
Abstract
Aims:
Past research has linked substance use to individual differences in discounting of future rewards. Since behaviours such as smoking and excessive drinking appear to involve a devaluation of future negative consequences, discounting of costs may also be relevant in the understanding of such behaviour. The primary aims were to investigate the association between cost discounting and the behaviours smoking and hazardous drinking.
Methods:
In four studies, individuals recruited from the crowdsourcing marketplace Amazon Mechanical Turk responded to measures of discounting. Results were combined by meta-analysis of the standardised mean differences (d) between self-reported smokers and non-smokers, and between participants with AUDIT scores of 10+ (hazardous drinking) and those with scores below 10.
Results:
In comparison with non-smokers, smokers’ relative valuations of future gains were lower, d = –0.32, 95% CI [–0.47, –0.18]. There was no association between smoking and cost discounting, d = –0.02, 95% CI [–0.17, 0.13]. Participants with AUDIT scores of 10+ valued future gains somewhat lower than participants with scores below 10, d = –0.17, 95% CI [–0.35, 0.01]. There was no association between hazardous drinking and cost discounting, d = –0.02, 95% CI [–0.21, 0.16]. According to Bayes Factors (BF), the data supported an association between gain discounting and smoking (BF > 100). It was insensitive in the analysis of gain discounting and hazardous drinking (BF = 0.6), but it strongly supported null-effects in both analyses of cost discounting (BFs = 0.1).
Conclusion:
The results suggest that the robust link between gain discounting and smoking status does not reflect a general devaluation of future outcomes among smokers.
Money received today is considered of more value than money to be received in the future. The process wherein subjective value diminishes as a function of delay is referred to as temporal discounting, and is a process reflected in the choices of humans and a range of other species (Vanderveldt et al., 2016). A preference for immediate over equal delayed rewards is in principle reasonable due to the uncertainty of the future, but in excess, discounting can result in the impulsive choice of a small immediate reward over a substantially better delayed outcome. Accordingly, temporal discounting has been used as a model to understand people’s suboptimal choices in domains such as economy and health, and it has been particularly important in research on addictive behaviour (see Bickel et al., 2019, for a recent overview).
In a temporal discounting task, participants are faced with choices such as receiving $10 today vs. $11 in one week. If people choose $10 today over $11 in a week, one may describe this preference as devaluation or discounting of future consequences, and if people still choose $10 today when the delayed reward is increased to $100, they severely discount future value. The idea behind research employing these tasks is that people’s performance to some extent should reflect their real-world preferences in conflicts between immediate versus delayed rewards, such as the immediate reward of a drug versus its long-term consequences. Indeed, past research has found little difference between preferences concerning hypothetical choices and preferences concerning actual monetary choices (Matusiewicz et al., 2013), and the link between tasks like the above and various types of substance use and substance use problems is well documented (MacKillop et al., 2011).
The typical discounting task is framed as a choice between a present positive monetary gain and a future one. As an analogy for substance use, one could picture this as a choice between the immediate positive experience of a drug and the long-term positive effects of not using the drug. However, a different analogy would be that of a choice between costs. The use of addictive substances such as tobacco predisposes a person to further consumption and the cumulative exposure over several years can produce negative social and health-related consequences. In many cases, the choice of not using a substance would involve withdrawal symptoms such as restlessness. It is therefore not unreasonable to consider choices between costs as relevant to the understanding of decision-making involving addictive substances.
The association between gain discounting and substance use is well established (MacKillop et al., 2011), but gain discounting and cost discounting may reflect fundamentally different processes (Myerson et al., 2017). When framing choices as losses instead of gains, there is typically far less discounting and it is not uncommon to find instances of negative discounting (e.g., Thaler, 1981), which is the tendency to prefer an immediate cost over an equal or even smaller delayed cost. The reason for this behaviour is likely that people want to “get it over with” (Thaler, 1981). In regard to smoking and alcohol use, one could expect that smokers and hazardous drinkers are more interested in avoiding an immediate cost (i.e., from not using the substance) than being concerned about the delayed cost (i.e., harm from long-term use of the substance). In discounting of gains, the immediate option (smaller/shorter) reflects impulsive choices, whereas in discounting of costs and losses, the option that gives larger overall costs (i.e., the choice of the larger/longer costs) can be considered as representing the most impulsive choice.
