
Abstract
Background:
Approximately half of all young adults in Sweden are university students, and alcohol consumption is often a central part of students’ social lives. Heavy drinking is associated with negative consequences, such as poor study skills, sexual risk-taking, violence and accidents. The aim of the present study is to assess the levels of alcohol intoxication as well as hazardous alcohol use among students at Swedish universities.
Methods:
In an alcohol field study, students (≥18 years old) were randomly selected and invited to participate. The settings were eight different parties at four universities in Sweden. Alcohol intoxication was measured using a breath analyser for breath alcohol concentration (BrAC). Demographic data (i.e., sex, age, number of years at the university) and responses to the Alcohol Use Disorders Identification Test-Consumption (AUDIT-C) were gathered through face-to-face interviews for the assessment of hazardous alcohol use.
Results:
In total, 723 students were invited to participate, 605 of whom consented (84% response rate). The mean age of the respondents was 22.2 years, and the proportion of women was 37%. A majority of the respondents (91%) reported drinking before arriving at the parties. Among those who had consumed alcohol before arriving, the average BrAC was 0.086%, and 36% had BrACs of 0.100% or more. The proportion of students reporting hazardous use was 86% for women and 87% for men.
Conclusions:
This study provides the actual levels of intoxication among university students in four different cities. Alcohol intoxication and hazardous use among Swedish university students is a concern, and the university setting is an important arena for implementation of alcohol prevention strategies.
Keywords
Alcohol consumption has become an important part of student life in many ways and, for many students, is associated with an active social life with new friends and parties (Karam, Kypri, & Salamoun, 2007). At universities, there are often traditions that form the basis of a culture in which alcohol plays a central role (Russel & Arthur, 2016). Since alcohol use is a normalised and frequent activity among university students, the risks associated with binge drinking or heavy episodic drinking (i.e., heavy drinking over a short period of time) and hazardous use are elevated in this group (Andersson, Johnsson, Berglund, & Ojehagen, 2009a; Erevik, Pallesen, Vedaa, Andreassen, & Torsheim, 2017; Karam et al., 2007; Podstawski, Wesolowska, & Choszcz, 2017; White & Hingson, 2014).
A 2014 report on approximately 7,000 Swedish students showed that 31% of the men and 22% of the women reported being intoxicated at least once a month and that binge drinking was much more common in the younger age groups than the older age groups (Elgán, Gripenberg, Jalling, Källmén, & Jägerskog, 2014). Approximately 37% of the men and 29% of the women also met the criteria for hazardous or risky alcohol use, i.e., a consumption pattern that entails a risk for physical or psychological harm. Furthermore, almost one-third of the students reported that they had performed poorly in their studies because of alcohol use the day before.
Other Swedish and international studies (Andersson et al., 2009a; Karam et al., 2007; White & Hingson, 2014) have confirmed that binge drinking and hazardous use are common among students. Binge drinking and hazardous use of alcohol increase the risk of negative consequences, such as poor study skills, violence, accidents, injuries, sexual risk-taking (Grann & Fazel, 2004; Hughes, Anderson, Morleo, & Bellis, 2008; Karam et al., 2007) and alcohol dependency (Knight et al., 2002). The high levels of hazardous use and binge drinking among students should be viewed as a public health problem in Sweden as well as other countries (Andersson, Johnsson, Berglund, & Ojehagen, 2009b; Knight et al., 2002). For this reason, it is important for both individuals and society as a whole to reach this target group through alcohol prevention measures (Hennessy, Tanner-Smith, Mavridis, & Grant, 2019; Saltz, 2011).
