
Abstract
Aim:
This study estimated (i) the risk function between different indicators of alcohol use and long-term sickness absence, adjusting for possible confounding factors, (ii) whether the risk function between average volume of consumption and sickness absence is modified by heavy episodic drinking (HED), and (iii) to what extent the risk for sickness absence among abstainers is due to health selection bias.
Data and methods:
The study was based on data from the Stockholm Public Health Cohort 2006, with an analytical sample of 16,477 respondents aged 18–64 years. The outcome included register-based long-term (> 14 days) sickness absence. Negative binominal regression was used to estimate the association between sickness absence and average weekly volume of consumption, frequency of HED, and both in interaction.
Results:
Abstainers, chronic heavy drinkers and respondents with the highest frequency of HED had approximately two-fold higher rates of sickness absence relative to the reference groups, i.e., moderate drinkers and those with HED one to 6 times per year. Adjustment for confounding factors did not materially affect the shape of the risk function. After exclusion of abstainers with alcohol-related problems, or poor health, the estimates for abstainers became non-significant. Moderate drinkers with HED did not have significantly higher rates of sickness absence than moderate drinkers without HED.
Conclusions:
Our results suggest a significant association between alcohol use and sickness absence. There were indications that the U-shaped risk function may largely be due to health selection bias among abstainers. We found no indication of effect modification of HED on moderate drinking.
Keywords
Sickness absence is associated with substantial costs at the individual and societal levels (Alexanderson & Norlund, 2004). In 2012, the public expenditure on sick leave was on average 0.97% of GDP in the member states of the European Union (Spasova et al., 2016). Moreover, sickness absence has been linked to other adverse outcomes, such as disability pension and premature mortality (Kivimäki et al., 2004; Kivimäki et al., 2003; Vahtera et al., 2004). Considering the public health and economic burden related to sickness absence, it is of great importance to assess the importance of modifiable risk factors for this outcome.
Alcohol use is one factor that has attracted increased attention in this context. Several plausible pathways and mechanisms may underlie a link between alcohol use and sickness absence. First, alcohol use, and in particular chronic heavy drinking, is causally linked to a large number of chronic health conditions and mental disorders (Rehm et al., 2017), of which the latter form one of the main diagnosis groups underlying sickness absence (Alexanderson & Norlund, 2004; Virtanen et al., 2018). Second, single occasions of heavy episodic drinking (HED) may result in acute impairment of work capacity, thus increasing the risk of short-term sickness absence. Finally, HED is related to an elevated risk of diagnoses arising from external causes, such as injuries and poisonings (Rehm et al., 2017), which account for a substantial proportion of all sickness absence (Alexanderson & Norlund, 2004; Virtanen et al., 2018).
Still, while numerous studies have found a link between alcohol use and sickness absence, two separate reviews concluded that previous research tends to suffer from limitations that impair the possibilities of pursuing causality of the association at issue (Hensing et al., 2010; Schou & Moan, 2016). For instance, most studies tend to be based on cross-sectional and/or non-representative samples, use poor measures of alcohol use or sickness absence, and fail to satisfactorily account for potentially confounding factors, such as other health-related behaviours and working conditions (Hensing et al., 2010; Schou & Moan, 2016).
Moreover, in line with some other alcohol-related health outcomes, including cardiovascular disease and all-cause mortality, the associations between alcohol and sickness absence found in cohort studies tend to be J- or U-shaped, i.e., with elevated risk among both abstainers and heavy drinkers in relation to light or moderate drinkers (Jørgensen et al., 2017; Upmark et al., 1999; Vahtera et al., 2002). However, it is not evident how the shape of the alcohol risk function should be interpreted in the context of sickness absence. On the one hand, the findings may imply that moderate alcohol consumption has a protective effect on sickness absence. But on the other, the findings may result from confounding or health selection bias, meaning that the group of non-drinkers tend to contain a significant proportion of individuals who have stopped drinking because of ill health (also termed sick quitter bias), as well as individuals abstaining because of previous alcohol problems. In this case, the elevated risk of sickness absence for this group would not reflect the true risks associated with non-drinking (Schou & Moan, 2016; Vahtera et al., 2002).
While the curve linear association between alcohol and cardiovascular disease has received considerable attention and debate, there is a lack of studies addressing these issues in relation to sickness absence. For instance, numerous recent reviews and meta-analyses have found health selection bias to account for a large proportion of the protective effect of alcohol in relation to cardiovascular disease (Fillmore et al., 2006; Naimi et al., 2017). To our knowledge, only one study has systematically explored the curve linear association between alcohol use and sickness absence, revealing a U-shaped association between alcohol and sickness absence that remained also after adjustment for factors associated with selection bias, including psychosocial problems, health status and former drinking (Vahtera et al., 2002). However, the analyses were based on a sample of municipal employees, thus impairing generalisations to the general working population. Furthermore, simply adjusting for pre-existing health conditions, or excluding those with poor baseline health, could actually introduce bias to the models. While this procedure (correctly) would exclude non-drinkers who have stopped drinking due to ill health, it would also exclude cases of ill health among drinkers that actually are caused, or aggravated, by alcohol consumption, thus increasing the seemingly protective effect of non-drinking (Naimi et al., 2017). One way of handling this issue would be to exclude individuals with poor baseline health from the group of non-drinkers only (and not from the groups of drinkers).
