
Abstract
Aims:
During inpatient substance abuse treatment, professionals seek to help clients to achieve improvement in various life domains affected by substance abuse. Progress monitoring during substance abuse treatment has been called for, and in this study we examine how clients’ levels of well-being and hope change during inpatient substance abuse treatment.
Methods:
Clients (N = 168) entered the treatment facility between January 1, 2017 and August 31, 2018. The prospective data were gathered from one treatment unit located in central Finland on entry into treatment, during and at the end of treatment. Using the Outcome Rating Scale (ORS) as a therapeutic tool was standard procedure in the treatment unit. Demographic information on participants, information on their previous substance use and scores on the State Hope Scale (SHS) were collected through structured questionnaires. Non-parametrical tests (Mann–Whitney U test; Kruskal–Wallis χ2; Spearman’s rho) were used to study changes in indicators of well-being and hope.
Results:
As hypothesised, inpatient treatment had a positive effect on both ORS and SHS and they were interrelated. Differences in gender, living situation and previous admissions were found when studying how the background information of the participants was related to the change achieved in ORS and SHS.
Conclusions:
Inpatient substance abuse treatment seemed to enhance both well-being and hope of the clients of inpatient substance abuse treatment.
People referred to inpatient substance abuse treatment often experience severe social, psychological and physical consequences of their alcohol, drug or prescription drug dependency. In such cases outpatient treatment has been considered insufficient and more intensive support, such as interventions in residential settings, is needed. Substance abuse treatment no longer seeks solely to achieve and maintain abstinence, but also to enhance individuals’ prospects for a fulfilling life (Laudet & White, 2010, pp. 51–52). This mirrors a broader concept of recovery as an “individualized, intentional, dynamic, and relational process involving sustained efforts to improve wellness” (Ashford et al., 2019, p. 183). In recent decades, well-being and hope have received increasing scholarly attention in general (see Gallagher & Lopez, 2018). However, research has been scarce in Nordic substance abuse treatment settings. In this article we focus on the effects of inpatient substance abuse treatment on clients’ well-being and hopefulness using data from one treatment unit located in central Finland.
In therapeutic treatment settings, systematic evaluation of treatment outcomes is increasingly becoming a customary procedure and has been called for in substance abuse treatment as well as in research (Goodman, McKay, & DePhilippis, 2013). In this study we used a prospective design to examine the effects of inpatient substance abuse treatment on change in clients’ well-being and hope. Assessing change in well-being and hope is an ethical and client-oriented way of studying the effectiveness of treatment. Assessments during treatment inform clinical decision-making during treatment and enhance client participation, but also address emerging requirements for effectiveness and progress monitoring imposed by funders (Lambert, Hansen, & Finch, 2001; Lambert et al., 2003; Miller, Duncan, Brown, Sparks, & Claud, 2003). It is essential to understand what happens during treatment and what basis it provides for maintaining the achieved change after treatment (see Shumway, Bradshaw, Harris, & Baker, 2013).
Well-being, hope, and substance abuse
As treatment is provided in order to generate positive change, well-being and hope together express essential elements of recovery (see Best & Lubman, 2012; Leamy, Bird, Le Boutillier, Williams, & Slade, 2011). Well-being and hope can both be theorised and defined in various ways. Well-being often refers to positive mental health, subjective, psychological or social well-being, life satisfaction or quality of life (Dodge, Daly, Huyton, & Sanders, 2012; Linton, Dieppe, & Medina-Lara, 2016). In their review, Dodge et al. (2012) define stable well-being as a state of equilibrium between an individual’s resource pool and the challenges faced in psychological, physical, and social domains of life (Dodge et al., 2012, p. 230). When encountering challenges, an imbalance is inevitable and individuals are compelled to adapt their personal resources to meet the new situation (Kloep, Hendry, & Saunders, 2009, p. 337). This highlights the dynamic nature of well-being. Substance abuse and issues related to it may cause imbalance, but it may also be the imbalance that leads to problematic substance use. This way, help seeking can be defined as an endeavour to exert influence on this imbalance. During inpatient substance abuse treatment, professionals seek to help clients to gain improvement in various life domains affected by substance abuse (Andersson, Otterholt, & Gråwe, 2017; Orford et al., 2006), such as intrapersonal well-being, social relationships, and life functioning, i.e. to enhance their well-being (see Miller et al., 2003; see also Lambert et al., 1996). Improvement in these domains may also increase clients’ hope of a better future.
Schrank, Stanghellini, and Slade (2008) in their review consider hope an important therapeutic factor and a vital component of recovery. While defining it in varying ways, they conclude that hope is a dynamic variable involving the attainment of individually valued future goals (Schrank et al., 2008). In terms of future goals, Snyder et al. (1991) conceptualise hope as a dual construct of agency (i.e., goal-directed determination or motivation) and pathways (i.e., strategies or plans for achieving goals). There has been discussion on whether hope is the same as, or how it differs from, other related constructs such as self-efficacy, outcome expectancies or optimism. There seem to be similarities and overlaps between the concepts, such as positive outlook on the future, but also some fundamental differences, such as whether thoughts about one’s ability to meet goals or the generalised expectancy that good things will happen is emphasised (Rand, 2018; see also Snyder et al., 1991). Altogether, the focus is on a better future. In substance abuse treatment the professionals’ task is to inspire their clients’ hope in a treatment process by actively creating different visions with them (Koehn & Cutcliffe, 2012, p. 85). Positive future goals formed during the treatment process can serve as a motivator and produce change.
As there are many ways to assess both well-being and hope (see Dodge et al., 2012; Linton et al., 2016; Schrank et al., 2008), definitions used in earlier studies and the results obtained vary. In terms of personal well-being, substance abuse has been associated with negative physical and mental health, injuries and substance-related deaths (e.g., Corrao, Bagnardi, Zambon, & La Vecchia, 2004; Onyeka et al., 2013; Pirkola et al., 2005; Rehm, 2011; Rönkä, Karjalainen, Martikainen, & Mäkelä, 2017). For example, in comparison with other populations, people who inject drugs report lower levels of both physical and mental health (Dietze et al., 2010; Fischer, Conrad, Clavarino, Kemp, & Najman, 2013).
