
Abstract
Keywords
After the World Health Organization declared the COVID-19 outbreak a pandemic in March 2020, many governments across the globe responded by implementing a number of restrictions in an attempt to prevent the spread of the virus. As a result, both substance use disorder (SUD) treatment and harm reduction services had to rapidly reorganise their services during the pandemic (Radfar et al., 2021), and changes in service provision became a major concern for service users, professionals affiliated with these services, and society at large (Lopez-Pelayo et al., 2020; Mellis et al., 2021; Zaami et al., 2020). Across many countries, the restrictions had a negative impact on the quality and outcomes of services, including medication-assisted treatment (MAT), needle exchange programmes, drug consumption rooms, and the provision of naloxone to treat opioid overdoses (Bartholomew et al., 2020; Basu et al., 2020; Collins et al., 2020; Crowley & Delargy, 2020; Davis & Samuels, 2020; Douglas et al., 2020; Dubey et al., 2020; Dunlop et al., 2020; European Monitoring Centre for Drug and Drug Addiction [EMCDDA], 2020; Grebely et al., 2020; Whitfield et al., 2020).
However, despite the many difficulties maintaining relevant and quality SUD-related services, studies show that the pandemic also resulted in new and more flexible service provisions, including larger take-home doses for MAT (Trujols et al., 2020), increased outreach treatment and home visits (EMCDDA, 2020; Grebely et al., 2020; O’Carroll et al., 2020), increased distribution of syringes and naloxone (Dubey et al., 2020; Grebely et al., 2020), and increased use of telemedicine (EMCDDA, 2020; Grebely et al., 2020; Roncero et al., 2020). In sum, both SUD treatment and harm reduction services seem to have experienced changes in both positive and negative directions (Radfar et al., 2021).
Considering the relatively short span of the COVID-19 pandemic, an impressive amount of research has already mapped the challenges related to the adjustments and reorganisation of services for individuals with SUDs as a result of the pandemic. However, an emerging topic is examining how the reduced access to service provision during the acute stage of the pandemic may have had a negative impact on the well-being of individuals with SUD beyond their use of substances (DeJong et al., 2020; Wang et al., 2021). Both the pandemic and service restrictions may have exacerbated pre-existing vulnerabilities, such as cardiovascular and metabolic diseases (Bahorik et al., 2017), and psychiatric disorders (Lozano et al., 2017) among individuals with SUD. A qualitative study conducted during the most acute stage of the lockdown in The Netherlands found that SUD patients were more concerned about their health than usual (DeJong et al., 2020). This was related to the fact that health care, in particular MAT, became more difficult during that period. The same study found that the patients were stressed by the reorganisation of services and by how treatment was delivered. For instance, appointments were often cancelled, and appointments by phone or videoconference were missed or interrupted because of a poor internet connection. Some patients worried about relapsing because of the increased social isolation and negative feelings, paired with lack of support from their therapists. Other studies have indicated that changes in service provision and difficulties in delivering MAT may have resulted in increased overdoses and excess deaths in the USA and Canada (BC Coroners Service, 2021; Linas et al., 2021).
The difficulties experienced by individuals with SUD and the new circumstances in the provision of services add to the already difficult effects of the pandemic found in the general population regarding poorer psychological well-being, increased social isolation, and interruption of daily routines (Fernandez-Abascal & Martin-Diaz, 2021). These factors suggest that the pandemic, particularly during the periods with higher governmental restrictions, have brought new challenges to both the service users and the employees, and that new needs may have emerged among individuals with SUD. However, compared to the research concerning limitations in service provision, the changing needs and challenges experienced by individuals with SUD during the pandemic have not been documented in much detail.
Denmark, where the current study was conducted, offers a wide range of free public treatment and harm reduction services (e.g., drop-in centres, health clinics, shelters) for individuals with SUDs across its 98 municipalities. Further, according to the Danish Act on Social Services, there is a guarantee for SUD treatment within 14 days after an initial request for treatment. When the pandemic was declared on the 11th of March, 2020, both SUD treatment and harm reduction services were defined as critical functions that needed to remain open. However, like in other countries, the provision of services had to be adapted to comply with the official guidelines from the National Board of Health for preventing the spread of COVID-19. Although an extensive report from the EMCDDA (2020) has documented many of the challenges faced by SUD treatment and harm reduction services in several European countries during the first lockdown, there has been extremely limited data published from Denmark.
