
Abstract
Background:
In accordance with recommendations from The United Nations’ Chief Executives Board of Coordination, several countries are in the process of reforming their punitive drug policies towards health-based approaches – from punishment to help. The Portuguese model of decriminalisation is generally seen as a good model for other countries and has been scientifically described in favourable terms, and not much scrutinised.
Method:
This article draws on foucauldian archaeological and genealogical approaches in order to understand and compare governance logics of the 19th century Norwegian sobriety boards and 21st century Portuguese commissions. In doing this, we problematize contemporary drug policy reform discussions that point to the “Portuguese model”, which aims to stop punishing and start helping drug-dependent people, are problematised.
Findings:
The Portuguese commissions investigate whether drug-using people are dependent or not. Dependency, circumstances of consumption and their economy are considered when the commission decides on penalising, assisting, or treating the person, or a combination of all this. This model was studied alongside the Norwegian sobriety boards mandated by the Sobriety Act that was implemented in 1932. Sobriety boards governed poor alcoholics. Authorities from the sobriety movement were central in creating sobriety policies that culminated in sobriety boards. The Portuguese commissions have similarities to Norwegian sobriety boards. They make use of sanctions and treatment to govern people who use illicit substances to make them abstain, with the view that this is emancipatory for these people. The different apparatuses have distinct and different ways of making up, and governing their subjects.
Conclusion:
This article contributes to debates on drug policy reforms and aims to investigate whether they might produce biopower effects of governance masked by an emancipatory language. There is a need for critical studies on drug policy reforms to avoid policies that maintain divisions and control marginalised populations.
In recent years, punitive drug policies have been widely criticised (Godlee & Hurley, 2016; Slagstad, 2016). Several countries have reformed, or are in the process of reforming their drug policies (Eastwood et al., 2016). The United Nations Office on Drugs and Crime (UNODC) have urged countries to provide treatment instead of punishment for drug-dependent people (UNODC, 2009). Recently, the Chief Executives Board of the United Nations endorsed decriminalisation of possession of illicit substances for personal use (Chief Executives Board for Coordination, 2019). Drug policy debates in the media in Ireland (Armstrong, 2019; Holland, 2018), New Zealand (New Zealand Drug Foundation, 2019), Latvia (Latvian Public Broadcasting, 2019), and Norway (Johnsen, 2017), have all referred to the Portuguese decriminalisation reform as a potential model for their own countries. The Portuguese policy was termed “best practice” by The International Narcotics Control Board (INCB) at the United Nations General Assembly Special Session on Drugs (UNGASS) in 2016 (Zipp, 2015). This “Portuguese model” has been widely promoted in mass media reports that criticise the practice of punishing sick people for minor drug law violations and promote treatment for their dependency instead (Aleem, 2015; Baer, 2016; Ingraham, 2015; Kristof, 2017; Oakford, 2016). In academic literature, the Portuguese reform has generally been described in favourable terms (Greenwald, 2009; Hughes & Stevens, 2012; Smiley, 2016), and has barely been scientifically scrutinised – especially in terms of whether the reform has emancipated drug users.
A recent article on Norwegian drug policy discussions suggested some similarities between the Portuguese Decriminalisation Act of 2001 and the much older Norwegian Sobriety Act of 1932. On the basis of both these laws, commissions were established with the aim of governing people with drug use or alcohol problems, by counselling and sanctioning them (Johansen et al., 2018). This current article, therefore, studies and compares the biopolitics of these two different systems by reading the laws that regulated them and studying their contexts, to better understand them. The differences and similarities in the interplay between power and knowledge and how the human subject is made, are examined. Moreover, we look for how these systems are planned and realised in their exercised biopolitical power over subjects.
In summary, this article makes clear the governance logics and repertoires of said systems and shows that they, albeit modelled differently according to sociocultural and historical contexts, with different views on substances and governable subjects, build similar sorts of power influence and that the sobriety boards perhaps were not as authoritarian as might have been believed, and that the Portuguese system involves more control than is reported in mass media and scientific studies. Moreover, it shows that a shift from punishment to treatment is not a straight-forward process and not necessarily as emancipatory as it is sometimes presented to be. Such shifts perhaps may even characterise discourses that serve to legitimise and ensure a continuation and cementation of control practices exercised on marginal populations by embedding them in a scientific and “neutral” language.
Method and theoretical seating
For this article, Foucault texts were read (e.g. Foucault, 1980; Foucault, 1991; Foucault and Rabinow, 1984) and concepts and thoughts were borrowed to analyse historical accounts and locate ruptures, cracks, and breakages in the different idea trajectories. This is done using an analytic strategy that draws on archaeology of discourses, power, and regimes, and by unfolding the making of governed subjects and an essence of the phenomenon of addiction. Moreover, a genealogical approach was drawn upon to point out logics of different power relations that have come into being over time through discursive changes, and that manifest themselves via different apparatuses. The aim of this study was to use historical accounts to be able to point out inherent problems with recent drug policy reform discussions, that point to the “Portuguese model” which promises to stop punishing and start helping and emancipate substance-dependent people. The study considers in what way various power exercises get their nourishment and how they are depicted as functioning in view of the governed subjects, their actions, and realities, locating similarities and differences between the investigated apparatuses. According to Foucault (1977), a genealogy is a historical analytical account, where the aim is to critically unfold entanglements of logics that normalise certain views on problems (Thomas et al., 2016). The genealogy seeks to thematise relations between truth, theory, values, and the social institutions from where they emerge. By doing this, it discloses the relationship between power, knowledge and the subject (Foucault, 2014), and it shows how power and knowledge come together, and how subjects are positioned in fields of power−knowledge (Biesta, 2008). Power is not necessarily prohibiting and residing with the state, but is complex and dispersed through power relations in the social body (Foucault, 1980).