While high levels of hope have been associated with engaging in health-enhancing behaviours (Berg, Ritschel, Swan, An, & Ahluwalia, 2011; Nothwehr, Clark, & Perkins, 2013), low levels of hope predicted alcohol use and binge drinking among college students (Berg et al., 2011; see also Brooks, Marshal, McCauley, Douaihy, & Miller, 2016). Hope helps to cope with pain (Snyder et al., 2005), injuries (Creamer et al., 2009), and illness (Madan & Pakenham, 2014; Stanton, Danoff-Burg, & Huggins, 2002). It is also related to satisfaction with life despite chronic and degenerative illness (Galin, Heruti, Barak, & Gotkine, 2018). Hope has been considered a protective factor against psychological distress and emotional hardship, promoting resilience and good mental health (Chang & DeSimone, 2001). In a review of hope as a source of resilience for physical and mental health, the link between hope and better health has been established. However, it is still inconclusive whether well-being is a result of hope or vice versa (Ong, Standiford, & Deshpande, 2018; see also the meta-analysis by Alarcon, Bowling, & Khazon, 2013).
Research on the social domain of well-being and hope is somewhat limited, but Lee and Gallagher (2018, p. 293) argue that they are intertwined, and that hope promotes social facets of well-being. Substance abuse affects not only personal well-being but also social identity and relationships (Dingle, Cruwys, & Frings, 2015; Dingle, Stark, Cruwys, & Best, 2015; Polenick, Cotton, Bryson, & Birditt, 2019) as well as resources like education, work, housing, and income (Onyeka et al., 2013), causing challenges to well-being and hopefulness. For example, a connection between hope and compassion for self, social skills, communication apprehension (Umphrey & Sherblom, 2014, 2018) as well as satisfaction with available social support (Horton & Wallander, 2001) has been found. Additionally, hope has been associated with problem-solving ability, academic achievement, and job performance (Abbas, Raja, Darr, & Bouckenooghe, 2014; Curry, Snyder, Cook, Ruby, & Rehm, 1997; Reichard, Avey, Lopez, & Dollwet, 2013).
The research so far on substance abuse treatment and its effects on both well-being and hope seems promising. While well-being on entering treatment has been reportedly low, the positive change in well-being during treatment has been significant (Quirk, Miller, Duncan, & Owen, 2013; Schuman, Slone, Reese, & Duncan, 2015). Moreover, well-being and hope appear to be intertwined in different treatments and their effects. In 12-step groups, hope has been acknowledged to have a mediating effect on health-promoting behaviours (Magura et al., 2003; Wnuk, 2017). In residential treatment settings, hope has been associated with better quality of life, greater social support from friends and family, and longer duration of abstinence (Irving, Seidner, Burling, Pagliarini, & Robbins-Sisco, 1998; see also Mathis, Ferrari, Groh, & Jason, 2009). Shumway et al. (2013) examined inpatient substance abuse treatment and its effect on readiness for change, craving, resilience, family functioning, and hope. The results were positive in all these domains. In family treatment settings, hope has been found to be related to readiness to change and healthy coping skills (Bradshaw et al., 2015).
Previous studies presented here used various definitions and measures for assessing well-being and hope. In this study we utilised the Outcome Rating Scale (ORS; Miller et al., 2003), which divides well-being into individual, relational, social and overall sense of well-being. To measure hope we used the State Hope Scale (SHS; Snyder et al., 1996), as it views hope as situational but is also goal and future oriented. As far as we know, in the inpatient substance abuse treatment context, there is so far no research using both ORS and SHS measures.
Hypotheses
Based on earlier research on well-being and hope, we hypothesised that during inpatient substance abuse treatment a positive effect on both well-being (ORS; Miller et al., 2003) and hope (SHS; Snyder et al., 1996) would appear. Our second hypothesis was that ORS and SHS would be positively interrelated.
Materials and methods
Study design
This study was conducted in an inpatient substance abuse treatment unit located in central Finland as a part of research project Changing expectations in clients and substance abuse treatment outcomes. The treatment unit provides non-medical, therapeutic community-based treatment for both individuals and families. The treatment applies cognitive behavioural therapy, i.e., the focus is on providing information about recovery, relapse and behavioural patterns in order to achieve change in problematic substance abuse. Therapeutic communities are both a way of organising daily practices during treatment and a therapeutic method including group sessions in addition to individual sessions with employees. Participants are also encouraged to take part in 12-step groups. These offer a place for peer support alongside the professional help received in inpatient treatment. A treatment period usually lasts one to three months and municipalities bear the majority of the treatment costs. As participants are usually referred to treatment from social services, they most likely do not have a clinical diagnosis of substance use disorder (SUD). Also, the criteria for referral to treatment may vary depending on the participant’s municipality of residence. However, professionals have viewed their substance use and its consequences as severe and outpatient treatment insufficient for their needs.
Consent from the directorate of the treatment unit was obtained in October 2014 and ethical approval was received from The Ethics Committee of the Tampere region. The research complies with the guidelines of the Finnish codes of research ethics and governance (Responsible conduct of research…, 2012). The implementation of the study adhered to naturalistic principles, that is, clients were not selected and treatment was arranged according to the unit’s everyday practices. The study arrangements were planned in such a way as to cause as little burden on participants as possible. Apart from filling out questionnaires and structured measurements, the treatment process was not disrupted (see Kypri, Langley, Saunders, & Cashell-Smith, 2007).
The treatment procedure was a prospective follow-up study with measurements at baseline, during, and at the end of the treatment and also at three and six-month follow-up. The present study consists of measures during treatment. The participants filled out structured questionnaires consisting of questions found useful in earlier studies on treatment effectiveness in Finland (see, e.g., Kuusisto & Saarnio, 2012) and structured measurements, such as the ORS and the SHS.
Monitoring of well-being (ORS; Miller et al., 2003) is standard procedure in the treatment unit. In the ORS, multiple assessments are conducted during treatment on a weekly basis, which may be useful for examining dynamic processes and making it possible to examine the mechanisms of change underlying treatment efficacy (see Witkiewitz & Marlatt, 2004). This part of the data arises from the treatment unit’s daily practices.
