline, while no significant relation could be identified at follow-up. Higher level of parental monitoring was consistently related to a lower probability of use across substances, that is, lower parental monitoring was a stable predictor for substance use. For instance, the risk ratios (RRs) for binge-drinking were 0.59 at baseline and 0.76 at follow-up. While emotional support was significantly associated with several outcomes in the unadjusted models, it was only associated with lifetime use of illegal substances in the adjusted models at both time points (RR 0.85 at baseline and RR 0.92 at follow-up).
As for the school variables, lack of academic ambition significantly predicted use of all substances at follow-up but not at baseline. At follow-up, those lacking academic ambition were 35% more likely to have smoked during the past 30 days compared to those who had academic ambition. For binge-drinking the increased risk was 25%, and for illegal substances it was 27%. A habit of truancy was significantly related to a higher likelihood of use of all substances at all time points. Those who played truant were, across substances, almost three times more likely to use at baseline compared to those who did not, and twice as likely at follow-up, making it a strong, stable predictor for substance use.
Regarding the individual/peer domain, minor criminal activities were significantly associated with use across substances and over time. For instance, the risk of monthly binge-drinking was 42% higher at baseline and 52% higher at follow-up among those with experience of minor criminality, compared to those who had no such experience. Compared to the unadjusted models, the severe criminality variable was less stable across time points in the adjusted models, with few statistically significant associations (binge-drinking and illegal substances at baseline).
Different medicines were, overall, weak predictors of substance use. In the adjusted model, use of ADHD medicine was not significantly associated with substance use at any time point. At follow-up, there was a statistically significant association between use of prescribed medicine for depression, anxiety or sleeping difficulties and use of cigarettes (25% increased risk) and illegal substances (57% increased risk) compared to those who did not use these medicines. We did not, however, find a significant association between use of such medicines and monthly binge-drinking.
Discussion
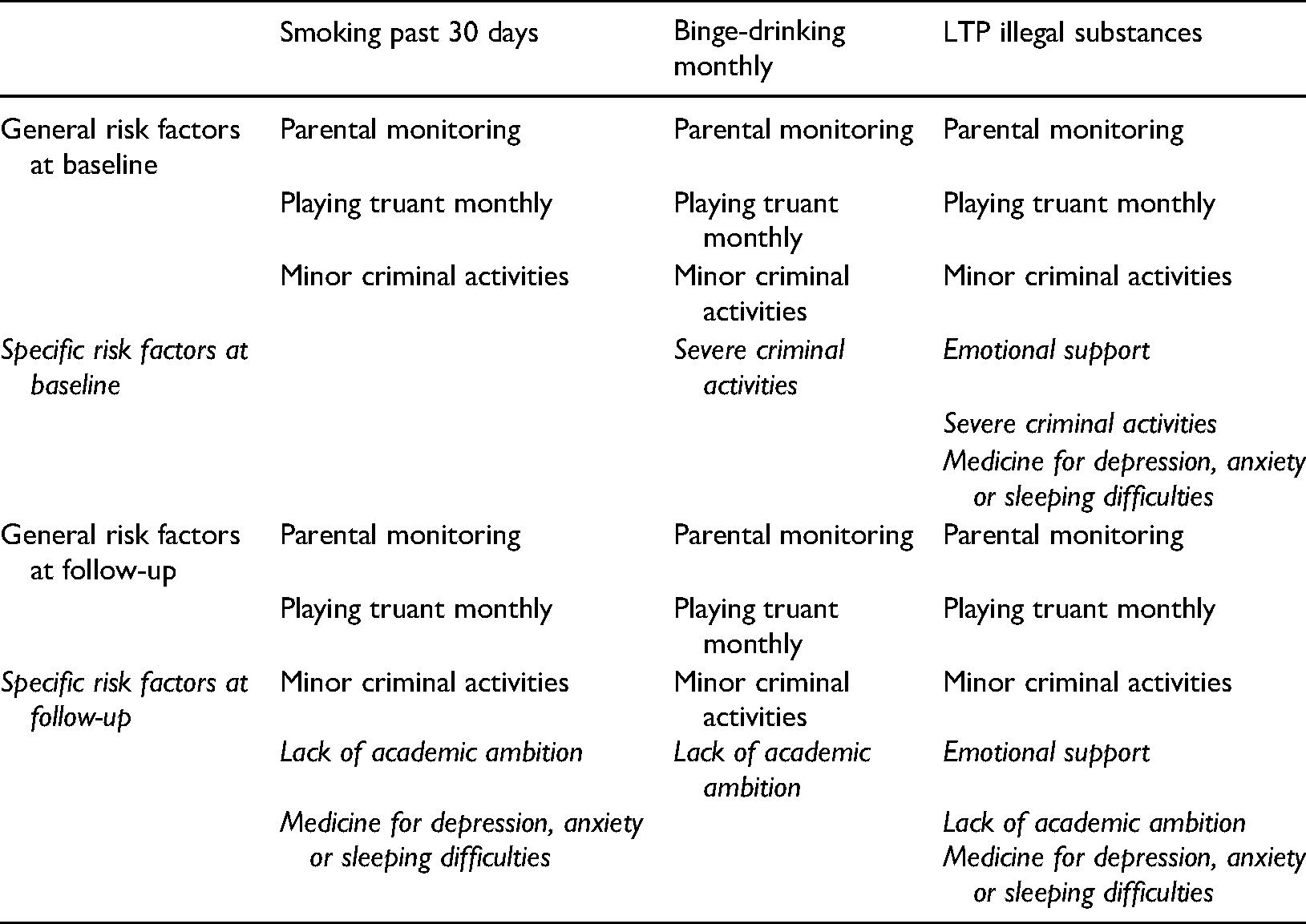
This study confirms some associations between “classic” risk factors and use of cigarettes, binge-drinking and illegal substance use in a representative sample of Swedish adolescents. While it is somewhat difficult to present a cohesive summary of associations across substances and over time, Table 4 summarises significant risk factors for each substance and time point, according to the adjusted modified Poisson regressions. Three risk factors were stable over time and applicable to all substances (“general”), while others were unstable, only significantly associated with a specific substance at a specific time point (“specific”).