Against this background, we conducted an online study with the aim of documenting changes in SUD treatment and harm reduction services in Denmark during the first and most restrictive lockdown lasting from March 11th to May 25h, 2020. Preliminary data from this study were published in a Danish report (Thylstrup et al., 2020). From these preliminary descriptive data, we sought to further analyse data that could be used to inform the organisation of services beyond the acute stage of the pandemic, and that could speak of the well-being of service users during and after the pandemic. To that end, in the present study, we examined whether the changes in services affected the capacity to meet the service users’ emerging needs during the lockdown period and whether there were indications that the reorganisation of services was related to the users’ well-being. Therefore, we examined (1) positive and negative changes in service provision in SUD treatment and harm reduction services during the first national lockdown, (2) whether the employees experienced challenges in meeting the users’ emerging needs during the lockdown as a result of the pandemic, and (3) the concerns that service users had during the same period.
Methods
Procedure and participants
The study participants were employees working at SUD treatment and harm reduction services in Denmark. They were recruited primarily by email invitations sent to the senior management of a number of workplaces providing with SUD-related services. The managers were asked to complete an online survey and to distribute the invitation and the link to the survey among all employees in their workplace. Furthermore, the invitation and survey link were posted in relevant online groups and professional networks on social media.
Six hundred and thirty-one employees working in SUD treatment or harm reduction services in Denmark accessed the survey between July 10th and September 20th, 2020. Of these, 396 completed the survey. Responses from 23 participants were excluded as the service type of their workplace could not be classified as either SUD treatment or a harm reduction service. Thus, the analysed sample consisted of 325 employees from SUD treatment services and 48 employees from harm reduction services (N = 373). There were no inclusion or exclusion criteria, as we wanted all employees at the services to respond to the questionnaire. Responses were anonymous and voluntary. Data were stored on a secure server at Aarhus University. The project was registered with the Danish Agency of Data Protection.
The majority of the respondents were practitioners with user contact (e.g., social workers, nurses, psychotherapists) (n = 270, 72.4%), followed by management (n = 75, 20.1%), administrative personnel (n = 17, 4.6%), and employees with other functions (e.g., cooks, guards) (n = 6, 1.6%). The majority had an educational background within the social disciplines (n = 209, 56.0%), followed by a health discipline (n = 103, 27.6%), while 37 (9.9%) held a master’s degree, and 23 (6.2%) had other educational backgrounds (e.g., office assistant, students).
Geographical and urbanicity coverage
The respondents were affiliated with SUD treatment and harm reduction services across all five regions in Denmark, and with 61 out of the 98 Danish municipalities. As for the regional location, 39% of the respondents worked in the Capital Region (n = 141), 22% in Southern Denmark (n = 82), 17% in Mid-Jutland (n = 63), 11% in Zealand (n = 41), and 10% in North Jutland (n = 37). Each municipality was categorised into one of five urbanicity groups (Qin, 2005), responding to the municipalities’ population reported by Denmark Statistics. The five urbanicity groups are: capital city (Copenhagen and Frederiksberg; > 700,000 inhabitants), suburban areas near the capital (25,000 to 75,000 inhabitants), provincial cities (over 100,000 inhabitants), provincial towns (10,000 to 99,999 inhabitants), and rural municipalities (less than 10,000 inhabitants). In our sample, the majority of respondents worked in provincial towns (n = 147, 40%), followed by the capital city (n = 97, 26%), and provincial cities (n = 83, 22%). The fewest respondents worked in suburban municipalities near the capital (n = 41, 11%). Data for geographical location were missing for nine respondents, thus neither their region nor urbanicity were classified for them.
Materials and data preparation
The online survey consisted of 25 questions on how the first national COVID-19 lockdown had affected the provision of services for individuals with SUD. The questions referred to experiences during the period between March 11th and May 25th, 2020. After this date, many restrictions started to be lifted on a national level, while other restrictions were imposed at local levels. Therefore, we focused on the most uniform period of restrictions on a national level.
The main areas covered in the survey were: (1) positive and negative changes in service provision, (2) challenges experienced by employees, (3) perceptions of users’ concerns, and (4) level of satisfaction with the response to the pandemic from the government and at the workplace. Questions from areas 1 and 3 were partly based on a study conducted at the same time by one of the authors (EH), which involved interviews with users of harm reduction services and a survey with drug users in Copenhagen (Houborg & Ramsbøl, 2021; Houborg et al., 2021). Area 3 was adjusted to reflect employees’ perceptions of users’ concerns instead of reflecting users' experiences as in the interview-based studies mentioned above. Areas 2 and 4 were new. In the present study, we focused on the first three areas of the survey for which we conducted new analyses.
Changes in service provisions
Participants completed a multiple-choice matrix question with 33 items on changes in specific service provisions (“What changes were caused by the corona lockdown in your workplace from the 11th of March to the 25th of May 2020?”). The items covered seven categories: (1) prevention of COVID-19 (three items), (2) organisation of services (six items), (3) access to SUD treatment (three items), (4) MAT delivery and administration (four items), (5) access to support services (four items), (6) supports for living conditions (seven items), and (7) user contact with practitioners (six items). The provisions of the latter category referred to access to psychologists, physicians, contact persons, outreach teams, modification of meeting formats for appointments (e.g., outdoors), and use of telehealth.