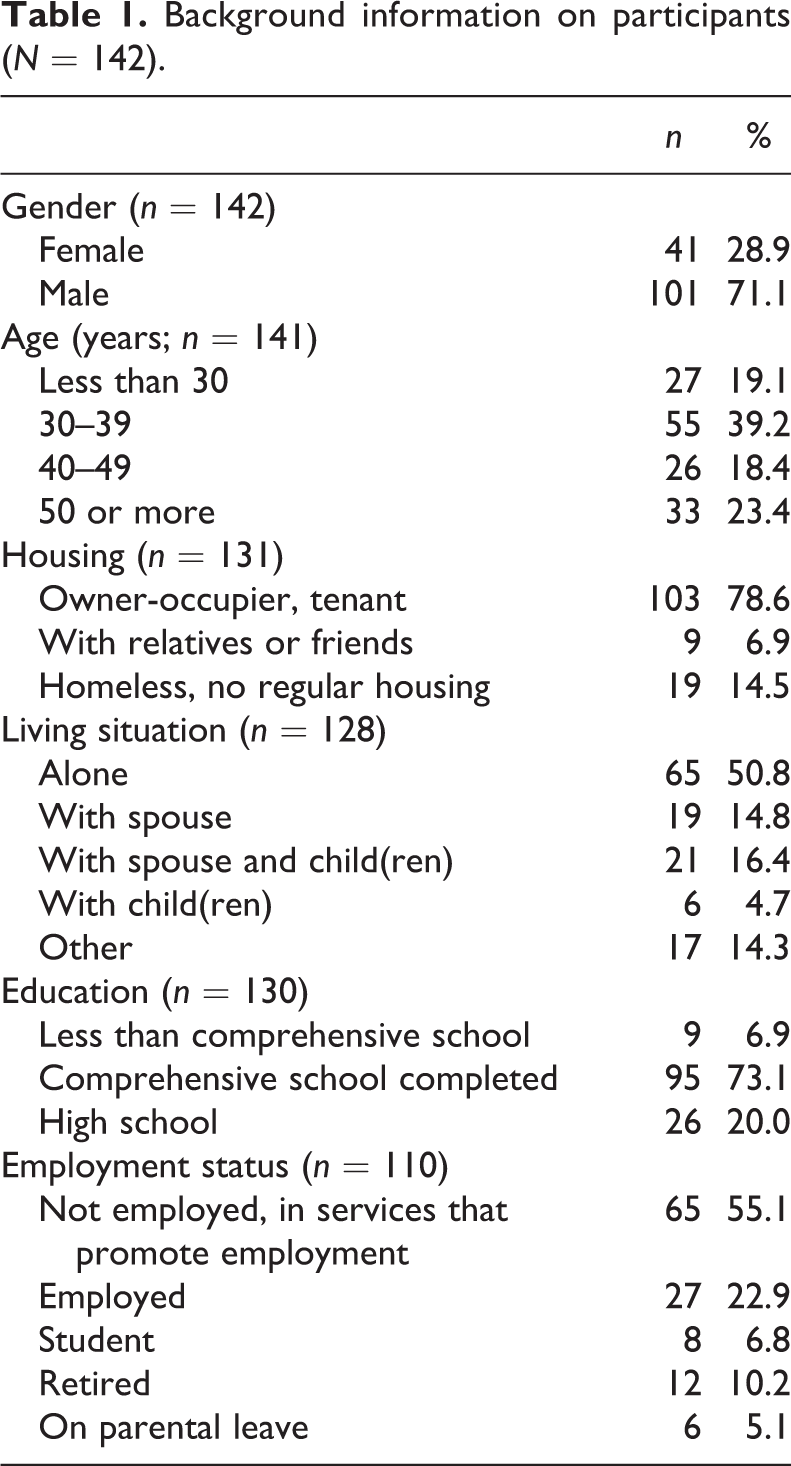
Demographic information on participants (see Table 1), information on their previous substance use (see Table 2) and scores on the SHS (Snyder et al., 1996) were collected through structured questionnaires. To study inpatients’ hopefulness, we utilised the SHS (Snyder et al. 1996), which is based on goal-focused conceptualisation of hope by Snyder et al. (1991).
Background information on participants (N = 142).
Information on participants’ (N = 142) substance use before treatment.
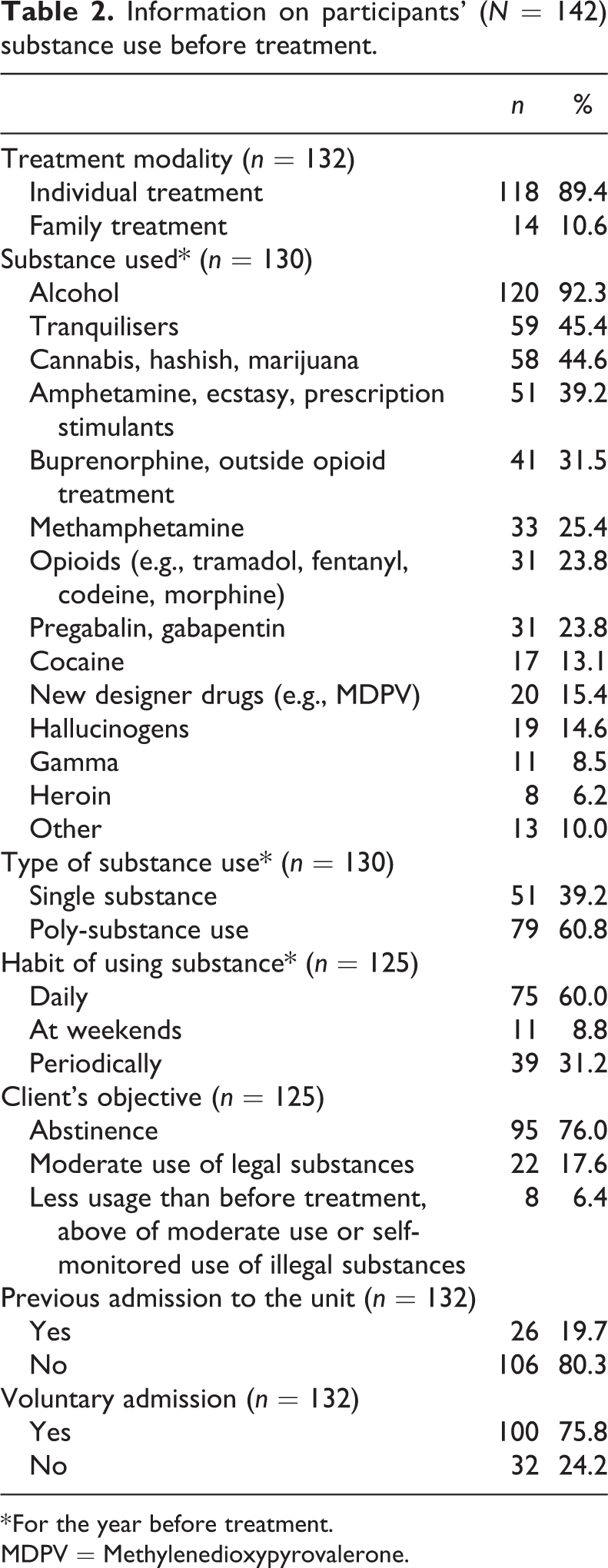
* For the year before treatment.