A potential connection between cost discounting and addictive behaviours is both of theoretical and practical relevance. Manipulating present and future costs or the way people perceive these could be elements in interventions, and measures of cost discounting may have predictive value as one of many factors that can identify vulnerable individuals. The type of impulsiveness observed in people with substance use problems is sometimes described as an insensitivity to delayed consequences (Petry et al., 1998). If gain discounting, but not cost discounting, is associated with addictive behaviours, it suggests that the devaluation of delayed outcomes in substance use problems is specific to rewards, or that impatience is more important than the devaluation (see Hardisty, Appelt, & Weber, 2013).
The current study is not the first attempt to connect measures of cost discounting with substance use. Heroin-dependent persons have been found to have higher discount rates for both gains and losses (Cheng et al., 2012), and in analyses across gains and costs, a main effect of smoking status has been reported (Johnson et al., 2007). In a study by Hardisty, Thompson, Krantz, and Weber (2013), smoking status was associated with cost discounting for one of three different measures of discounting, but this association was not found in a replication study reported in the same article. Whereas Li, Hardisty, and Wade (2019) found low predictive value of cost discounting on measures of tobacco and alcohol use, Takahashi, Ohmura, Oono, and Radford (2009) reported a correlation between cost discounting and the frequency of drinking.
Except for the study by Li et al. (2019), the sample sizes of the studies above were small (less than 30 participants in each cell for group comparisons, and correlational analyses with 50 participants or less), and none of the studies specifically and systematically investigated cost discounting and substance use. In the present research, cost and gain discounting were investigated using four different assessment methods, and with relatively large samples.
The main research questions were: (a) To what extent are gain and cost discounting associated with smoking status? (b) To what extent are gain and cost discounting associated with hazardous drinking?
Method
Participants and sample size
Participants were US residents recruited through Amazon Mechanical Turk (MTurk). MTurk is a crowdsourcing marketplace where companies and institutions can outsource various tasks such as labelling, transcribing, translation, and participation in experiments and surveys. The total number of participants who smoked was 229 (vs. 738 non-smokers) for the analysis on cost discounting and 249 (vs. 790 non-smokers) for the analysis on gain discounting. The total number of participants with a hazardous drinking pattern was 129 (vs. 832 non-risk) for analyses of cost discounting and 142 (vs. 887 non-risk) for analyses of gain discounting. Demographic data for each of four different studies can be found in Table 1. The studies were conducted in 2014 and 2015.
Demographics of samples.