Each of the 33 items could be rated as new, improved or increased, not changed, worsened or reduced, or not relevant for the workplace. We classified reductions and worsening under the umbrella of negative changes (−1), and new, improved, or increased services under positive changes (1). Items marked as “not changed” were scored 0, whereas “not relevant” answers were not used for the analyses. Although we had grouped items into categories, any given item was relevant for a different sub-sample of employees, and thus we analysed the items individually.
Challenges experienced by employees
An eight-item checklist asked the respondents to select from the list the major challenges experienced during the lockdown period (“What were the major challenges that you experienced in your workplace during the lockdown?”). The items included lack of COVID-related protection supplies, challenges related to maintaining a safe physical distance, worries regarding risk of COVID-19 infection, using new technology, meeting the emerging needs of the service users because of the pandemic, experiencing anxiety and stress, “other”, and “do not know”. More than one item on the checklist could be selected, and thus we coded individual items as 1 = selected or 0 = not selected. This coding was used to estimate the percentage of employees endorsing specific challenges.
Service users’ concerns
Perceived concerns among the service users during the lockdown period were selected from a checklist with six items: concerns regarding COVID-19 infection (e.g., being infected, infecting others), use of substances (e.g., access to), living conditions (e.g., housing), physical and mental health (e.g., loneliness, anxiety), social relationships and isolation, and not being concerned. Again, more than one item in the list could be selected, and we calculated percentages for each of the concerns.
Analytical strategy
First, we report the mean change in existing service provisions and their direction. We interpret means under zero as referring to negative changes, and means above zero as positive changes. Due to the different sample size between SUD treatment and harm reduction services, the means for each service type are reported separately. We also report the percentage of employees who experienced the different challenges listed, as well as the percentage of users’ concerns observed by the employees.
There were two sets of main analyses. The first set examined whether changes in contact with the service users were associated with employees’ perceived challenges in meeting users’ emerging needs. For these analyses, we conducted six logistic regressions, in which having challenges in meeting the service users’ needs was the (binary) dependent variable, and the ratings for the changes in the six types of contact with the practitioners were the independent variables. The regressions were conducted separately for each of the six types of contact given that specific provisions were not relevant for all employees, thus introducing a variable sample size per question. As a means to contextualise the interpretation of the findings, we conducted supplementary analyses employing the remaining 27 service provisions from the other survey categories.
The second analysis focused on the association between user concerns identified by the employees and perceived challenges in meeting service users’ emerging needs. As we did not have direct data of the needs experienced by the users, this analysis allowed us to connect the emerging needs with the concerns that employees perceived. We employed a single multiple logistic regression, in which the (binary) variable on experiencing challenges in meeting users’ needs was again the dependent variable, whereas the six potential user concerns were the independent variables. In this analysis, a single multivariate logistic regression model was possible, as we had answers from all respondents for each of the six concern items.
All logistic regression models controlled for service type (SUD treatment vs. harm reduction service). Effect sizes are reported as adjusted odds ratios (AORs).
Results
Changes in existing service provisions
Employees across SUD treatment and harm reduction services identified both positive and negative changes in service provisions during the lockdown period. Table 1 shows the mean changes for each service provision.
Perceived changes in services provided by SUD treatment and harm reduction centres.
