
Abstract
Background and aim:
Although problem gambling typically involves substantial distress, few seek face-to-face treatment. In Norway, problem gamblers can participate in a governmental supported internet- and telephone-based intervention programme. The current study aimed to evaluate the outcomes of this programme in terms of gambling behaviour, gambling-related cognitions and mental health in a one group pre-test post-test design with a follow-up assessment.
Methods:
The sample consisted of the 67 participants who completed the intervention programme within a one-year timeframe. Gambling behaviour (SOGS-R), gambling-related cognitions (GBQ) and mental health (SCL-90-R) were measured pre-intervention, post-intervention and at a 6−12 months follow-up. A total of 25 (37.3%) participants completed the follow-up assessment. T-tests were conducted to investigate development in gambling behaviour, gambling-related cognitions and mental health from pre-intervention to post-intervention and follow-up.
Results:
The analyses showed a significant reduction in gambling behaviour, gambling problems, gambling-related cognitive distortions and mental health symptoms from pre-intervention to post-intervention and follow-up. The corresponding effect sizes for the reductions in gambling and gambling-related cognitive distortions were very large, while the effect sizes for the reductions in mental distress were moderate.
Conclusion:
The internet/telephone programme appears to have several positive outcomes including reduction in gambling behaviour, gambling problems, gambling-related cognitive distortions and symptoms of mental disorders both in the short and long term. Another positive outcome of participation appears to be a lowered threshold for seeking additional treatment. The current study entails, however, important limitations, and future studies should investigate the outcomes of the programme while including a control group.
Keywords
Problem gambling can be defined as gambling behaviour that causes harm to the individual, those close to the individual and/or society (McMillen & Wenzel, 2006). Formally, gambling disorder is defined by endorsement of at least four of the nine diagnostic criteria found in the 5th edition of the Diagnostic and Statistical Manual of Mental Disorders (DSM-5; American Psychiatric Association, 2013). Still, those endorsing two to three criteria (subclinical) report significant distress related to several aspects of psychosocial functioning (Weinstock et al., 2017). In the following, the term “problem gambling” will be used to refer to those satisfying the criteria for gambling disorder, those suffering from subclinical gambling problems, and those who experience their gambling behaviour as problematic.
Estimates of current serious problem gambling prevalence in European countries generally range from 0.5% to 3.0%, although some estimates fall outside this range (Abbott, Romild, & Volberg, 2018; Calado & Griffiths, 2016; Economou et al., 2019; Terzic-Supic et al., 2019). Problem gambling can have serious and detrimental effects for the individual, including mental health problems, in particular depression and suicidal thoughts/behaviours, financial difficulties and relational stress (Langham et al., 2015; Li et al., 2017). Further, problem gambling involves substantial distress in terms of financial harm, emotional pain and relationship conflicts for those close to the gambler (e.g., family, partner); and can be costly on a societal level, including involving loss of productivity at work and burden on the legal system (Ladouceur et al., 1994; Langham et al., 2015; Li et al., 2017). The costs inflicted by gambling problems to the individual, next of kin, and society substantiate the importance of offering treatment for those affected. Problem gambling is often associated with shame and stigma and problem gamblers tend to be hesitant to seek treatment (in particular traditional face-to-face treatment), suggesting that identifying treatment or intervention alternatives that reduce the threshold for problem gamblers to seek treatment should be a priority (Hing et al., 2014; Suurvali et al., 2008; Suurvali et al., 2012). The need for alternative treatment and intervention programmes is also substantiated by findings from prospective studies suggesting that even if the rates of natural recovery from problem gambling are high, so are the relapse rates (Abbott, Romild, & Volberg, 2018; Abbott et al., 2004; Black et al., 2017; Hodgins & El-Guebaly, 2004; Slutske et al., 2009).
Internet- and/or telephone-based interventions (i.e., remote interventions) may be a particularly conducive intervention approach for problem gambling. Such approaches have been shown to be effective in treating a wide range of mental disorders, and may be easier to approach for people who typically avoid face-to-face treatment (e.g., due to stigma) (Bee et al., 2008; Hailey et al., 2008; Hing et al., 2014). Accordingly, some studies have demonstrated that remote intervention programmes may be effective in alleviating both gambling problems and associated mental health problems both the short and long term (Abbott, Hodgins, et al., 2018; Canale et al., 2016; Carlbring et al., 2012; Carlbring & Smit, 2008; Castrén et al., 2013; Hodgins et al., 2019; Hodgins et al., 2004; Myrseth et al., 2013; Yakovenko & Hodgins, 2016). Positive treatment outcomes related to participation in web- and/or telephone-based interventions programmes for problem gambling have also been documented by reviews which generally suggest counsellor contact to be a potent moderator of effects of such interventions (Petry et al., 2017; Rash & Petry, 2014; van der Maas et al., 2019; Yakovenko & Hodgins, 2016).
In Norway, gamblers who self-identify as problem gamblers can participate in a free-of-charge, cognitive behavioural therapy-based, remote intervention programme for problem gambling, i.e., The Norwegian remote intervention programme for problem gambling. The intervention programme lasts for approximately 10 weeks, during which time the participants are given web-based assignments and have telephone sessions with a trained counsellor weekly. The outcomes of this programme in terms of gambling behaviour, gambling-related cognitions and mental health have been investigated in a previous study by Myrseth et al. (2013), who found that participants who completed the programme had a reduction in gambling problems, gambling-related cognitive distortions and symptoms of mental health from pre-intervention to post-intervention, and that the reductions in gambling problems were maintained three months post-intervention. The outcomes of participating in this remote intervention programme in terms of gambling problems over longer time spans than three months have not previously been investigated, nor have there been any previous studies on whether the post-intervention reductions in gambling-related cognitive distortions and symptoms of mental health related to participation in the Norwegian remote intervention programme for problem gambling are maintained beyond intervention completion. Further, the rapid and constant changes in gambling regulations, types of games offered, and intervention alternatives suggest that an updated evaluation of the intervention programme is warranted.