Moreover, the concepts of biopower and biopolitics are used, and refer to processes whereby power relations make possible the control of populations by channelling self-governance and other governmentalities (Eliassen, 2016; Farsethås, 2009). Contemporary biopower is a politics dependent on the domination, exploitation, and expropriation of the vital existence of subjects it is exercised over (Rabinow & Rose, 2006). Biopower includes at least one or more truth discourses regarding the “vital” character of living humans, and authorities that speak the truth about it. Said discourses can combine biological and demographic, or sociological styles of thought. Moreover, it must include strategies for interventions upon collective existences in the name of life and of health. In addition, modes of subjectification must be included, in which individuals are made to work on themselves. This happens under a form of authority, in relation to the truth discourses, in order to address their own health, life, and their family’s or some other group, or the population (Rabinow & Rose, 2006). It is the administration of life through the mix of biology and politics for ensuring, sustaining, and multiplying life in the interest of productivity; it works through bodies in different modes of governance. The biological perspective involves the site of the body for discipline and control.
Moreover, propositional truths are integral to the development of law, and therefore, forms of power that have played an important role in modern times. Constitutive to the genealogy therefore, is a critique of norms, laws and patterns taken for granted and claimed as neutral; it is a critique of propositional truth that is law’s pretentions to be pure and unsullied by the blatant use of power (Foucault, 2014). Law permits perpetual dominations and stages repeated scenes of violence (Foucault, 1984). Such an interruption of what is constitutive of everyday life, habits and memories, can raise awareness about how we are involved in the event-full movement from moment to moment; that they are part of the production of “reality”, truth, values etc. (Pløger, 2016). Historical events become complicated and pluralised through an investigation of their constitutive elements, their relations, and points of reference (Biesta, 2008). By breaching what is taken for granted, one shows that things are not necessarily what they seem (Burchell et al., 1991). Therefore, this approach might bring about a situation in which what has up until then been taken for granted, becomes problematic, difficult, and dangerous (Biesta, 2008). By unsettling the taken-for-granted, the analysis opens up a space, and a demand for judgement (Foucault & Rabinow, 1984). This study takes the Portuguese model and the Norwegian sobriety boards and compares them in order to deconstruct a taken-for-granted premise of the emancipatory nature of decriminalisation that characterises contemporary drug policy reform discussions.
In contrast to other methodologies, a study like this that draws on the genealogical and archaeological approaches, attains its efficacy not from its neutrality, but from its politicisation (Crano, 2011). It does not try to produce objective truth, but truth-claims that may have a political significance by opening up for potential futures (Foucault, 1991; Foucault & Rabinow, 1984). Past events are not seen as leading to the present, but used in order to establish the radical otherness of it, its difference, by seeking out familiarities, contingencies, and emergences (Foucault & Rabinow, 1984). What follows from this is that the approach is necessarily selective, and in part steered by the researcher’s judgement of what is seen as important and relevant with regard to the topic (May, 1993; Mills, 2003; Thomas et al., 2016).
In carrying out this study, Law No. 30/2000, of 29 November, The Sobriety Act of 1932, and the revised version of 1939, were studied together with selected contextualising literature picked from database searches. The journal database JSTOR was searched with the search string ((“Sobriety boards” OR “Temperance boards”) AND boards) AND (alcohol*) AND ((Norway) OR (Sweden)), with 26 results, where five articles were considered relevant to the topic and time-frame of the Norwegian sobriety policies. The National Library of Norway database was searched using the search string “edruskapsvern” OR edruskap* OR “lov om edruskapsvern” OR edruskapsnevnder OR edruskapsnemnder, with 30 results, of which five were excluded. Based on the results, four more texts were found through a manual search. To investigate the Portuguese decriminalisation act and its context, Hein Online was searched with the search string ((drug*) AND (policy*)) AND (decriminal*) AND (portug*) with 26 results, and a social citation index with ((drug*) AND (policy*)) AND (decriminal*) AND (portug*) that produced seven results. Articles in Portuguese language were not included. In order to situate the legal texts, secondary literature was searched and read on how the target population has been addressed (e.g., Hamran, 2005; Skålevåg, 2008). Historical literature and topical study reports were found through a literature search, a manual search of certain journals and review of indexes and references from relevant sources. In the following, the “Norwegian model” and the “Portuguese model” are used as normative frameworks and described with one chapter each that describes the context, and one chapter that describes the special commissions and models with references to the legal texts in question. Then, the uncovered relationships between power, knowledge and the subject in each model are presented and jointly analysed.
The Norwegian model: The poor alcoholic is freed from immoral drinking
In late 19th and early 20th century Norway, the use of alcohol was a defining political issue (Hamran, 2005). Regarded as the biggest political movement in Norway, the sobriety movement fought for abstinence, sobriety, and alcohol prohibition. It consisted of individuals, associations, and orders such as the International Order of Good Templars (Strøm, 1944), which originated in Utah and came to Norway in 1877 (Haave, 1940). By 1919, they had succeeded in achieving prohibition only to lose it seven years later when alcohol distribution was legalised by referendum (Sørli, 1944). This crippled the movement (Haave, 1940). Following this, they started addressing individual alcoholics rather than the more ambitious goal of creating an alcohol-free society (Hamran, 2005). For this purpose, special commissions, sobriety boards, were established (Skålevåg, 2008).
The movement linked alcohol use to debasement, animality, and evil – abstinence to truth, man, and God. In a speech to the 1857 annual meeting of the Norwegian Association Against Spirits, Bishop Jens Lauritz Arup stated that religion and reason would be used to fight the use of spirits. The movement, he claimed, should come together under the banner of Christianity and speak in the Lord’s name, led by the righteous words of the scripture and strengthened by God’s spirit against the evils of drunkenness, its debasement and its conflict with all that is Christian. Moreover, the way of reason, with its sound judgement, science and empiricism, would succeed in making people conclude that the use of spirits, when not medicinally applied, was abuse and ruinous (Arup, 1890). All use of spirits was misuse, and led to the damnation (misery, crime, poverty, and early death) of people ruled by drinking (Brun, 1890; Meling, 1931). Alcohol use encouraged abuse of women and children and, when it became common, ruined the very core of society (Brun, 1890). Therefore, the combination of religion and reason would result in a prohibition as willed by the people (Arup, 1890). This reasoning was systematised and put into practice by the International Order of Good Templars (IOGT). To be initiated, one had to abstain from alcohol and not provide it to others. On that basis, the templar would work for an army of light (Sørli, 1944), world peace, and brotherhood between all peoples. Consisting of five degrees, the aim of the order was to purify people and society, impossible without first being abstinent. Alcohol use was the vice at the base, or below the base, of the temple – world peace was at the top. Faithfulness, mercy, and justice were scaled between (see Figure 1) (Strøm, 1944).
