
Abstract
Aim:
Studies on recovery from alcohol and other drugs (AOD) among young adults are scarce. In the present study, young adults, previously interviewed with a focus on their recovery process shortly after they completed treatment, were re-interviewed five years later focusing on their recovery process during the last five years in relation to their former AOD problems, other problems and processes of change.
Methods:
Twenty-one young adults were interviewed: 16 women and five men aged between 25 and 33 years. After transcribing the interviews, the material was analysed thematically.
Results:
Three overall themes emerged: previous problems, mental illness and the search for identity. The results were discussed in relation to recovery capital, primarily focusing on human and social capital. The results indicate that the group in focus often needs professional support for mental health issues in order to reach a stable recovery.
Conclusions:
Since the problems described were heterogeneous, this client group might benefit from individual treatment and extended support after treatment. Further, the results indicate that the established period of five years for a stable recovery might need to be extended for young adults.
The concept of “recovery” is an established term used to describe positive processes of change concerning problems related to alcohol and other drugs (AOD) (Witbrodt, Kaskutas, & Grella, 2015). The recovery process stretches over a long period of time and it is suggested that stable recovery is achieved after five years at the earliest (Hibbert & Best, 2011). There are many pathways to recovery (White & Kurtz, 2006) and variations of important factors have been found between different timespans during the recovery process (Laudet & White, 2010; Litt, Kadden, Kabela-Cormier, & Petry, 2009; Best et al., 2012; Best, Groshkova, Sadler, Day, & White, 2011) and between groups (Ammon, Bond, Matzger, & Weisner, 2008; Orford et al., 2006; Skogens & von Greiff, 2014; Timko, Finney, & Moos, 2005; von Greiff & Skogens, 2017). However, studies on the recovery process in adolescents and young adults are scarce (Hennessy, 2017; Hennessy, Cristello, & Kelly, 2019).
In the present study, young adults, previously interviewed in Swedish studies (Skogens, von Greiff, & Esch Ekström, 2017; von Greiff & Skogens, 2017) focusing on recovery processes shortly after they completed treatment for AOD problems, were re-interviewed five years later. The research questions for the present article were on how their recovery process during the last five years was related to their former AOD problems, to other problems and to processes of change. 1 How their specific problems relate to other areas and challenges that characterise this age group in general has been an issue of specific interest.
Recovery and recovery capital
In research on treatment for AOD problems, the concept of recovery is well established and it has been defined by Betty Ford Institute as “voluntary maintained lifestyle characterized by sobriety, personal health, and citizenship” (The Betty Ford Institute Consensus Panel, 2007, p. 222). Although there are no empirically established timeframes for describing stability of recovery from AOD problems, three phases are identified: early sobriety (1–12 months), sustained recovery (1–5 years) and stable recovery (more than five years) (The Betty Ford Consensus Panel and Consultants, 2010; see also Hibbert & Best, 2011). Related to this, the concept of recovery capital (RC) has been used to provide professionals with in-depth knowledge to assist individuals in their process of change (Best et al., 2010; Davidson & White, 2007). RC was introduced by Cloud and Granfield (1999, 2008) inspired by theories in social science on certain preconditions relating to resources and social structures (cf. Bourdieu & Wacquant, 1992; Coleman, 1990; Teachman, Paasch, & Carver, 1997). Along with the exploration of recovery capital in research on recovery from AOD problems, variations of this original model have been developed (Hennessy, 2017) albeit with consistent main properties and domains but varying in labelling and fine-tuning. RC, according to Cloud and Granfield’s model, consists of social capital (such as a stable social network offering support and trust as well as demands), physical capital (financial and material resources), human capital (knowledge and skills, education, physical and mental health) and cultural capital (norms and values). A central premise for the use of recovery capital is that it is not static but constitutes a changeable description of a person’s ability to initiate and maintain a recovery process which implies that individuals are able to change their recovery capital (with or without professional assistance). Since RC includes personal as well as contextual resources, it is considered useful for the analysis of preconditions and possibilities for positive change.