Overview of general and specific predictors by substance and time point.
The results suggest that two of three variables from the family domain were inconsistently related to legal and illegal substance use. Previous research has shown that factors within the family domain, for example parental skills and practices, are important predictors of alcohol use in adolescents (Mak et al., 2020; Van Ryzin et al., 2012; Vashishtha et al., 2020). However, the family domain has been considered a weaker predictor across substances than the individual/peer domain (Cleveland et al., 2008; Cleveland et al., 2012), with associations varying by substance and adolescent time period (Mak et al., 2020; Van Ryzin et al., 2012). The different domains may thus be more or less salient over time (Cleveland et al., 2008). The findings related to the family variables in this study cannot uniformly confirm the relevance of the family domain in predicting legal or illegal substance use. Parental monitoring was the only variable that consistently predicted substance use across time points, when controlling for other variables (Van Ryzin et al., 2012).
The school domain also was not consistently associated with substance use. Individuals who reported a lack of academic ambition were significantly more likely to have used different substances at follow-up (Gauffin et al., 2013) but not at baseline. In contrast, previous research has found an association between school connectedness and substance use at 5th grade (Catalano et al., 2004) and 8th grade (Bond et al., 2007).
Corresponding with previous research, a habit of truancy was associated with use across substances (Henry & Huizinga, 2007; Karlsson et al., 2018; Rocque et al., 2017) at both time points and was thus a general risk factor. The associations were strong throughout, with those playing truant having an excess risk of substance use of about three times at baseline and about two times at follow-up. However, as previous researchers have discussed, the causal relations between these variables are likely to be complex; that is, truancy may partly be affected by substance use as well as youth delinquency (Rocque et al., 2017).
Minor criminality in the individual/peer domain showed expected links with use across substances and time points, which corresponds with previous research (Arthur et al., 2007; Pape & Rossow, 2021). The associations were particularly strong for illicit drug use, though notable for the other substances as well. Severe criminality, on the other hand, was only significantly associated with two outcomes at baseline and with none at follow-up in the adjusted models, thus supporting prior work showing that the association may be less evident later on in adolescence or in early adulthood (Cleveland et al., 2012; Epstein et al., 2017; Mak et al., 2020).
The second aspect of the individual/peer domain included in this analysis was use of different medicines. While significantly associated with some outcomes in the unadjusted models, ADHD medicines did not predict use of substances in the adjusted regression models, in contrast to previous findings (Lee et al., 2011). Moreover, partly supporting previous research (Mathers et al., 2006), medicines for depression, anxiety or sleeping difficulties were significantly related to use of cigarettes at follow-up, but not at baseline.
The use of medicine for depression, anxiety or sleeping difficulties was also associated with use of illegal substances at follow-up. Previous research found little evidence of an association between infrequent use of cannabis and depression and moderate evidence of an association between higher levels of use and depression (Degenhardt et al., 2003). Moreover, medicines for depression, anxiety or sleeping difficulties did not significantly predict binge-drinking at any time point, in contrast to previous research (Pape & Rossow, 2021). As these medicines may reduce neurological or mental problems, it is possible that employing such indicators may have led to an underestimation of the “true” association between these conditions and substance use. Being inconclusive and preliminary, these results thus underscore the need for future research on time of diagnosis/treatment, self-medication and the relevance of neurological and mental problems as risk factors for substance use.
What, then, can we make of the associations between risk factors and substance use analysed here? Our study found relatively few, easy-to-grasp tendencies, that would suggest that certain risk factors are more important than others in predicting certain substance use during a certain period of adolescence. Some risk factors – minor criminal activities, parental monitoring and playing truant – were general predictors for all substance use over time. Other risk factors, such as prescribed medicines for depression, anxiety or sleeping difficulties only had specific associations with some of the outcomes. Thus, the findings portray a rather complicated picture pertaining to risk factors for substance use in this large sample of Swedish adolescents.