Against this backdrop, the current study aimed to evaluate the outcomes of the Norwegian remote intervention programme for problem gambling in terms of gambling behaviour, gambling cognitions and mental health in a one group pre-test post-test design with a 6–12-month follow-up assessment. In addition, the current study aimed to assess the participants’ experiences with the programme.
Methods
Procedures and sample
The sample consisted of all the 67 participants who completed the intervention programme between August 2017 and August 2018. Only completers of the intervention programme were included in the sample as we wanted to have post-intervention data on all participants. The characteristics of those who entered but did not complete the programme in the timeframe between August 2017 and August 2018 are unfortunately not known. Myrseth et al. (2013), who investigated the same intervention programme as the one investigated in the current study, had a total sample of 112 participants, 32 of these did not complete the programme and 56 participants participated at the three-month follow-up. Myrseth et al. (2013) found no significant differences between completers and non-completers in terms of gender, mental health or severity of gambling problems, but the non-completers were younger, had fewer gambling-related cognitive distortions and were more likely to play poker compared to the completers. A counsellor (not the one who had provided the intervention) attempted contact with all 67 participants by phone up to three times and they were asked to participate in a follow-up assessment, including a phone interview and a web-based survey in the timeframe between August 2018 and February 2019. The follow-up assessment was carried out between 6 and 12 months after intervention completion. A timeframe of 6 to 12 months after intervention completion was chosen to obtain an adequate sample size while ensuring that the data collection period was not too long-lasting as the intervention programme had too few participants to make it feasible to only contact participants who had the same length of time elapsed since intervention completion (e.g., 6 months). In all 36 participants (53.7%) agreed to take part in the follow-up, of these 11 (16.4%) participants completed the follow-up phone interview (but not the survey) and 25 (37.3%) participants completed both the follow-up survey and the phone interview. The participants had to sign a written informed consent form where they were informed that they could be asked to participate in a follow-up study and that the data they contributed with could be used for research, before they gained access to the intervention programme. As this is an evaluation of an existing health service, the study was exempted from approval from the regional committee for medical and health related research ethics in Norway.
The full sample, including those who did and did not participate in the follow-up, consisted of 35.8% women, had a mean age of 39.7 years (SD = 10.9) and consisted of 66.7% who identified themselves as having current gambling problem pre-intervention, whereas the remaining participants regarded themselves as previous problem gamblers pre-intervention. One of the included measures, the South Oaks Gambling Screen – Revised, permits categorising responses into “some gambling problems” and a more severe category, “probable pathological gambling”. At pre-intervention all participants were in the probable pathological gambling group (i.e., both those who self-identified as problem gamblers and those who did not). The finding that all participants were in the probable pathological gambling group may relate to the timeframe of the instrument (past three months) as many of the participants are likely to have experienced gambling problems in this timeframe even if they did not experience problems at the same level when they started the intervention. Further, some participants may have answered based on life-time experiences with gambling problems rather than their experiences in the past three months.
Measurements
Demographics and intervention adherence. The participants’ legal gender and age, number of telephone sessions with counsellor and number of completed web-based assignments were registered.
Gambling behaviour was assessed with the South Oaks Gambling Screen – Revised (SOGS-R) pre-intervention and at the follow-up (Lesieur & Blume, 1987, 1993). The SOGS-R consist of 26 items concerning symptoms of problem gambling (e.g., feelings of guilt in relation to gambling, difficulties controlling own gambling) experienced the past three or six months. The participants in the current study were asked to answer based on their experiences the past three months both at pre-intervention and follow-up. In the first question the respondents are asked to indicate how often (i.e., never; less than once a week; weekly; more often) during the past three months they have gambled on different games (i.e., slot machines; horse betting; sports betting; soccer betting; the national lottery; scratch cards; online gambling; card games; dice games; casinos (legal or illegal); stock market; others). A total of 20 of the items are scored (i.e., 0 or 1) and the composite scores thus range between 0 and 20. Scores of 0 are interpreted as an indication of no gambling problems, scores between 1 and 4 indicate that the respondent is experiencing some gambling problems, while scores of 5 or above indicate that the respondent is a “probable pathological gambler”. In the current study, the SOGS-R obtained a Cronbach’s alpha of .61 pre-intervention, possibly due to low variance at pre-intervention which is common in treatment populations (e.g., Hagatun et al., 2019) and a Cronbach’s alpha of .82 at the follow-up.
Gambling-related cognitions was measured with the Gamblers’ Belief Questionnaire (GBQ) at all assessment points (Steenbergh et al., 2002). The GBQ includes 21 items assessing gambling-related cognitive distortions, where the respondents are asked to indicate to which degree from 1 representing “strongly agree” to 7 representing “strongly disagree”, they agree with statements concerning gambling (e.g., “If I am gambling and losing, I should continue because I don’t want to miss a win”). The items were reversed during scoring so that higher scores indicated more gambling-related cognitive distortions. Total scores range between 21 and 147. The GBQ has two subfacets: “luck/perseverance” which is assessed by 13 items (total score range: 13−91) and “illusion of control” which is assessed by eight items (total score range: 8−56). The full-scale GBQ obtained Cronbach’s alphas of .93, .89 and .95 pre-intervention, post-intervention and at follow-up, respectively. The subscale luck/perseverance obtained Cronbach’s alphas of .92, .81 and .94, respectively, and the subscale illusion of control obtained Cronbach’s alphas of .84, .81 and .89, respectively.