Factors that have been suggested as strengthening RC during a change process are related to an improved and deepened quality of life and include, for example, a sober social network (Litt et al., 2009), engagement in meaningful activities that reduce the risk of relapse (Best et al., 2012) and the development of a healthy and productive life (White, 2007). Stable social relationships are important for improving mental health and quality of life (Best et al., 2011). Studies on clients treated for AOD problems suggest that those with a marginalised social position need more time for recovery and the strengthening of RC in order to maintain recovery compared to people with a more integrated social position (Skogens & von Greiff, 2014; von Greiff & Skogens, 2017). Further, research on clients with co-occurring AOD and mental health problems concludes that important factors for the recovery process are leaving the identity of being institutionalised behind, and gaining agency in life (Skogens, von Greiff, & Topor, 2018).
Adulthood and young adults with psychosocial problems
For young adults recovering from AOD problems, the process of change often also concerns the process of moving from adolescence to adulthood. This “youth transition” may offer a time of hope and positive change, but may also create exclusion and marginalisation (Giddens, 1997; Masten et al., 2004), and in a more individual-based and untraditional society, the paths for transition to adulthood are less linear and more fragmented. Some examples of this are more years spent in education systems, more flexible and changing working conditions, later parenthood and marriage. Arnett (2005) uses the term emerging adulthood to describe the development period characterised by identity uncertainty and exploration. However, the term has been criticised for ignoring variations, for example, related to social class (cf. Côté, 2014). Recently, another concept – young adults, based on studies on people well into their thirties – has been launched to describe the phase between adolescence and adulthood that is characterised by social ambiguity and oscillation between dependence and independence (Magaraggia & Benasso, 2019).
A strong body of research shows that, in relation to other young adults, those leaving care have limited possibilities for this oscillation between dependence and independence (Furlong, Cartmel, Biggart, Sweeting, & West, 2003; Höjer & Sjöblom, 2009; Osgood, Foster, & Courtney, 2010) which leads to a shorter and more compressed transition compared to their peers (Höjer & Sjöblom, 2014; Stein, 2012). Also, it has been reported that this group tends to have complex problems and that they struggle with problems such as poor mental health, poor school performance and crime more often than their peers (cf. Berlin, Vinnerljung, & Hjern, 2011; Courtney & Dworsky, 2006; Vinnerljung & Sallnäs, 2008).
Research on RC has primarily focused on recovery among adults. However, studies focusing on young adults imply that RC might have a somewhat different meaning and implications for them (Elswick, 2017; Hennessy et al., 2019; Hennessy, Glaude, & Finch 2017; Mawson, Best, Dingle, & Lubman, 2015). An Australian study stresses that low social and human capital (for example, level of education and health) among young adults with AOD problems reduces the possibilities for recovery (Mawson et al., 2015). However, it has also been suggested that high social capital, such as sober networks, may reduce the negative effects of low human capital and, further, that the social network can be supportive or work as an incentive for change (to encourage the young adult to leave or disassociate him or herself from an old social network). During adolescence, social capital tends to be focused on peers (Bassani, 2007) and this is accentuated for those with problematic upbringing conditions. However, in line with RC for adults, employment and/or education (Laudet & White, 2010) are also highlighted as being important (Skogens et al., 2017).
Methods
In two Swedish projects on recovery from AOD problems, 32 young adults were interviewed approximately six months after finishing treatment (Skogens et al., 2017; von Greiff & Skogens, 2017). The inclusion criteria were that the interviewees should: (a) have undergone a treatment intervention; (b) be at the end of or have recently completed a post-treatment intervention; and (c) be judged by a professional to be in a positive process of change regarding the AOD problems they had received treatment for. The intention was to recruit interviewees with some distance from the treatment in order to be able to reflect on their process of change. The focus of the first interview was what the clients themselves highlighted as important for initiating and maintaining positive change, and overall themes in the different phases were the importance of internal, social and treatment-related factors. The recruitment of interviewees was conducted through contact with treatment units (outpatient and inpatient) in seven Swedish city areas.