Within alcohol epidemiology it is well established that both volume of consumption and pattern of drinking (typically measured as frequency of HED) as well as their possible interaction, should be considered when assessing the link between alcohol use and health outcomes (Babor et al., 2010; Rehm et al., 2017). In line with this, recent meta-analyses have found that the relationship between average volume and cardiovascular disease is modified by HED, so that moderate drinkers with HED have an increased risk (rate ratio [RR] 1.75) relative to moderate drinkers without HED (Roerecke & Rehm, 2010, 2014). Hence, the apparent protective effect of moderate drinking disappears when combined with HED, implying that only considering average volume of consumption is not sufficient to fully depict the risk function between alcohol use and cardiovascular disease. Considering that HED is related to many of the diagnoses underlying sickness absence (Rehm et al., 2017), it is possible that moderate consumption is modified by HED also for this outcome. However, so far, no study has addressed this issue in relation to sickness absence.
The present study aims to overcome the above-mentioned limitations of previous research on the link between alcohol use and sickness absence by using data from a large and representative register-linked cohort from Stockholm County. More specifically, we will estimate the risk function between alcohol use (average volume and frequency of HED) and long-term sickness absence (> 14 days) and assess to what degree the relationship is affected by potentially confounding factors, including socioeconomic position (SEP), working conditions, and other lifestyle factors. To further strengthen our approach, we will test whether the risk function between average volume of consumption and sickness absence is modified by frequency of HED, and explore to what extent the risk for sickness absence among non-drinkers can be attributed to pre-existing health conditions and history of alcohol-related problems.
Data and methods
Study population
The analyses were based on data from the 2006 baseline of the Stockholm Public Health Cohort (SPHC). The SPHC is a cohort study with data from an area- and sex-stratified random sample of residents in Stockholm County, Sweden. SPHC data collection procedures and response rates are described in full elsewhere (Svensson et al., 2013). The SPHC survey is sent out every fourth year and comprises questions on health, lifestyle, social relations, housing, finances, occupation, working conditions, and sickness absence. To mitigate sampling error and attrition bias, the SPHC employed calibrated weights computed by Statistics Sweden using register-based auxiliary data on age, sex, country of birth, area of residence, marital status, income and educational level, along with their covariation with survey-based data (Svensson et al., 2013). Out of the sample frame in 2006 (56,634 individuals aged 18–84 years) 34,707 individuals (61%) responded. Respondents who were between 18 and 64 years of age, employed or engaged in similar activity daily, without register-based (> 14 days) sickness absence the year before baseline and without missing information on the studied variables, constituted the analytical sample for the present study, n = 16,477.
Measures
Outcome
Information on sickness absence was obtained from the Swedish social insurance registers, which are compiled by the Swedish Social Insurance Agency (Försäkringskassan). In the Swedish insurance system, the first 14 days of a sickness absence period (minus the first “qualifying” day) are covered by the employer. From day 14 onwards, sickness benefits are paid by the Social Insurance Agency and registered in the social insurance registers. Accordingly, the register includes information on the number of sickness absence days, after day 14. As outcome measure for the present study we calculated the number of sickness absence days (after day 14) that occurred between entry into the study (14 September 2006 at the earliest) until date of emigration, disability pension, retirement by age, death, or end of follow-up (31 December 2008).
Exposure: Alcohol use
Self-reported information on alcohol use was collected from the baseline survey and measured as average volume of weekly alcohol consumption and frequency of HED. For the volume measure, the respondents were asked about the amounts (in centilitres) of spirits, wine, beer, and cider/alcopops they consume during a “normal week”. Average volume of consumption was then calculated by converting the centilitres of each beverage consumed into grams of 100% alcohol intake per week, and categorised into five groups, with separate cut-offs for men and women: abstainers (0 g), light (men and women: > 0 to 84 g 100% alcohol/week), moderate (men: > 84 to 252 g, women: > 84 to 168 g), heavy (men: > 252 to 420 g, women: > 168 to 280 g) and chronic heavy drinkers (men: > 420 g, women: > 280 g) (Roerecke & Rehm, 2014; Smyth et al., 2015). Frequency of HED was defined as the number of times a respondent had consumed alcohol amounting to at least 120 g 100% alcohol on a single occasion in the last 12 months, and divided into five categories: abstainers, drinkers with no HED, HED one to six times per year, HED one to three times per month and HED once a week or more often.
To test whether the risk function for volume of consumption is modified by HED, we constructed an interaction variable that combined the average volume and frequency of HED, consisting of eight categories: (i) abstainers, (ii) light drinkers, (iii) moderate drinkers with no HED, (iv) moderate drinkers with HED one to six times/year, (v) moderate drinkers with HED monthly or more often, (vi) heavy drinkers with no HED, (vii) heavy drinkers with HED up to three times/month, and (viii) heavy drinkers with HED weekly or more often. As there were few chronic heavy drinkers without HED, we collapsed this group with the heavy drinkers when constructing the interaction variable.
Confounders
As possible confounding variables, we included a number of risk factors for sickness absence that tend to be more prevalent among heavy drinkers and/or abstainers.
