
Abstract
Introduction:
Although a clear relationship has been established between elevated alcohol consumption and psychiatric problems in old age, there are few descriptions of the prevalence of elevated alcohol consumption in older adults who have been referred to geriatric psychiatric treatment.
Aim:
To describe the prevalence of self-reported elevated alcohol consumption in men and women referred to geriatric psychiatry wards in Norway, and to explore factors associated with elevated alcohol consumption.
Method:
This cross-sectional study includes data from a registry of geriatric psychiatry patients aged ≥ 65 years from December 2016 until December 2018. The outcome measure was reported elevated alcohol consumption assessed with the short version of the Alcohol Use Disorders Identification Test (AUDIT-C). The analyses used demographic data as well as a measure of cognitive function, psychiatric diagnosis and use of psychotropic drugs.
Results:
In total, 367 patients (131, 35.7% men) with a mean (SD) age of 74.7 (7.6) years were included. Of these patients, 27% scored above the pre-set cut-off for elevated alcohol consumption according to AUDIT-C (≥ 3 and 4 for women and men, respectively). The prevalence of elevated alcohol did not differ by gender. In adjusted logistic regression analysis, older age, living with someone and use of antidepressants were associated with reduced odds for reporting elevated alcohol consumption (OR 0.93, 95% CI 0.89–0.96; OR 0.54, 95% CI 0.31–0.97; and 0.54, 95% CI 0.32–0.92, respectively).
Conclusion:
A relatively high proportion of psychiatric patients aged 65 years or older reported elevated alcohol consumption, regardless of diagnosis. Older age, living with someone and use of antidepressants were associated with lower odds for elevated alcohol consumption.
Keywords
Adults older than 65 years are generally more vulnerable to the effects of alcohol compared to younger adults, with regard to occasional, regular, and elevated alcohol consumption (Hallgren, Högberg, & Andreasson, 2009). In the decade to come, a larger proportion of older people will have a higher education compared to old people today. Such a change may be expected to contribute to higher alcohol consumption (Slagsvold & Hansen, 2017). Elevated consumption entails harmful and risky use as well as misuse. However, neither the guidelines for various countries nor the Diagnostic and statistical manual of mental disorders (DSM-5) contain a standard definition of elevated consumption (Hoffmann & Kopak, 2015). It is generally recommended that people aged 65 years and older limit their alcohol consumption to one unit per day. Even so, alcohol consumption below this limit may also harm some frail older people (Fillmore, Stockwell, Chikritzhs, Bostrom, & Kerr, 2007; Moos, Brennan, Schutte, & Moos, 2004), in being linked to health problems due to age-related physiological changes (Davies & Bowen, 1999; Institute of Alcohol Studies, 2013; National Institute on Alcohol Abuse and Alcoholism, 1998; Squeglia, Boissoneault, Van Skike, Nixon, & Matthews, 2014) as well as many of the commonly prescribed drugs given to older people (Korrapati & Vestal, 1995).
Alcohol is stated to have a negative influence on at least 60 medical diseases (World Health Organization, 2004) and negatively affects cognitive function if alcohol consumption has been elevated over time (Kuzma, Llewellyn, Langa, Wallace, & Lang, 2014; Langballe et al., 2015). Moreover, a review reported an association between medical health problems and degree of alcohol consumption among older individuals (Sorocco & Ferrell, 2006). Furthermore, there are reports of relationships between elevated alcohol consumption and suicide and psychiatric illness, such as depression and anxiety, but it is not always easy to tell which came first, the disease or the elevated alcohol consumption (Caputo et al., 2012). Also, it is highlighted that older peoples’ psychosocial status, such as being retired, bored, lonely or homeless, is linked to elevated alcohol use (Holdsworth et al., 2017). In this context, there is also a gender perspective, but women today have moved more towards men’s patterns of drinking (Bratberg et al., 2016). Lastly, regular, frequent and elevated alcohol consumption are in general found to be associated with a higher level of education (Johannessen, Engedal, Larsen, Stelander, & Helvik, 2017; Li, Wu, Selbaek, Krokstad, & Helvik, 2017; Li, Wu, Tevik, Krokstad, & Helvik, 2019; Tevik et al., 2019).