In the present study, the young adults were contacted again for a new interview five years later. When designing the study, one of the worries were that we would not get data from the interview persons (IPs), even if we had written consents to contact them again. Thus, in order to increase the IPs’ possibilities to take part in the study, it was decided to keep the interviews limited in time and, further, to offer interviews by telephone. This turned out to be important since many IPs were busy, for example, with work and/or small children. The IPs were approached via telephone and asked if they were willing to be interviewed again. Thus, when the actual interview took place, the IP was prepared for the subject of the interview (i.e., how their recovery process had proceeded during the last five years). Twenty-one clients were re-interviewed with the overall aim to study the stable recovery of young adults. Of those not interviewed, nine were impossible to reach via the contact information available (the five-year old telephone number did not work and no new number was found in internet searches) and two individuals declined to participate. The majority of the interviews in the follow-up study were conducted by telephone and lasted about 30 minutes. The interviews were recorded and transcribed verbatim within 48 hours. Both authors were responsible for the complete process of collecting and analysing data at the initial and the follow-up study. In order to follow individuals between the first and second interviews, the interview guide was thematised in the same way, i.e., internal, social and treatment-related factors. The interviews began with the interviewer giving a brief summary of how the IP had described his/her process of change the last time. With this as a starting point, the IP was asked to describe the last five years in terms of both possible so-called relapses and the retention and/or resumption of positive change. The interview guide also dealt with questions on treatment contacts during the follow-up period (frequency, extent and type), the view of one’s own and others’ alcohol consumption, and factors that were important to continuing or resuming a positive change.
Analysis
After transcribing the interviews, the material was analysed thematically (Braun & Clarke, 2006) by coding the interview passages according to what was brought up. After re-listening to the interviews and scrutinising transcripts, the material was categorised and summarised by selecting relevant parts from each transcript. By iteratively analysing and compiling these in an increasingly condensed form, themes were created at an aggregated level, following a process of going back and forth between transcripts and the emerging themes as described by Braun and Clarke (2006). NVivo, a software package for qualitative data analysis, was used to validate the condensed descriptions and thematisations made manually by returning to the transcripts and comparing highlighted sentences at the level of the individual with general aggregated descriptions.
Quotations are followed by numbers referring to a specific interviewee.
Results
Description of the IP n = 21
Sixteen women and five men were interviewed five years after the first interview. The majority described their former AOD problems in terms of polydrug use (12 IPs), a third reported drugs as the main problem (7 IPs) while two IPs reported alcohol abuse as their main problem. 2 Thirteen IPs had undergone individual treatment, while eight had undergone group treatment (strictly following or based on the 12-step philosophy). Although all the clients had undergone treatment for AOD problems, most of them reported several and often complex problems including, for example, crime and destructive relations. As shown in Table 1, below, all IPs brought up mental health problems, but most often only in passing. However, these problems can be described as rather severe: diagnosed ADHD/ADD/PTSD (9), suicide attempts (6), psychosis (3), anxiety (6), and an eating disorder (1).
Mental health problems, living situation and occupation at first interview and at follow-up (N = 21).