However, to obtain a basis for alcohol prevention efforts, it is important to know how much alcohol university students actually consume and what factors are associated with consumption. Studies have measured intoxication levels among university students using biological markers, which give more reliable data than self-report measures, which lend themselves to under- or over-reporting (Clapp et al., 2006; Clapp et al., 2009; Grant, LaBrie, Hummer, & Lac, 2012; Hustad & Carey, 2005; Rossheim et al., 2017; Rossheim et al., 2016; Rossheim, Thombs, Krall, & Jernigan, 2018). A common biological marker for intoxication is breath alcohol concentration (BrAC), which is expressed as a percentage and measured with a breathalyser. Several studies have measured BrACs among university students, demonstrating varying results. For instance, international studies have shown the average BrAC to range from 0.087% to 0.100% in this group (Legrand, Goma-i-Freixanet, Kaltenbach, & Joly, 2007; Quigg, Hughes, & Bellis, 2013). A Swedish study from Lund University revealed similar results in that the median level among students was 0.084% (Johnsson & Berglund, 2003). Many studies have used well-defined thresholds for distinguishing a higher from a lower level of intoxication. These thresholds are often based on driving laws defining limits for driving under the influence (DUI) due to some degree of impairment (T. L. Martin et al., 2013). For instance, many studies conducted in the US have used a blood alcohol concentration (BAC) threshold of 0.080% since it is the legal driving limit for drivers 21 years or older (see, for instance, Lac & Donaldson, 2016; R. J. Martin, Chaney, & Cremeens-Matthews, 2015; Rossheim et al., 2017; Rossheim et al., 2016; Rossheim et al., 2018; Van Dyke & Fillmore, 2017). In Sweden, the legal limit for DUI is 0.020%, and the limit for gross DUI is 0.100%. Therefore, studies conducted in Sweden commonly use a threshold of 0.100% (Durbeej, Elgan, Jalling, & Gripenberg, 2017; Feltmann, Elgan, & Gripenberg, 2019; Gripenberg-Abdon et al., 2012). Studies measuring actual intoxication levels among university students are relatively rare, particularly in the Swedish context. Previous research among student populations has demonstrated that a number of factors are associated with high intoxication levels, such as preloading (Foster & Ferguson, 2014; Riordan et al., 2018), hazardous or risky alcohol use (Demartini & Carey, 2009; R. J. Martin et al., 2015), and being a relatively young student (Caudill et al., 2006; Kypri, Langley, & Stephenson, 2005). The overall aim of this study was to examine intoxication levels and hazardous alcohol use among students attending parties at universities in four different geographically dispersed cities in Sweden. The specific research questions were as follows: What is the average BrAC among university students attending student parties? What is the proportion of students with a high level of intoxication, defined as a BrAC of 0.100% or higher? What is the proportion of students reporting hazardous or risky alcohol use? Which factors are associated with a higher BrAC among students?
Methods
This study was a cross-sectional alcohol field study, and the data were collected during one weekend in November 2016. The settings were eight parties held by student unions on university campuses in four different large, geographically dispersed university cities in Sweden: Gothenburg, Linköping, Stockholm and Umeå. The participants were student partygoers at least 18 years of age (i.e., the legal drinking age in Sweden). The study was approved by the Regional Ethical Review Board in Stockholm (registration no. 2016/1787-31). All participants were verbally presented with information about study participation and an informed consent statement.
Measurements
The data were collected using a face-to-face interview developed by our research group. The interview contained questions on the participant’s sex, age, number of years at the university, and number of standard drinks consumed prior to attending the party; the time of measurement; and whether the participant had been denied alcohol service at the party; as well as the questions from the Alcohol Use Disorders Identification Test-Consumption (AUDIT-C) (Bohn, Babor, & Kranzler, 1995; Bush, Kivlahan, McDonell, Fihn, & Bradley, 1998). The AUDIT-C contains the following three questions and response options pertaining to the past 12 months: How often do you have a drink containing alcohol? (never = 0 points, monthly or less = 1 point, 2–4 times a month = 2 points, 2–3 times per week = 3 points, 4 or more times a week = 4 points); How many drinks containing alcohol do you have on a typical day when you are drinking? (1–2 = 0 points, 3–4 = 1 point, 5–6 = 2 points, 7–9 = 3 points, 10 or more = 4 points); How often do you have six or more drinks on one occasion? (never = 0 points, monthly or less = 1 point, 2–4 times a month = 2 points, 2–3 times per week = 3 points, 4 or more times a week = 4 points). The range of the total possible score is 0–12 points, and the threshold for hazardous or risky use is five or more points for men and four or more points for women (Gual, Segura, Contel, Heather, & Colom, 2002). Actual intoxication levels, expressed with BrAC, were measured using a breathalyser (Dräger Alcotest 6820, Drägerwerk AG & Co. KGaA, Germany). Results from similar breathalyser models have been shown to be reliable when compared to blood samples (Roiu et al., 2013) and the model used in the current study is the same as that used by the Swedish police.