Among older people, the relationship between elevated alcohol consumption, the risk factors for this type of consumption and mental health is hardly known (Støver, Bratberg, Nordfjørn, & Krokstad, 2012). Even though research on this topic has been conducted amongst younger age groups, the results may not easily be extrapolated to older age groups. A previous small study explored the association between patients’ and general practitioners’ (GPs) information and elevated alcohol consumption among patients referred to geriatric psychiatry wards (Johannessen, Engedal, Larsen, et al., 2017). However, factors associated with patient-reported elevated consumption were not explored. Thus, we wanted to further explore this topic.
Aim
The aim was to describe the prevalence of self-reported elevated alcohol consumption in women and men referred to treatment by specialist mental healthcare services designed for older people, and to explore factors associated with elevated alcohol consumption.
Method
Setting and participants
This cross-sectional study acquired data from the Norwegian Quality Registry of Geriatric Psychiatry Patients from both the southern and northern parts of the country from December 2016 until December 2018. The inclusion criteria for the present study were: age ≥ 65 years, answered the short version of the Alcohol Use Disorders Identification Test (AUDIT-C) (Babor, De La Fuente, Saunders, & Grant, 1989) and capacity to give informed written consent to participate in the study. No specific exclusion criteria were defined.
Of 708 patients (≥ 65 years) included in the registry between December 2016 to December 2018, 367 (51.8%) had answered the AUDIT-C and were included in the study.
Assessment of the patients
The outcome variable was the Alcohol Use Disorders Identification Test (AUDIT-C) (Babor et al., 1989). This test has three items assessing alcohol consumption, where each item is rated from 0 to 4, giving a sum-score. Higher scores indicate higher consumption. The cut-off score for elevated alcohol consumption on AUDIT-C was set to 3 for women and 4 for men (Crome, Dar, Janikiewicz, Rao, & Tarbuck, 2011). Socio-demographic characteristics included the variables age, gender, living alone (or not), and level of education (≥ 10 years or < 10 years). Information was provided by patients. Cognitive function was assessed by the Mini Mental State Examination (MMSE), Norwegian revised version (Engedal, Haugen, Gilje, & Laake, 1988; Folstein, Folstein, & McHugh, 1975; Strobel & Engedal, 2008). The scale consists of 20 items, with a possible score between 0 and 30. A lower score denotes more impairment. The World Health Organization’s International statistical classification of diseases and related health problems, 10th edition for research (ICD-10) (World Health Organization, 2010) was used to make diagnoses, which were made by specialists in geriatric psychiatry at discharge from the hospital. Further, the psychotropic drugs prescribed at discharge were grouped according to the Anatomical Therapeutic Chemical (ATC) (WCC+DSM, 2019) code into the following categories: antipsychotics (N05A except lithium), antidepressants (N06A), anxiolytics (N03A & N05B), hypnotics/sedatives (N05C), and opioids (N02A) (yes versus no). This information was collected from hospital medical records.
Procedure
A consent-based quality registry that includes patients admitted to in-patient wards in geriatric psychiatry in Norway has been approved by the Norwegian Directorate of Health and the Data Protection Agency (Kristiansen & Engedal, 2013). Data in the registry are from a comprehensive and standardised examination protocol used in 13 hospitals. AUDIT-C was included in the registry in December 2016. The assessments were conducted during the first two weeks after admission, whereas the primary diagnoses and drugs taken (or prescribed) in this study were made at discharge. The study was presented to the Regional Committee for Ethics in Medical Research, Southern Norway, and was approved (number 2017/2439). Ethical principles outlined in the Helsinki Declaration (World Medical Association, 2013) were followed.
Statistics
The statistical analysis was performed with IBM SPSS version 25 (Chicago, IL, USA). Descriptive analysis for categorical variables was performed with the Pearson’s chi-squared test or Fisher’s exact test (depending on sample size) and for continuous variables, the non-parametric Mann–Whitney U test was used since the data were not normally distributed.
Logistic regression analysis (the ‘Enter’ method) was performed to study factors associated with the outcome elevated reported use of alcohol (AUDIT-C ≥ 3/4 for women and men, respectively) versus no elevated reported use. Independent variables included in the unadjusted analysis were demographic variables (gender, age, living alone, and level of education), diagnoses, and information about psychotropic drugs used at study entrance. All demographic variables and variables regarding diagnoses and psychotropic drugs associated with the outcome variable at p ≤ 0.150 level in the unadjusted analysis could be potential confounders and were included in the adjusted logistical regression model. Due to missing information on independent variables, the total number in the adjusted regression analysis was 306 patients.