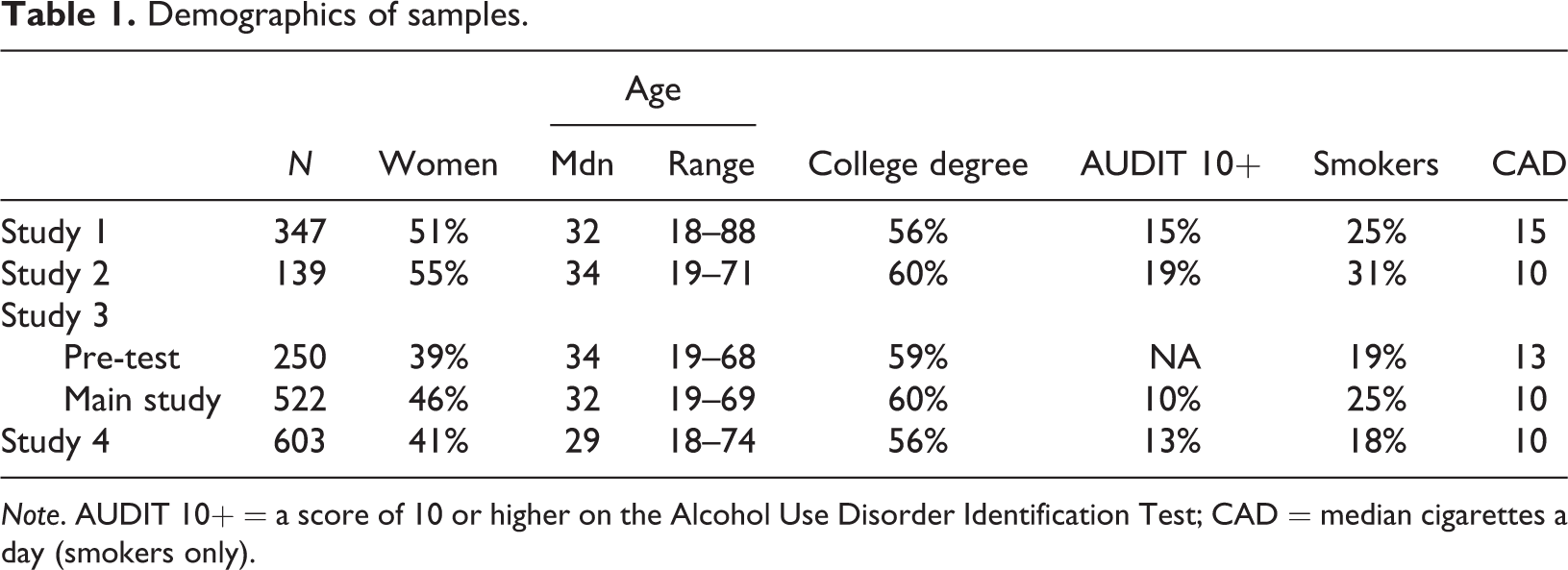
Note. AUDIT 10+ = a score of 10 or higher on the Alcohol Use Disorder Identification Test; CAD = median cigarettes a day (smokers only).
The sample sizes for each of the studies were determined based on the effect size found for non-clinical samples in the meta-analysis of gain discounting by MacKillop et al. (2011; d = 0.45). For a power of .80 and a p-value threshold of .05, the required sample size would be 246 for a group allocation ratio of 1:4 (smokers vs. non-smokers). The sample of Study 2 was smaller because the original reason for conducting that study was to see whether the pattern of cost discounting changed after adjusting the procedure (i.e., whether there would be more cost discounting in general).
Measures
Discounting
Study 1 employed a computerised adjustment procedure (Richards et al., 1999) where the immediate amounts corresponding to receiving/paying $10 were determined for three different delays. Specifically, participants repeatedly received the question: “Would you rather have (a) [amount] now or (b) $10 in [number] days?” For the costs condition, the question was: “Would you rather pay (a) [amount] now or (b) $10 in [number] days?” Cost and gain choices were intermixed. The delays were 0 days, 2 days, 30 days, and 365 days. The amounts varied from 0 to 10 for the gain items, and from 0 to 11 for the loss items. The data for “0 days” items were not used.
Judged from the responses and comments by participants, the task was difficult, and the procedure was therefore simplified in Study 2 by separating choices regarding costs from gains into two distinct counterbalanced blocks, and by omitting distractor trials that were part of the original procedure.
In Study 3, the 21-item Kirby Questionnaire (Kirby et al., 1999) was employed in its original form and in a version with choices framed as costs. The questionnaire gives 21 choices such as, “Would you prefer $54 today, or $55 in 117 days?”
In Study 4, participants chose between receiving/paying an immediate amount of $300 and future amounts from $150 to $900.
In addition to the above traditional measures, for which results are reported in Tables 2 and 3, Study 3 included a measure that specifically tapped individual differences in negative cost discounting. This measure consisted of five choices between an amount to be paid immediately and the very same amount to be paid after a given delay. For analyses on this measure, we also included data from a pilot study. Detailed descriptions of methods for each study can be found in online Supplementary Materials.
Demography and substance use
Education was coded into “college degree” and “no degree”. In Studies 3 and 4, current financial situation was indicated by two items about the ability to handle unexpected expenses (Cronbach’s alphas = .84 and .91).
Smoking status was assessed with the question: “Do you smoke (tobacco/nicotine)?” With the options: “Yes, daily”, “Yes, but not daily”, “On rare occasions”, “Former smoker. I have quit”, “No, but I have tried”, “No, and I have never tried” (two first options defined smokers).