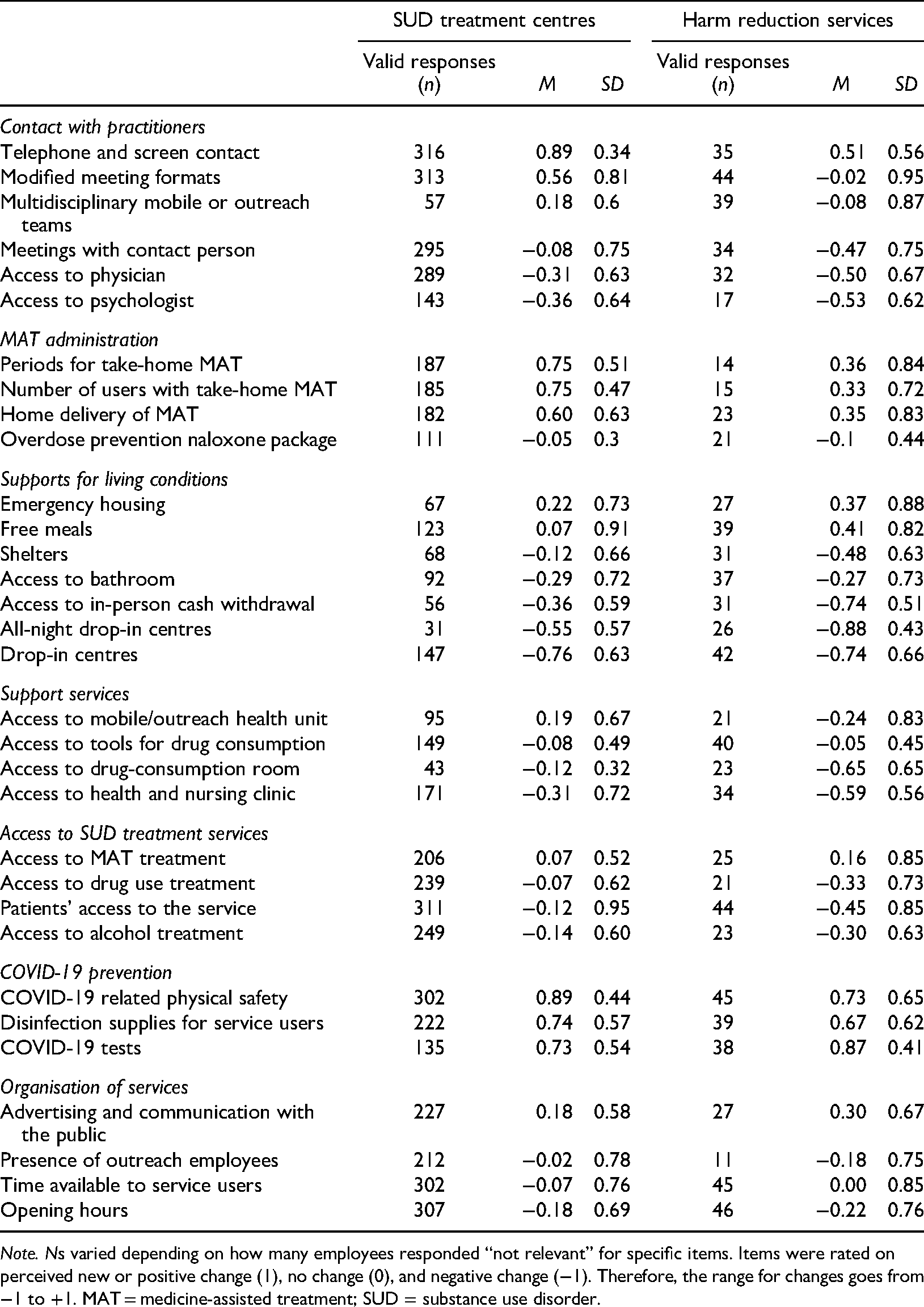
Note. Ns varied depending on how many employees responded “not relevant” for specific items. Items were rated on perceived new or positive change (1), no change (0), and negative change (−1). Therefore, the range for changes goes from −1 to +1. MAT = medicine-assisted treatment; SUD = substance use disorder.
Within the treatment services, the three highest ranked positive changes were the use of phone and/or screen contact (i.e., telehealth), increased COVID-19 related physical safety, and longer periods for take-home MAT medicine. Within the harm reduction services, the three highest ranked positive provisions were access to COVID-19 tests, supply of disinfection supplies for service users, and COVID-19 related physical safety. In both SUD treatment centres and harm reduction services, the three most negative changes were access to all-night drop-in centres, access to cash withdrawal in person in the bank (a common method for this population), and access to drop-in centres in general (see Table 1).
Provisions related to direct contact with practitioners
Use of screens or phones (i.e., telehealth) were rated as the most positive change in both SUD treatment and harm reduction services, whereas access to physicians and psychologists were ranked as the most negative changes across both service types. Other positive and negative changes related to contact with practitioners differed between service types (see Table 1).
Challenges experienced by employees
The most frequent challenge in both SUD treatment and harm reduction services was (not) meeting the emerging needs of the service users during the lockdown period (35%). The frequency of this challenge was not statistically different between service types (see Table 2). Lack of concern for keeping physical distance was the second most frequent challenge identified across both services (30%). This challenge was significantly more frequent within the harm reduction services. Worries regarding COVID-19 infection, use of new technologies, shortage of supplies to protect against COVID-19, and anxiety and stress were endorsed by less than 30% of all employees (see Table 2).
Percentage of employees experiencing different challenges during the lockdown.