Tests were performed for interaction between gender and other independent variables as well as possible collinearity between independent variables. Probability values below 0.05 were considered statistically significant.
Results
Sample characteristics
Of a total of 367 patients, 131 (35.7%) were men and the mean (SD) age for the total sample was 74.7 (7.6) years (Table 1). Men were significantly younger and less likely to live alone compared to women. No gender differences were found between mean MMSE and frequency of various categories of diagnoses. The category “other diagnoses” included 10 patients with diagnoses due to alcohol misuse (three men) and eight patients with disorders due to psychotropic or illegal drug use (one man).
Characteristics of the sample by gender (n = 367).
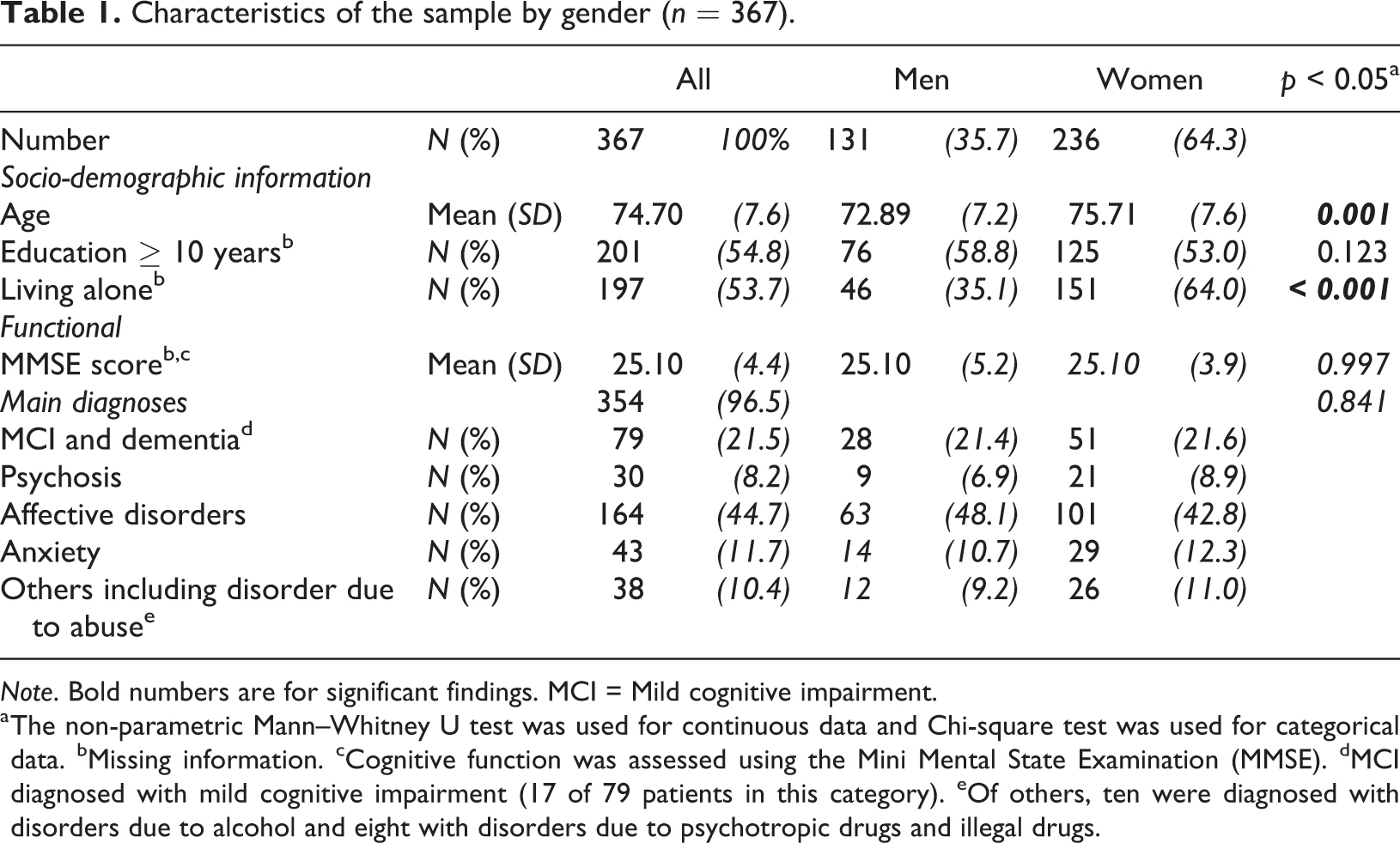
Note. Bold numbers are for significant findings. MCI = Mild cognitive impairment.