Procedure
Before data collection, all student unions were contacted to gain permission for conducting the study. All research staff were trained in the methodology prior to data collection. The research staff gathered well ahead of each party to review the procedure and were divided into teams of three (1−2 teams per party), where one team member was responsible for recruiting participants and the other two conducted the interviews and BrAC measurements.
Data collection was performed between 21:00 and 03:00 at data collection sites inside the party venues near the entrances. The participants were randomly selected using a methodology in which every third person passing an imaginary line at each measuring station was invited to participate. If the person was part of a larger group, everyone in the group was invited to participate to minimise refusal rates. If a person declined participation, he or she was treated as a dropout, and the recruiter recorded the person’s sex and estimated age. Verbal approval was considered consent to participate in the study.
The participants were first asked to rinse their mouth with water and then to complete the face-to-face interview including the BrAC measurement. If a participant expressed any concerns regarding his or her alcohol use, the person was provided with an informational brochure on where to find further information and receive support.
Analysis
Descriptive statistics, e.g., the means, standard deviations (SDs), frequencies and ranges, were computed for participant sex, age and BrAC. In addition, chi-square tests (χ2) were used to test the differences in the proportions of each sex and hazardous alcohol use among the four data collection sites as well as the proportion of hazardous use versus sex. Independent samples t-tests were used to test the BrAC differences between the sexes and between those who did and did not report risky use, and one-way analyses of variance (ANOVA) with Tukey post hoc tests were used to compare both the mean age and mean BrAC versus the four data collection sites. Multiple linear regression was conducted to explore which factors were associated with a higher BrAC. Here, the continuous dependent variable was the BrAC, while the independent variables included in the analysis were the time of measurement (coded in one-hour intervals), age of the participant, number of standard drinks consumed before arriving at the establishment, total score on the AUDIT-C, and number of years enrolled at the university. All analyses were computed using SPSS, version 23. For all analyses, a P-value <0.05 was used to define statistical significance.
Results
To avoid identifying individual student unions or cities, the locations for data collection are hereafter referred to as Cities 1, 2, 3 and 4. In total, 723 individuals were invited to participate, 605 of whom consented to participate, yielding a total response rate of 84%. Of the total number of participants, 19% participated in City 4, 19% participated in City 2, 30% participated in City 3 and 32% participated in City 1. The proportion of women was 37% (n = 217), and among the participants, there was a statistically significant difference in the sex distribution between the cities, with the lowest proportion of women in City 4 (13%) and the highest in City 1 (43%; χ2(3) = 20.18, p < 0.001). The mean age of the respondents was 22.2 years (SD = 2.2, range = 18−33 years), and there was a statistically significant difference in the age distribution across the cities, with the lowest mean age in City 3 (M = 21.6, SD = 1.9) and the highest in City 4 (M = 23.2, SD = 2.4; F(3, 601) = 14.83, p < 0.001).
Measured intoxication levels
The vast majority of the participants (90%, n = 545) reported that they had consumed alcohol before arriving at the venue (i.e., preloading), and the average number of standard drinks reportedly consumed was 5.3 (SD = 2.7, range 0.5−15.0). The measured BrAC levels ranged from zero to 0.240%, and the mean total values and mean values for each data collection site are shown in Table 1. There were no significant sex differences. There were significant differences between the cities, as City 4 had the lowest average BrAC level at 0.063%, and Cities 2 and 3 both had levels of 0.084%.
Mean breath alcohol concentrations (BrACs) (%) and proportions (%) of participants with high intoxication levels and hazardous alcohol use.