SEP was measured using self-reported information on occupational class retrieved from the baseline survey. The respondents indicated their current (or previous) occupation, which was categorised into six groups according to the Swedish socioeconomic classification of occupations (Statistics Sweden, 1982): unskilled workers, skilled workers, lower non-manual employees, intermediate non-manual employees, higher non-manual employees, and self-employed.
Working conditions: Physical working conditions were measured using the question, “How much have you moved or exerted yourself physically at work during the past 12 months?” with the response alternatives: sedentary work (your job is predominantly sedentary), light physical work (your work involves moving/walking around a lot, but no heavy lifts), moderately heavy work (your work involves moving/walking around a lot, some heavy lifts, and/or walking on stairs or slopes), and heavy work (your work involves lifting heavy objects and exerting a lot of physical effort). The responses were coded into a variable with the categories: sedentary to light work, moderately heavy work and heavy work.
Psychosocial working conditions were assessed using eight questions measuring the degree of job control and job demands. The questions were derived from the demand–control model that builds on the notion that employees who do not have sufficient job control to meet the demands of their job will experience job strain, which in turn is related to increased risk of several health outcomes, including sickness absence (De Lange et al., 2003). The questions were combined into a variable with the categories: high strain (low control with high demands), passive work (low control with low demands), active work (high control with high demands), and low strain (high control with low demands).
Lifestyle factors: To assess the possible contribution of lifestyle factors, we created a lifestyle index including information on: smoking status, snuff use status (wet smokeless tobacco), body mass index (BMI), physical activity (PA), sleep duration, and vegetable and fruit intake. In line with previous research (Foster et al., 2018; Public Health Agency of Sweden, 2019; Skillgate et al., 2017), respondents received 1 point for each unhealthy lifestyle factor: current daily smoking, current daily use of snuff, less than 150 min per week of moderate PA, sleeping less than 7 hours or more than 9 hours per night, eating less than four portions of fruit and vegetable per day, or having a BMI of less than 18.5 or more than 25. The index variable was coded into three categories: most healthy (0–2 points), moderately healthy (3–4 points) and most unhealthy (5–6 points).
Health selection variables
To assess the possible effect of health selection bias among abstainers we included the following variables:
Alcohol-related disorders were measured using alcohol-related hospitalisations prior to baseline or during follow-up. This information was obtained through record linkage with the National Hospital Discharge register and included the following ICD codes: ICD-9: 291, 303, 305A, 357F, 425F, 535D, 570.0, 570.1, 571A-D, 790D, 980; ICD-10: E244, F10, G312, G621, G721, I426, K292, K70, K852, K864-7, O354, T51, X45, X65, Z502, Z714, Z721, Y90, Y91.
Self-rated health was measured using the question, “How do you assess your overall health condition?”, with five response options ranging from “very good” to “very bad”. The responses were categorised into a dichotomous variable where “bad” or “very bad” was coded as 1.
Mental health status was measured using 12 questions corresponding to the 12-item version of the General Health Questionnaire (GHQ12). The GHQ12 is a well-established scale for screening of psychiatric morbidity in general population samples. Following a previous study of the association between GHQ12 and sickness absence, we applied a ¾ threshold to identify cases with poor mental health status (Virtanen et al., 2007).
Health-related quality of life (HRQoL) was measured using the EQ-5D (The EuroQol Group, 1990). This scale includes five dimensions of HRQoL: mobility (ability to walk), self-care (daily personal care), usual activities (e.g., work, study, housework, family or leisure activities), pain/discomfort and anxiety/depression. There were three response levels for each of the dimensions: “no problems”, “some problems” or “severe problems”. For the analyses, the variable was coded into the categories “no problems” and “some or severe problems”.
Statistical analyses
The association between alcohol use and sickness absence was estimated using negative binomial regression. The regression estimates express rate ratios (RR), and their 95% confidence intervals (CI). We included an offset variable measuring the logarithm of person–time at risk in the study, calculated from the date a participant entered the study (14 September 2006 at the earliest) until being censored by date of emigration, retirement by age, disability pension, death, or end of follow-up (31 December 2008). The Statistics Sweden calibration weights mentioned above under “Study population” were used to ensure that the study sample was representative of the target population of Stockholm County in terms of the major sociodemographic and health-related determinants (Svensson et al., 2013).
We found no significant interaction between sex and alcohol use in relation to sickness absence. Therefore, the analyses were performed on the full sample of men and women combined. All models were adjusted for the background covariates age (as a continuous variable), sex, and country of birth.
In a first step, we estimated a minimally adjusted model of the association with sickness absence for each of the alcohol use measures (adjusted for age, sex, and country of birth). Next, we estimated a series of models with separate adjustment for the possible confounders (i) SEP, (ii) working conditions, and (iii) lifestyle factors. Finally, we estimated a fully adjusted model where all confounders were entered concurrently.
The percentage attenuation on the RR estimates following adjustment for confounders was calculated using the following formula: (RRminimally adjusted – RRadjusted)/(RRminimally adjusted –1) × 100.
To assess the possible effect of health selection bias among abstainers, we replicated the fully adjusted models, after excluding abstainers with an alcohol-related disorder prior to baseline or during follow-up (n = 45), and abstainers who reported poor self-rated health, poor mental health status or HRQoL problems at baseline (n = 599).