a The non-parametric Mann–Whitney U test was used for continuous data and Chi-square test was used for categorical data. bMissing information. cCognitive function was assessed using the Mini Mental State Examination (MMSE). dMCI diagnosed with mild cognitive impairment (17 of 79 patients in this category). eOf others, ten were diagnosed with disorders due to alcohol and eight with disorders due to psychotropic drugs and illegal drugs.
The 341 patients who did not answer the AUDIT-C did not differ in terms of age (mean age 75.8, SD 7.8 years), gender (31.3% men), educational level (44.9% with ≥ 10 years), living alone (54.3%), cognitive functioning (mean MMSE 24.7, SD 4.7) or category of diagnoses (mild cognitive impairment and dementia 24.6%, psychosis 8.8%, affective disorder 49.6%, anxiety 10.0% and other diagnoses 10.9%) from those who responded to the AUDIT-C.
Elevated alcohol consumption and use of psychotropic drugs
In total, 98 of 367 (26.7%) scored above a predefined cut-off from AUDIT-C, which indicates elevated alcohol consumption, and no gender difference was found. However, men living alone more frequently reported elevated alcohol consumption than men not living alone (p = 0.005), but no such differences were found among women. Women with high education levels (≥ 10 years) more frequently reported elevated alcohol consumption than women with low education levels (< 10 years) (p = 0.016), but no such significant differences were found among men.
Men less often used anxiolytics and sedatives than women, but no gender differences were found for the use of other psychotropic drug categories (Table 2). Women using antidepressants were less likely to report elevated alcohol consumption than those not using antidepressants (p = 0.006), but no such difference was found for men.
Elevated alcohol consumption and psychotropic drugs taken (or prescribed) by gender (n = 367).
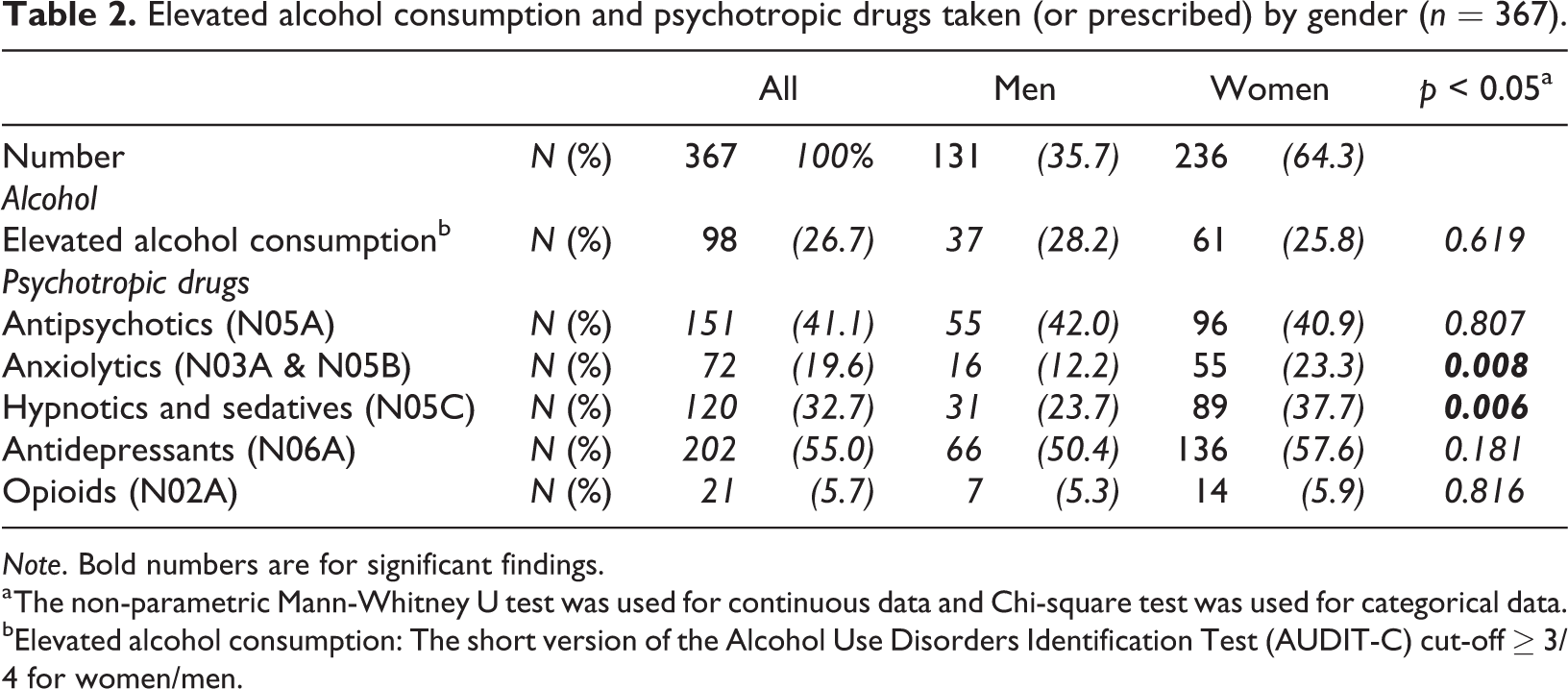
Note. Bold numbers are for significant findings.
a The non-parametric Mann-Whitney U test was used for continuous data and Chi-square test was used for categorical data.