Mental health was assessed with the Symptom Checklist-90-Revised (SCL-90-R; Derogatis, 1994). The SCL-90-R consists of 90 items where the respondents are asked to rate the degree to which (not at all – scored as 0; a little bit – scored as 1; moderately – scored as 2; quite a bit – scored as 3; extremely – scored as 4) different symptoms of psychopathology (e.g., “feeling blue”) have bothered them in the past week. Common ways of scoring the SCL-90-R include computing a Global Severity Index (GSI) which is the mean score on all 90 items, a Positive Symptom Total (PST), which is the number of items endorsed (i.e., scoring 1 or more), and a Positive Symptom Distress Index (PSDI), which represents the mean score on the endorsed items. In the current study, the items of the SCL-90-R obtained Cronbach’s alphas of .98, .99 and .98 at pre-intervention, post-intervention and at follow-up, respectively, which are rather high values. The SCL-90-R was originally designed to assess symptoms of different mental disorders, and thus is a multidimensional measure. However, several scholars have found a unidimensional model to fit better for some groups (e.g., women with depression, individuals with low self-reported levels of distress, community samples), which suggests that the SCL-90-R may actually primarily measure general psychological distress for some groups, rather than different symptoms reflecting different mental disorders (Holi et al., 1998; Paap et al., 2012; Vassend & Skrondal, 1999). Thus, the high Cronbach’s alphas obtained for the SCL-90-R in the current study may in part be attributed to the high number of items included in the SCL-90-R and the instrument’s unidimensional nature in some groups.
Questions in the follow-up interview. In the follow-up phone-interview the participants were asked how satisfied they were with the intervention programme (on a scale of 1−10), whether they had received additional treatment for mental disorders and/or gambling problems since they completed the programme, whether they had experienced difficulties controlling their own video/online gaming in the time after they ended the intervention programme, and whether they had any general feedback to the intervention programme (open-ended question).
Intervention
The Norwegian remote intervention programme for problem gambling is based on principles from cognitive behavioural therapy. Participants are offered weekly phone sessions with a counsellor for approximately 10 weeks. Further, they are given nine assignments, with various topics (e.g., motivation/goals, financial situation, social relationships), which they can perform and submit online. See Myrseth et al. (2013) for a more thorough description of the remote intervention programme.
Analyses
Those who did not participate in the follow-up, those who participated in the follow-up interview but not the survey and those who participated in both the follow-up interview and the survey were compared on demographic characteristics, gambling behaviour, gambling-related cognitions and mental health scores pre-intervention in order to identify potential differences between these groups. Data for comparison purposes were analysed using one-way analyses of variance and chi-square tests.
Changes in gambling behaviour (i.e., active gambling, total score on SOGS-R and the percentage of participants who identified themselves as current problem gamblers) were investigated pre-intervention to follow-up with a paired sample t-test and McNemar’s tests. The active gambling variable was computed by giving respondents who reported weekly or more frequent gambling on at least one of the specific games included in the SOGS-R (excluding the national lottery) in the past three months a score of 1 while those who reported less frequent gambling where given a score of 0. Change in gambling cognitions (i.e., total score on GBQ and scores on the two subscales: luck/perseverance and illusion of control) and mental health (i.e., the three global indexes of SCL-90-R: Global Severity Index, Positive Symptom Total and Positive Symptom Distress Index) pre-intervention to post-intervention and pre-intervention to follow-up were investigated with paired sample t-tests. The effect sizes of the likelihood of being an active gambler and the likelihood of identifying as a problem gambler pre-intervention versus at the follow-up, which was significance tested with McNemar’s tests, were reported as odds ratios (ORs), where ORs of 2.0, 3.0 and 4.0 have been suggested to represent small, moderate and large effect sizes, respectively (Ferguson, 2009). In the paired sample t-tests, the effect sizes of the differences pre-intervention to post-intervention and pre-intervention to follow-up were reported as standardised mean change (Becker, 1988). The standardised mean change scores and their 95% confidence intervals were calculated based on Becker’s (1988) suggestions, where standardised mean change is computed by subtracting mean scores at post-intervention (or at the follow-up) from mean scores at pre-intervention, and dividing this by the standard deviation of the pre-intervention scores. In terms of interpreting the effects’ magnitude, standardised mean change is similar to Cohen’s d, where values of 0.20, 0.50 and 0.80 suggest small, moderate and large effect sizes, respectively (Cohen, 1988). The full sample (N = 67) was included in the analyses comparing pre-intervention to post-intervention scores, while only those who participated in the follow-up survey (i.e., n = 25) were included in the analyses comparing pre-intervention to follow-up scores. For participants who had missing data on one to four items of a scale (approximately two participants per scale), missing values were replaced by the participant’s mean item score on the specific scale. Participants who had missing data on four items or more on a specific scale were excluded from the analyses that included that specific scale. In total one participant (not the same participant for each scale) was excluded from the analyses involving pre-intervention and post-intervention GBQ, pre-intervention SOGS-R and pre-intervention and post-intervention SCL-90-R.
Finally, descriptive analyses of the participants’ responses to the questions at the follow-up interview were conducted. Central tendencies to the questions of recovery from gambling problems, receiving additional mental health treatment after finishing the programme, and having difficulties controlling video/online gaming were computed. Theme coding was used on the open-ended feedback to the intervention programme question, where every answer was carefully read, and the percentage of participants who reported common topics (i.e., mentioned by at least two participants) is reported.
Results
Results from the analyses comparing those who participated in the follow-up and those who did not are presented in Table 1. There were no significant differences between the groups except for the percentage who were actively gambling (i.e., weekly or more often) pre-intervention, where a larger proportion of those who participated in the follow-up were active gamblers pre-intervention compared to those who did not participate in the follow-up. Except for this difference which had a moderate effect size, all the effect sizes of the group differences were within the realms of what is usually considered as small or very small, suggesting potential group differences to be of little practical importance.
Dropout analyses, N = 67.