The 10-item Alcohol Use Disorders Identification Test (AUDIT) was used as a measure of hazardous alcohol consumption. The cut-off for defining hazardous drinking is 8 or 10 (Saunders et al., 1993). The cut-off 10 was chosen because we were more interested in the potentially problematic sides of drinking.
Statistical analyses
Scores from the discounting measures were treated as indicators of individual differences without concern for the underlying discount functions (e.g., hyperbolic, exponential, quasi-hyperbolic; see Benhabib et al., 2010). In Studies 1, 2 and 4, the indifference points (i.e., the value at the switch point between choices of immediate amounts and delayed amounts) were converted to z-scores and averaged. For Study 3, the overall proportions of choices of the delayed amounts were used as the measure of discounting.
Data were excluded from analyses when participants failed criteria for attention (attention checks and patterns of responding) and when participants’ scores on the final measures of discounting were three standard deviations above or below the mean of the samples (see online Supplementary Materials for further details).
The standardised mean differences (d), weighted for unequal sample sizes, were computed for comparisons between smokers and non-smokers, and for participants with AUDIT 10+ scores vs. those with scores below 10. Confidence intervals were based on 1999 bootstrap samples (bias-corrected and accelerated) computed with the R package “bootES” (Gerlanc & Kirby, 2013). The results of the individual studies were subjected to an overall analysis (random effects meta-analyses with adjustments for sampling bias and adjustment for unequal sample size). Bayes Factors were computed with the “meta.ttestBF” function from the R package “BayesFactor” with default priors (Morey & Rouder, 2015).
Results
Cronbach’s alphas (measure of internal reliability) for the gain measure in Studies 1, 2, and 4 were .70, .65, and .77, respectively. For the cost measure the alphas were relatively low in Studies 1 and 2 (.59 and .48), but slightly better in Study 4 (.65). In Study 3, the split-half reliability was .88 for gain discounting and .93 for cost discounting.
Results for smoking status are presented in Table 2 and results for AUDIT status are presented in Table 3. Note that the signs of the effect sizes have been adjusted such that a negative effect size means that smokers and hazardous drinkers value future consequences relatively less than non-smokers and the alcohol low-risk group. That is, if lower discounting is a desired behaviour, negative effect sizes indicate that smokers or those with hazardous alcohol consumption perform worse.
Standardised mean differences (d) between smokers and non-smokers on measures of discounting.
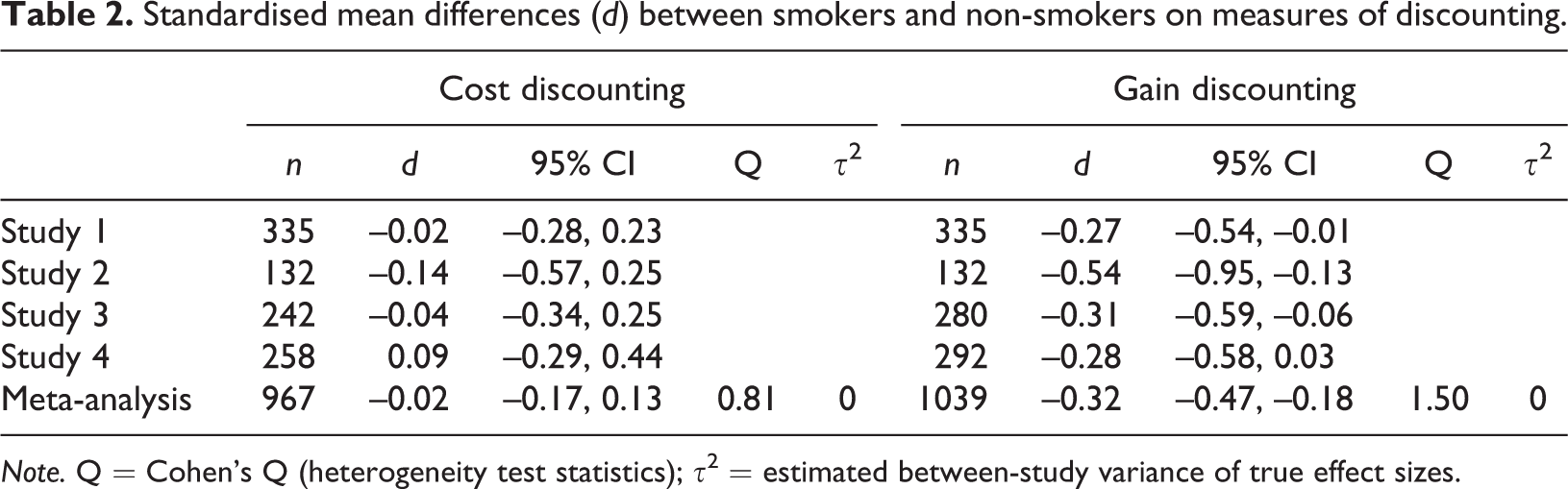
Note. Q = Cohen’s Q (heterogeneity test statistics); τ2 = estimated between-study variance of true effect sizes.