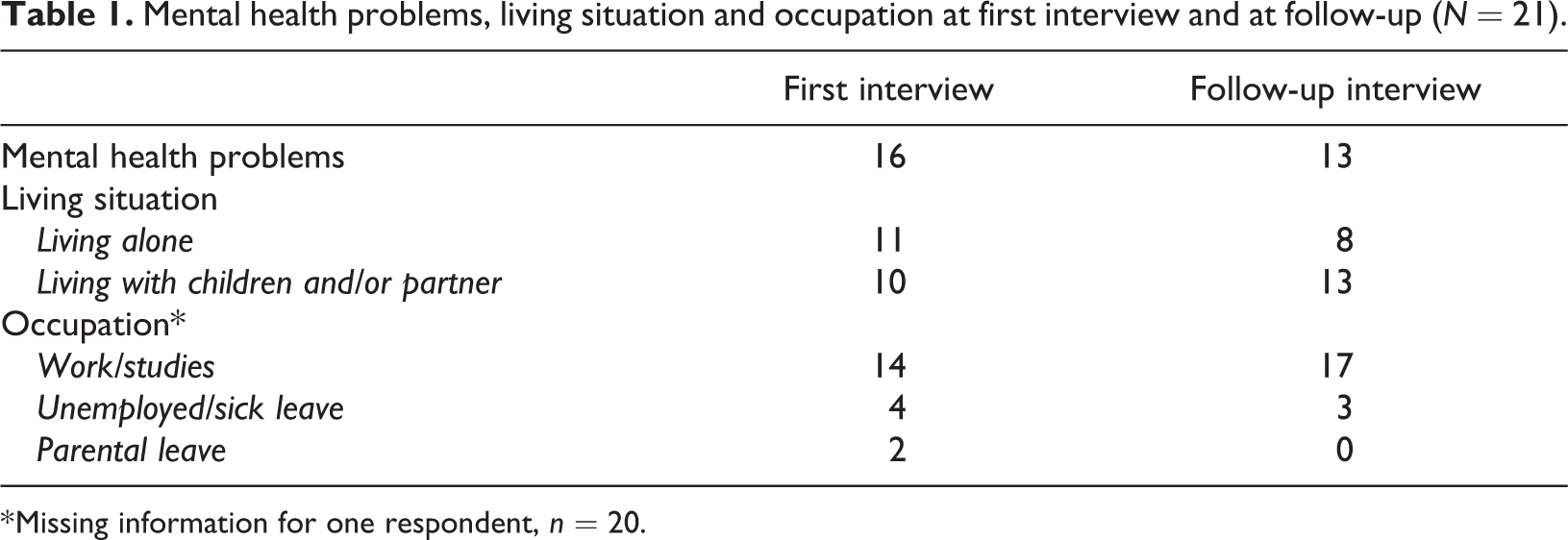
* Missing information for one respondent, n = 20.
At follow-up, the IPs were aged between 25 and 33 years (mean age 29). A majority (13 IPs) described that they used alcohol in a controlled way and just under a third (6 IPs) were sober (half of whom had been so throughout the whole follow-up period). One IP described ongoing drug abuse and another described recurring periods of overconsumption of alcohol but did not define it as a problem since it did not affect the rest of his life (such as work). While the majority of the women (12/16) reported living with partners and/or children at follow-up, four out of five men were single. The majority of the IPs did not bring up contact with parents or siblings. In general, the IPs described their social network, including friends, as limited.
How IPs relate to previous problems
When asked to describe the past five years in relation to their recovery process, not everyone shared the perception that they used to have AOD problems – although all the IPs had met the inclusion criteria to have undergone treatment for AOD problems. Some said that there were others who had expressed concerns about their “abuse”. Other IPs admitted that they had used drugs but that their alcohol use had never been a problem (thus making a clear distinction between alcohol and drugs) and therefore did not see their current use of alcohol as an issue. However, apart from the one IP who described recurring bouts of overconsumption, it was generally a matter of small amounts of alcohol and only on a few occasions. I use alcohol but to a very limited extent. I was very careful to begin with because you don’t know whether it will trigger something. But for me alcohol doesn’t have that effect so I can have a glass now and then. But that happens maybe twice a year, I don’t get drunk. (IP9) I might smoke on occasion, but then I do it as an alternative to going to the pub, [I] stay at home with a friend, we smoke and chat and bake a chocolate cake. (IP10) A part of me says that this is the first step in a relapse process, but my gut feeling says that it’s ok, because I trust myself. I don’t think it’s as clearly black and white as it was ingrained in me during the 12-step programme. (IP1) I did my treatment, which was my first, and since then I’ve stayed sober and drug free. (IP3, who used to inject drugs) When I stopped using what was classified as drugs, I was over 20 and was allowed to drink alcohol. Since I didn’t view this [alcohol] as a drug, I drank during the first few months of my sober phase. But I stopped doing that because I realised that the so-called addictive behaviour follows every substance that comes my way. (IP12) I used to have problems with food and stuff…// for me there really isn’t that big a difference between an eating disorder and an addiction and…these are different types of self-harming behaviour.// I’ve had a lot of treatment. It started with the 12 steps, followed by a form of eating disorder treatment. // Then I started another course of treatment that was crucial to me, a kind of family therapy in a group. (IP4) I had a lot of anxiety so after a couple of days I felt that this was no good, I had to get sober and take control of everything, this really was no good. (IP18) I survive by committing crimes, and the addiction helps me get through the day. (IP17)
Mental health problems
More than half (13/21) stated that they had suffered from mental health problems during the follow-up period. There were major variations in severity from “common” concerns and stress (in particular associated with the process of transition to adulthood) to various psychiatric diagnoses (depression, ADHD, PTSD and eating disorders). While ADHD was relatively common, other diagnoses were mentioned by individual IPs. Some had had continuous contact with psychiatrists and/or had undergone therapy with a psychologist, while others had had occasional or sporadic contact. The problems for which IPs sought professional help were not described in relation to their previous AOD problems (i.e., not caused by the AOD problems) but were described as something separate or an underlying factor. Then I also got psychiatric care, after having dealt with what was the addictive disease in the