MDPV = Methylenedioxypyrovalerone.
The clients providing written consent to participate in the study (N = 168) entered substance abuse treatment between January 1, 2017 and August 31, 2018. Participant flow during the study is presented in Figure 1. As we study change during inpatient treatment, numbers of ORS and SHS assessments were decisive exclusion criteria. At the beginning and at the end of treatment at least two ORS and SHS assessments were conducted among 133 and 89 participants respectively. Eighty participants had undergone at least two ORS assessments and two SHS assessments.
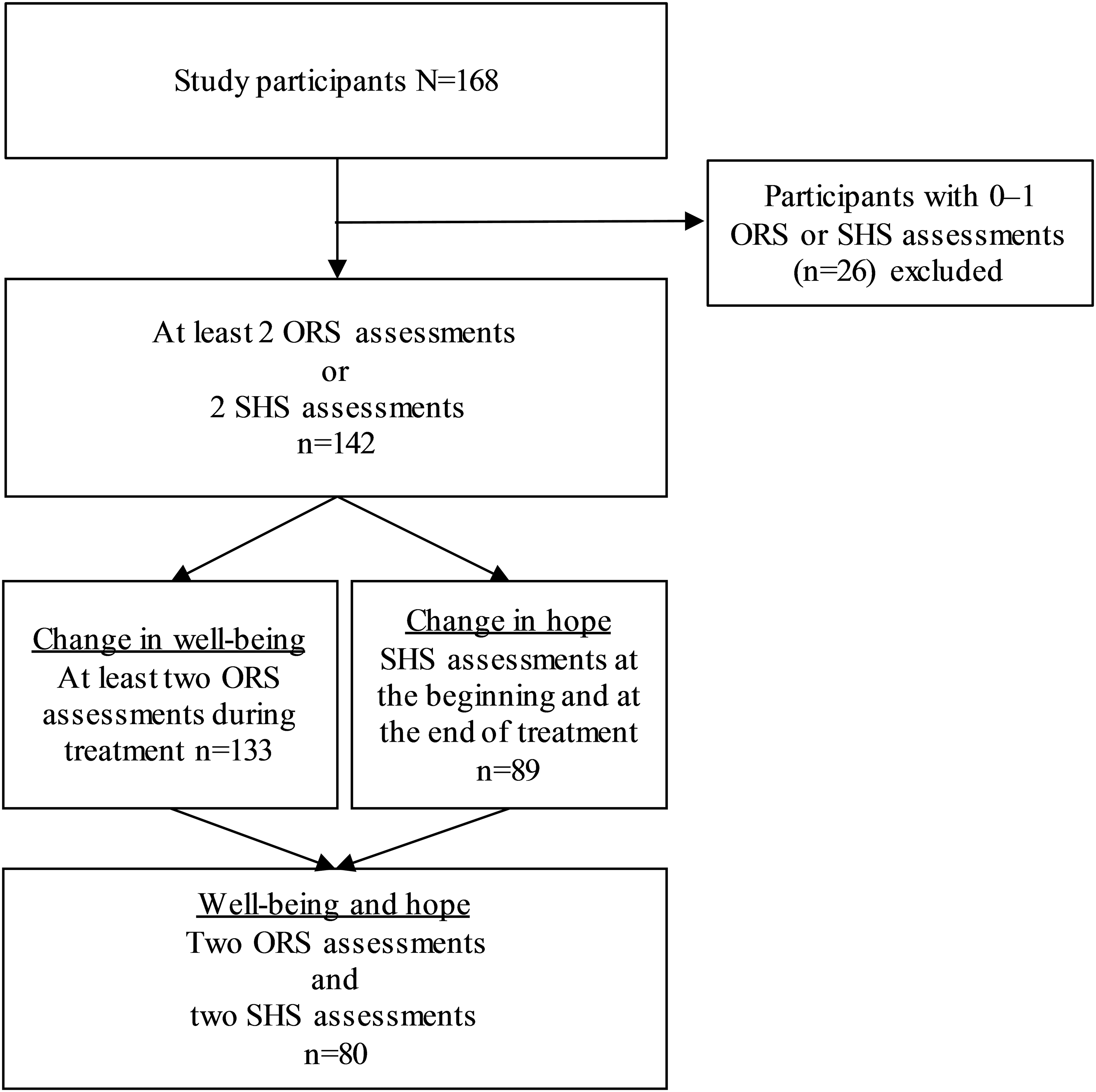
Participant flow and exclusion criteria.
Participants
Tables 1 and 2 present demographic data on the participants and their prior substance use. The majority were men and the largest age group was 30–39 years. A minority of the participants were homeless or lacked regular housing. Their level of education was rather low and the employment rate among participants was high. The demographic data corresponded to that of clients of inpatient substance abuse treatment described in earlier Finnish studies (Saarnio et al., 1998).