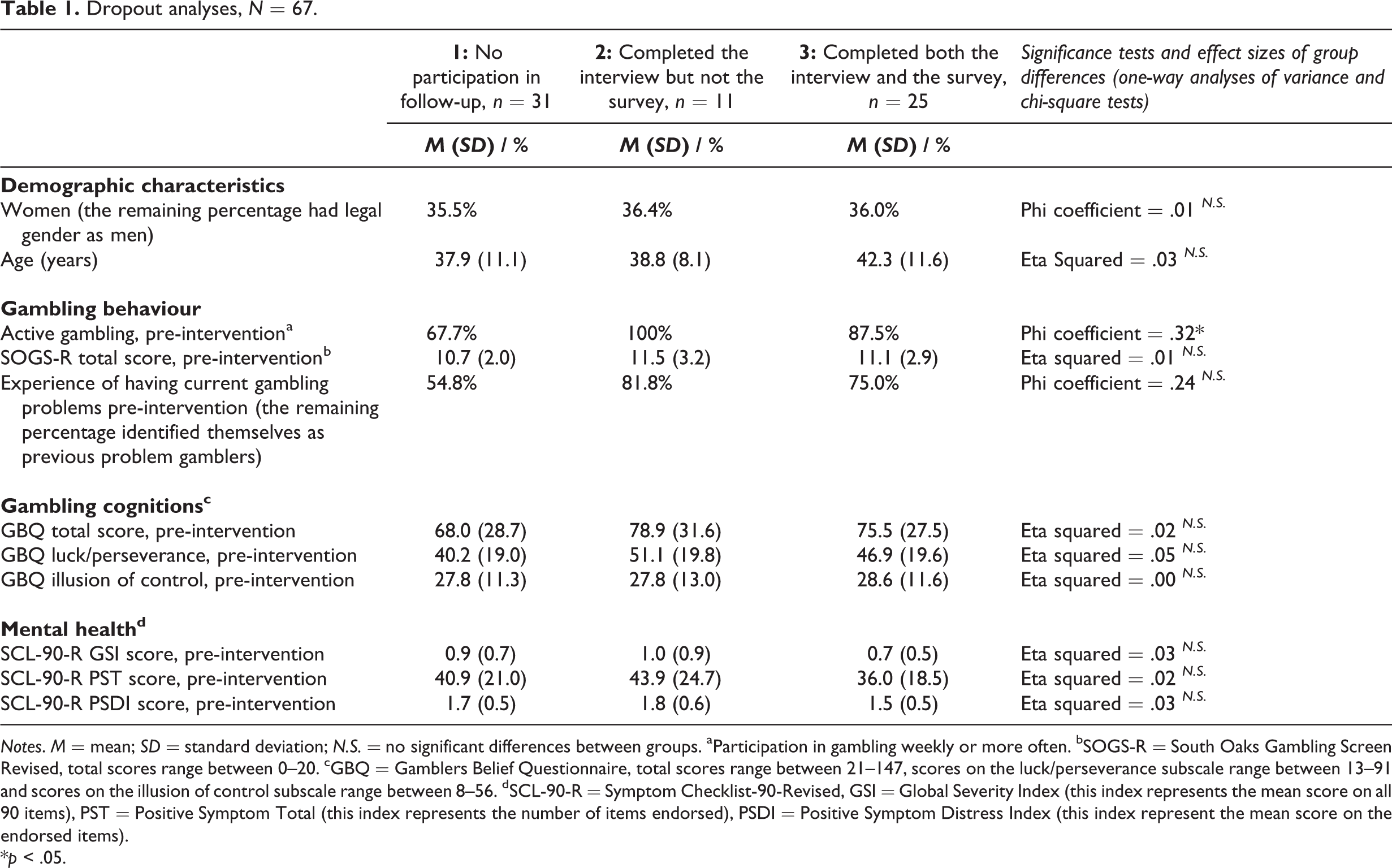
Notes. M = mean; SD = standard deviation; N.S. = no significant differences between groups. aParticipation in gambling weekly or more often. bSOGS-R = South Oaks Gambling Screen Revised, total scores range between 0–20. cGBQ = Gamblers Belief Questionnaire, total scores range between 21–147, scores on the luck/perseverance subscale range between 13–91 and scores on the illusion of control subscale range between 8–56. dSCL-90-R = Symptom Checklist-90-Revised, GSI = Global Severity Index (this index represents the mean score on all 90 items), PST = Positive Symptom Total (this index represents the number of items endorsed), PSDI = Positive Symptom Distress Index (this index represent the mean score on the endorsed items).
*p < .05.
A comparison of the participants’ pre-intervention and follow-up scores on gambling behaviour and a comparison of the participants’ scores on gambling-related cognitions and mental health, pre-intervention to post-intervention and pre-intervention to follow-up are shown in Table 2. The McNemar’s test on active gambling pre-intervention versus follow-up was statistically significant, indicating that fewer participants were actively gambling at follow-up (26.1%) compared to pre-intervention (87.5%). The participants had a significant reduction in total SOGS-R score from pre-intervention to follow-up. The participants’ mean scores on SOGS-R both pre-intervention and at follow-up were above the cut-offs for probable pathological gambling and 100% and 88.0% were in this category pre-intervention and at follow-up, respectively. Further, the McNemar’s test on self-identification as a problem gambler pre-intervention versus follow-up was statistically significant, indicating that fewer participants identified themselves as current problem gamblers at follow-up (20%) compared to pre-intervention (75.0%). The reductions in gambling behaviour had large effect sizes. The participants had a statistically significant reduction in total GBQ score and in scores on the GBQ subscales luck/perseverance and illusion of control from pre-intervention to post-intervention and from pre-intervention to follow-up. The effect sizes of the reductions in gambling-related cognitive distortions were all large. Further, the participants had a significant reduction in the three global indexes of SCL-90-R from pre-intervention to post-intervention and from pre-intervention to follow-up. The effect sizes of the reductions in mental health symptoms were moderate (except for the reduction in the Positive Symptom Total index from pre-intervention to follow-up which had a large effect size).
Changes in gambling behaviour, gambling cognitions and mental health, pre-intervention to post-intervention and follow-up, N = 67.
