
Abstract
Background:
While homelessness and problem gambling are both recognised as social and public health concerns and the prevalence of addictive disorders among homeless populations tends to be high. These questions have been studied predominantly independently.
Aim:
The aim of the study was to explore the co-occurrence of the two phenomena among the homeless population using shelters and night shelters in Warsaw, and, more specifically, to provide information about the forms and frequency of gambling in this homeless population.
Method:
Homeless persons (N = 690) were interviewed in rehabilitation-shelters (n = 17) and night-shelters (n = 2) in Warsaw from November 2015 until January 2016. The core component of the questionnaire was a screening test (Problem Gambling Severity Index). In addition, data regarding the intensity of gambling and various types of games or settings were collected.
Results:
The prevalence of problem gambling in this population of homeless people was 11.3%, whereas the prevalence of problem gambling in the general population in Poland is much lower (0.7%). Similarly to the general population, the most prevalent gambling games in the homeless population were lotteries; however, homeless people gambled in lotteries almost three times more often compared to the general population.
Conclusions:
This is the first study examining the prevalence of problem gambling in the homeless population in Poland. The findings of the study suggest that problem gambling among the homeless is a significant social and public health concern. High rates of problem gambling in the homeless population show the need to identify and monitor this problem in shelters and consequently to provide easier access to gambling treatment or prevention programmes.
There are more than 400,000 homeless people in the European Union. It is known that the causes of homelessness stem from an interaction between such individual factors as poverty, family problems, mental health issues, and substance misuse problems on the one hand, and structural factors, mainly the availability of low-cost housing (Fazel, Geddes, & Kushel, 2014), on the other. Contrary to other Western European countries, research on homelessness in Poland has a very short history. According to Marxist theory, which was a dominating framework until 1989, homelessness was to disappear as soon as a socialist society was built. As a result, the issue was absent from the public debate in post-war Poland. It gained attention only after the collapse of the Soviet Bloc and the political transformation in 1989, but the legal definition of homelessness was introduced in Poland as late as the year 2000 (Pindral, 2011). In 2015, the number of homeless people in Poland reached 36,161. Of these, 37% were living in the 18 biggest cities (n = 13,428) while the rest lived in smaller cities and towns. In 2015, the capital city of Warsaw (population 1,754,000) had the highest absolute number of homeless persons (n = 2516). In comparison, in Bydgoszcz (with a population of 355,000) the number was 1436, and in Szczecin (with a population of 405,000) the number was 1176 (MPiPS, 2015).
Research has stressed the heterogeneity of homeless populations and suggested different subtypes of homelessness. For example, Przymeński (1998) differentiates between shelter and non-shelter homelessness, arguing that institutionalised (shelter) homeless show less dissocial behaviour, are less often involved in harmful drinking or drug use, and more often make efforts to overcome their life crises. Pindral (2011) maintains that the differentiation between shelter and non-shelter homelessness is too static, as periods of living on the streets and in various forms of shelters are often intertwined. Polish data from 2015 show that 60% of the homeless population stayed in rehabilitation shelters and night shelters, 4% in healthcare institutions, 6% in prisons and detention, less than 1% in sobering-up stations – and 29% “on the streets” (squats, garden sheds, and other places not suitable for residence) (MPiPS, 2015).
Rehabilitation shelters and night shelters are two different types of institutional settings offering help to the homeless population in Poland. Residents of rehabilitation shelters are obliged to follow certain rules: to perform different work tasks for the shelter, follow individual plans of overcoming homelessness prepared by the rehabilitation shelter staff (psychologists and social workers), pay a (symbolic) rent for staying, and maintain abstinence from alcohol and drugs. The night shelter rules are less strict, but the clients stay there only for short periods of time. Night shelters are places where the homeless people are allowed to spend time between 7:00 p.m. and 7:00 a.m. but no more than three nights in a row. The main rule of conduct is that one has to be sober to be admitted; however, this rule is not enforced during wintertime.
Homeless people have higher rates of premature mortality than the rest of the population, especially from suicide and unintentional injuries. Also, they suffer from an increased prevalence of a range of infectious diseases, mental disorders, and substance misuse (Fazel et al., 2014). Moreover, without support, homelessness will quickly cause the individual’s health status to deteriorate, and vice versa, poor health will further reinforce homelessness (Dai & Zhou, 2018).