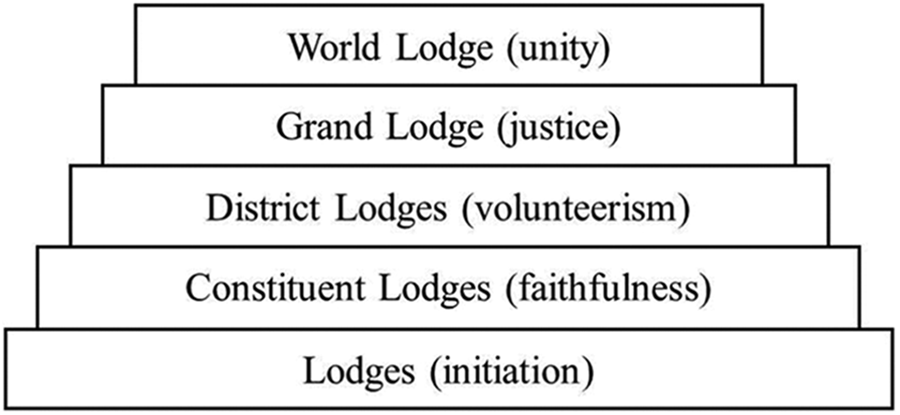
International Order of Good Templars lodge system.
Since the most damaging effects of alcohol use were seen among the lower classes, people of good standing should become members of the movement out of social responsibility (Stang, 1890). Among the poor, drinking was linked to disease, bodily weakness, accidents, laziness, vagrancy, moral transgression, sexual misconduct, crime, and the costs of judicial inquiries (Faye, 1890). Scientific studies concluded that alcohol slowed the brain and disintegrated muscles and therefore, impacted labour ability negatively. Alcoholics were seen as both victims and criminals, frequently robbed by men and women, while cravings made them break into pharmacies to steal spirits, money, or other valuables to buy alcohol (Nissen, 1933). Moreover, they were victims of the drinking custom tyranny. The sobriety movement was the resistance. According to an authority from the movement, Dr. Ragnar Vogt (1933), habitual drinking was a custom that produced alcoholics. The usual responses to custom transgressions were to break, destroy, and beat down. Only high-cultured people managed not to become offended. Therefore, since this drinking tyranny ruled the lower classes, it was necessary for the higher classes to suppress it (Stang, 1890). The problem of suppressing people’s free will was recognised, but the movement was inspired by the fact that the lower classes did not resist spirit brewing bans in the USA (Faye, 1890). It was deemed problematic that one had the right to enjoy alcohol since enjoyment should not harm the only value that had value in itself, the free personality (Landsrådet for edruelighetsundervisning, 1948). Since alcohol dulled the part of the brain that governed judgement and self-control, the personality organ, drinking violated the noblest result of human evolution. Consequently, abstaining from alcohol was not a sacrifice, but a logical consequence of the demand for total personal truth. The abstinence principle was a simple design of the idea of eternal truth. Total sobriety was the personality’s being in truth, or being in itself (Landsrådet for edruelighetsundervisning, 1948). Humanity would only lose lies and self-deception by suppressing its drinking custom. It would gain freedom, prosperity, and energy surplus deemed important for happiness. Courage and a desire to work would ensue (Landsrådet for edruelighetsundervisning, 1948; Torup, 1933). From the perspective of the individual, it was unreasonable, and therefore unworthy, to weaken the inhibitions that made one’s actions goal-oriented and responsible with alcohol. The starting point for personal abstinence was that one wants to be, under all circumstances and in all one’s actions, in full self-control. Only then, one was truly free and responsible (Mohr, 1938).
Emancipation by force: Sobriety boards
Scharffenberg became a member The Sobriety Committee of 1926 which laid the groundwork for the Sobriety Act of 1932. There, he suggested legislating sobriety policies so that they became municipal and state policy, with special boards to ensure public control with the alcohol question (Nissen, 1933). Ideally, he claimed, people should choose sobriety, but acknowledged that immature people needed external guidance (Landsrådet for edruelighetsundervisning, 1948) in order to attain the freedom to choose sobriety (Landsrådet for edruelighetsundervisning, 1948; Mohr, 1938). Thus, the committee suggested establishing sobriety boards (Skålevåg, 2008). Their mandate became a central feature of the law of 26 February 1932 on sobriety boards and treatment of drinkers (hereafter: The Sobriety Act). The law was inspired by the Swedish Alcohol Act of 1913 and, as did the Vagrancy Act, mainly concerned itself with poor alcoholics (Johansen et al., 2018; Skålevåg, 2008; Stenius & Edman, 2007).
The boards would improve conditions for sobriety, take care of alcoholics, and provide help to their families (The Sobriety Act, 1932 §3). They would be established in municipalities that were licenced to distribute alcohol. The poor relief was responsible for this task in municipalities that lacked the capacity to establish boards (The Sobriety Act, 1932 §1). With regards to institutionalisation, the boards communicated with the ministry. Otherwise, the boards were advised by The State Sobriety Council. Correspondence about other activities was with the council (Mohr, 1939). Only certain people could report an alcoholic to the boards and ask for intervention: the person themselves, their husband or wife, parents, children, siblings, relatives near or distant, guardian, a public trustee, the guardian council, poor relief provider, relief and assistance organisations, and the police. Finally, a priest or doctor could make a request on behalf of the person themselves for the reasons mentioned above. Then, when the board proceeded to investigate the home of the person, it would make sure to receive a written statement from the person themselves, their family, and other people who were aware of the situation. The board could demand a statement from whatever public authority was understood to possess information. The police had to notify the board if a person had been punished three times in the last 12 months for drunkenness. When summoned, the person in question had to appear before the board, and if they failed to do so, the police could transport them. If more information to decide on what kind of injunction to make was needed, the board could demand assistance from the police or receive proof from the district or city court (The Sobriety Act §4). The board should first try to persuade the person to lead a better life voluntarily. It should try to influence them to keep away from alcohol, help them obtain work, and move them into environments where alcohol was less tempting and where they could lead a better life – preferably as members of a sobriety lodge or association (The Sobriety Act, 1932 §5). If not, the boards would have them promise to be sober for three months, and then another three months, and so on. This agreement had to make the person feel that keeping their promise was an honorary debt. If the promise was broken, the boards would enforce coercive measures (Mohr, 1939). The board could make an alcoholic agree to give their spouse or someone else control over their finances, see a doctor and follow their prescriptions, or they would risk being institutionalised. The board would then see that the decided arrangement was followed and could place the person under special supervision for up to one year by one or more of its members, or by specially appointed persons or institutions (The Sobriety Act §5). If the person in question (a) did not follow the board’s demands; (b) abused their spouse or children or exposed them to neglect or moral depravity; (c) neglected their duty of care; (d) proved a danger to themselves or others; (e) repeatedly annoyed those surrounding them; (f) was a burden to poor relief or to their family; or (g) forfeited their estate so that they placed need upon themselves or their family, the board could place them in a place of cure, a nursing home, a labour camp, or other institution against their will (The Sobriety Act §§6,7, 1932).