programme, other problems were discovered. (IP11) …they [professionals in AOD treatment] didn’t take into account the effects of how you felt when you became drug free and sober. You often have other problems; most people who do drugs have some form of disability. You didn’t really get any help for that. There was no one you could talk to about it. That’s why I have contacted professional psychotherapists and experts in psychiatry. //…[I have] childhood trauma, there’s quite a lot of grief. (IP6) …I’ve been given a lot of tools to handle my everyday life and stress and to not put so much pressure on myself. (IP7) Throughout my journey I’ve had a lot of support from therapists and psychologists, until a year ago. It’s been a huge…, a support in this process. There have been different people who have helped me with different things. That they have been outside the community has helped me in that process…(IP5)
Professional contacts were also mentioned when ADHD was being diagnosed, with regard to medication for cravings and as examples of shorter outpatient contacts during the follow-up period.
Searching for identity and the process of becoming an adult
Identity seeking ran as a silver thread through several descriptions – what was mainly emphasised was that IPs did not want to identify themselves as drug addicts and/or as something negative. Professional contacts and the context conveyed in treatment became central for some IPs in this process. It was not just about the view of abuse conveyed during treatment, but rather that this view influenced their entire identity. [I] was lost then – the programme and the treatment had given me that, my life was like a blank slate, I knew nothing about how to behave, thought everything was thanks to the 12-step programme, but now I feel it was thanks to me, that I struggled so hard. (IP1) …you identify yourself so much, all the behaviours are because you’re an alcoholic, for example, and it’s something negative and I don’t want to identify myself with something negative. (IP2) [There] are other ways than the dogmatism that exists within NA and it was a process in itself because five years ago my social contacts were mostly within NA. It was like losing a large part of your family when you chose to leave. //…I started to feel that I wasn’t able to say that I was addicted, I had been addicted but today I’m just not that. //…a long process since I stopped [going to NA meetings] and when I started drinking again. [Authors’ note: drinking in a controlled and limited way] (IP5) I’ve now got a lot of tools so I can handle my everyday life and stress and not put so much pressure on myself. (IP7) Sure, I can provide for myself now, but the future is very uncertain. How can I enter the labour market? I’m almost thirty, have never had a permanent job, have no education after upper secondary school. I feel quite a lot of stress about how I will manage in society because I have the difficulties I have. (IP6) …it’s a bit more stressful, existential angst and so on; others [peers] are having children, they are studying and so on. What should I do? But compared to five years ago, I feel better within myself, my basic outlook on life is better. (IP10) It feels like I haven’t accomplished as much as I wanted, or want. It’s probably one of the reasons why I have started to get organised and to study. I don’t even have upper secondary school qualifications, I have to start there. It’s really things like these, it makes you feel fairly…that you’re lagging behind, that you’ve missed out on a lot. You should finish upper secondary school when you’re 18–19 years old, I’m over 30 now. It feels a bit stressful, that I have to achieve all the time. (IP14)
Discussion
To start with, it is important to mention that there are always exceptions to the general patterns that will be described and discussed below. For example, there were individual IPs who described their lives very much in the same way as they had in the interview five years ago, as a quiet life without any particular obstacles or shifts. However, in line with previous research describing recovery as a long process (Best et al., 2011, 2012; Laudet & White, 2010), the dominant pattern was an ongoing process of both recovery and change throughout the last five years.