Ethical considerations
Respondents to the SPHC baseline survey gave informed consent for register linkage. Ethical approval for the present study was obtained from the Regional Ethical Review Board in Stockholm: Dnr 20–/320-31/5.
Results
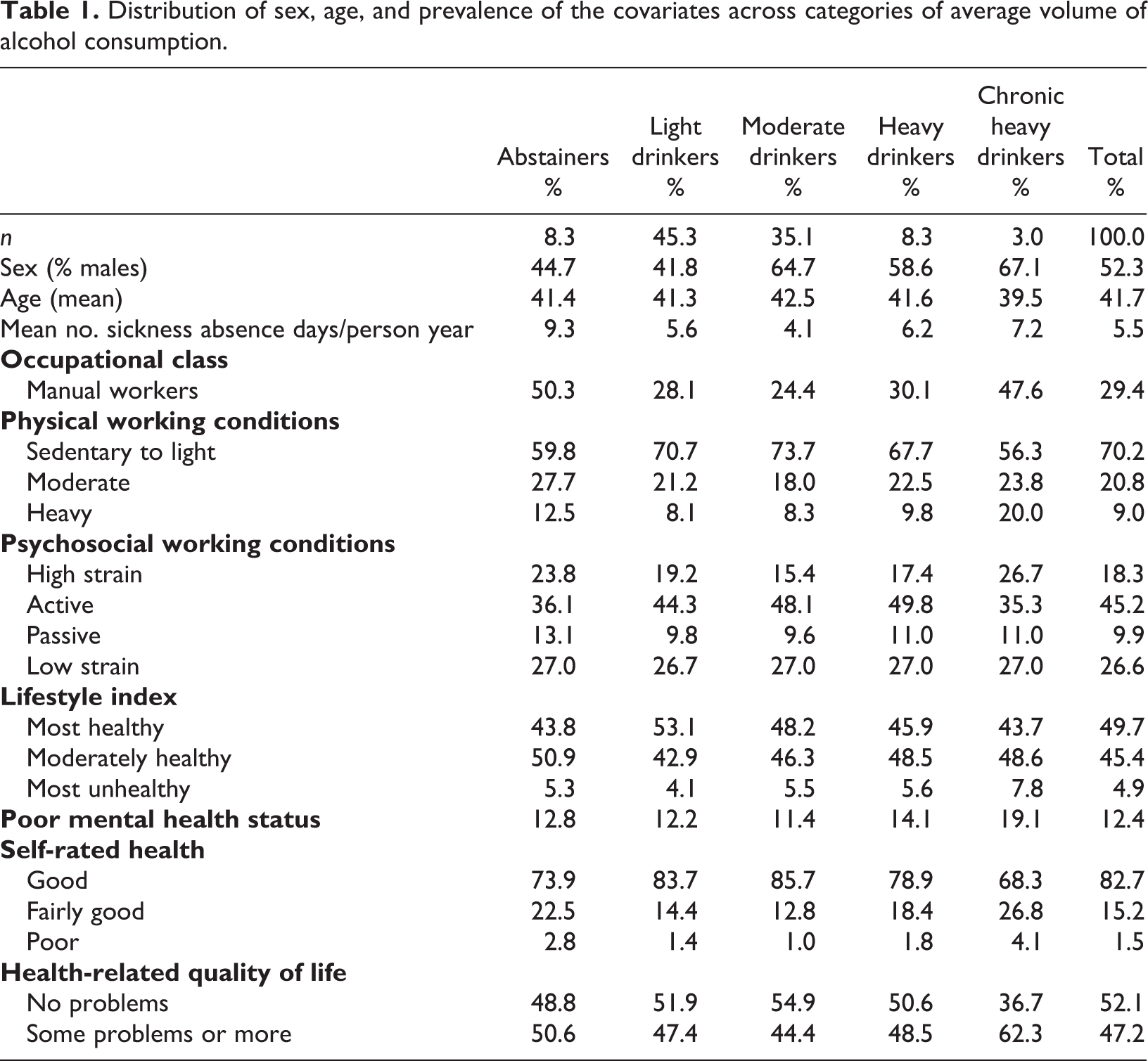
Tables 1 and 2 show the distribution of sex, age, and the prevalence of the possibly confounding variables across the measures of average volume of consumption and frequency of HED. The prevalence of the variables generally displays a U- or J-shaped association with the alcohol use measures. For instance, compared to moderate drinkers, both abstainers and heavy/chronic heavy drinkers were more likely to be manual workers, have heavy working conditions, high job strain and to be in the group with the unhealthiest lifestyle. Likewise, the three health-related measures indicative of poorer health were generally more prevalent among abstainers and heavy/chronic heavy drinkers than among moderate drinkers. However, mental health status was an exception, with an elevated prevalence of poor mental health only among chronic heavy drinkers.
Distribution of sex, age, and prevalence of the covariates across categories of average volume of alcohol consumption.
Distribution of sex, age, and prevalence of the covariate variables across categories of frequency of heavy episodic drinking (HED).