bElevated alcohol consumption: The short version of the Alcohol Use Disorders Identification Test (AUDIT-C) cut-off ≥ 3/4 for women/men.
In adjusted logistic regression analysis, higher age, living with someone and use of antidepressants were associated with reduced odds for reporting elevated alcohol consumption (Table 3). The explained variance was 15.9% (using Nagelkerke’s R-squared).
Participant reports of elevated use of alcohol assessed with AUDIT-C.a Unadjusted and adjusted estimates.b,c
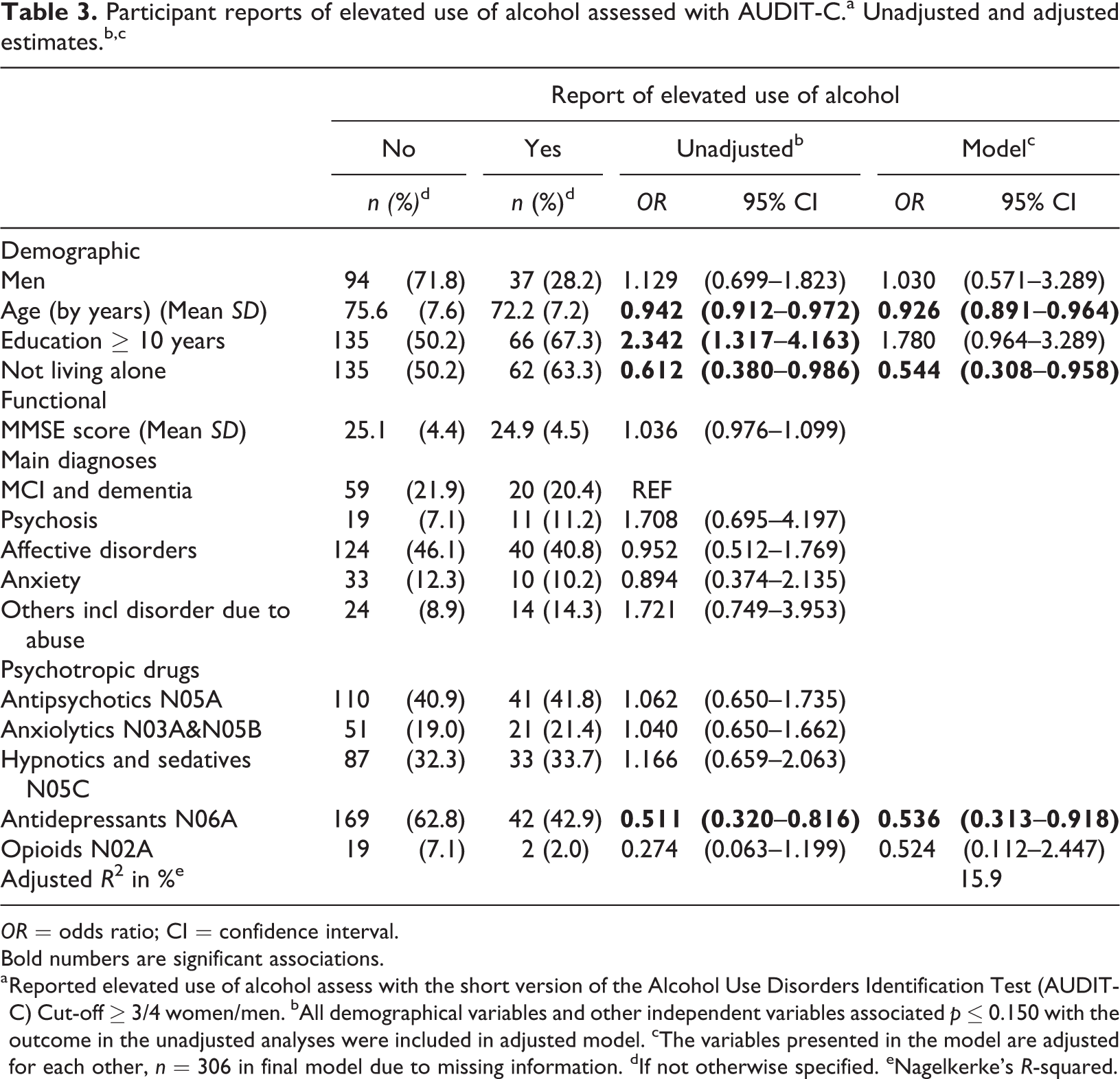
OR = odds ratio; CI = confidence interval.
Bold numbers are significant associations.
a Reported elevated use of alcohol assess with the short version of the Alcohol Use Disorders Identification Test (AUDIT-C) Cut-off ≥ 3/4 women/men. bAll demographical variables and other independent variables associated p ≤ 0.150 with the outcome in the unadjusted analyses were included in adjusted model. cThe variables presented in the model are adjusted for each other, n = 306 in final model due to missing information. dIf not otherwise specified. eNagelkerke’s R-squared.
Discussion
The prevalence of reported elevated alcohol consumption was about 27% in the present study, based on information from a Norwegian quality registry, including older hospital in-patients in specialist mental healthcare. No difference in prevalence was found by gender. Men living alone more often reported elevated alcohol consumption than men not living alone, while women with a high educational level (≥ 10 years) and women who did not use antidepressants more often reported elevated alcohol consumption than women with less education or who used antidepressants. In adjusted logistic regression analysis, higher age, not living alone and using antidepressants were associated with lower odds for reporting elevated alcohol consumption.
The prevalence of reported elevated alcohol consumption was considerably high in older psychiatry patients and higher compared to what is reported in Norwegian population-based studies (Li et al., 2019; Tevik et al., 2017). However, the prevalence in the present study (27%) was in line with the prevalence found in a previous Norwegian