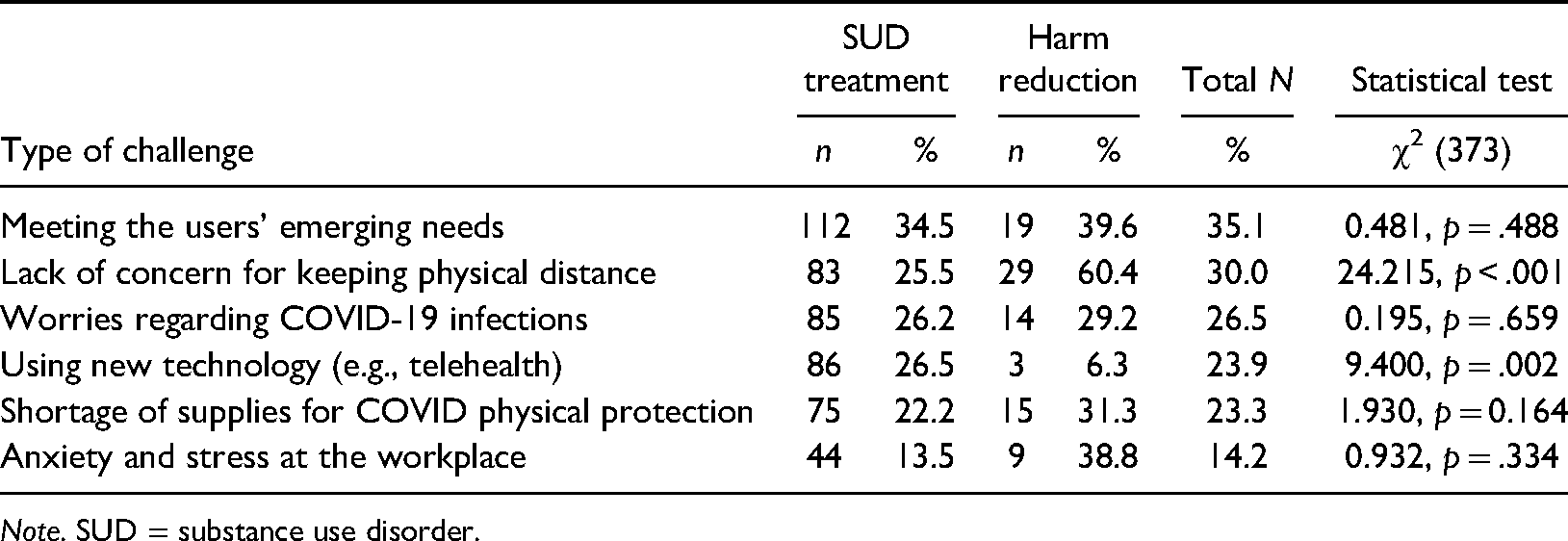
Note. SUD = substance use disorder.
Employees’ perceptions of service users’ concerns
According to the employees, the most frequent concerns among the service users were related to COVID-19 infection (n = 308, 83%), social interaction and isolation (n = 295, 79%), and reduced physical and mental health (n = 243, 65%). The distribution of these concerns did not differ significantly between service types (ps > .050). However, concerns over living conditions, χ2(373) = 22.7, p < .001, and substance use, χ2(373) = 6.25, p = .012, were endorsed more frequently in harm reduction services (living conditions, 65%; substance use, 29%) than in SUD treatment (living conditions, 28%; substance use, 15%). Only four percent (n = 16) of the employees reported that the service users were not concerned about any of these areas.
Relation between changes in the services and challenges in meeting service users’ emerging needs
Four out of the six questions asking about changes in direct contact with practitioners were significantly associated with challenges in meeting the users’ emerging needs during the lockdown (see Table 3). When controlling for service type, negative changes in the access to multidisciplinary mobile or outreach teams, as well as reduced or worsened access to physicians, psychologists, and contact persons, all predicted higher odds for reporting challenges in meeting the users’ emerging needs. Changes in the use of telephone and screen contact, as well as modified formats for appointments were not significantly associated with reporting challenges in meeting users’ needs. Table 3 presents the AORs for all the associations examined in the main analyses.
Relation between challenges in meeting the users’ emerging needs, changes in contact with practitioners, and users’ concerns.