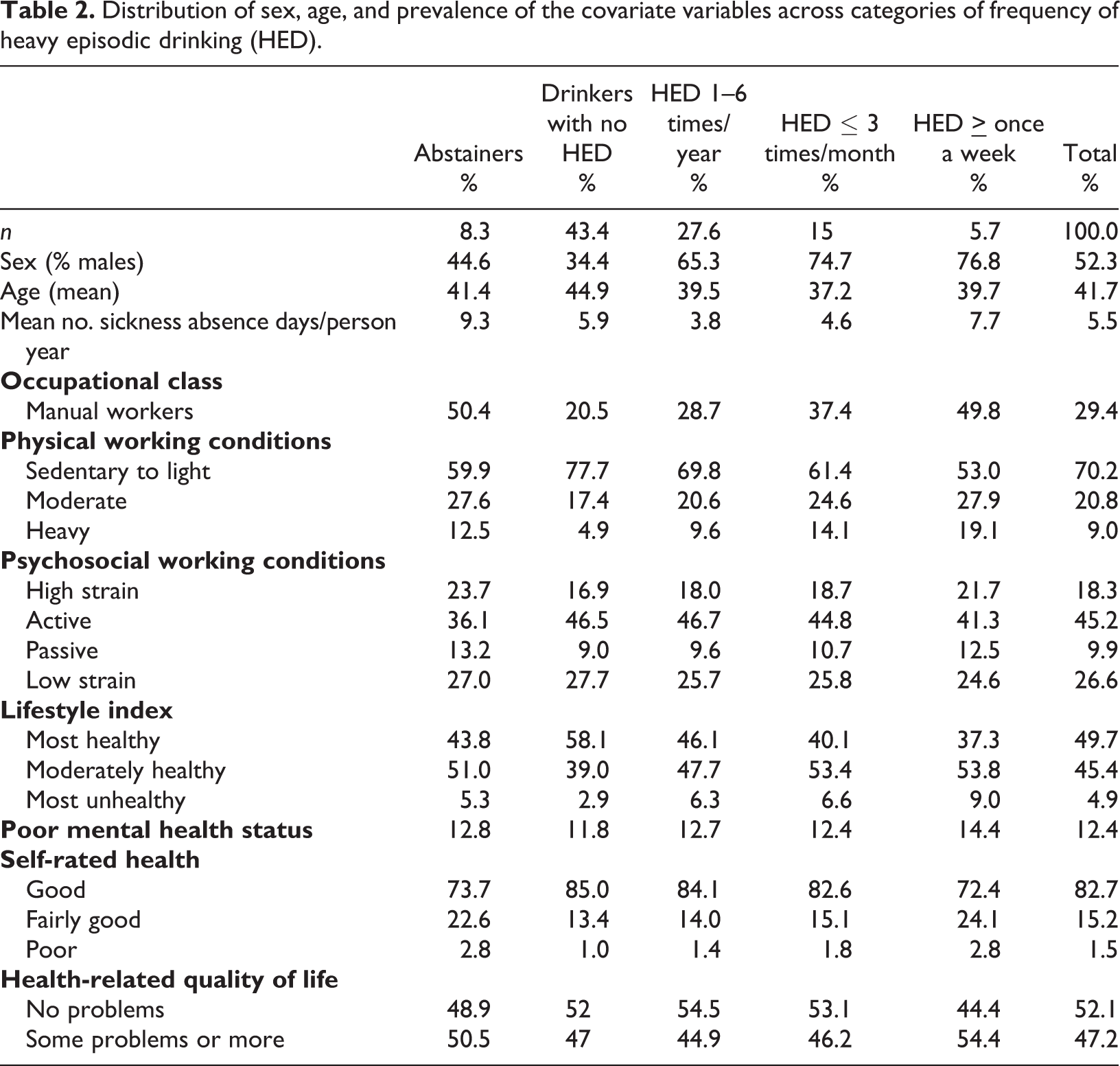
Similar associations were found for frequency of HED. That is, the prevalence of the most unfavourable categories of the confounding variables was generally higher among abstainers and respondents who reported HED once a month or more often compared to drinkers without HED.
With regard to the association to sex and age differences, heavy drinking and higher frequency of HED were more common among men than women and among lower ages.
The association between alcohol use and sickness absence
Both alcohol use measures were significantly associated to sickness absence, with U-shaped risk functions (Table 3). Starting with average volume, the minimally adjusted estimates (Model 1, adjustment only for age, sex, and country of birth) for chronic heavy drinkers (RR 2.09 [95% CI 1.27, 3.43]) and abstainers (2.00 [1.44, 2.78]) correspond to an approximate two-fold increase in the rates of sickness absence compared to moderate drinkers, whereas heavy and light drinkers had 44% and 32% higher rates, respectively. Similarly, for frequency of HED the minimally adjusted estimates imply that HED once a week or more often (RR 2.31 [95% CI 1.52, 3.51]), or being an abstainer (RR 1.94 [95% CI 1.36, 2,75]), is associated with an approximate two-fold increase in the rates of sickness absence, relative to respondents with HED one to six times per year – whereas HED up to three times a month (RR 1.41 [95% CI 0.92, 2.17]) is associated with 40% higher rates.
Negative binomial regression models of the association between different indicators of alcohol use and long-term sickness absence (> 14 days). Rate ratios (RR) with 95% confidence intervals (95% CI). All models adjusted for sex, age, and country of birth.