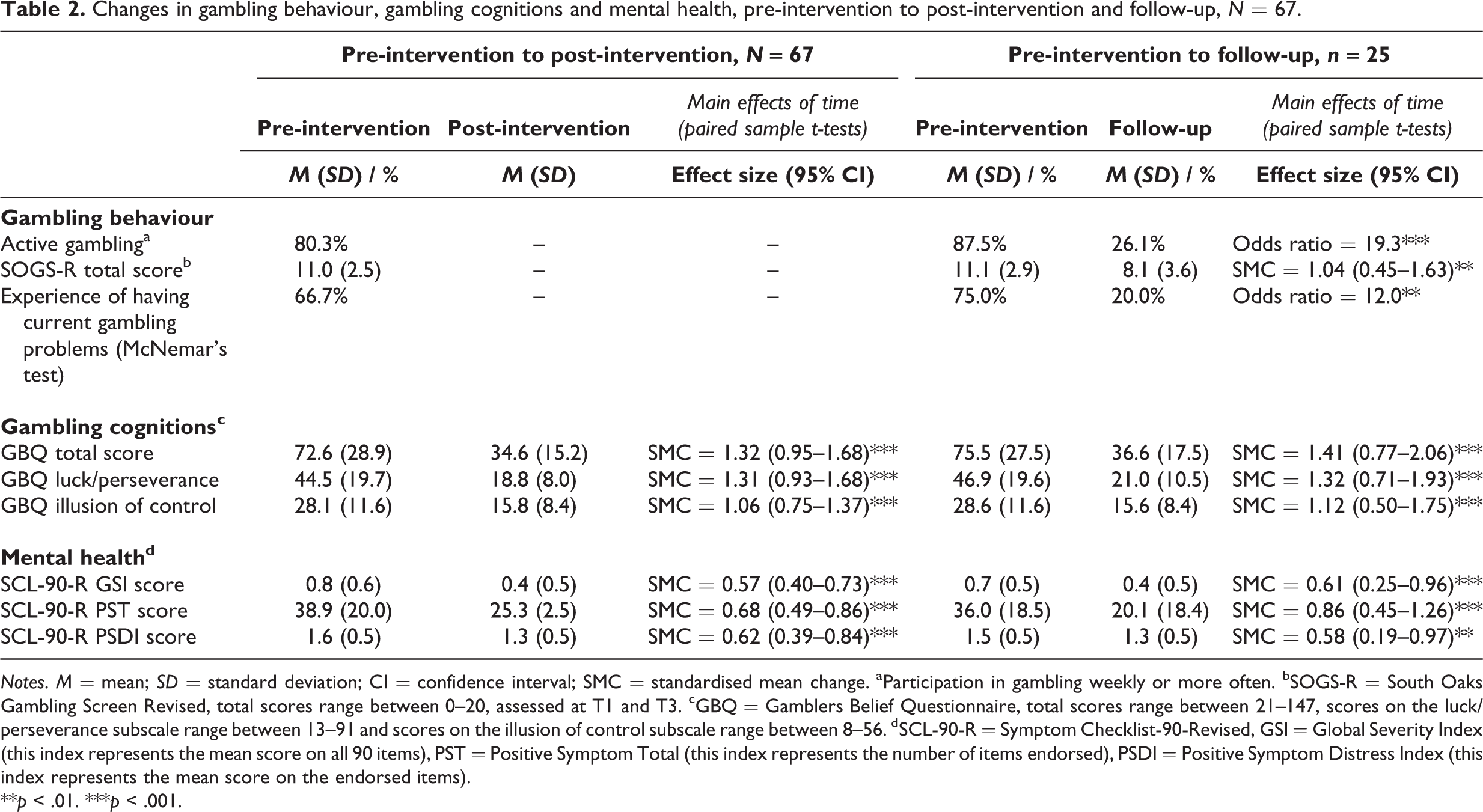
Notes. M = mean; SD = standard deviation; CI = confidence interval; SMC = standardised mean change. aParticipation in gambling weekly or more often. bSOGS-R = South Oaks Gambling Screen Revised, total scores range between 0–20, assessed at T1 and T3. cGBQ = Gamblers Belief Questionnaire, total scores range between 21–147, scores on the luck/perseverance subscale range between 13–91 and scores on the illusion of control subscale range between 8–56. dSCL-90-R = Symptom Checklist-90-Revised, GSI = Global Severity Index (this index represents the mean score on all 90 items), PST = Positive Symptom Total (this index represents the number of items endorsed), PSDI = Positive Symptom Distress Index (this index represents the mean score on the endorsed items).
**p < .01. ***p < .001.
Central tendencies on the questions asked in the follow-up interview are shown in Table 3. Of the 36 participants who completed the follow-up interview, 75.0% considered themselves as recovered from their gambling problems, 13.9% reported to have current gambling problems and 11.1% did not provide any information concerning their current gambling status. A total of 37.1% had received mental health treatment after termination of the intervention programme (i.e., for gambling disorder or other mental disorders) and 17.1% had received mental health treatment for gambling problems, specifically. A total of 20.0% reported difficulties controlling their own involvement in video/online gaming in the time after completing the intervention programme. On a scale from 1 to 10 for how satisfied the participants were with the intervention programme, the mean score was 8.7. In the open-ended feedback question the following themes emerged: (1) Some participants (8.3%) reported that the programme should have been better adjusted to different levels of problem gambling, e.g., that the content of the programme did not have enough relevance for those with previous, but not current, gambling problems; (2) Some participants (19.4%) reported that they felt there was too much paperwork to fill out, in particular before starting the programme; (3) Several participants (30.6%) reported that they appreciated the anonymity and flexibility (in terms of time and place) associated with receiving the intervention via phone, and/or the flexibility the counsellors gave them in terms of the topics discussed during the phone sessions; (4) More than half of the participants (58.3%) highlighted that the sessions with the counsellor were appreciated; (5) Some participants (5.6%) reported that they found the ending of the programme to be too sudden.
Reports from the interviews, n = 36.