Similarly to the studies of homelessness, social scientific research on gambling is also in an early phase in Poland. The first general population survey conducted in 2011 showed that 23.5% of the respondents (15 years or older) gambled at least once during the 12 months prior to the study. The second survey conducted in 2014 showed that 34.2% of the respondents (15 years or older) gambled at least once, and 7.1% at least a few times a week during the 12 months prior to the study. As the second survey used a modified methodology, the discrepancies in frequency may not reflect an increase but are possibly attributed to varying formulations of the items measuring gambling behaviour (CBOS Report, 2012, 2015). However, the ranking order of popularity of particular forms of gambling has not changed between these two surveys. Lotteries were the most popular games, followed by scratch cards, SMS lotteries, and slot machines (CBOS Report, 2012, 2015).
A recent US study estimated that between 1% and 2% of adults and between 3% and 5% of youth meet the clinical criteria of a gambling disorder (Nower, Eyrich-Garg, Pollio, & North, 2015). In Poland in 2011, 3.7% of respondents scored at least one point on the scale of the Problem Gambling Severity Index (PGSI) screening test, and 0.2% met the criteria for problem gambling. In 2014, 5.3% of Poles scored at least one point on the PGSI, and among them almost 4% indicated a low level of risk (1–2 points), 0.7% a moderate risk level (3–7 points), and 0.7% indicated problem gambling (8 and more points) (CBOS Report, 2012, 2015). The prevalence rate of problem gambling in Poland is thus similar to that in other European countries: 0.6% in Germany and Finland, 0.7% in the United Kingdom and Norway, and 0.9% in Sweden (Calado & Griffiths, 2016; Erbas & Buchner, 2012; Wardle et al., 2011). A comparison of the results from 2011 and 2014 shows that the number of at-risk gamblers decreased in big cities and increased in rural areas. Moreover, gambling problems were more prevalent among men and in the group with a lower educational level (CBOS Report, 2015).
While homelessness and problem gambling are recognised as social and public health concerns (Holdsworth, Tiyce, & Hing, 2011; Lorains, Cowlishaw, & Thomas, 2011; Odlaug, Stinchfield, Golberstein, & Grant, 2013; Reardon, Burns, Preist, Sachs-Ericsson, & Lang, 2003) and the prevalence of addictive disorders among the homeless population tends to be high (Shaffer, Freed, & Healea, 2002), these areas of research have predominantly been studied independently (Sharman, Dreyer, Aitken, Clark, & Bowden-Jones, 2015). To provide evidence for the co-occurrence of these phenomena and to assess the relative importance of comorbidity, recent studies in the US, Canada, and the United Kingdom have focused on the estimation of the prevalence and rates of problematic gambling in homeless populations (Matheson, Devotta, Wendaferew, & Pedersen, 2014; Nower et al., 2015; Sharman et al., 2015; Sharman, Dreyer, Clark, & Bowden-Jones, 2016). These studies support an assumption of relatively high rates of comorbidity compared to the general population. A study conducted in the US in 2002 shows that “the levels of gambling disorders among the homeless with a history of substance abuse who sought treatment are higher than those in the general adult population” (Shaffer et al., 2002, p. 1115). A more recent American study based on a sample which also included homeless persons recruited on the streets and which used more differentiated diagnostic instruments showed a 12% (n = 33) correspondence with the South Oaks Gambling Screen (SOGS) criteria for gambling disorder, and a 46% (n = 127) prevalence of at least one symptom of problem gambling (Nower et al., 2015). Similarly, lifetime prevalence rates among clients of the Canadian homeless service agencies – with 10% of the clients reaching problem gambling prevalence – have been qualified as “alarmingly high” (Matheson et al., 2014, p. 537). The results of the most recent study from the United Kingdom also show “significantly higher rates of problem gambling in a service-accessing homeless population compared to the general population in the UK” (Sharman et al., 2015, p. 530). Despite growing research in this area, the cross-country comparability of data is limited due to differences in the sampling procedures, sample size, and use of different screening instruments (Griffiths, 2015).
This article presents data from the first study conducted in Poland and also in Central and Eastern Europe regarding prevalence of gambling in a homeless population. (The phenomenon has not been researched in the Nordic countries, either). The aim is to explore the co-occurrence of the two phenomena among the homeless population using shelters and night shelters in Warsaw, and more specifically to provide information about the forms and frequency of gambling in this homeless population.