study (23%), including comparable patients (Johannessen, Engedal, Larsen et al., 2017). A comparable high prevalence of elevated alcohol consumption (20%) has also been reported in Australian patients referred to a geriatric medicine hospital (Draper et al., 2015). Elevated alcohol consumption in old age may be a risk factor for mental and physical health problems, but also a way of coping with mental and physical health problems (Caputo et al., 2012; Sorocco & Ferrell, 2006). It is not always easy to know which comes first (Caputo et al., 2012), but older adults are more vulnerable to alcohol consumption than younger adults (Davies & Bowen, 1999; Hallgren et al., 2009; Institute of Alcohol Studies, 2013; National Institute on Alcohol Abuse and Alcoholism, 1998; Squeglia et al., 2014), and detecting elevated consumption among older adults, both in primary and specialist healthcare services, may be health promoting (Wang & Andrade, 2013), if a brief intervention on elevated consumption (Schonfeld et al., 2010) or alcohol abuse treatment is carried out (Dauber, Pogarell, Kraus, & Braun, 2018). Only five per cent of the patients in the present study had disorders due to abuse as their main diagnoses. The prevalence of this diagnosis was comparable to the previously described Norwegian study (Johannessen, Engedal, Larsen, et al., 2017). Of patients with disorders due to abuse, 10 (seven women) had disorders due to alcohol. We do not know whether these figures reflect the situation in the general public. Nevertheless, Norwegian GPs have experienced that many older people have existential needs that are not necessarily met or handled adequately by them, their next of kin, or society, and for some alcohol consumption may seem to be a solution to improve wellbeing (Johannessen, Helvik, Engedal, Ulstein, & Sørlie, 2015). Within this framework, elevated alcohol consumption may arise independently of the type of mental health problems or disorders older people experience. Consequently, it was not unexpected that type of diagnosis was not associated with reported elevated alcohol consumption in this relatively restricted study sample.