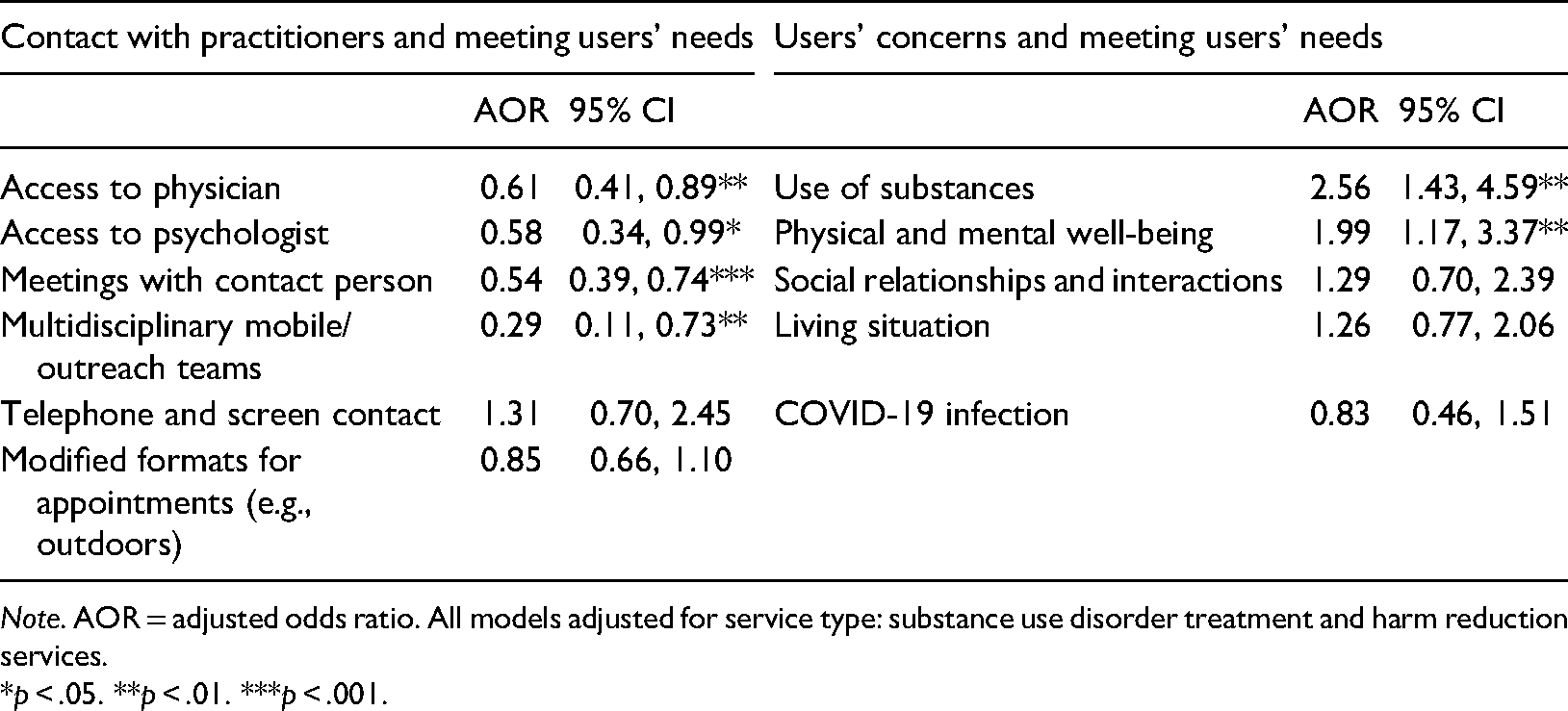
Note. AOR = adjusted odds ratio. All models adjusted for service type: substance use disorder treatment and harm reduction services.
*p < .05. **p < .01. ***p < .001.
Supplementary analyses.
When examining the remaining 27 service provisions, we found that negative changes in the number of users with take-home MAT (AOR = 0.53, p = .033), periods for take-home MAT (AOR = 0.53, p = .019), presence of outreach employees (AOR = 0.65, p = .019), time available to service users (AOR = 0.60, p = .019), and options for appointments (AOR = 0.62, p = .019) were significant predictors of experiencing challenges in meeting users’ needs. The remaining 22 service provisions were not significantly associated with challenges in meeting users’ needs (ps > .05; data not shown).
Relation between perceived service users’ concerns and meeting their needs
Perceiving that the users were concerned about their substance use, as well as their physical and mental health was significantly associated with difficulties in meeting the users’ emerging needs (see Table 3). Other users’ concerns, including concerns about COVID-19 infection, social relationships and interaction, and living situation were not associated with the employees’ difficulty meeting the users’ emerging needs.
Discussion
To our knowledge, this is the first study examining in detail how the COVID-19 restrictions during the first lockdown period in Denmark affected SUD treatment and harm reduction services. It is also the first study examining whether the changes in service provision were related to difficulties in meeting the emerging needs of the service users. We found that according to the employees, the lockdown resulted in both positive and negative changes in service provision; however, the majority of these changes were perceived as negative. Beyond documenting changes in service provision during the first lockdown in Denmark, we found that (1) negative changes in the contact with practitioners were associated with challenges in meeting the users’ needs, and that (2) difficulties meeting the emerging needs of the service users during the lockdown were linked to concerns with their physical and mental health, as well as patterns of substance use. Our findings helped in identifying key research areas to focus on as we move through and out the pandemic, by considering the more extended consequences that service restrictions and reorganisation may have had for the well-being of service users.