From 1932, internments were decided by the Court on Guardianship that could incapacitate people above the age of 18 years if they lacked the ability to care for themselves or their estate due to insanity or addiction to intoxicating substances (Lov av 28. november 1898 om umyndiggjørelse, 1993). Before the board made such a decision, a doctor had to issue a declaration (The Sobriety Act §7, 1932). It had to contain precise information about the person in question, the investigations that had been undertaken, and the arrangements that had been made. Moreover, internment had to be supported by evidence. The doctor’s declaration (§6) was attached and if the judge at this point did not dismiss the case, the person would be summoned to a court hearing (§1). If the person did not appear without good reason, the police could transport them there (The Sobriety Act §§8, 9, 1932).
If the accused person could give written consent to living abstinently, and there was reason for the court to believe the promise to be truthful, and that the person had the faculties to maintain it, the case could be postponed. The board would then supervise that the person upheld their promise, and if they did so for one year, the case could be dismissed (The Sobriety Act §11, 1932). The court would announce the verdict regarding internment and the court or the social ministry would decide where the person would be interned for up to two years. The board would make sure the verdict was consummated and, if needed, could request assistance from the police (The Sobriety Act §12, 1932). When interned, the person could be discharged on parole if the institutional board decided that there was reason to think that they could live a sober and decent life. The board could set terms to which the person had to submit in a time-period that corresponded to the rest of the treatment. It had to be informed about the discharge, so that it could see that the terms were respected. When they were not, the board would address the board of the cure home, so that the person could be interned again and for the rest of the time-period (The Sobriety Act §17, 1932). The sobriety board could appeal to the Supreme Court if it disagreed with the Court of Guardianship’s verdict. The person in question could also appeal to the Supreme Court, but in such a case, the court’s appeal committee had to agree that internment would not be necessary. Furthermore, if the person’s appeal was dismissed, they had to face legal costs according to their ability (The Sobriety Act §§14, 16, 1932). After a revision in 1939, the board had the power to start an investigation on the basis of its own decision, without notification, to intervene at an early stage to save the alcoholic and to care for the family (Mohr, 1939). This was the result of a 1935 electoral victory by the Labour Party, which, in contrast to the Conservative Party, saw alcoholism as a disease, not a personal choice (Skålevåg, 2008).
The Portuguese model
Portuguese authorities perceived the country to be facing severe social misery during the 1980s and 1990s coinciding with a more prevalent heroin use in Portugal than in any other European country (Felix & Portugal, 2017; Sapp, 2014). In 1993, Portugal had adopted Decree Law 15/93, which focused on drug-money laundering and drug precursors. While drug use was criminalised, drug users were punished in a quasi-symbolic way by undergoing treatment in order to separate users from sellers (Sapp, 2014). However, HIV, Hepatitis B and C, tuberculosis, and overdose mortality rates remained high comparatively to other countries, and were perceived as a public health crisis (Felix & Portugal, 2017; Hughes, 2006; Hughes & Stevens, 2010; Laqueur, 2015). Moreover, Portugal was home to Casal Ventoso, the largest open drug scene, a public space where drug users gather to sell and use drugs (Waal et al., 2014), in Europe. It was located on the outskirts of Lisbon and was characterised by extreme poverty. Up to 5000 people visited it daily to obtain drugs and as many as 800 drug-dependent homeless people and socially excluded migrants resided there (Hughes, 2006). Even though statistics on drug use prevalence were insufficient (Loo et al., 2002), there was a general consensus of drug consumption as a pressing social problem (Felix & Portugal, 2017; Laqueur, 2015; Sapp, 2014). Portuguese policymakers determined that criminalisation was not enough (Sapp, 2014) and even regarded it as an obstacle to solving the problem (Hughes, 2006). The social exclusion of drug users (Hughes & Stevens, 2010; Whitelaw, 2017) led to a will to reduce the stigma of criminalisation (Loo et al., 2002). In 1998, the government appointed the Comissão para a Estratégia Nacional de Combate à Droga (Commission for the National Strategy to Combat Drugs) to suggest a revised and knowledge-based drug policy to tackle the country’s drug problems (Loo et al., 2002; Sapp, 2014). Three issues were addressed: prevention through information and awareness, treatment and social integration of drug users, and control with supply and demand (Sapp, 2014). The commission published 13 recommendations addressing these issues. Decriminalisation was one of them (Loo et al., 2002). The recommendations were adopted and became the Estratégia Nacional de Luta Contra a Droga (National Strategy for the Fight Against Drugs) which was built on eight principles, including pragmatism and humanism. For policymakers, the main objective was to make Portuguese drug policy science and evidence based rather than reactive (Hughes, 2006). The National Strategy for the Fight Against Drugs steered the drug policy towards preventive measures, low-threshold and harm-reduction approaches, increased treatment capacity and decriminalisation, with a primary focus on preventing drug consumption through the Comissões para a Dissuasão da Toxicodependência (CDTs) (Commissions for the Dissuasion of Drug Addiction) that were tasked with issuing civil sanctions (Hughes, 2006; Hughes & Stevens, 2012; Laqueur, 2015). The aim of the model was to move people with drug problems out of the courts and into treatment (Hughes, 2006; Sapp, 2014; Smiley, 2016).