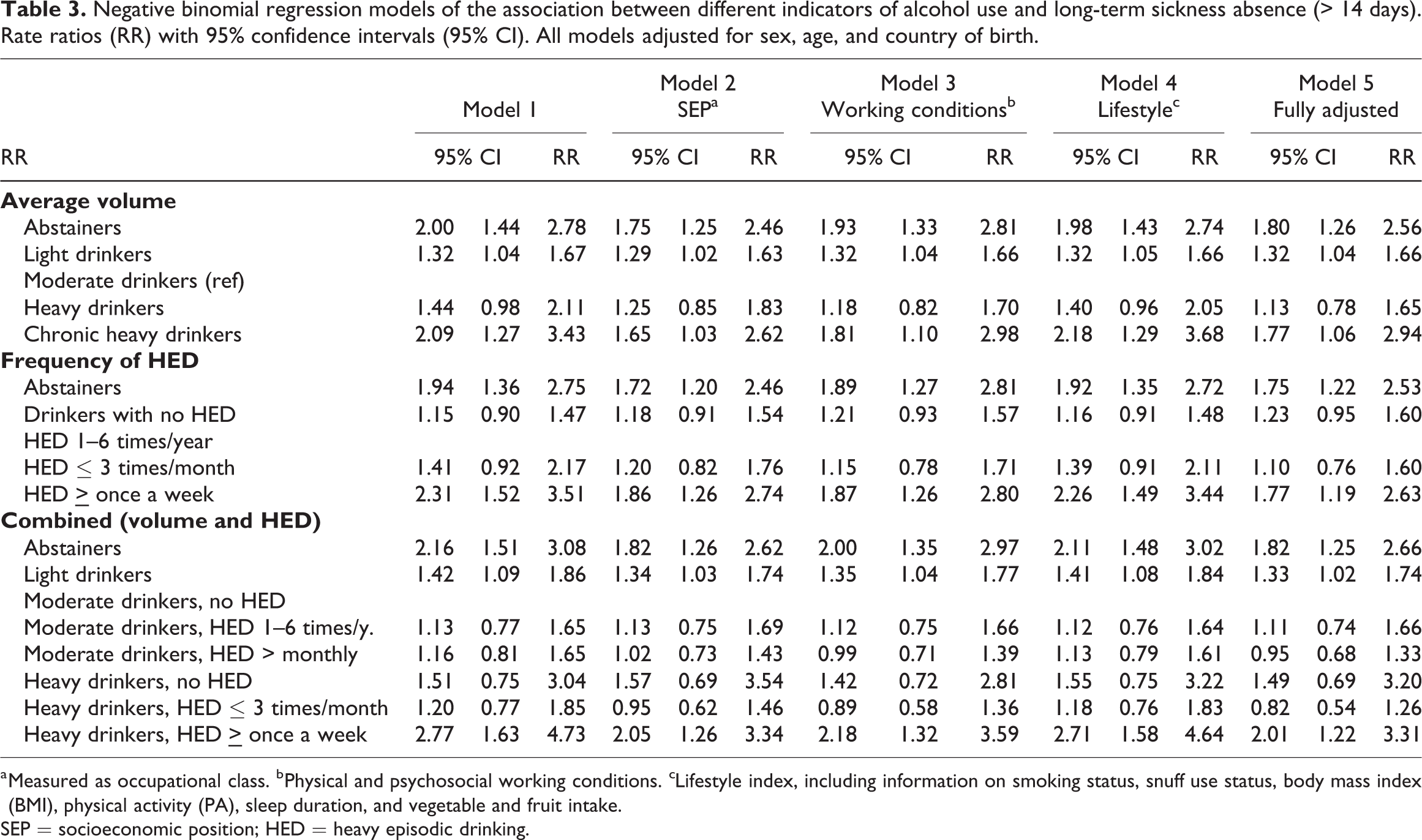
a Measured as occupational class. bPhysical and psychosocial working conditions. cLifestyle index, including information on smoking status, snuff use status, body mass index (BMI), physical activity (PA), sleep duration, and vegetable and fruit intake.
SEP = socioeconomic position; HED = heavy episodic drinking.
Adjustment for possible confounders (Models 2 to 4, adjusted for SEP, working conditions, and lifestyle factors, respectively) did not substantially affect the RR estimates for abstainers, chronic heavy drinkers, or respondents who reported HED at least once a week. However, for heavy drinkers and respondents who reported HED up to three times a month, adjustment for SEP and working conditions resulted in larger attenuations of the RR estimates: by 43% and 59%, and 51% and 61%, respectively. In the fully adjusted model (Model 5) the RR estimates became close to fully attenuated, i.e., by 70% for heavy drinkers and 76% for those with HED up to three times a month.
Moving on to the combined measure of average volume and frequency of HED, we found no evidence of effect modification of HED on moderate consumption. That is, moderate drinkers with HED one to six times a year (RR 1.13 [95% CI 0.77, 1.65]) or HED once a month or more often (RR 1.16 [95% CI 0.81, 1.65]) did not have significantly higher rates of sickness absence compared to moderate drinkers without HED. The only category above moderate drinking that obtained a significant RR estimate was heavy drinkers with HED at least once a week (RR 2.77 [95% CI 1.63, 4.73]), who had an approximate three-fold increase in the rates of sickness absence. Moreover, both abstainers and light drinkers obtained positive and significant RR estimates, indicating a U-shaped risk function also for this variable.