The majority of participants were in individual treatment. However, some participants attended family treatment with their child(ren) and/or partners. Participants had used various substances before entering treatment. For those abusing only one substance, this was alcohol. The fact that under 10% of the participants used substances only at weekends highlights the severity of the clients’ problems. Thus, it is noteworthy that the majority of participants were striving for abstinence. Involuntary admission included, for example, clients referred from the child protection or other social or healthcare services.
Attrition was analysed using both the ORS and the SHS. First, we compared clients with 0–1 ORS assessments to participants with at least two ORS assessments. We also compared clients with 0–1 SHS assessments to participants with at least two SHS assessments. Attrition was analysed using crosstabulation and Chi Square analysis. Only statistically significant differences in background information variables (see Tables 1 and 2) were found regarding age. In both the ORS and the SHS, age of 30 years or more was associated with higher probability of multiple assessments (ORS: χ 2 = 9.746, df = 3, p = .021; SHS: χ 2 = 11.372, df = 3, p = .020) indicating longer treatment periods.
Materials
The Outcome Rating Scale, ORS
Subjective well-being was assessed using the Finnish version of the Outcome Rating Scale (ORS; Miller et al., 2003), a self-report instrument designed to measure progress in client functioning during treatment. The treatment unit calls the ORS a well-being assessment (in Finnish: Hyvinvoinnin arvio). The ORS consists of a visual analogue scale with four items: individual, relational, social, and overall sense of well-being. Each of the four 10-cm lines indicates one of the four items, with instructions to place a mark on each line with low estimates to the left and high estimates to the right, adding up to a total score of 40 (Miller et al., 2003). In the treatment unit, the ORS was used as a therapeutic tool on a weekly basis. The client conducted the first assessment in a session with the therapist. Later assessments were conducted in therapeutic groups with other clients and a unit employee. It took approximately one to two minutes to complete the ORS; however, clinical discussions about the reasons behind the scores lasted approximately 20 minutes per client.
The overall alpha reliability for the ORS composite score in the original study was .93. It has been shown to be sensitive to change in treatment settings while remaining stable for those not undergoing treatment (Miller et al., 2003). Across studies using the ORS, Cronbach’s alpha coefficients for scores have been .85 on average in clinical samples (Gillaspy & Murphy, 2011; see also Bringhurst, Watson, Miller, & Duncan, 2006; Campbell & Hemsley, 2009). In the present sample, the Cronbach’s alpha coefficient for the ORS composite score at baseline was .83. On average clients’ well-being was measured six times (Mdn = 5, mode = 4).