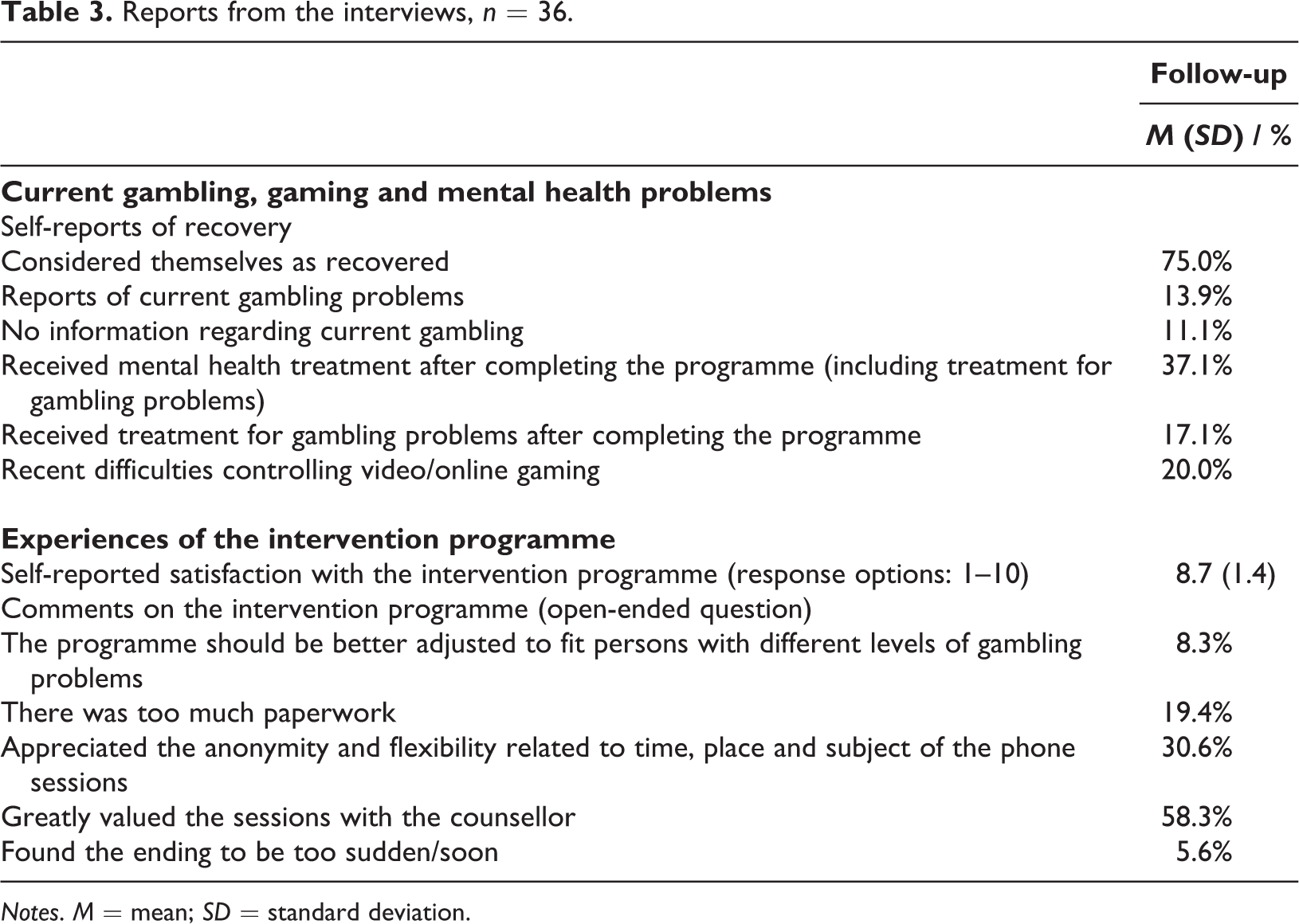
Notes. M = mean; SD = standard deviation.
Discussion
In line with the results from Myrseth et al.’s (2013) study, the results from the current study suggest that the Norwegian remote intervention programme for problem gambling is associated with reduced gambling behaviour, gambling problems, gambling-related cognitive distortions and general symptoms of mental distress. The effect sizes of the reductions in gambling behaviour, gambling problems and gambling-related cognitive distortions were all large, which suggests that the findings have clinical relevance. A novel finding in the current study was that the reductions in gambling behaviour, gambling problems, gambling-related cognitive distortions and symptoms of mental disorders were maintained 6−12 months after completing the programme. Further, the participants reported high satisfaction with the programme: 80.0% of the participants who completed the follow-up survey considered themselves to be recovered from their gambling problem 6−12 months after completing the programme and 73.9% were not actively gambling (i.e., weekly or more often) at this time. The effect size of the reduction in SOGS-R from pre-intervention to follow-up (i.e., standardised mean change of 1.04) is comparable to the mean effect size of intervention outcomes (i.e., Cohen’s d of 1.59) at follow-up found in a large meta-analysis of psychological treatments of pathological gambling (Pallesen et al., 2005). Similar findings were also found in a meta-analysis investigating outcomes (i.e., reduction in gambling problems, frequency of gambling and/or gambling losses) related to participation in face-to-face treatment for problem gambling which found effect sizes (Hedges’ g) ranging from 0.67 to 1.15 (Goslar et al., 2017). Most of the studies included in these meta-analyses investigated more extensive treatment programmes than the remote intervention programme, thus we argue that the comparable effect size of the remote intervention programme, compared with the intervention programmes included in Pallesen et al. (2005) and Goslar et al. (2017), suggest that the remote programme is quite cost-effective compared to more traditional treatment programmes. The Norwegian remote intervention programme for problem gambling is, however, counsellor intensive compared to some other types of interventions. Quilty et al. (2019) conducted a meta-analysis on outcomes related to participation in individual, face-to-face, brief interventions for problem gambling (≤ 3 sessions) and found short-term reductions in gambling behaviour (including frequency of gambling and the amount of money spent gambling) to have a Hedges’ g of 0.19 (p < .05), albeit the long-term reductions (g = 0.17, p > .05) were not significant. Further, in contrast to the current findings, Quilty et al. (2019) did not find significant short- (g = 0.13, p > .05) or long-term (g = 0.20, p > .05) reductions in gambling problems. Goslar et al. (2017) investigated outcomes (i.e., reduction in gambling problems, frequency of gambling and/or gambling losses) related to participation in another type of brief intervention, self-guided treatments, which include limited counsellor contact, in their meta-analysis, and found Hedges’ g ranging from 0.12 to 0.30. The reduction in gambling behaviour (i.e., OR = 19.3) and gambling problems (i.e., standardised mean change of 1.04) in the current study were considerably larger compared to the effect sizes found in these meta-analyses of brief interventions. Hence, the Norwegian remote intervention programme for problem gambling, although more costly, may be more effective than brief interventions in reducing gambling and gambling problems. It is, however, important to stress that the studies included in Quilty et al. (2019)’s and Goslar et al. (2017) meta-analyses were methodologically robust compared to the current study, including and comparing outcomes to the outcomes of a control group. As such the current findings are not directly comparable to the findings reported by Quilty et al. (2019) and Goslar et al. (2017).