Right-wing parties and conservatives lobbied against the policy reform that passed in parliament with the support of the Socialist Party, the Communist Party, the Green Party, and the Left Block. The social democratic Cabinet Minister of the Autonomic Region of Madeira threatened not to regulate the law, unveiling the possibility of a government crisis (Casao, 2001). The INCB regretted Portugal’s approved draft law that stipulated drug users to face fines rather than jail sentences for drug use. Drug abuse and possession of drugs for personal use would be an administrative rather than a criminal offence, and this was not in line with international drug control treaties (INCB, 1999). Most policymakers saw the CDT system as a political marketing strategy to prevent criticism for allowing drug use (Hughes, 2006). In the academic literature, the reform has been seen as harm-reduction oriented, and as an equilibrium between legalisation and prohibition (Bagaric et al., 2014; Loo et al., 2002), while maintaining abstinence as the aim for drug users (Hughes, 2006). It is seen as more humane than criminalisation, and sober in that it frees resources to target drug traffickers. One result has been a greater number of drug seizures compared with Italy and Spain (Smiley, 2016). The introduction to the National Strategy for the Fight Against Drugs document declared the aim of the reform to be a continued fight against drugs: With the strategy now defined, it is time for action. And on this point, it is best to have no illusions: drugs are not a problem for other people, for other families, for other people’s children. Nor can the fight against drugs be exclusive to others, to specialists, to technicians, to the authorities or to politicians. Together we have created a strategy and together we shall fight. (Sócrates, 1999)
The CDTs as taxonomy instruments of the state
The Portuguese Decriminalisation Act (Law n.o30/2000, of 29 November, 2000) targets consumption of illicit substances and the medical and social welfare of people who use these substances without medical prescription. The law becomes applicable when a person is caught by the police in possession of drugs for up to 10 days’ use (Law n.o30/2000, of 29 November, 2000 art. 2; Decree-law No. 15/93 of 22 January, Table I-IV). If the person spontaneously requests health service assistance, provisions of the law are not applied (Law n.o30/2000, of 29 November, 2000 art. 3 -1). The commissions for the dissuasion of drug addiction (CDTs) are provided with administrative and technical support as well as expenses for their members, by the Instituto Português da Droga e da Toxicodependência (Institute of Drugs and Drug Addiction) (Law n.o30/2000, of 29 November, 2000 art. 5-4, 5), which also keeps a register of proceedings with regard to offences (Law n.o30/2000, of 29 November, 2000 art. 6). The CDTs consist of three people, one of whom acts as chair, appointed by a government member responsible for the coordination of drug policies (Law n.o30/2000, of 29 November, 2000 art. 7 -1). One member is a legal expert and appointed by the Ministry of Justice, while the Health Minister and the government member appoint the other two. They can be doctors, psychologists, sociologists, social service workers, or have other relevant expertise in the field of drug addiction (Law n.o30/2000, of 29 November, 2000 art 7 -1, 2). These members shall prevent ethical conflicts (Law n.o30/2000, of 29 November, 2000 art. 7-2).
The CDTs are located in the “Governo Civil” and are responsible for the enforcement of fines and penalties (Law n.o30/2000, 5 -1, 2). When a person is caught using illicit substances (listed in Decree-law n.o15/93 of 22 January, Table I-IV) below the quanta for 10 days (Law n.o30/2000, Article 2-2), the police shall identify, and they may search them. Then, they shall confiscate the substances and produce a report that shall be forwarded to the relevant territorial CDT (Law n.o30/2000, Article 4 -1). If identification is impossible, they may detain the person to make sure that they appear before the CDT (Law n.o30/2000, Article 4-2). Upon appearance, the commission shall hear the person, and gather information needed to reach a judgement as to whether they are an addict or not, what substances have been consumed, the circumstances surrounding their consumption, and the person’s economic situation (Law n.o30/2000, 10 -1). For the CDT to be sure of the basis of the situation, if there is disagreement, the CDT or the person can request a medical examination, including a blood or urine sample (Law n.o30/2000, 10-3, 4). Then, after the person has been placed in one of two categories, addicted or non-addicted drug user, taking circumstantial specificities into account, measures are applied. If the person is a non-addict with no prior record of offences under the law, the commission shall provisionally suspend proceedings (Law n.o30/2000, 11 -1). However, if the person is an addict, proceedings may only be suspended if they consent to undergo treatment and if they have no prior record of transgressions (Law n.o30/2000, 11-2, 3). If the person is not addicted to drugs and does not repeat the transgression, the suspension may last for up to two years before the records are archived and sealed. The same goes for the addicted person who undergoes treatment without dropping out (Law n.o30/2000, 13 -1, 2). Suspensions are revoked if one fails to abide by requirements issued by the CDT. Then, penalties shall be enforced (Law n.o30/2000, 23-2, 3). The CDT must notify the health service that the person in question chooses when they agree to undergo treatment. The treatment service becomes obliged to notify the commission quarterly about the continuation of treatment (Law n.o30/2000, 12 -1, 3). Only non-pecuniary penalties can be applied to people addicted to drugs, while fines and non-pecuniary penalties might be applied to the non-addict (Law n.o30/2000, 15 -1, 2, 3). To decide upon these penalties, the CDT must consider the seriousness of the drug use, the degree of fault, the type of drugs, and the public or private nature of the use, and the economic situation of the perpetrator. In the case of public use, the CDT must consider the specific place (Law n.o30/2000, 15-4). Then, if defined as addicted, the CDT can apply penalties with the aim of changing the person’s behaviour, either as an alternative to a fine or as the main penalty. The CDT may prohibit the person from working in a profession or a job that requires a licence, it may ban them from certain places and from being in the company of certain persons, as well as travelling abroad without permission. Furthermore, the CDT may demand that the person presents themself periodically at an appointed place. The CDT may also remove the right of the person to own a licence for a firearm and may confiscate objects considered to be a risk to themself or the community, as well as take control over public benefits. Such subsidies shall then be managed by the organisation managing proceedings or monitoring the treatment process – when agreed to by the person. Alternatively, if the CDT and the person agree, the person can choose to donate to a charitable organisation or carry out community service to avoid the penalties (Law n.o30/2000, 17-2,3). If the person cannot or will not undergo treatment, the CDT may suspend enforcement of penalties if the person periodically attends a designated health service (Law n.o30/2000, 21 -1). Furthermore, if the CDT considers it to be effective in dissuading the person, it can deliver a warning, a verbal reprimand that warns the person about the consequences of drug use and urges them to abstain from drugs (Law n.o30/2000, 18-2). If they waive the right to appeal, the warning shall be given immediately (Law No. 30/2000, 18-3).