Regarding users’ direct contact with practitioners, there were negative changes in terms of access to physicians, psychologists, multidisciplinary outreach teams, and primary contact persons. At the same time, there were positive changes regarding the formats of appointments and the use of telehealth. However, only the negative changes in access to practitioners (e.g., physician, psychologist, outreach worker) were significantly related to experiencing difficulties in meeting users’ needs, thus suggesting that access to practitioners who support the physical and mental health of individuals were considered key services during the pandemic. That this may indeed be the case, is further supported by the findings that when users were particularly concerned about their substance use, and physical and mental health, the employees were more likely to experience challenges in meeting the users’ needs. This result pattern further aligns with DeJong et al.'s study (2020) in which SUD patients reported stress and worries accessing services during the lockdown, as well as frustration due to lack of support from their therapists. Therefore, the potential impact that the pandemic and service restrictions may have had on the service users’ physical and mental health are a key area for research in the near future.
We also found positive changes in the use of telehealth in Denmark, particularly within the SUD treatment services, which is in line with findings from other European countries (EMCDDA, 2020). However, the use of telehealth was not related to (not) experiencing difficulties in meeting the emerging users’ needs during the first lockdown. The use of telehealth during the pandemic for SUD-related services has been a major focus of discussion in the COVID-related research, and many researchers and service providers anticipate an increased use of telehealth for delivering SUD-related services (Lopez-Pelayo et al., 2020; Roncero et al., 2020), including for MAT (Grebely et al., 2020), after the pandemic. While this may be an exciting opportunity for the field, our findings also suggest that in order to maximise the impact of the use of telehealth, and digital tools more broadly, both SUD treatment and harm reduction services will need to evaluate their implementation to determine how these technologies can be used to better address the needs of service users.
The supplementary analyses suggested that changes in MAT administration as well as the broader organisational changes, such as reduced time available for service users, were also related to challenges in meeting the users’ needs. Regarding MAT administration, international research suggests that this varied to a great extent between countries during the pandemic (Dubey et al., 2020; Dunlop et al., 2020; Grebely et al., 2020). For example, Spain has reported increased flexibility in provision of MAT (Trujols et al., 2020), whereas other countries have faced significant challenges providing MAT, especially during the first months of the pandemic (Collins et al., 2020). Therefore, flexible MAT administration is another key area to be investigated in order to understand the impact of the changes in MAT administration on the physical health of the service users, as well as its efficacy in addressing drug use.
Lastly, we identified a number of other negative and positive changes in service provision that were not significantly linked to meeting the users’ needs. Among these other negative changes there was a reduced access to physical facilities (e.g., drop-in centres, shelters, bathrooms, drug-consumption rooms), and overall access to the services. These negative changes were in line with difficulties reported in other European countries during the same period (EMCDDA, 2020). Among other positive changes found, there was the introduction or improvement of COVID-19 safety measures (e.g., providing disinfection supplies to service users), and supporting the users’ general living conditions (e.g., emergency housing, food). However, our data suggest that these changes were not particularly salient for the employees as factors relevant for (not) meeting the users’ needs during the lockdown, which further reinforces the importance of securing direct contact with practitioners despite service reorganisation.
The positive changes found in services for SUD during Denmark's lockdown suggest a more positive picture compared to some European countries. However, at the same time, our findings also align with the concerns expressed early in the pandemic regarding the increased adverse consequences as a result of COVID-19 (Dunlop et al., 2020; Murphy et al., 2021; Zaami et al., 2020). Individuals with SUD are at particular risk in relation to drug-related health and psychological problems due to the pandemic and the lockdown (Mallet et al., 2020).
Implications and recommendations for future research and policy
We have identified four important areas that should be addressed in future research and practice. First, the present study highlights the need to examine the long-term consequences that the reduced access to SUD services may have had on the service users’ physical and mental health (Dunlop et al., 2020; Murphy et al., 2021; Zaami et al., 2020). Here, a more systematic examination could include register-based studies on changes in admission rates and drop-outs from SUD treatment and psychiatric treatment before, during, and after the pandemic.
Second, with the increased use of telehealth and of other digital technologies for SUD services, it will be important to assess their feasibility and efficacy within different service types. In our study, we found that the use of technology was unrelated to perceived challenges in meeting the users’ needs; however, DeJong et al. (2020) found that SUD patients experienced barriers in using technology during the pandemic. Although the use of digital technologies for SUD treatment pre-dates the pandemic (Nesvåg & McKay, 2018), the present findings highlight the need to explore and understand the opportunities and limitations of digital technologies in service provision (Blanco et al., 2021). Studies on access to the required technology among services users, as well as service users’ attitudes towards digital technologies, could be important starting points to address.