Methods
Sample selection
The phenomenon of homelessness can be operationalised in different ways. In this study, we have focused on institutionalised homelessness, that is, on the population without regular residence, staying at rehabilitation shelters or night shelters. A quantitative self-report survey was conducted in the rehabilitation shelters and the night shelters in Warsaw during two weeks in November 2015 and one week in January 2016. The winter is an especially suitable time for this type of study, as there is high access (especially via night shelters) to a more heterogeneous homeless population (including street homeless and homeless from smaller towns and rural areas) in these institutions. The severe cold motivates the street homeless to look for warm shelter, and therefore the night shelters organise additional space during wintertime (about 15% more places) and offer low-threshold places for those who are under the influence of alcohol (low-threshold accommodation constitutes about 9% of the accommodation offered to homeless people during the winter) (MPiPS, 2015). Of all the Warsaw rehabilitation shelters and night shelters, 87% participated in the study (17 rehabilitation shelters, two night shelters). The number of beds in Warsaw’s rehabilitation shelters varied between 15 and 112, while Warsaw night shelters had a much bigger capacity with between 100 and 300 beds each.
The interviewers approached every person present in the facility during their evening shift. If the respondents agreed to be interviewed, they were given an individual code, which allowed us to eliminate potential overlaps. In total, we identified 23 cases of overlapped subjects, included the first set of data in the sample, and eliminated the second. Frequent changes of residence between different shelters could lead to the researchers reaching out to the same persons in different institutions. This possible overlap has to be taken into consideration in the recruitment (Sochocki, 2010). To lower the risk of overlaps, two groups of seven interviewers collected the data during a short period of time, each group having shifts during the evening in one of the rehabilitation shelters or night shelters. The interviewers were students of psychology and social street workers in the field of harm reduction and were experienced in reaching hard-to-reach populations. They received an additional two-hour training by the study’s investigators.
The respondents (N = 690) met the following eligibility criteria: (a) minimum age of 18 years, (b) lack of stable residence, (c) current residents of Warsaw rehabilitation shelters or night shelters, and (d) capable of giving informed consent to participate in the study. The interviewers assessed each respondent’s condition and ability to interact, but did not conduct sobriety tests. However, those respondents who were noticeably under the influence of psychoactive substances and/or were not able to provide informed consent were excluded from the study. We did not monitor the number of refusals or the level of inability to participate in the study.
Measures
Each interview took approximately 10 minutes. The core component of the questionnaire was a nine-item screening test, the Problem Gambling Severity Index (PGSI) based on the Canadian Problem Gambling Index (CPGI). Zero points on the scale is interpreted as no problem gambling, 1–2 points indicate low problem gambling, and 3–7 points indicate moderate problem gambling. Scores of 8 points or more indicate problem gambling (Ferris & Wynne, 2001). Additionally, the questionnaire included questions about sociodemographic characteristics (gender, age, educational level, and time spent in homelessness) and intensity of gambling, taking into account various types of gambling or settings (sport betting without using the internet, lotteries, scratch cards and lotto, slot machines, horse race betting, casinos, playing cards privately, online, etc.) during the last 12 months.
Data analysis
We analysed the data using SPSS (version 21). The single-variable analysis was applied, which allowed us to analyse the value distribution. Also, we calculated the descriptive statistics (mean, median, and standard deviation [SD]) and performed Chi-square comparisons. A p-value of <0.05 was considered significant.
The multivariate model of logistic regression was used and odds ratios were obtained to explore the relation between the sociodemographic characteristics of the homeless population and the occurrence of problem gambling. The reference groups were female for gender and university degree for education. Age was included as a continuous variable. The logistic regression analysis aimed also to explain the relation between age and frequency of various types of gambling games (intensity of play – very often). In this case age and education were adjusted and odds ratios obtained for a 10-year change.
Ethical concerns
The study sought and received ethical approval from the Bioethical Commission of the Institute of Psychiatry and Neurology in Warsaw, Poland (ref. 24/2015). Participation in the survey was voluntary, and the respondents were not paid for their participation. All respondents received an information sheet describing the research objectives, benefits and risks of participation, data confidentiality, and how to contact the researchers. Written informed consent was obtained from all respondents. Similarly to Morán-Sánchez, Luna, Sánchez-Muñoz, Aguilera-Alcaraz, and Pérez-Cárceles (2016) we have assumed that “in the absence of acute withdrawal, or intoxication, or advanced cognitive impairment, we should assume that addicted persons possess decision-making capacity. Thus, the view that people with SUD (Substance Use Disorders) would ipso facto lose decision-making power for research consent is flawed and stigmatizing” (Morán-Sánchez et al., 2016, p. 9).