The governed subject: Sobriety boards and commissions for drug addiction
According to a Christian morality underpinning the Norwegian sobriety movement, sobriety was associated with God and peace on earth. Alcohol, on the other hand was ruining the core of society. Following this, a biopower strategy was deployed that instrumentalised the use of knowledge, reason and morals, to make people understand and want an alcohol-free society. First, it was attempted to gather support for a prohibitionist policy and when that failed, for people of a high social standing to suppress the drinking custom in order to emancipate people from the lower classes from imminent ruin and make them into functional worker subjects. These people would attain the ideal position of the human subject as free and responsible citizens. The sobriety boards, being the machinery of this strategy, forced drinkers to abstain from alcohol and to become morally and economically responsible citizens who cared for their families and, preferably, joined a lodge or abstinence association. At a certain point, alcoholism became a disease, not necessarily as a scientific discovery, but as a political decision, ensuring executive powers to become vested in the sobriety boards (Skålevåg, 2008). This biopower technology functioned as a negotiation of normality with its own system. First, the boards were asked to investigate a person from designated people (the family, guardians, police, priest, or other people who were considered to play a significant role in the person’s life, or who had special status with regard to the drinking question). Then, the boards investigated and monitored the person and acquired intimate knowledge about them in order to tailor sanctions to make them abstain from alcohol. The board could also intern them for up to two years in an institution for alcoholics. Since the alcoholics were conscious of this possibility, they would choose to admit themselves to treatment to avoid internment. From this, it can be observed that power was dispersed, and that when various people in connection to the alcoholics suggested they be investigated, that power became vested with the boards, and, by extension, the ministry and the council that accumulated, organised, and archived the acquired knowledge. As such, these boards became the centre-point of a power that placed individuals under surveillance, relieved them of ownership of their money and placed them in designated institutions to labour physically, but also religiously and psychologically upon themselves, to become improved citizens – the normal and ideal subject that contributes to society by being employed and taking care of their family.
In the case of the Portuguese CDTs, the aim of making drug users stop using drugs was never changed. The science-based strategy suggested various measures to prevent drug use, treat drug users and curb the supply of and demand for drugs. The background was that the country had found itself in a public health crisis with visible poverty and problems relating to immigration, and high prevalence of heroin use. It was clear that the existing health-oriented and penal policy where convicted drug users were coerced into treatment instead of imprisonment was insufficient. Following this, the CDTs were established to dissuade drug users from using drugs and make them go into treatment by effectuating civil sanctions if they did not abide by health advice. As such, the CDTs would integrate drug users into society, while the police reallocated their resources to investigate and arrest drug traffickers. Administrative and technical support for the CDTs were provided by the Institute of Drugs and Drug Addiction, and appointed members of the CDTs would have experience from the field of drug addiction treatment and law, seating the model within an epistemological context where drug use is understood in terms of addiction and crime. The person who is caught by the police is ordered to present themselves for the CDT. Violation of this might result in criminal sanctions, thus, bridging the justice and health sectors. Then, the CDTs acquire detailed knowledge about the person, such as their economic status and their psychological, social, and physiological wellbeing and degree of addiction, making a subject in need of and open for examination and regulation. Following this, risk associated with drug consumption is measured, and motivational interviewing (MI) is used to make the person choose to change, admit to treatment, and stop using drugs. This disciplinary power is thus localised with public authorities placed in the CDTs by different branches of government and posited on the intersection of the justice and health sectors. Acquired knowledge about the person is used to investigate and regulate their social relations, psychological motivation, geographical movements, and choosing treatment and abstinence, conscious of possible sanctions if they do not make the right choice or agree to what the CDT suggest.
The joint analysis of the models in reflection with Foucault
For biopower to work, institutions are established to separate functioning from non-functioning people to construct normality. The functional average, the norm, is made possible precisely by addressing deviants who are intervened against in order to change them (Eliassen, 2016). Early sobriety truth discourse in 1800s Norway took upon itself the task of instrumentalising reason, supported by religious views, to shape public consciousness to integrate and channel the immorality of drinking alcohol and to save society from ruin by alcohol. The Portuguese strategy to combat drugs based itself on a similar formula – science would be used to prevent drug use, treat drug users, and curb the supply and demand for drugs in order to tackle the public health crisis posed by drug addiction. In these truth discourses and within the institutional apparatuses, subjects were positioned as deviants to ideals of the alcohol or drug-free individual, family and population. In the case of 1930s Norway, the person’s normality was to be a responsible and free person who provided economically for their family as father and husband. In Portugal, they had to choose living a life without the use of drugs and take care of their own health, not with the same emphasis on the family or civil society/local community (by joining associations or lodges) as in the Norwegian case (see Table 1).
The sobriety boards and the CDTs both addressed the lower classes but with different terminologies. In Norwegian, the term “lower classes” was used, while in Portugal, “extreme poverty” and “migrant population” were used to characterise the subjects (see Table 1). The constraints on issuing economic sanctions against an individual who had been “diagnosed” with addiction indicates an implication that the main target group for the commissions were believed to be poor. Central to the sobriety boards, was the exercise of defining the person’s functionality in terms of whether he could function as a breadwinner. The CDTs would investigate if the person was an addict or not in order to tailor the right sanctions and/or health responses. The governed subject in Portugal was perhaps more elaborately biomedicalised, with references to the professions involved in deciding on sanctions and treatments, and suggested approaches such as enforced medical check-ups with the aim of reducing overdose deaths and infectious diseases. In the case of Portugal, the members of the commissions were experts, while sobriety board members were elected representatives of the municipal or city council, but preferably chaired by a medical doctor.