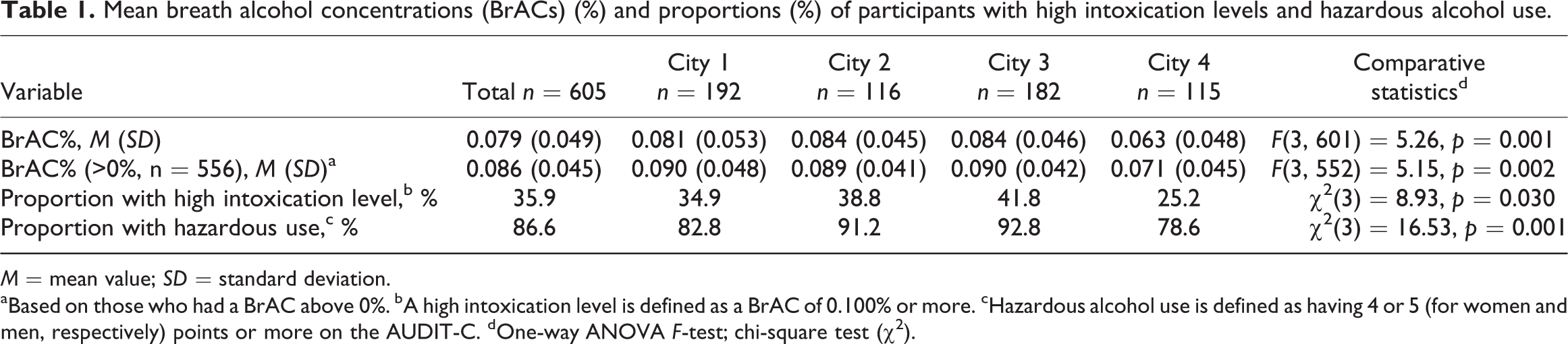
M = mean value; SD = standard deviation.
aBased on those who had a BrAC above 0%. bA high intoxication level is defined as a BrAC of 0.100% or more. cHazardous alcohol use is defined as having 4 or 5 (for women and men, respectively) points or more on the AUDIT-C. dOne-way ANOVA F-test; chi-square test (χ2).
The proportion of participants with BrACs of zero was 8% (n = 49), while the proportion with BrACs over zero but below 0.100% was 56% (n = 339). Among the latter, the average BrAC was 0.057% (SD = 0.25). The proportion of participants with BrACs of 0.100% or more, indicating a high intoxication level, was 36% (Table 1), among whom the average level was 0.131% (SD = 0.28). There was also a significant difference between the cities with regard to the proportion of participants with a high intoxication level, as City 4 had the lowest proportion, at approximately 25%, and City 3 had the highest proportion, at approximately 42% (Table 1).
Self-reported alcohol use and hazardous alcohol use
The most common pattern among both female and male students was alcohol consumption 2−4 times a month (54% and 49% for women and men, respectively), followed by 2−3 times a week (32% and 41%). However, these differences between sexes were not statistically significant (p = 0.054, two-tailed Fisher’s exact test). Of those students who reported consuming alcohol, most reported consuming 5−6 drinks per occasion. A larger proportion of men than women reported that they usually consumed 7−9 drinks or 10 or more drinks per occasion (30% vs. 17% and 17% vs. 3%, respectively, p < 0.001, two-tailed Fisher’s exact test). A larger proportion of women than men reported usually consuming 3−4 drinks per occasion (37% vs. 22%, respectively, p < 0.001, two-tailed Fisher’s exact test).
In response to the question about how often they consumed six or more drinks in a single occasion, a statistically significantly larger proportion of women than men responded that they never did so (8% vs. 2%, respectively) or did so less than once a month (28% vs. 16%), p < 0.001, two-tailed Fisher’s exact test. Moreover, a larger proportion of men than women reported that they consumed six or more drinks in a single occasion every week (44% vs. 30%, respectively, p < 0.001, two-tailed Fisher’s exact test).
By using the total AUDIT-C scores and the thresholds of 4 points for women and 5 points for men (Gual et al., 2002), the proportion of individuals engaging in hazardous or risky alcohol consumption could be estimated. The proportion of women reporting hazardous use was 86%, and the proportion of men was 87%, which were not significantly different (χ2(1) = 0.135, p < 0.713). For women, the mean BrAC among those reporting hazardous use was 0.081% as opposed to 0.038% for those below the threshold for hazardous use, and this difference was significant (t(215) = 4.71, p < 0.001). The same pattern was observed for men, with those reporting hazardous use having a mean BrAC of 0.087% and those with no hazardous use having a mean BrAC of 0.045% (t(374) = 5.82, p < 0.001). Regarding the total proportion of participants reporting hazardous use, as seen in Table 1, there was a significant difference between the cities.