As a preventive measure, and whether they experienced gambling problems or not, all respondents were given a leaflet with a helpline number offering support to individuals with gambling problems.
Sample characteristics
The vast majority of the total sample (N = 690) was male, only 10% (n = 70) were female. The average age of the respondents was 49.5 years (SD = 12.80 years). The most numerous group among respondents were people aged 35–54 years (44%, n = 302) and older than 55 years (41%, n = 284). Young adults (18–34 years) made up only 15% (n = 103) of the sample. Most participants reported vocational and secondary education (38%, n = 258 and 35%, n = 233 respectively). One fifth of the interviewees (21%, n = 139) had only completed education at primary level, and 7% (n = 45) had a university degree (see Table 1).
Respondents’ sociodemographic characteristics (percentages and frequencies).
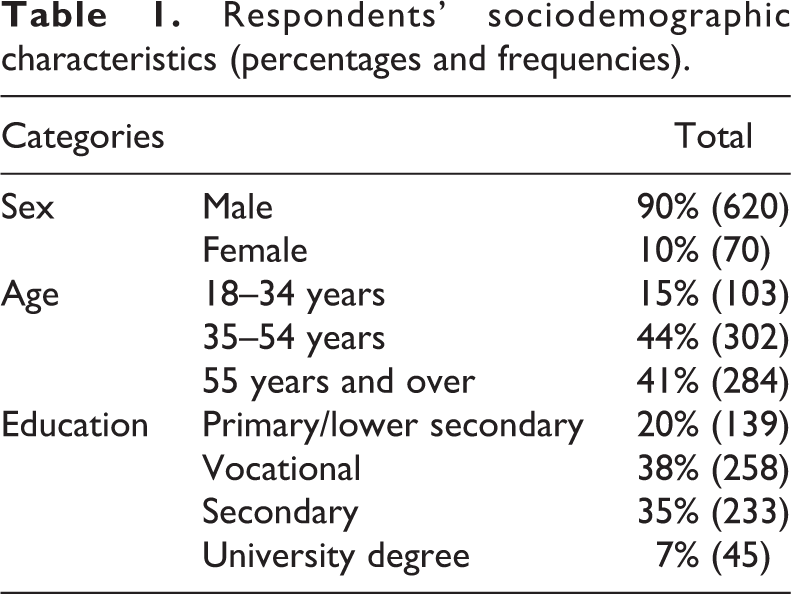
Homelessness had lasted six years on average (SD = 7.65 years): 30% (n = 207) of the respondents had been homeless for from three to nine years, 28% (n = 194) for up to a year, 25% (n = 171) had experienced long-term homelessness (above 10 years), and 13% (n = 89) had remained homeless for one to two years.
Results
Prevalence of gambling and problem gambling
The majority of the surveyed persons had not gambled during the last 12 months. However, 30.2% (n = 208) of the respondents scored more than 1 point in the PGSI screening test. Prevalence of problem gambling in the homeless population was 11.3% (n = 78). Among those who reported problem gambling, the most frequently endorsed symptoms in the PGSI screening test (response options “sometimes, often, and very often”) were: (a) gone back another day to try and win back the money they lost (95%), (b) gambling caused financial problems (90%), and (c) bet more than could be lost (89%). The least frequent symptom reported by almost three quarters (71%) of problem gamblers was that gambling had caused them health problems, including feelings of stress and anxiety.
The prevalence of problem gambling among men (12%) was higher than for women (3%, p < 0.001, see Table 2). Problem gamblers were the youngest group in the whole sample. The mean age for this group of respondents was 43.3 years (SD = 12.37), while non-gamblers (those who scored 0 points on PGSI) were the oldest group, with a mean age of 50.9 years (SD = 12.57). Problem gamblers and those who scored 0 in the PGSI screening test had most often completed vocational or secondary education. The mean time remaining in homelessness was 5.9 years for problem gamblers (SD = 8.20) and 6.2 years for non-gamblers (SD = 7.65). Both groups (problem gamblers and non-gamblers) had mainly completed vocational or secondary education (see Table 2).