A finding that may question the cost-effectiveness of the programme was the large proportion of the participants who had sought additional mental health treatment after completing the programme (37.1% in general, and 17.1% for gambling problems specifically). The proportion who reported to have sought additional treatment for their gambling problems was considerably larger in this study than the 10% life-time prevalence of treatment-seeking among pathological gamblers found in a national US survey (Slutske, 2006; Slutske et al., 2009). The finding that a large proportion of participants had sought additional treatment should be regarded as a positive outcome as many scholars have expressed concerns regarding the low percentage of problem/pathological gamblers seeking treatment (Slutske, 2006; Suurvali et al., 2012). One could thus view the large percentage who had sought additional treatment as a positive outcome, suggesting that the remote intervention programme may lower the threshold for users to seek more resource-intensive treatment for their gambling problems or other mental health problems if needed.
The observed high SOGS-R score at the time of the follow-up and the large proportion of participants who reported experiencing difficulties controlling their gaming may call into question the benefits of the intervention programme. The participants’ mean SOGS-R scores at follow-up were above the cut-offs for probable pathological gambler and 88.0% of the participants had SOGS-R scores above this cut-off at follow-up. Some of the participants’ reports in SOGS-R were inconsistent; for instance, some reported that they did not gamble, but still, they reported symptoms of pathological gambling in the past three months. Hence, it is possible to speculate on whether the high mean SOGS-R score at the follow-up assessment may be partly explained by the participants answering SOGS-R based on their life-time experiences, rather than their experiences in the past three months as instructed. The high SOGS-R scores may also in part be explained by some of the participants being in a state of partial rather than full recovery, as recovery from gambling problems is likely to reflect a multifaceted and non-linear process (Nower & Blaszczynski, 2008). Further, 20.0% of the participants reported difficulties controlling their video/online gaming (i.e., a symptom of problems associated with gaming), which suggest that problems associated with gaming may be more common in this group compared to in the general Norwegian population – where 3.3% has been estimated to be problem gamers (Pallesen et al., 2016). An association between problem gaming and gambling has also been reported in previous studies among adolescents and young adults (Parker et al., 2008; Walther et al., 2012). Further, an association between problem gaming and gambling was also found in a longitudinal study among the Norwegian general population (Molde et al., 2019). The findings in Molde et al.’s (2019) study suggested that problem gaming predicts problem gambling and not vice versa. The study design of the present investigation does not allow for inferences about the causal relationship between gambling and problems associated with gaming. It is, however, possible that video/online games served as a “substitute addiction” for some of the participants and hence that the intervention programme did not treat “addiction” per se (Sussman & Black, 2008). Based on the findings in Molde et al.’s (2019) study, one may assume that the participants who may have “replaced” gaming with gambling had previous experiences with gaming. If problem gamblers who successfully abstain from gambling develop problems associated with gaming this may be reason for concern. However, according to the replacement theory of addiction, the substitute “addiction” – in this case gaming – will usually be less extensive and harmful than the original addiction (Sussman & Black, 2008). Thus, even if some of the problem gamblers in the current study replaced gambling with gaming, problems related to the latter are likely to be less severe compared to the former.
In summary, the current results suggest that a remote intervention programme might be associated with beneficial outcomes for people with gambling problems and that participation in the programme may increase the likelihood of seeking additional treatment if needed.
Recommendations
Some recommendations regarding the Norwegian remote intervention programme for problem gambling and other remote intervention programmes for problem gambling seem warranted based on the current and previous findings. The current study precludes conclusions regarding which components should be included in such programmes. The participants’ reports suggested, however, that the sessions with the counsellor comprised an important component. As highlighted by others, contact with a counsellor may boost compliance with the intervention and reduce attrition, and intervention programmes may hence benefit from including such contact (Hodgins et al., 2019). Further, many participants reported appreciating hallmarks of having sessions over the phone compared to face-to-face sessions (e.g., not having to leave work for sessions), hence sessions via phone may represent an important component in remote intervention programmes’ potential effectiveness. However, studies comparing different forms of remote intervention programmes are needed in order to conclude on this issue.
One of the rationales for conducting the current study was the rapid and constant changes in the gambling environment substantiating a need for updated evaluations of the programme. The current findings suggest that participation in the Norwegian remote intervention programme for problem gambling is still associated with positive outcomes. Some suggestions for how the programme could be developed to meet new needs could, however, be made. One hallmark of the current gambling environment is the abundance of targeted and rather aggressive gambling marketing (Newall et al., 2019). Gambling marketing may affect gambling behaviour and both researchers and problem gamblers are concerned that marketing, especially in the form of bonuses and free spins, may hamper problem gamblers’ recovery (Newall et al., 2019). Thus, the Norwegian remote intervention programme for problem gambling and other intervention and treatment programmes may benefit from addressing coping with gambling marketing as a part of the programmes. Another change in the gambling environment is the blurring of the boundary between gambling and gaming, where online/video games often include elements of gambling and vice versa (Teichert et al., 2017). The current finding of 20.0% of the participants reporting difficulties controlling their video/online gaming, also supports the notion of an overlap between gaming and gambling. Hence, treatment and intervention programmes for problem gambling might be improved by assessing and addressing gaming. Based on the replacement theory of addiction, one may assume that intervention/treatment programmes for problem gambling may benefit from addressing the risk of replacement addictions or addiction-like conditions in general (i.e., not limited to gaming) (Sussman & Black, 2008). This can be implemented, for instance, by adding a psychoeducational component of replacement theory of addiction in a relapse prevention session. The feedback from the participants in the current study, where 8.3% reported that the programme should have been better adjusted to different levels of problem gambling and 5.6% reported that they found the ending of the programme too sudden, further suggests that the Norwegian remote intervention programme for problem gambling could benefit from including a stronger emphasis on relapse prevention in general and a more individual tailored approach.