In the unadjusted analysis, men living alone more often reported elevated alcohol consumption than those living with someone, while for women, those who took antidepressants were less likely to report elevated alcohol consumption. However, in the regression analysis adjusting for gender and other independent variables, living with someone and using antidepressants were both independently associated with lower odds for reporting elevated alcohol consumption. Population studies of alcohol use among younger adults have, in line with our study, previously reported that divorced and unmarried men and women had a higher alcohol consumption than those living with a partner (Vedøy & Skretting, 2009).
In the present study, no interaction was found between gender and factors associated with the outcome. Thus, we cannot say that there are gender-specific factors for reporting elevated consumption. The association between living alone and elevated consumption is in line with previous studies of home-dwelling older adults (Li et al., 2019), but no association was found in the previous Norwegian study of departments of geriatric psychiatry (Johannessen, Engedal, Larsen, et al., 2017). Thus, we need more insight into the significance of living alone for elevated alcohol consumption in older people with mental health problems. We found that people using antidepressants were less likely to have elevated alcohol consumption. We do not have a clear explanation for this. It may be that people who use antidepressants know that combining these drugs and alcohol is not healthy and therefore did not consume alcohol frequently or did not report elevated consumption. Alternatively, they may have preferred use of antidepressants as a treatment rather than using alcohol. However, we do not know the length of time the various drugs were used or if they were newly prescribed.
This registry study has some limitations. First, as stated above, the timeframe for patients’ use of psychotropic drugs is unclear. Of equal importance is the restricted number of patients who reported alcohol consumption in the registry. We do not know whether there are systematic differences in how AUDIT-C is used in different hospitals, or whether the lack of information is due to the unwillingness of patients to answer questions or the staff not asking questions when reviewing patients, even if it is a part of the standard protocol. A previous study of health personnel who reviewed patients in departments of geriatric psychiatry reported that personnel found it difficult to include questions on alcohol use in their overall review (Johannessen, Engedal, & Helvik, 2017). The low response rate may not only restrict our statistical power, give us less precise estimates of prevalence of elevated alcohol and uncertain associations to elevated alcohol consumption, but may contribute to selection bias. We do not know whether patients who responded to AUDIT-C are different from those who chose not to respond to the questions. Thus, the external validity may be hampered and the study results should not be generalised to cover geriatric psychiatry patients in general. Furthermore, we have relied on the patients’ own reports of alcohol consumption to assess elevated alcohol consumption, which is commonly done, but may be an unreliable source (Crome et al., 2011; Feunekes, van ‘t Veer, van Staveren, & Kok, 1999; May et al., 2018; O’Connell, Chin, Cunningham, & Lawlor, 2003). Moreover, the research design does not enable us to draw any causal conclusion. Although our study has some limitations due to high drop-out rate, it shows that health personnel should increase their awareness of elevated alcohol consumption when assessing older people with psychiatric morbidities, particularly since alcohol consumption and alcohol-related problems in older adults are expected to rise in the years to come (Slagsvold & Hansen, 2017). Future research including older psychiatric patients should pay more attention to use of alcohol.
To sum up, a relatively high proportion of older psychiatric patients reported elevated alcohol consumption, regardless of diagnosis. Older age, living with someone and use of antidepressants were associated with lower odds for elevated alcohol consumption.
Footnotes
Author contributions
Anne-Sofie Helvik has performed the analysis and drafted the manuscript, Aud Johannessen had the research idea, Aud Johannessen and Knut Engedal continuously discussed findings and interpreting of results with Anne-Sofie Helvik. All authors contributed in the manuscript development and the final critical revisions.
Acknowledgements
The authors wish to thank all the participating hospitals for collecting the data and the patients for sharing information and experiences, as well as Norwegian National Advisory Unit on Ageing and Health and Faculty of Medicine and Health Sciences, NTNU, which both supported the study.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.