The IPs’ descriptions of how and in which areas they had worked with strengthening their RC during the follow-up period can be linked to the complex problems that often characterise the client group in focus (Berlin et al., 2011; Courtney & Dworsky, 2006; Vinnerljung & Sallnäs, 2008). This implies that the initial treatment for AOD problems was mainly the start of a recovery process and that the strengthening of RC needed to continue in order to maintain positive changes and reach a stable recovery. As in previous research on young adults with AOD problems (Mawson et al., 2015), the IPs mainly described that they needed to strengthen their human capital, and most often this concerned their mental health but also their education. Strengthening their social capital was also crucial; this was, for example, evident in the importance they placed in establishing a family of their own at an early age. This does not imply that other areas were less important, rather that other areas had been relatively stable for the vast majority of the IPs. During the interview five years ago, the IPs reported a relatively stable – although sometimes fragile – base concerning employment or other financial aspects and housing. In most cases, these needs were attended to by their treatment facility or social service unit. The importance of having these basic needs met as a prerequisite for being able to deal with other issues was identified more than half a century ago in Maslow’s hierarchy of needs (Maslow, 1954), and has also been described in particular for marginalised groups with AOD problems (Skogens & von Greiff, 2014; Skogens et al., 2018).
It seems that the results are in line with previous research stressing that compared with young people in general, the moving out process, i.e., moving into your own home, is short and occurs at a younger age for young adults leaving care (Höjer & Sjöblom, 2014; Stein, 2012). On the other hand, the need to strengthen human capital, such as mental health and education, as actualised during the follow-up period, can be interpreted as a somewhat delayed transition to adulthood.
As mentioned above, a central theme for the IPs during the follow-up period was strengthening their mental health, and the majority had done that with support from mental health professionals such as psychiatrics and therapists (cf. White, 2007). This strengthening was not predominantly described as leaving mental health problems behind them but, rather, that the IPs had got to know themselves better, learnt to handle issues in this area and thus become more accepting of themselves. It is worth noting that the mental health problems that the IPs sought professional help for were not described in relation to their AOD problems but as problems separated from these and/or underlying the AOD problems. When the need for professional support was described, this did not only concern severe mental health problems. Although a majority of the IPs described a history of severe mental health problems in the first interview, what was often stressed was a need for ordinary support in life in terms of guidance and support in decisions and about worries. Thus, this can be related to the kind of support that is often fulfilled through social capital, i.e., family and friends. During the follow-up, IPs referred to social capital in relation to establishing a family of their own. However, even though a majority had a partner and/or children, this did not provide sufficient support to strengthen their human capital. This might be related to the general descriptions of IPs regarding the lack of a stable relationship with their birth family. This implies that the importance of professionals empowering individuals as a prerequisite for recovery generally highlighted in research on recovery (cf. Best el al., 2010; Davidson & White, 2007) seems to be even more significant in this group and, moreover, crucial over a long period of time (cf. Bengtsson, Sjöblom, & Öberg, 2018; Wade & Dixon, 2006).