A total of eight people (1%) reported that they had been denied alcohol service during the evening. All of these participants reported that they had preloaded before arriving at the establishment, and their mean BrAC was 0.123%. All had AUDIT-C scores indicating hazardous use.
Factors associated with higher intoxication levels
As revealed in Table 2, the results from the regression analysis showed that the following factors were associated with a higher BrAC: fewer years at the university (p = 0.009), a higher age (p = 0.001), higher alcohol consumption before coming to the venue (p < 0.001), the time of measurement being later at night (p = 0.013) and a higher AUDIT-C score (p < 0.001). The regression model was statistically significant (F(5, 530) = 24.44, p < 0.001) and explained 18.7% of the variance in the outcome.
Factors associated with participant breath alcohol concentration (BrAC), assessed by linear multiple regression (n = 530).
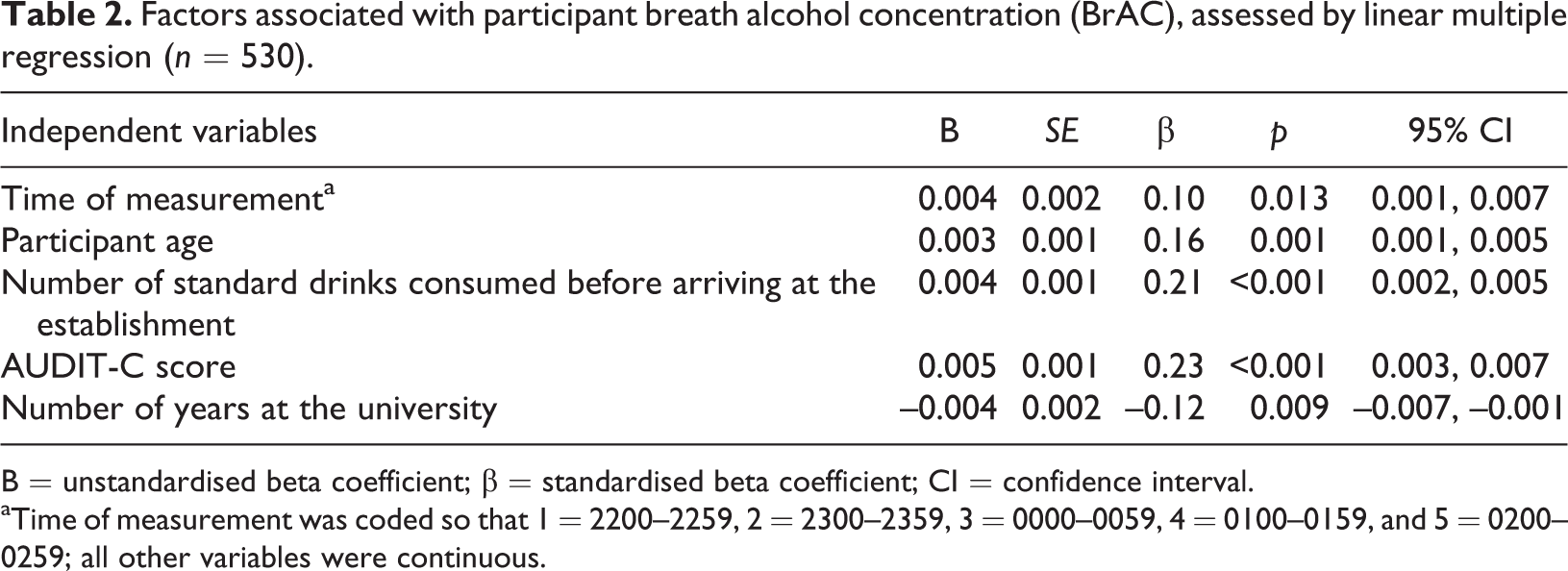
B = unstandardised beta coefficient; β = standardised beta coefficient; CI = confidence interval.
aTime of measurement was coded so that 1 = 2200–2259, 2 = 2300–2359, 3 = 0000–0059, 4 = 0100–0159, and 5 = 0200–0259; all other variables were continuous.