The results thus generally indicate that some risk factors are related to use of some substances but not others. Additionally, some associations were weaker later in adolescence. Consequently, the assumption of the specific characteristics which distinguish users from non-users, although still largely valid, becomes less pronounced later in adolescence (Arthur et al., 2002; Hawkins et al., 1992). Overall, the public health model for prevention of disease and disorder in part seems relevant for predicting use of different substances for adolescents in Sweden, although the relevance of its different domains appears to vary. A cautious interpretation of the results suggests that substance use, as measured in the present study, can generally be understood as deviant behaviour, due to its association with truancy and minor criminal activities. This interpretation is supported by European data showing decreasing levels of cigarette and alcohol use among adolescents in general, and comparably low prevalence of illegal substance use among young people in Sweden (ESPAD, 2019).
The lack of association between some of the variables in the family domain and adolescent substance use raises some further questions. While it can be expected that the relevance of clear parental rules, monitoring and emotional support in predicting adolescent substance use should decline with age, only parental monitoring was consistently associated with substance use at both time points. Since the family domain, taken as a whole, was inconsistently associated with substance use, a natural recommendation would be to focus prevention interventions on adolescent behaviour, rather than on psychosocial and emotional factors related to their close family networks. However, we believe that such a recommendation would be premature, since other behaviours that are potentially associated with adolescent substance use may be shaped by the socialisation process within the domain of the family, family-based prevention (Mak et al., 2020; Van Ryzin et al., 2012) as well as other tailored public health interventions (Bonnaire et al., 2022) relevant.
Strengths and limitations
A main strength of the current study is the use of a large and nationally representative cohort of Swedish adolescents. The data allowed us to assess the associations between risk factors and legal and illegal substance use at two time points among the same individuals. One limitation worth mentioning is that there were students who, for different reasons, either chose not to fill out the survey or were playing truant on the day of baseline data collection. A total response rate of 82.3% among the students who were invited to participate should, however, be considered adequate. The participation rate at follow-up should also be considered relatively good, with more than 70% of the baseline sample participating.
There are some other important limitations that should be mentioned. The data encompass only a relatively small number of individuals with experience of illegal substance use. This did not allow us to make substance-specific analyses, and potentially important differences across different illegal substances could not be identified. It can also be assumed that those individuals who had extensive experience of illegal substance use were less likely to engage in this research.
In relation to the aim of this study, we had a number of reasonable indicators at our disposal, covering the family, school, and individual/peer domains. However, the data do not cover all risk factors previously outlined (Arthur et al., 2002), and other findings might have been reported had other indicators been included. Subsequent research should be carefully designed to include as accurate indicators as possible, facilitating a more comprehensive test of the public health model for prevention of disease and disorder at different periods during adolescence.
As to the adjusted Poisson regressions, we entered the different risk factors simultaneously, without explicitly considering mediated paths. Some of the risk factors can be assumed to be located at a different “distance” from the outcomes, and controlling for more proximal risk factors may reduce the strength of the association between the former and the substance use outcomes (cf. Westreich & Greenland, 2013). This, however, does not necessarily mean that the more distal risk factors are unimportant, but rather that their association with substance use is transmitted through the more proximal risk factors. For instance, if the criminality measures mediate the link between the family variables and substance use, the family variables can appear to be less important predictors than they in fact are. An example of this would be emotional support, which was more consistently related to substance use in the unadjusted than in the adjusted models.
Also, given that the data are cross-sectional, we emphasise that causal inferences cannot be drawn. Many of the associations identified in this study are likely to be due to reciprocal causation or confounding, rather than solely due to the impact on the risk factors on substance use.
Conclusion
We conclude that the study in part supports the public health model for prevention of disease and disorder. The findings confirm that some risk factors related to the family, school and individual/peer domains are consistent predictors of substance use among Swedish adolescents, while others are not. Our findings show inconsistent associations across substances and time points, and they thus challenge the assumption that the associations between risk factors and adolescents’ substance use are stable over different periods of their lives. Thus, while the findings agree to some extent with the public health model for prevention of disease and disorder, the support for this is far from conclusive. We encourage researchers to continue addressing these issues. Knowing which risk factors are general and which are specific to certain substances or time points is crucial for pushing this field forward. Our study, and another recent Nordic study (del Palacio-Gonzalez & Pedersen, 2022), suggest that the patterns are likely to be complex, and that more research is needed to inform theoretical conceptualisations of adolescent substance use.
According to our findings, policy makers, practitioners and non-governmental organisations that try to prevent adolescent substance use and related harms would benefit from rejecting a singular conceptualisation of this issue (see also del Palacio-Gonzalez & Pedersen, 2022). Our study suggests the need for flexible prevention interventions spanning across substances and domains, which can be modified depending on the heterogenous needs of different age groups.
Footnotes
Disclosure statement
The authors alone are responsible for the content and authorship of the article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Forskningsrådet om Hälsa, Arbetsliv och Välfärd (grant number 2019-00378).