Further, the current findings where almost all participants were in the probable pathological gambling group at pre-intervention and follow-up, suggest that the SOGS-R may not be an ideal measure for assessing treatment outcomes. Hence, the Norwegian remote intervention programme for problem gambling may consider replacing the SOGS-R with another instrument. One instrument that might be more suitable for clinical use is the Problem Gambling Severity Index (PGSI; Ferris & Wynne, 2001). The PGSI may be more suitable than the SOGS-R because it has fewer questions which may make it easier for the respondents to remember that they are instructed to answer based on their experiences the past months rather than their life-time experiences. Another strength of the PGSI is that each item has several response options (i.e., never; sometimes; most of the time; almost always) while several of the items in the SOGS-R have dichotomous response options (i.e., yes; no). Several response options allow for more precise nuancing and may make it easier to detect change. The Norwegian remote intervention programme for problem gambling should also include an updated measure of actual gambling participation where a measure that was developed for the Norwegian gambling market for use in population studies is recommended (Pallesen et al., 2020). Finally, an assessment of harms associated with gambling should be included, for instance the Short Gambling Harm Screen (SGHS; Browne et al., 2018). Knowledge of the type of harm the participant experiences could improve the tailoring of the programme to each participant’s individual needs, for instance by guiding what one could focus on in discussions with participants who do not gamble or have symptoms of problem gambling, but who struggle with harms from previous gambling.
Limitations
The current study has several limitations that should be highlighted. Importantly, this study had no control group. It is therefore not possible to conclude as to whether the observed effects were attributable to the intervention, or whether they were a result of regression towards the mean or spontaneous recovery. The latter is assumed to be quite common among problems gamblers (although relapse rates are also high), e.g., in one study approximately two thirds of all problem gamblers (both problem gamblers who had and who had not received treatment) were not in this category one year later (Abbott, Romild, & Volberg, 2018; Abbott et al., 2004; Black et al., 2017; Hodgins & El-Guebaly, 2000; McMillen & Wenzel, 2006; Slutske et al., 2009). Further, as only those who had completed the intervention programme were included, we do not know the drop-out rate or what characterised the dropouts. It is possible that those who dropped out had other characteristics than those who completed the intervention, and that this may affect the generalisability of our findings. Myrseth et al. (2013) who investigated the same programme as in the current study, included some information regarding drop-out rates and characteristics associated with drop-out. The authors found quite high drop-out rates, where 37.4% of the participants dropped out before initiating intervention and 17.9% dropped out after completing just parts of the intervention programme. These high drop-out rates might suggest that such interventions are not suitable for all individuals with gambling problems. Myrseth et al. (2013) further compared those who only completed parts of the intervention to those who completed the whole programme and found no differences in terms of gender, mental health or severity of gambling problems between the two groups. However, the non-completers were younger, had fewer gambling-related cognitive distortions and were more likely to play poker compared to the completers, which suggests that steps to tailor the intervention to these groups might be expedient (Myrseth et al., 2013). The low sample size is another limitation of the current study. The sample size was too low to fulfil the required number of cases per cell for multivariate analyses, which is why we had to perform statistical analyses on one variable at a time. Analysing data on one variable at a time increases the number of statistical tests conducted, which in turn increases the likelihood of type I errors. The low sample size also impedes the assessment of differences between those who participated in the follow-up and those who did not, thus hampering conclusions regarding the representativeness of the results.
The measurements used also involve some limitations. The validity of the SOGS-R may have been affected by some participants answering based on their previous experiences with gambling rather than their experiences in the past three months as instructed. We suspect that this might have been an issue based on some participants providing quite contradictory answers and the counsellors’ impression that some participants answered based on their previous experiences with gambling rather than their experiences in the past three months. For GBQ, it should be noted, that the measure may not optimally reflect gambling-related cognitive distortions among gamblers playing skill games. In particular, the subfacet illusion of control may be suboptimal for gamblers playing skill games (e.g., poker) as they will have some control over the outcome of the game, making it imprecise to term perceptions of control as cognitive distortions. Further, the participants’ responses may have been affected by different response biases, such as social desirability bias and demand characteristics, as the participants were interviewed by the counsellors in the intervention (not the same counsellor who provided the intervention for them) and knew the purpose of the study (i.e., to evaluate the intervention), thus the participants may not have felt anonymous and some may have been motivated to please the counsellors by exaggerating treatment benefits (Edwards, 1953; Orne, 1962).
Conclusions
The remote intervention programme for problem gambling appears to have benefits in terms of reducing gambling and alleviating gambling problems, gambling-related cognitive distortions and symptoms of mental disorders, in both the short and long term. Further, another positive outcome of participation appears to be a lowered threshold for seeking additional treatment at a later stage if needed. The participants’ reports suggested that remote interventions for gambling problems may benefit from including phone contact with a counsellor. However, our findings should be considered in view of some important limitations, including the lack of a control group, the small sample size, and the fact that the respondents were interviewed by counsellors associated with the intervention programme. Future studies should evaluate the effect of the remote intervention programme for problem gambling in a randomised controlled trial and compare the intervention with treatment as usual or a wait-list control condition.
Footnotes
Acknowledgements
We want to thank the participants in the intervention programme for contributing with data and permitting these data to be used for research.
Declaration of conflicting interests
The authors declared following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Mette Mohn and Trond Aspeland are both counsellors in the remote intervention programme for problem gambling investigated in the current study.
Funding
The authors have declared the following financial support for the research, authorship, and/or publication of this article: The research reported in this publication was funded by the Norwegian Directorate of Health. The Norwegian Directorate of Health approved the research questions but was not involved in any other stages of the current research (e.g., determining research design, analyses or write-up).