Discussion
The purpose of this alcohol field study was to examine intoxication levels and hazardous alcohol use among university students. The results show that the students’ average BrAC was 0.079% or 0.086%, depending on whether those who had not consumed alcohol were considered, and there was no significant difference in the average BrACs between women and men. Furthermore, 36% of the participants had BrACs of 0.100% or higher, indicating high intoxication levels. In fact, the limit for DUI in Sweden is 0.020%, but at 0.100%, when a person generally starts to experience impairments in speech, vision, motor control and balance, the crime is considered gross. These results are in line with the observations in a study from 2003 among students at Lund University in Sweden (Johnsson & Berglund, 2003), in which students’ median BrAC was 0.084%, and 38% of participants had BrACs of over 0.100%. Our results are also comparable to those of a recent US study in which the mean BrAC was found to be 0.086% among a sample of bar-attending college students (R. J. Martin et al., 2015). However, a relatively higher BrAC (mean BrAC = 0.100%) was observed in Sweden among young adults attending an event at a so-called “party cruise” (Gripenberg-Abdon et al., 2012). Furthermore, the results of the present study reveal that the total proportion of participants who self-reported risky alcohol use was 87% for the whole group. This proportion is comparable to that in the study by Martin et al. (2015), in which 87% of bar-attending college students met a lower threshold for risky use, i.e., 3 AUDIT-C-points for women and 4 points for men, as opposed to 4 and 5 points used in the current study. Our results are also consistent with those of the aforementioned study performed on a party cruise, where the proportion of consumers reporting risky use, according to the same threshold as in the present study, was 78% (Gripenberg-Abdon et al., 2012). However, our results are much higher than those presented in an earlier Swedish report (Elgán et al., 2014), in which the proportion of respondents exhibiting risky use was 37% for male students and 29% for female students. This difference may be explained by the fact that the studies used different samples. The current study included students attending student parties. These students may have had different alcohol consumption habits than the students included in the study by Elgán et al. (2014), comprising a general student population of more than 7,000 respondents. The mean BrAC among students reporting hazardous use was 0.081% for women and 0.087% for men. Interestingly, these values are above the legal driving limit for both sexes used in the US and are associated with some degree of impairment (T. L. Martin et al., 2013).
The results also show that the following factors were associated with a higher BrAC: fewer years at college, a higher age, higher alcohol consumption before coming to the venue, a time of measurement later at night, and a higher AUDIT-C score. The results are in line with those of earlier research demonstrating that self-reported hazardous use is associated with high BrAC (Demartini & Carey, 2009; R. J. Martin et al., 2015). There is also support for the idea that having spent fewer years at college is related to higher intoxication levels (Caudill et al., 2006), which in turn supports the hypothesis of a maturity effect, i.e., that students consume more alcohol during their first years as students and then gradually decrease their consumption of alcohol over time (Vik, Cellucci, & Ivers, 2003). In line with this, earlier studies have demonstrated that higher intoxication levels are more common among younger students (Caudill et al., 2006; Kypri et al., 2005). However, this finding is to some extent contradicted by the results in the present study, which found an association between higher age and higher intoxication levels. One explanation may be that some students are enrolled at universities at a relatively older age, which also means that older students do not necessarily need to have been enrolled at the university for a longer time period than younger students.
Further, our findings show that over 90% of participants had consumed alcohol before coming to the parties and that they had, on average, consumed more than five standard drinks. Preloading before attending the parties and a time of measurement later at night were associated with higher intoxication levels in earlier studies (Beirness, Foss, & Vogel-Sprott, 2004; Pedersen & Labrie, 2007). A recent field-based study by Chaney and co-workers in a college bar district in the US demonstrated that for every standard drink consumed before coming to the bar district, there was a 0.014% increase in BrAC among the participants (Chaney et al., 2019). Our study found a smaller association; for every standard drink consumed, there was a 0.004% increase in BrAC. Nonetheless, most factors explaining higher levels of intoxication among students in this study have been identified as explanatory factors in earlier research (Beirness et al., 2004; Caudill et al., 2006; Demartini & Carey, 2009; Kypri et al., 2005; Pedersen & Labrie, 2007; Vik et al., 2003).