Assessment of health selection bias among abstainers
Replicating the fully adjusted models after exclusion of abstainers with alcohol-related disorders (Model 1, Table 4) did not materially affect the estimates for abstainers in any of the alcohol use measures. However, after additional exclusion of abstainers with poor baseline health (Model 2) the RR estimates for abstainers turned non-significant both relative to moderate drinkers (RR 1.27 [95% CI 0.72, 2.24]) and those with HED one to six times a year (RR 1.25 [95% CI 0.70, 2.23]), and were close to fully attenuated, by approximately 75%, compared to the minimally adjusted models Table 3.
Negative binomial regression models of the association between different indicators of alcohol use and long-term sickness absence (> 14 days), excluding abstainers with alcohol-related diagnosis or with poor health at baseline. Rate ratios (RR) with 95% confidence intervals (95% CI). All models adjusted for sex, age, country of birth, socioeconomic position (SEP), working conditions and lifestyle factors.
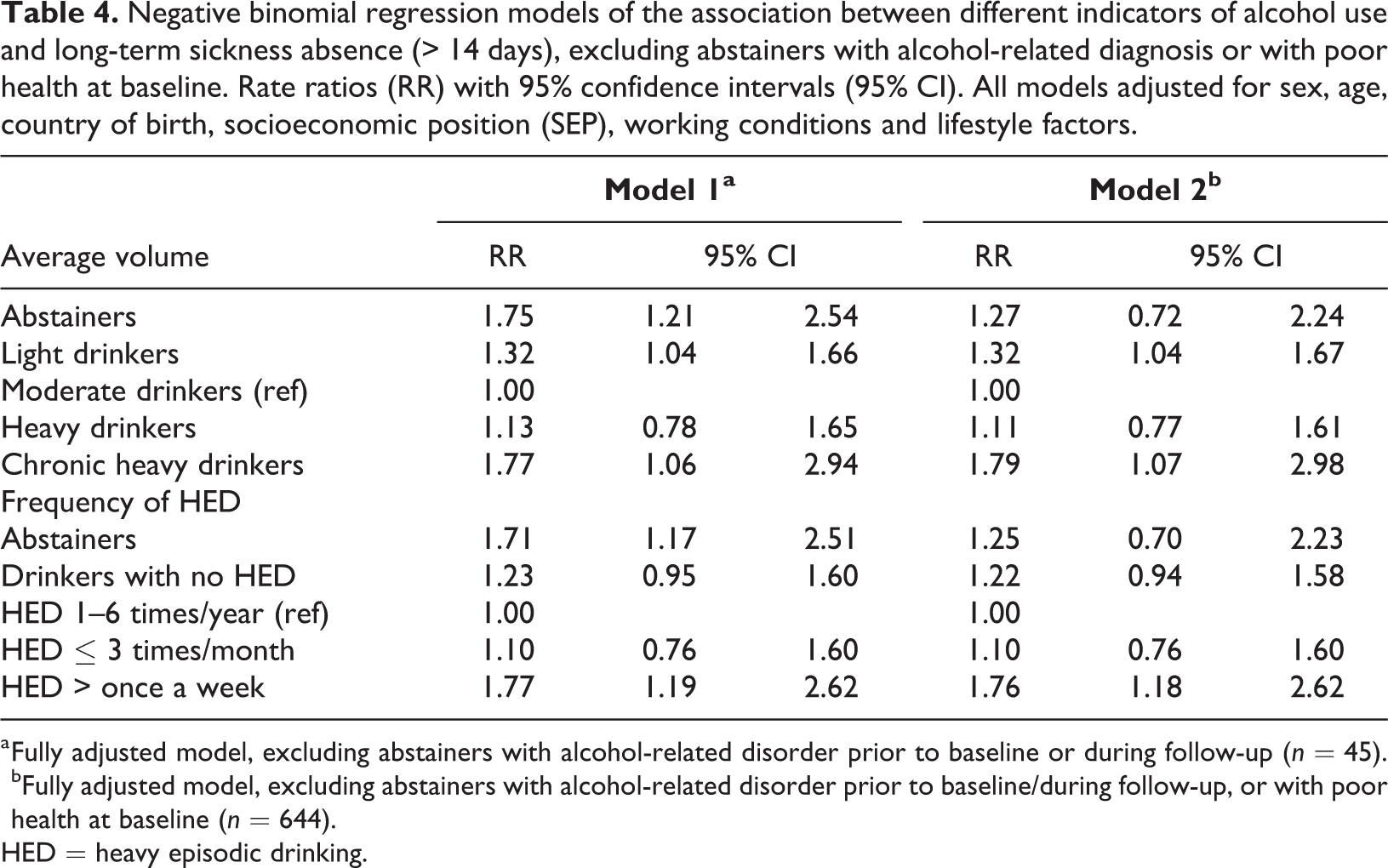
a Fully adjusted model, excluding abstainers with alcohol-related disorder prior to baseline or during follow-up (n = 45). bFully adjusted model, excluding abstainers with alcohol-related disorder prior to baseline/during follow-up, or with poor health at baseline (n = 644).