All those who did not define themselves as abstinent, but at the same time stated that they definitely did not have any problems with alcohol, emphasised that their consumption was limited. They rather emphasised the possibility of having a glass of wine, not having to take a completely sober attitude in contexts where alcohol was used, and not having to identify themselves as abstainers. In turn, this meant that the social capital of family and friends did not need to be completely abstinent but, rather, needed not to consist of people who did have AOD problems. This relates to the suggestions made by Hennessy et al. (2017) that successful recovery among adolescents does not necessarily require lifelong abstinence. However, Hennessy et al. highlight that initial abstinence seem to be important. The IPs in the present study followed this suggested pattern: they were abstinent when they initiated a “successful recovery process” five years ago and all but one of them continued this process at the follow-up but with mixed attitudes towards abstinence. Many of the young adults in the study described drinking alcohol in a controlled and unproblematic way after a period of sobriety. This was not only linked to the severity of the problem but also to the image they had of themselves, i.e., there were those who did not see themselves as “former addicts”.
This can be compared with adults recovering from AOD problems where the identity of “former addict” is often used as a tool to stay abstinent. For young adults, this identity might instead be perceived as a barrier in the process of developing an adult identity. In fact, there were IPs who did not share the perception that they used to have AOD problems, although they had undergone treatment for AOD problems. The often complex problems of young adults reported in previous research (Berlin et al., 2011; Courtney & Dworsky, 2006) together with the fact that young adults have often had AOD problems for a shorter period of time than other adults, might be linked to having less of a need to identify as abstainers.
This might add a nuance to the proposed model of recovery capital for adolescents made by Hennessy et al. (2019). In the model, social capital consisting of sober and supportive relationships with family and friends is emphasised as important. Based on the assumption that total abstinence is more crucial for the young adults at the beginning of the recovery process but can be, at least for some, abandoned later during recovery, it might accordingly be suggested that a sober networks (in terms of total abstinence) are less central over time. However, more research is needed to confirm this.
Some IPs described that they had an “addictive behaviour”, which included other addictions as well as the addiction to substances. This underlines the individual variations in how the nature of the AOD problems in the group investigated can be defined. However, also for these IPs, the AOD problems themselves were not described as the main problem. Rather, the IPs defining themselves in this way described that they, after getting help with their AOD problems, were able to get to know themselves better and identify ways of dealing with themselves. Another result that differs from previous research on adults is the experience of an extra stigma related to the transition into adulthood, expressed as the feeling of lagging behind peers of a similar age and resulting in internal and external pressure. Professional contacts during the follow-up period can be interpreted as a way of mentally and practically dealing with this, in terms of, for example, guidance when choosing education and/or profession.
Conclusions
The young adults in the study did receive treatment for AOD problems and at the first interview this seemed to be sufficient for continuing their recovery. However, the results from the follow-up interviews indicate that this group often also needs professional support for mental health issues in order to reach a stable recovery. Since the problems described were heterogeneous, it is suggested that this client group could benefit from individual treatment and extended support after treatment. Further, the results indicate that the period of five years in order to reach a stable recovery might need to be extended for young adults.
Limitations and strengths
Previous research on different phases of recovery has mainly focused on adults and knowledge about whether these phases also are suitable for young adults is therefore limited. Thus, the article can contribute to the research field on recovery processes with a recovery capital perspective. However, the follow-up interviews were rather short and do not allow for in-depth analysis.
The IPs consisted predominantly of women, which may have had an impact on the results. There were gender differences; several women described becoming a parent as central, while only one of the men had children and he described this as important at the first interview but not during the follow-up process.
The group investigated in the study were between 25 and 33 years old when interviewed. As pointed out in the introduction, previous research highlights that young adulthood is characterised by specific issues but, at the same time, is difficult to limit to a specific timespan. This complicates the study of this group in general, and especially when comparisons are made with other adults. Thus, the results discussed, for example, on identity-seeking cannot be interpreted as applying to a clearly identified age group. However, the results may help to shed light on factors that might be of more importance in younger age groups that are establishing their adult lives during their recovery process.
Footnotes
Ethics
This research project was scrutinised and approved by the Ethical Review Board in Stockholm, Sweden (2018/1770-32; 2018/1973-32)
Notes
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Swedish Research Council for Health, Working Life and Welfare [Grant # 2018-00743].