The State Hope Scale, SHS
Hope was measured using a Finnish version of the State Hope Scale (SHS; Snyder et al., 1996) as a part of a structured questionnaire in the first and last weeks of treatment. The SHS was used in this study due to its goal and future-oriented view on hope (see Snyder et al., 1991). The SHS has two domains, both using a Likert scale 1–8: three items about agency thinking (i.e., goal-directed determination or motivation) and three items about pathways thinking (i.e., strategies or plans for achieving goals) (Snyder et al., 1996). As treatment should provide participants with tools for recovery and progress, it is important to measure situational hope (see also Irving et al., 1998). The SHS measures hope as a situational and dynamic phenomenon. However, state hope typically fluctuates within a limited range around a person’s level of dispositional (i.e., trait) hope. In the original study, college students completed the SHS every day for 29 consecutive days. The Cronbach’s alpha coefficients ranged from .82 to .95. In agency thinking, indices ranged from .83 to .95, and for pathways thinking, from .74 to .93. (Snyder et al., 1996). In the present sample the Cronbach’s alpha coefficient for SHS composite score at baseline was .89, for agency thinking .86, and for pathways thinking .75, and at the end of treatment these were respectively .89, .86, and .81.
Statistical analysis
Statistical analyses were carried out using IBM SPSS Statistics 25 software. Data are seldom normally distributed in treatment studies, as also in this study. In our analyses we utilised non-parametrical tests – Mann–Whitney U test (U), Kruskal–Wallis test (χ 2), and Spearman’s rho (r s) – for testing correlations.
Results
The analysis started by examining how well-being (ORS) changes during treatment. The change in individual, relational, social, and overall well-being can be seen in Figure 2. These items seem intertwined especially at the second, third, and fourth assessment points.
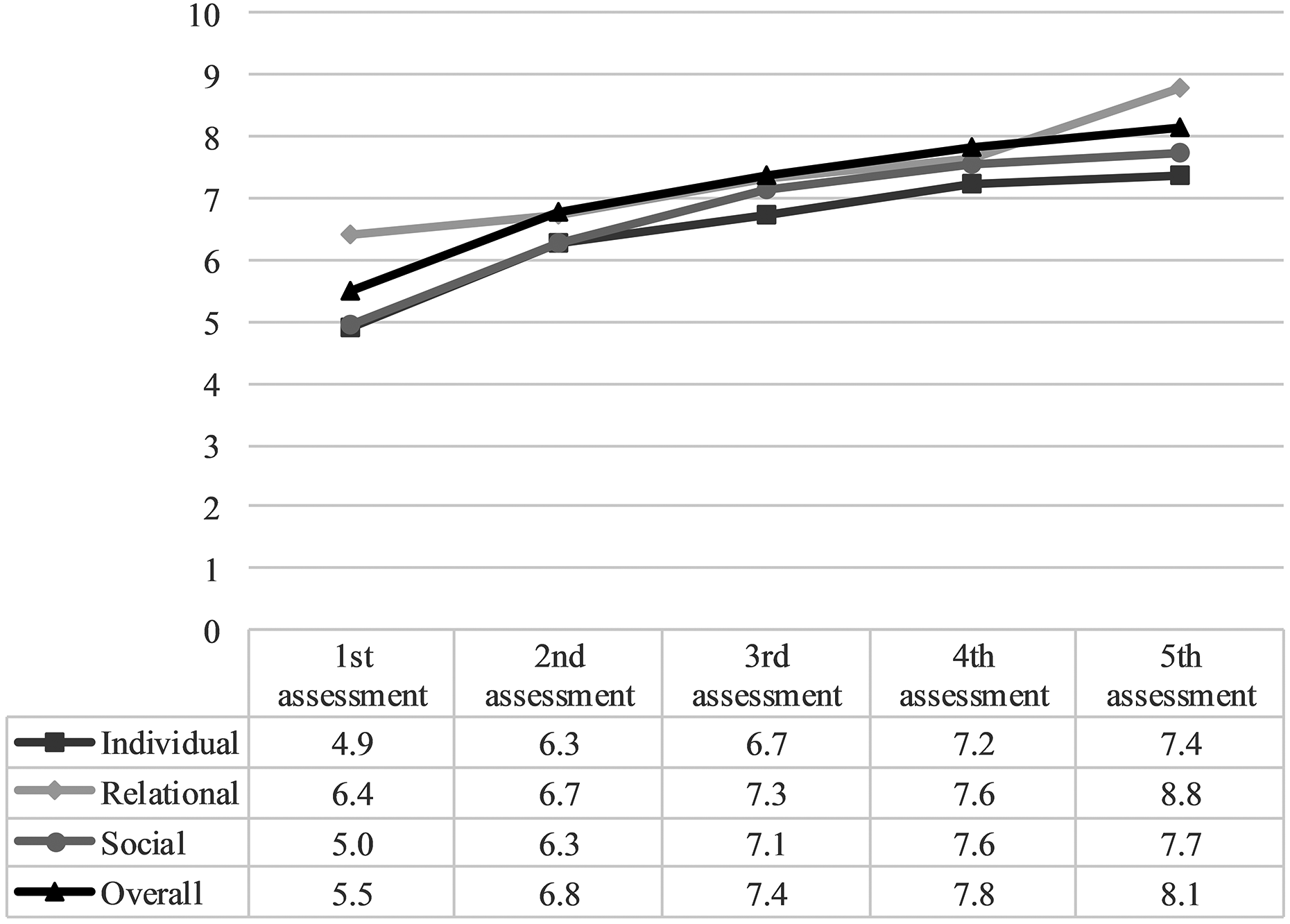
Items of the Outcome Rating Scale (ORS) within five assessments.
Change in total ORS mean scores during the first five assessments is presented in Figure 3. The mean total ORS score at the first assessment was less than 25, which has been considered a cut-off point for well-being (Miller et al., 2003). It indicates that the level of well-being is likely to be in a reduced state when entering treatment.
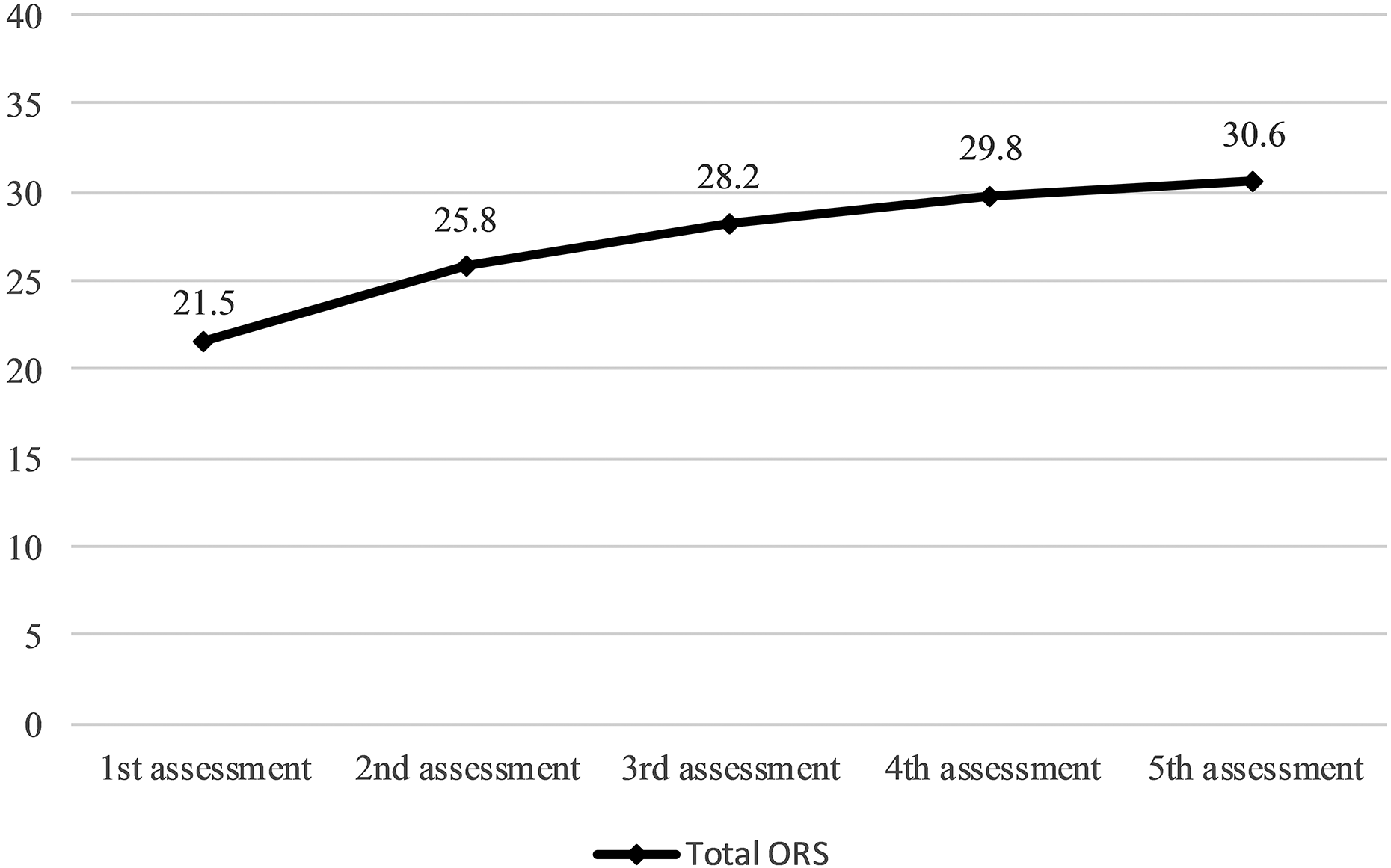
Change in total Outcome Rating Scale (ORS) scores within five assessments.