Standardised mean differences (d) between persons with AUDIT scores of 10 or more vs. AUDIT scores below 10 on measures of discounting.
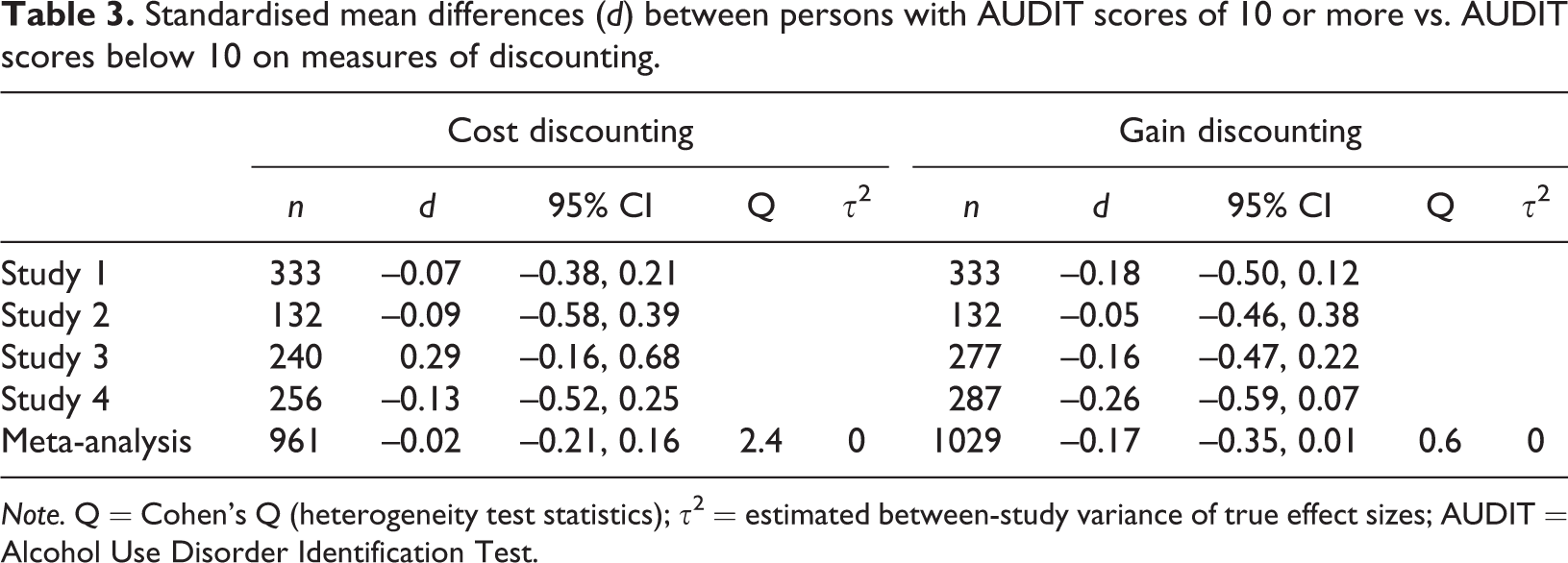
Note. Q = Cohen’s Q (heterogeneity test statistics); τ2 = estimated between-study variance of true effect sizes; AUDIT = Alcohol Use Disorder Identification Test.