These ruptures, where transgressors would be taken out of the courts, were results of conscious shifts. According to a former drug strategy coordinator in Portugal, the country faced increasing drug use even though it had been criminalised since the 1970s. Many people were caught using drugs and sent to jail, without the problem being solved. It even seemed to increase their drug use. Moreover, courts were spending too much of their resources without results, and police and judges believed that it was of no use to arrest these people who were sick, not criminal (Hughes, 2006). In the Norwegian case, the Justice Committee chair in The Norwegian Parliament, in 1936, stated that the intention with getting the sobriety boards out of the court system, was to get people away from the perception that the boards were judicial courts and that the approach was punishment, rather than medical treatment of people. According to the sobriety committee, the deepest reason for establishing the boards, however, was an intent to deal with individuals who posed a risk to society (Christie, 1963).
Comparison of the different apparatuses.
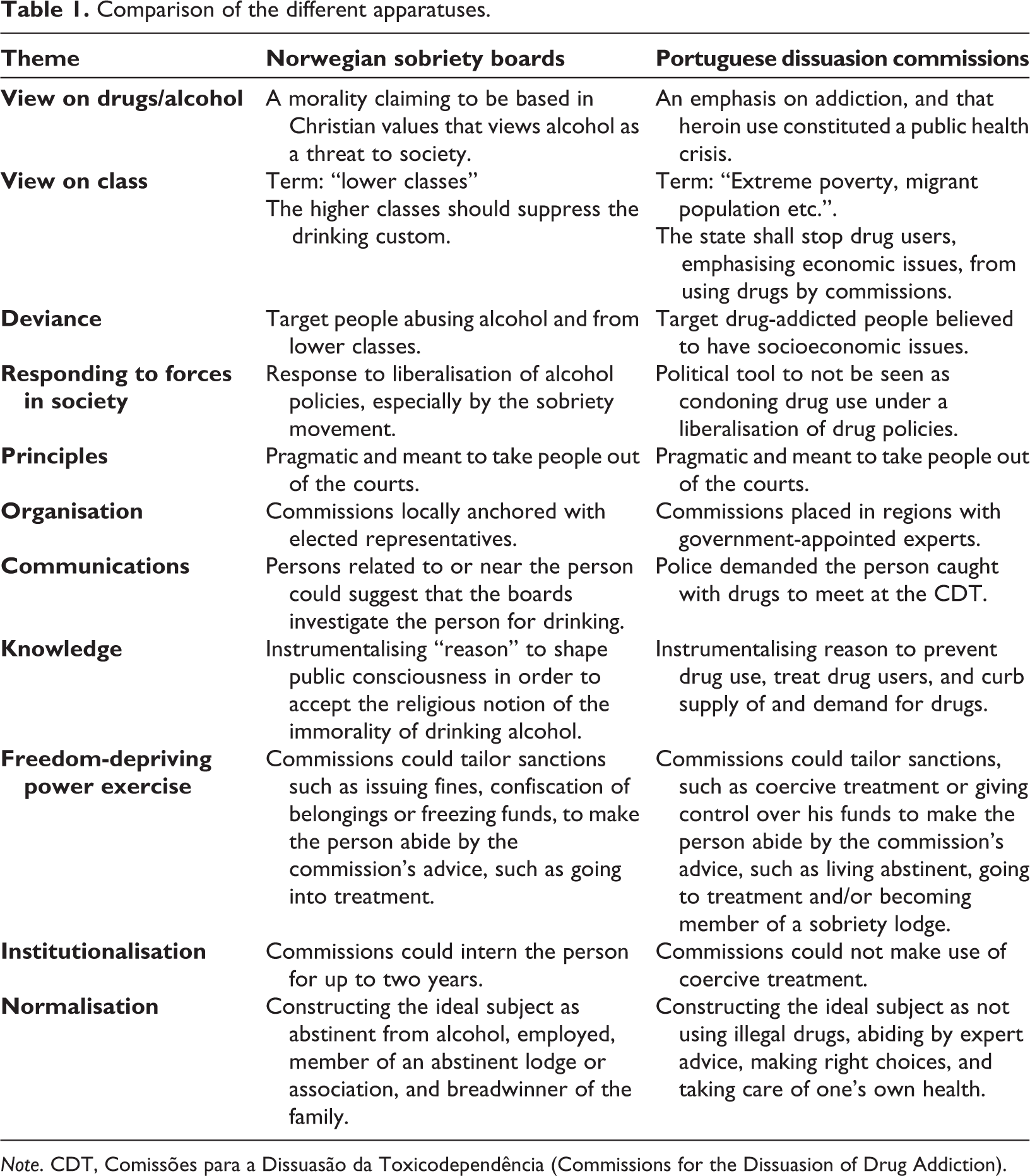
Note. CDT, Comissões para a Dissuasão da Toxicodependência (Commissions for the Dissuasion of Drug Addiction).
Discussion and conclusions
This study made use of an analytic strategy drawing on archaeology and genealogy approaches in order to study truth discourses, power relations, and problematise drug policy reform discussions that are pointing to the “Portuguese model”. This article attempts to contribute to post-structural literature that might help uncover the cementing of biopower strategies that are portrayed as neutral, and evidence-based, but which serve to make up and control marginalised groups. The opposition between punishment and treatment that drug policy reform discussions rest upon, is problematised by comparing and looking at the “Portuguese model” and comparing it with the 1930s Norwegian sobriety board in order to make clear the governance logics of the different systems. The sobriety boards have previously been defined as a biopower technology (Skålevåg, 2008), and this article shows that they have similarities with the Portuguese CDTs in that they construe and address drug-using subjects with the intent to exercise power over them and make them choose to work on themselves in order to adapt to a predefined normative framework as integrated citizens. The different systems separate these persons out from society and designate their deviant labels in order to help them back into society.