Studies measuring actual alcohol intoxication levels using biological markers among students in a university setting are relatively rare, particularly in the Swedish context. Our study primarily adds to the existing literature by providing the actual levels of intoxication among students in a university setting in four different Swedish cities.
There are a number of limitations and strengths of this study. Some of the self-reported data were collected from students with high intoxication levels. Their intoxication might have affected their cognitive functioning, judgement and memory, which could have contributed to a lower capability to provide reliable responses during the face-to-face interview. However, these self-reported data were combined with the collection of biological sampling, which is not affected by self-report bias. Furthermore, the current study examined intoxication levels and hazardous alcohol use at four different universities in Sweden; thus, the generalisability on a national and international level could be questioned. Notably, the cut-offs for defining hazardous alcohol use may have been slightly low, especially since the timeframe of consumption of six standard drinks during one drinking occasion is not included in the AUDIT-C (Jackson, 2008; Read, Beattie, Chamberlain, & Merrill, 2008). One strength that should be mentioned is the high response rate of 84%. Another strength is that participants were randomly invited to be included in the study. Finally, we used AUDIT-C, a valid and reliable measurement to assess hazardous alcohol use (Rumpf, Wohlert, Freyer-Adam, Grothues, & Bischof, 2013).
The current study implies that students at Swedish universities might benefit from prevention measures to reduce alcohol consumption and alcohol-related problems. A community-based approach to alcohol prevention, including components such as community mobilisation, server training, and improved enforcement, could be an important contribution. For instance, our research team at the STAD unit previously developed an alcohol prevention model for the nightlife setting. Evaluations of this model, which is a community-based alcohol prevention programme including responsible beverage service training, have shown that service of alcohol to both obviously intoxicated and underage partygoers has decreased along with nightlife-related violent crimes (Wallin & Andreasson, 2004; Wallin, Gripenberg, & Andréasson, 2002, 2005; Wallin, Lindewald, & Andreasson, 2004; Wallin, Norström, & Andréasson, 2003). This model has also been adapted for graduation parties at secondary schools, and an evaluation showed that the number of violent crimes decreased by 23% (Ramstedt, Leifman, Muller, Sundin, & Norstrom, 2013). Moreover, a Swedish study at four universities showed that alcohol prevention measures, including the training of bar staff, had effects on the proportion of students with risky alcohol habits. The study concluded that much can be gained from such efforts (Statens Folkhälsoinstitut, 2010). The fact that only eight individuals in this study were denied alcohol service at the student parties, while 36% of participants had an average BrAC of 0.100% or more, suggests there is a need to have the serving staff trained in responsible beverage service (RBS). Thus, we propose that in order for establishments at colleges or universities to have an alcohol licence, there should be a strong recommendation or a condition from their licensing boards to have alcohol-serving staff participate in RBS training. In fact, a national study conducted by our research group demonstrated that student union representatives had positive attitudes towards alcohol prevention in the student union setting (Strandberg, Elgán, Jägerskog, & Gripenberg, 2018). The same study also showed that approximately 80% of the student unions had a written alcohol policy. Future research should expand the knowledge base to include alcohol purchase observations using pseudo-intoxicated actors attempting to purchase alcoholic beverages at licensed premises at universities and colleges. The testing of an alcohol prevention intervention such as RBS training would also be a reasonable next step for future research.
Conclusions
This study provides data on the actual levels of alcohol intoxication among university students attending university campus parties in four different Swedish cities. The levels of intoxication and rate of hazardous use among university students visiting campus parties were high, and several factors, such as preloading and a risky consumption, were associated with higher levels of intoxication. Alcohol use among students can therefore be regarded as a substantial public health problem. Further, the results imply that Swedish university students, particularly in the setting of student union festivities, are a group who can benefit from prevention measures to counteract high alcohol consumption and alcohol-related problems. Efforts such as the STAD model for alcohol prevention, including for instance RBS training, could be an important contribution in this context.
Footnotes
Acknowledgements
We would like to express gratitude to the student unions that allowed us to conduct this study on their premises. We are also grateful for the contributions of colleagues and external staff to the data collection.
Declaration of conflicting interests
The authors declare no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: grants from Stockholm County Council. The funding institution was not involved in planning the study design, collecting the data, writing the manuscript or deciding to submit the article for publication.