For smoking, the results are relatively clear. The estimated differences in cost discounting were practically zero. The result on gain discounting shows a difference corresponding to about one third of a standard deviation. The Bayes Factor for cost discounting was 0.09, strongly favouring the assumption of null-effect, whereas the Bayes Factor for gain discounting was > 100, strongly supporting the assumption of differences between groups according to smoking status.
As presented in Table 3, the relation between cost discounting and AUDIT status was also practically zero, with a Bayes Factor of 0.11. There were tendencies of a small effect size for gain discounting and AUDIT status in the order of one sixth of a standard deviation, but the Bayes Factor of 0.59 suggested insensitive data.
Means and adjusted means (controlled for education, age, and gender) for all studies can be found in the online Supplemental Materials. Meta-analyses on adjusted means (with original SDs) produced effect sizes that were virtually identical (± .01) to the above analyses, except the comparison between smokers and non-smokers in the gain condition, where the effect size was reduced to d = –0.26, 95% CI [–0.41, –0.12].
To see whether the association between smoking status and gain discounting could be explained by differences in financial situation, marginal means from Studies 2 and 3 (the studies that included the measure of financial situation) were aggregated. When controlling only for gender, age and education, the effect size was d = –0.27, 95% CI [–0.47, –0.07], and with additional control for financial situation, the effect size was d = –0.23, 95% CI [–0.43, –0.04]. For alcohol, the effect size across these two studies when adjusting for age, gender and education was d = –0.21, 95% CI [–0.47, 0.05], and with adjustments for financial situation, d = –0.15 95% CI [–0.41, 0.11].
In addition to the traditional measures of discounting, a five-item negative discounting scale (measuring preference to pay an amount today instead of an equal amount in the future) was introduced in Study 3 and in a pre-test for Study 3. Cronbach’s alphas were .88 in both studies. Weighted across the two studies, the mean number of negative discounting choices out of five possible was 2.3 (SD = 2.0, n = 178) for smokers and 2.2 (SD = 1.9, n = 584) for non-smokers, d = 0.08, 95% CI [–0.08, 0.25]. For hazardous drinking (main study only) persons with AUDIT scores of 10 or above made negative discounting choices on average 2.1 times (SD = 1.96, n = 54), whereas the average for those with scores below the AUDIT cut-off was 1.9 (SD = 1.91, n = 468), d = 0.14, 95% CI [–0.14, 0.42]. If anything, smokers, and those with hazardous alcohol consumption, made slightly more negative discounting choices on this supplementary measure (contrary to the idea that they would choose delayed costs).
Analyses of the relation between discounting and indices of smoking severity are presented in Table 4. In contrast to the above results on smoking status, the direction of the effects indicated a potential association between cost discounting and smoking severity. That is, a higher number of cigarettes smoked, less time to first cigarette, and higher Fagerström score (Heatherton et al., 1991) could be associated with higher levels of discounting, but the statistical evidence was weak.
Meta-analyses of Spearman’s rank correlations (rho) between discounting and measures of smoking severity among smokers.