HED = heavy episodic drinking.
Discussion
Aiming to improve on previous research, this article has used data from a large and representative register-linked cohort from Stockholm County, to explore various aspects of the association between alcohol use and long-term sickness absence.
First, we estimated the risk function between alcohol use and long-term sickness absence and assessed to what degree the association may be attributed to confounding factors and health selection bias among abstainers. Consistent with several previous studies (Jørgensen et al., 2017; Upmark et al., 1999; Vahtera et al., 2002), we found U-shaped relationships. Being an abstainer, a chronic heavy drinker, or reporting HED at least once a week was associated with a two-fold increase in rates of sickness absence compared to the reference groups, i.e., moderate drinkers and those who reported HED one to six times per year. Adjustment for factors that may underlie the increased risk among both abstainers and heavy drinkers, including SEP, working conditions, and lifestyle factors, did not materially change the shape of the risk function. This result is partly in line with the findings of Salonsalmi et al. (2009), that working conditions only accounted for a small part of the association between alcohol use and self-certified sickness absence. However, in our fully adjusted models, the RR estimates for heavy drinkers and those who reported HED up to three times a month became close to fully attenuated. Our study thus adds to previous research by showing that it is primarily the most hazardous levels and patterns of drinking (i.e., chronic heavy drinking and HED once a week or more often) that are related to later sickness absence, over and above the influence of SEP and working conditions. Moreover, while the elevated rates of sickness absence among abstainers could not be attributed to previous drinking problems, we found indications that the increased risk for this group may be largely due to health selection bias. That is, excluding abstainers with alcohol-related disorders did not affect the increased rates of sickness absence for this group, whereas additional exclusion of abstainers with poor baseline health resulted in substantial attenuations and non-significant RR estimates. Still, this finding should be interpreted with caution, considering that we cannot determine what proportion of the attenuations are due to exclusion of abstainers who have stopped drinking because of ill health, or to cases that reflect a general clustering of health problems among non-drinkers.
Second, following recent research on the risk function between alcohol use and cardiovascular disease, we tested whether the association between average volume and long-term sickness absence is modified by HED, so that the protective effect of moderate drinking disappears when it is combined with HED (Roerecke & Rehm, 2010, 2014). Our findings suggest that this notion is not applicable in the context of alcohol and long-term sickness absence. That is, moderate drinkers with HED did not have significantly higher rates of sickness absence compared to moderate drinkers without HED, including after adjustment for possible confounders. Rather, the only category above moderate drinking that obtained a significant RR estimate was the group with the most hazardous combination, heavy drinkers who reported HED at least once a week. The lack of effect modification of HED on moderate drinking can be attributed to the risk function between frequency of HED and sickness absence (Table 3), i.e., the lowest rates of sickness absence were actually found among those with HED one to six times a year, rather than among drinkers without HED (as would have been expected in the case of effect modification). Still, it is possible that the notion of effect modification of HED on moderate drinking would be more valid for short-term sickness absence, which to a larger degree may be attributable to absence due to single HED occasions (e.g., hangovers), compared to the outcome of long-term sickness absence used in the present study.
Some limitations of the study should be mentioned. First, we lacked the possibility to separate the group of abstainers into lifetime abstainers and former drinkers. Research on alcohol use and cardiovascular disease suggests that the increased risk among non-drinkers tends to become weaker, or disappear, when defined as lifetime abstainers (Naimi et al., 2017). Hence, it is likely that the U-shaped risk function between alcohol and sickness absence would have become weaker if we also had separated former drinkers from lifetime abstainers. Still, an indication that this not might be the case is provided in a study by Vahtera et al. (2002), who found a U-shaped association between alcohol and sickness absence, even after separation of abstainers into former drinkers and lifetime abstainers. Second, we did not have access to diagnosis-specific sickness absence. This is a limitation, considering that previous research has found that the U-shaped risk function between alcohol and sickness can be largely attributed to sickness absence due to chronic somatic and mental illness diagnoses being more common among abstainers, whereas sickness absence due to injuries or poisonings is more common among heavy drinkers (Ervasti et al., 2018). Finally, it should be noted that the threshold for HED used in the present study, 120 g on one occasion, is higher than the standard cut-off. It is possible that the use of a lower threshold, e.g., 60 g, would result in significant effect moderation of HED on volume.
In conclusion, our results suggest a significant association between both studied measures of alcohol use and sickness absence. However, only the highest levels of consumption and frequency of HED were significantly related to sickness absence, over and above the influence of SEP, working conditions and lifestyle factors. Moreover, there were indications that the U-shaped risk function between alcohol use and sickness absence is largely due to health selection bias among the group of abstainers. Lastly, the association between volume of consumption and long-term sickness absence does not appear to be moderated by HED. Future studies should test for effect modification by HED, using lower thresholds for HED, and considering also short-term sickness absence as an outcome.
Footnotes
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was funded by Forte, Swedish Research Council for Health, Working Life and Welfare (Swedish: Forskningsrådet for hälsa, arbetsliv och välfärd) Dnr: 2014-02040.