The change in total ORS scores (0–40, N = 133) between the first and last assessments was positive for the majority of participants (n = 117, % = 88, M = 11.60, SD = 7.14, min = 0.20, max = 35.90). Negative change was more infrequent and smaller (n = 16, % = 12, M = −4.69, SD = 4.83, min = –16.20, max = –0.70).
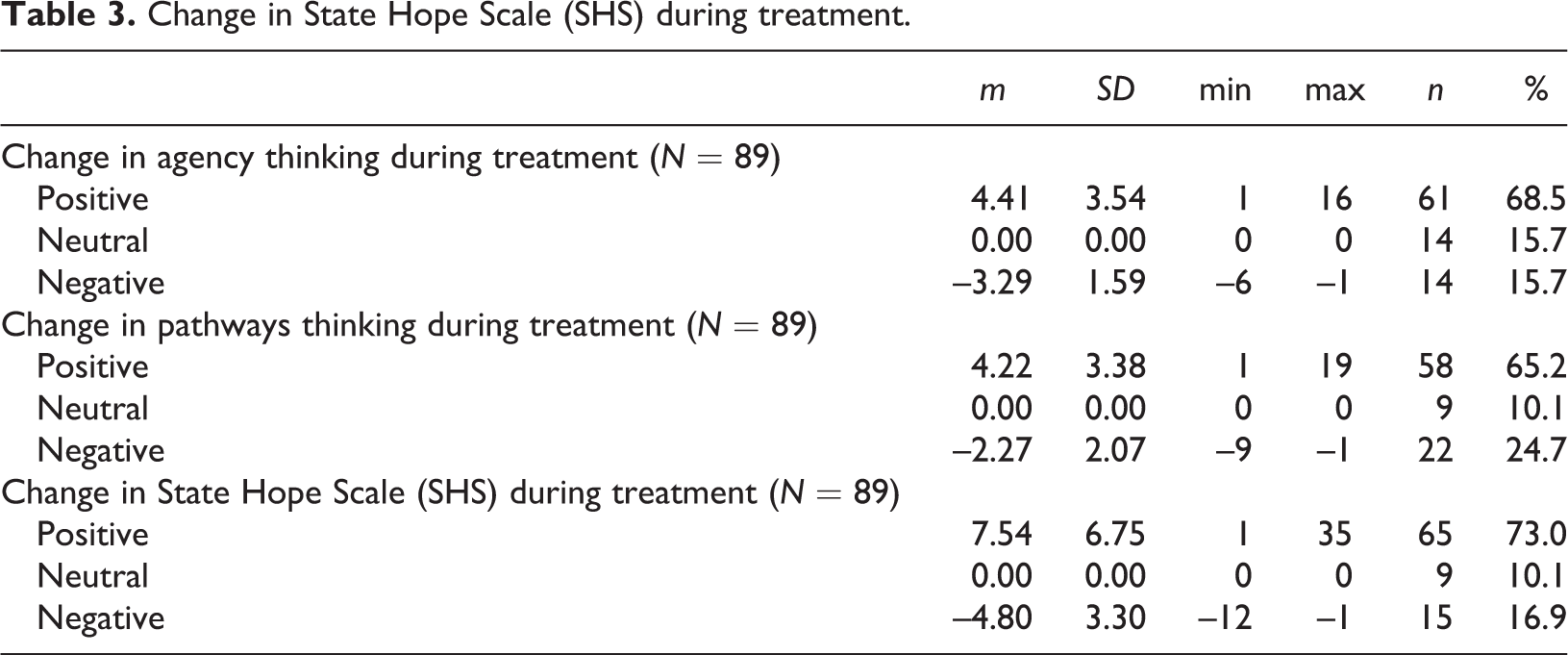
Second, we studied how hope (SHS) changes during treatment. Table 3 presents changes in agency thinking, pathways thinking, and total SHS. As in ORS, the change in SHS and its domains was positive for the majority of participants. However, almost every fourth person experienced a negative change in pathways thinking.
Change in State Hope Scale (SHS) during treatment.
After investigating the previous research questions, we concluded that our first hypothesis, during inpatient substance abuse treatment a positive effect on both ORS and SHS will appear, was confirmed. We continued the analysis by examining how the background information of the participants was related to the change of ORS and SHS scores.
Mann–Whitney U and Kruskal–Wallis tests were used to test distribution of well-being and hope regarding the background information variables (presented in Tables 1 and 2). In the tests, null hypotheses were that distributions of ORS and SHS would be the same across categories of background information variables.
In the case of change in ORS, we found statistically significant differences in previous admissions (U = 1658.500, p = .003). For those participants who had previously been admitted to the inpatient treatment unit, the mean rank of change in ORS was higher (n = 24, mean rank = 81.60), i.e., perceived change was greater than for those not previously admitted (n = 99, mean rank = 57.25).
In analysing change in SHS, differences were seen in gender (U = 506.000, p = .007), indicating that the change was greater for women (n = 25, mean rank = 56.76) than for men (n = 64, mean rank = 40.41). Differences were also found in living situation (χ 2 = 6.965, df = 2, p = .031). Higher mean rank was associated with living in the situation “other” (n = 11, mean rank = 55.86) than alone (n = 39, mean rank = 47.12) or with spouse and/or children (n = 36, mean rank = 35.81).
In this study, we did not have exact information on how long the treatment periods continued. However, the number of weekly ORS assessments correlated with changes in both ORS (r s = .231, p = .008) and SHS (r s = .313, p = .004), indicating that longer treatment periods were associated with greater change in ORS and SHS.
In order to test our second hypothesis that well-being and hope are positively interrelated, we utilised Spearman’s correlation analysis. Scores on the ORS and the SHS correlated positively both at the beginning (r s = .416, p = .000) and at the end of treatment (r s = .318, p = .004) thus confirming the hypothesis. Controlling for background information variables and number of ORS assessments did not affect the correlation.