A third important area is to continue evaluating the impact that the changes in provisions of MAT have had on the service users’ health. Specific examples are examining the relation between changes in MAT delivery and hospital visits resulting from drug overdoses, as well as increased risk of all-cause mortality (Hesse et al., 2021). Lastly, a key area for policy will be devising protocols to smooth out transition periods of rapid reorganisation in SUD services, with particular attention to securing a continuous support for the users’ physical and mental health. In agreement with Radfar et al. (2021), we suggest that clear and effective regulations and communication are needed within the services and with the service users during periods of rapid reorganisation in order to mitigate the concerns and frustrations that both individuals with SUD and service providers may experience. In this regard, alternatives for collaboration across sectors may also help in optimising services during periods in which different service types are restricted (EMCDDA, 2020).
Taken one step further, a potential research area deriving from wider national data, such as registers, is the identification of sub-groups of service users who might be at higher risk of becoming ‘invisible’ during periods of service reorganisation. According to a report from the EMCDDA (2020), a reduced user contact with SUD-related services in some European countries during the first months of the pandemic was partly due to service users not actively seeking help. Relatedly, an international study found that immigrants and refugees were the most affected service users in both low-income and high-income countries (Radfar et al., 2021). Therefore, studies with larger samples and historical data may help in identifying individuals who are particularly vulnerable during pandemics or other emergencies leading to service reorganisation. As noted by Volkow (2020), social support from professionals, families and others is essential for individuals with SUD, and the social isolation and major reorganisation of service provisions during the lockdown present additional barriers that can work against their recovery, and may even contribute to greater social inequality and marginalisation among this population.
Finally, we note that some of the recommendations for future research and policy may be relevant to other patient groups and individuals experiencing other forms of addictions. For instance, a recent Finnish study with gamblers identified mixed attitudes towards using telehealth in treatment of gambling behaviour, and found that individuals normally accessing interventions for gambling also experienced difficulties navigating service reorganisation (Marionneau & Järvinen-Tassopoulos, 2021). Thus, the present findings may provide a broader basis to examine the consequences of the reorganisation of intervention services and their intersection with users of physical health, mental health, and addiction services.
Limitations and strengths
This study is the most detailed investigation to date reporting employees’ experiences of the changes in service provision in Denmark during the first lockdown caused by the COVID-19 pandemic. However, there were several limitations to our study. First, some of the service provisions examined were not relevant to all workplaces, thus the generalisation of the results to specific workplaces may be limited. Relatedly, most regions and urbanicity areas were well represented when compared to the actual distribution of services in Denmark (Ministry of Social Affairs and Senior Citizens, 2021). However, there was a slight overrepresentation of employees working in the Capital Region (expected: 28%; obtained: 39%), and no representation from workplaces in rural towns. Second, the way the matrix question was posed in relation to changes in the provision of 33 specific services was ambiguous for some items as the response options could indicate an objective change in one direction (either increase or decrease), that was also compatible with a subjective interpretation in the opposite direction (improvement, worsening), for which the respondent had to choose one. This ambiguity was more problematic for some of the items in supplementary analyses, whereas the items referring to practitioners were likely to be compatible only in one direction (i.e., a decrease in contact with physician is unlikely to be rated as improved access at the same time). Thus, we caution towards the interpretation of the findings deriving from supplementary analyses. Third, our data were based on self-report and on the employees’ perceptions only. That is, we did not document the experiences of service users and do not have direct examples of the emerging needs experienced by service users. This information would also be important to direct decisions on service reorganisation and establishing priorities in the future.
The study has important strengths, including a large sample size, a good geographical coverage, and respondents with a wide range of educational and professional backgrounds. Further, the findings have important implications for the future development of service provisions for individuals with SUD in the event of future service restrictions related to COVID-19 and for future quality development in general.
Conclusions
During the first lockdown in Denmark, employees within SUD treatment and harm reduction services identified access to physicians, psychologists, primary contact persons, and the outreach teams as central for meeting the service users’ needs. Employees were more likely to experience challenges in meeting the users’ needs when the service users were perceived to be concerned with their physical and mental health, as well as with substance use during the pandemic. Our findings suggest that the needs of service users may shift during periods of rapid and drastic reorganisation of services. Key areas for future research and policy are focusing on supporting the physical and mental health of service users, investigating the potential and limitations of a more flexible MAT administration and telehealth, and preparedness for rapid service reorganisation.
Footnotes
Authors' contributions
APG: Conceptualisation, investigation, methodology, data curation (coding and preparation), formal analysis, writing (first draft, reviewing, and editing), visualisation. BT: conceptualisation, investigation, methodology, data curation (coding), writing (first draft, reviewing and editing). EH: conceptualisation, investigation, methodology, data curation (coding), writing (editing, reviewing).
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Danish National Board of Social Services (Socialstyrelsen).