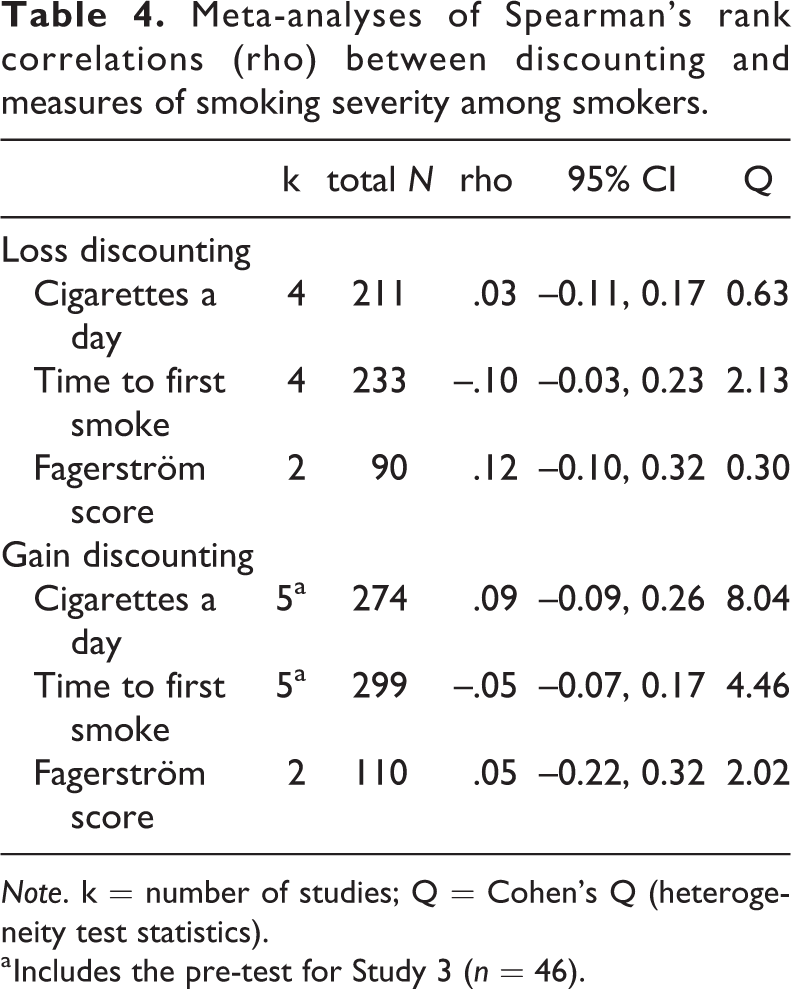
Note. k = number of studies; Q = Cohen’s Q (heterogeneity test statistics).
a Includes the pre-test for Study 3 (n = 46).
Discussion
On measures of gain discounting (e.g., the choice between receiving $100 now and $120 in one week) there were clear differences between smokers and non-smokers, but on measures of cost discounting (e.g., the choice to pay $100 now versus $120 in one week), there were no differences. Thus, the type of cost discounting tapped by the present operationalisations does not appear to be relevant for understanding why people smoke. However, the analysis on smoking severity leaves open the question of whether cost discounting is relevant for understanding the extent of smoking.
In terms of hazardous drinking, there was no effect of cost discounting. For gain discounting, there was a tendency towards more discounting in the alcohol risk group, but the data were insensitive (not able to confirm or disconfirm an effect).
In some of the past data on tobacco use and discounting, there were tendencies of more cost discounting among smokers (Bickel, Yi, Kowal, & Gatchalian, 2008; Hardisty, Thompson, et al., 2013), whereas other data did not suggest such an association (Hardisty, Thompson, et al., 2013; Ohmura, Takahashi, & Kitamura, 2005). These studies have in common their small sample sizes. The present research utilised relatively large samples and four different methods of assessing cost discounting. The estimated effect size of differences in cost discounting was practically zero for both hazardous drinking and smoking.
Some studies with smaller sample sizes have shown a link between gain discounting and the severity of smoking (Heyman & Gibb, 2006; Ohmura et al., 2005; Reynolds, 2004; Sweitzer, Donny, Dierker, Flory, & Manuck, 2008), suggesting that the effect should be larger for heavier users of tobacco. The analyses of smoking severity in the present study show, at best, only a slight tendency for more cigarettes smoked with higher gain discounting, and slightly shorter time to the first cigarette of the day with higher gain and loss discounting (Table 4; see also Bickel et al., 2012). However, the confidence intervals in the present study were wide, and it is possible that the moderate levels of tobacco use in the present samples could be a problem for identifying effects that exist in heavier users of tobacco.
In comparison with results from the literature, the association between gain discounting and risky drinking was weak. Although studies using one-item measures of discounting have found very small effects (e.g., Rossow, 2008), the typical effect sizes for comparisons of controls and different classifications of problematic drinking have been about d = –0.5 or higher (see MacKillop et al., 2011). However, the present results are more in line with some of the larger studies in the literature. A study of 121 alcohol-dependent participants and 98 controls yielded a group difference of d = –0.18 (Bobova et al., 2009), and a study employing a large MTurk sample of 523 non-problem drinkers and 269 hazardous-to-harmful drinkers (AUDIT score of 8+) reported group differences corresponding to d = –0.16 (Bickel et al., 2012); almost identical to the effect in the present data. The effect size for smoking in the current study was also smaller than reported in past literature (MacKillop et al., 2011) but seems to be in line with results from other large studies (e.g., Jarmolowicz et al., 2012).