Discussion
In this study we used a prospective design to examine the effects of the inpatient substance abuse treatment on change in clients’ well-being and hope. Both our hypotheses were confirmed: inpatient treatment had a positive effect on well-being (ORS; Miller et al., 2003) and on hope (SHS; Snyder et al., 1996) and they were positively interrelated. The change in well-being between the first assessment at the beginning of inpatient treatment and the last assessment at the end of treatment was significant. The scores changed from distressed state to scores typical for the functional population as described in the studies by Schuman et al. (2015) and Quirk et al. (2013). Also, the mean values in the various ORS items (individual, relational, social, and overall sense of well-being) indicate that the experience of well-being can be comprehensive. The change in SHS and its domains (agency and pathways thinking) was positive for the majority of participants.
The scientific significance of this study with a prospective research design is in providing information on how well-being and hope change during inpatient treatment. In addition, to the best of our knowledge, there is so far no research using both ORS and SHS measures in the inpatient substance abuse treatment context. However, the results obtained are in line with studies using other measures of well-being or hope and studies using either the ORS or the SHS to examine well-being and/or hope in various substance abuse treatment settings. For example, Shumway et al. (2013) obtained positive results in inpatient substance abuse treatment and its effect on hope (measured using the Herth Hope Index) in addition to readiness for change, craving, resiliency and family functioning. Regarding well-being and hope, in the 12-step groups, hope (measured using the Hopelessness Scale) had a mediating effect on health-promoting behaviours (Magura et al., 2003). The results of this study confirm the existing body of literature in an area that is still quite understudied. In addition, research has been scarce in Nordic substance abuse treatment settings.
In this study we also took a closer look at the background variables in light of ORS and SHS. We discovered several differences in how the background information of the participants is related to ORS and SHS and the change achieved. The differences found in previous admissions, gender, and living situation imply that it is vital to see the clients’ situations as a whole as well as the individual needs for improvement. The change in ORS was greater for those with previous admissions. This may have to do with clients’ expectations regarding treatment. Previous treatment periods may influence their evaluations (Kuusisto, Knuuttila & Saarnio, 2011). According to Cooney and colleagues (2003) treatment has an impact through its attraction; when the client believes in the treatment the results are better. Regarding gender, in previous studies it has been acknowledged that women generally enter treatment less often than men and there are mixed results in treatment retention and outcomes of women (Greenfield et al., 2007). In this study, women seemed to benefit from treatment more often than men in terms of their hopefulness. Also, people without regular housing, living with friends or relatives, or using different housing services achieve more positive change than do those living in more stable conditions. It may be that during inpatient treatment their basic needs, such as accommodation, nutrition and healthcare, are met and that this reflects on their evaluations of hope. Additionally, personnel may assist participants with housing-related issues.
In terms of length of treatment and treatment outcomes, the results of previous studies are mixed. For example, Condelli and Hubbard (1994) found that longer length of stay in therapeutic communities is associated with better treatment outcomes, while Harris, Kivlahan, Barnett, and Finney (2012) argue that they are not related. In the present study, the number of ORS assessments correlated positively with the changes in ORS and SHS, indicating that length of treatment may play an important role in achieving change. While the most visible change in well-being occurs in the very early phases of treatment (see Figures 2 and 3), adequate duration of treatment to stabilise obtained results cannot be overlooked.
For professionals, the existing research has found that there are prerequisites to be able to nurture hope in their clients. Working conditions within the service system affect professionals’ own hope and their ability to hope on behalf of others. In addition to using language and communication as a tool to inspire hope, helping the client with practical issues is essential (Sælør, Ness, Borg, & Biong, 2015). Monitoring the change in well-being and utilising the ORS as a therapeutic tool may in itself enhance the client’s well-being and hopefulness. Systematic evaluation of treatment outcomes is increasingly becoming a customary procedure in therapeutic treatment in order to respond to emerging requirements imposed by funders, but also to inform clinical decision-making during treatment and to enhance treatment effectiveness and client participation (Lambert et al., 2001; Lambert et al., 2003; Miller et al., 2003). Goodman et al. (2013) have addressed the need to observe effects by adopting progress monitoring in substance abuse treatment as well as in research. In this case, the treatment unit utilised progress monitoring as a therapeutic tool at the individual level and we conducted the study in order to understand the bigger picture.
Although the changes in well-being and hope were mainly positive, negative change also deserves attention. While professionals seek to help clients, some remain beyond reach. For example, it is noteworthy that in pathways thinking almost a quarter of participants experience negative change. This highlights the need to create strategies for achieving goals during treatment, and it is professionals’ task to actively envisage a different future together with clients (see Koehn & Cutcliffe, 2012, p. 85). There may be several factors behind negative change, such as suitability of community-based treatment for some clients. There is also the issue of “false hope” (Snyder, Rand, King, Feldman, & Woodward, 2002). During treatment clients may realise the difficulty of their situation, which may lead to negative experience of well-being and hope, especially at the end of treatment and near their discharge. However, the inspiration of hope may foster coping and perhaps eventually attainment of goals (Koehn & Cutcliffe, 2012). One must also bear in mind that even though treatment often provides significant help, after treatment many clients may relapse into problematic substance consumption (Allsop, Saunders, Phillips, & Carr, 1997; Kramer Schmidt et al., 2018). More research is needed on how well-being and hope change after discharge. It would also be worth studying how the levels of well-being and hope achieved are related to other treatment outcomes such as abstinence or reduced substance use.
The main limitation of this study is its rather small sample size despite 20 months of baseline data gathering. Data were collected from one treatment unit and the participation rate varied at different stages of the study. Thus, the results are descriptive even when statistically significant. The strength of this study is that both baseline information and progress monitoring were used by measuring well-being (ORS) during treatment and hope (SHS) at baseline and at the end of treatment. Several assessments on the ORS and its items shed light especially on change during treatment. Unfortunately, we had only two measuring points for hope. Thus, the extent to which we can identify a trend in this is limited. However, to strengthen our analysis of hope, we also analysed changes in agency and pathways thinking. Despite the limitations, we can conclude that treatment seems conducive to both well-being and hope. For many, it provides a solid starting point for a better future and recovery (see Robertson & Nesvåg, 2019; Shumway et al., 2013).
Footnotes
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Ekqvist has received financial support from the Finnish Concordia Fund (grant 2018). Changing expectations in clients and substance abuse treatment outcomes - research project has received financial support from The Finnish Foundation for Alcohol Studies (grant 20192020).