The significance of the phenomenon of addiction in culture and language has increased in recent history, with the concept representing an emergence and diffusion of individualisation (Hellman, 2010; Room et al., 2015). This is supported by this analysis of the Portuguese case vis-à-vis the Norwegian case, where the individual and their health is emphasised rather than the person in relation to their family. Coercion of free will was considered problematic in early 20th-century Norway, and in Portugal, the law emphasised the choice of the person who had been caught in possession of drugs. The person’s choosing, however, had to be in accordance with the CDT’s advice if they were to avoid sanctions.
With regard to modern forms of political power, the state has no essential necessity or functionality, and the problem of government is codified in discourses prompting the analysis to be about how the state is articulated into the activity of government. Government, therefore, becomes an activity that posits the obligations of its rulers with regard to the problems they address. Governing ideals, then are connected to the problems they revolve around (Rose & Miller, 1992). When it comes to regimes that aspire to liberalism, apparatuses based on knowledge connection and problematisation exercise their demands to and constraints on central powers (Rabinow & Rose, 2006). Moreover, power is not only seen as prohibiting and constraining on people but creates a people who are carriers of a regulated freedom. Personal autonomy, resting on the notion of free will, should therefore be central to the exercise of political power since individuals actively take part in it. Further, political rationalities are articulated in relation to the governed objects, such as people over whom government is to be exercised, in this study, drug-using people or alcoholics. Said rationalities are morally coloured, grounded upon knowledge and made thinkable through language. And those who cannot keep their contractual obligations appear as anti-social or as bizarre and might be placed under medical treatment, or treated as criminals who violate norms need to be managed by law enforcement (Rose & Miller, 1992).
While the sobriety boards were promoted by sobriety movement authorities that had just lost their political cause for prohibition, the CDTs seemed to have protected Portugal from criticism from the INCB for violation of the international treaties conventions (Hughes, 2006). By seeing the establishment of CDTs and the sobriety boards through the lens of governmentality, one can see policies emerge from responding to contradictory forces, striving for meso-level (family/civil society) functioning subjects in Norway, morally justified, and a micro-level focus on whether the individual is addicted or not in Portugal alongside a public health macro perspective, supported by an emphasis on evidence, renewing the social contracts for the addressed populations that were expected to take care of their health and abstain from drugs and seek treatment for drug addiction and stop spreading infectious diseases. In the cases of both Portugal and Norway, there were general impressions of social crises that placed a demand for political action while at the same time constraining power and “making up” a people (dependent populations) with its regulated freedom. We can see, thus, contradicting forces of will: (a) police (in this case, state intervention to address the poor drug-using populations in Portugal and poor alcoholics in Norway), and (b) liberalism (constraints placed upon police power, and the importance of free will). The Sobriety Act of 1932 and the Decriminalisation Act of 2001 were concerned with resolving the problem of treating deviants via legal, social, and medical measures. In both cases, the populations addressed were categorised as sick, allowing a combination of paternal and pastoral power technologies to construct the subject who chose to be free from their slavery, either to alcohol in Norway or to drugs in Portugal. Whereas alcohol was seen as a threat to the core of Norwegian society (Brun, 1890), illicit drugs became a threat to public health in late-1990s Portugal (Hughes & Stevens, 2012). We have described how the Norwegian sobriety movement consisted of working-class groups, the bourgeoisie, and Christian communities. Working-class groups made efforts to prohibit alcohol because of its negative effects on their peers, while prominent and educated people advocated a class-transcending solidarity to eliminate drinking and ending social misery to increase productivity and construct the free human subject. In Portugal, consequences of drug addiction also transcended different strata of society and resulted in political consensus for reform, economic challenges being factored in, with the with extreme poverty and visible migrant population being central aspects in justifying the drug policy reform (Laqueur, 2015; Loo et al., 2002). One of the key aims of this reform was to re-allocate resources from addressing individual drug users to drug traffickers (Smiley, 2016) and, post-reform, the state continued to address individual drug users through sanctions and treatment instigated by special commissions. It was described how Norway after 1932 and Portugal since 2001, established special commissions to investigate, define, and govern drinking or drug-using populations to make them change their ways of life.
This study has shown that decriminalisation reforms can unleash effective means of control where compromises that serve to stitch up contradicting forces might in turn produce biopower effects and coerce deviants to choose a predefined “freedom”. This seeming paradox of forced freedom has been suggested as an immanent problem of liberalism, where people are born free, but also made free through autonomy training − often by despotic means (Valverde, 1997) and where the sobriety boards and the dissuasion commissions serve as organisational examples that bridge what politically might be defined as opposites between justice and health. This study contributes to the questioning of this portrayed dichotomy between punishment and treatment, between penal and assistential approaches, where medicalisation of the individual’s condition becomes necessary to justify said reforms. The outcome of the reforms was a social contract that situated the police, the accused person’s relatives, and the church as contact points for public bodies responsible for the taxonomy of the addicted subject with regard to the degree of their rationality (freedom in making choices), individual problems, and risk. The CDTs and the boards were equipped with tools for coercion, deterrence, and social integration, that placed the individual in the centre with the aim to stop them from drinking alcohol or using drugs.
Further studies on how local power relations create conditions for such biopower effects is advised and could give insight into how policy reforms that claim to be neutral (evidence based) and emancipatory, provide new frameworks for governing deviant subjects. The abovementioned processes might make social work and healthcare professionals in the field of addiction become mere functionaries in a fight against drug use, masked by discussions on policy reforms that promise emancipation for marginalised drug-addicted people. Foucault has been criticised for prophesising that normalising devices anchored in the carceral institutions would spread through all of the social body, while what has actually happened is that a penal dragnet under neoliberalism has essentially addressed the lower social classes and continued to divide populations according to ethnicity, class and moral worth (Wacquant, 2016). The sobriety movement emerged from the higher social classes (Göransson, 1938) and tried to suppress the drinking custom that tyrannised especially the lower classes, and the Portuguese reform tried to remove the public misery of Casal Ventoso. Attention should therefore be given to the possibility of the coming drug policy reform in Norway cementing social divisions by framing its biopolitics in a medico-welfare policy terminology. Socioeconomically weak groups of people are targeted by the biopower technologies of a drug policy reform, and social workers and health personnel might therefore be the ones implementing these technologies and merging them with the general health and welfare system neutralised by a terminology emphasising humanism and pragmatism.
Footnotes
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.