Could the null results for cost discounting be due to low reliability of the measures? Assuming that the effect size for cost discounting should be comparable to the effect for smoking and gain discounting, a reliability as low as .50 would give an expected effect size of about .25 (calculated by disattenuating the effect size for gain discounting and attenuating this true-effect estimate). This expected effect size is outside the present credibility intervals of the meta-analyses on cost discounting, and it is therefore not likely that the lack of effect is due to low reliability (assuming a similar effect size). Furthermore, the reliability of the three cost discounting measures in Studies 3 and 4 was acceptable to high.
The results were relatively consistent across a range of measurement methods, but all the methods involved hypothetical choices. The use of hypothetical choices may limit the generalisability of the results, but several studies have documented a close correspondence between decisions regarding actual and hypothetical outcomes (e.g., Matusiewicz et al., 2013). Another limitation of the generalisability of the findings is that the samples were recruited through MTurk. We cannot preclude the possibility that discounting of costs is consequential in more clinical settings.
Furthermore, we have chosen to investigate two types of addictive behaviours, smoking and drinking, with relatively lenient cut-offs. We included non-daily smokers in the smoking group and we set the AUDIT cut-off at 10 (hazardous drinking) instead of e.g. 20 (possible dependence). This decision was partly based on the high prevalence of the chosen behaviours. High prevalence makes it feasible to obtain enough data for meaningful group comparisons, and it also means that the behaviours are interesting in their own rights due to the costs they inflict on many individuals. However, for the same reason, the behaviours may not be good representatives of more severe forms of addictive behaviours. The analyses of smoking severity hinted at a possible association between cost discounting and more severe forms of addictive behaviour.
The participants did not discount much on the cost discounting measures (for descriptive data see the online Supplementary Materials), which indicates that people prefer to avoid the dread of future payments, regardless of their smoking or AUDIT status. Even when targeting the point of negative vs. positive discounting (choice between equal amounts today vs. in the future) with a supplemental measure in Study 3, the effect size was practically zero. This was somewhat surprising, since it seemed reasonable that people with potentially harmful substance use patterns, who are often characterised by impulsiveness relating to lack of foresight and planning for the future, would care more about avoiding an immediate cost than a future one. However, lack of planning/foresight may have two different interpretations: one is that the future is undervalued or disregarded, but another is impatience in the form of wanting things now, whether good or bad (see Hardisty, Appelt, & Weber, 2013). The results did not show a tendency towards of the predictions, with more choices of immediate costs for smokers. It does therefore not appear as though smokers have a general tendency to do things now. In principle, a desire to do things now and a devaluation of future costs could cancel each other out. However, the most parsimonious interpretation of the present data is that smokers and individuals with a risky drinking pattern discount costs in a similar manner to other individuals. This suggests that higher cost discounting is not a vulnerability factor for substance use, and that the higher rates of discounting of gains observed for individuals with substance use problems do not generalise to all types of value.
In conclusion, discounting of cost, as operationalised by choices between present and future payments, was not associated with smoking status or a measure of hazardous drinking (AUDIT score of 10+). The present studies replicated the association between smoking status and discounting of gains and showed that the effect was robust across different measures. The association between hazardous drinking and gain discounting was weak. As smokers discount rewards, but not costs, the association between smoking and discounting does not seem to be due to a general devaluation of future consequences.
Supplemental material
Supplemental Material, sj-doc-1-nad-10.1177_1455072520985971 - Smoking, hazardous drinking and individual differences in cost and gain discounting
Supplemental Material, sj-doc-1-nad-10.1177_1455072520985971 for Smoking, hazardous drinking and individual differences in cost and gain discounting by Torleif Halkjelsvik in Nordic Studies on Alcohol and Drugs
Footnotes
Declaration of conflicting interests
The author declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author received no financial support for the research, authorship, and/or publication of this article.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.