Respondents’ sociodemographic characteristics from the perspective of the results obtained from the Problem Gambling Severity Index (PGSI) screening test (percentages and frequencies).
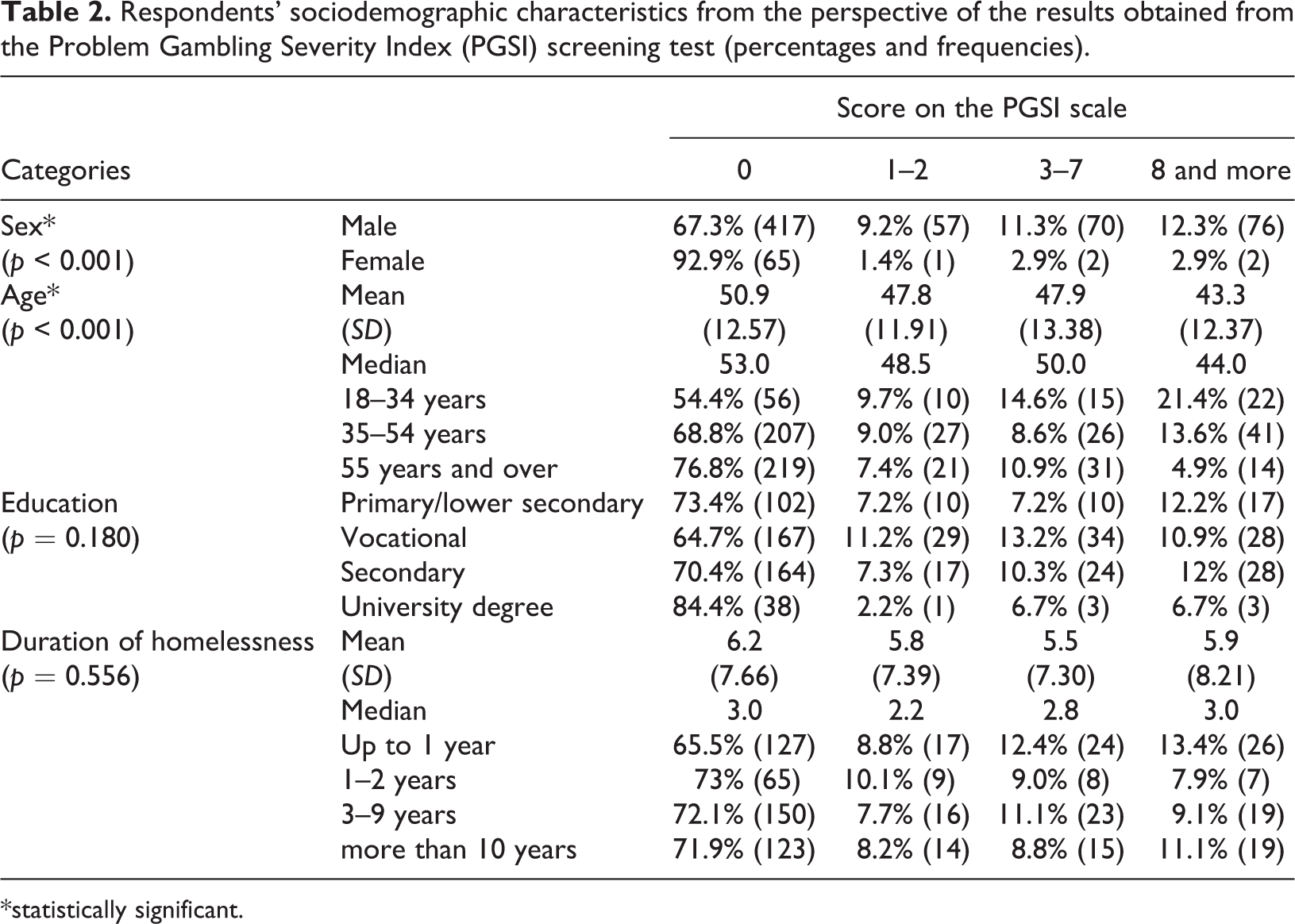
*statistically significant.
These results are confirmed by the multivariate logistic regression, which shows that homeless men had a 5.1 times higher likelihood than women to be involved in problem gambling (lower bound 1.21, upper bound 21.71). As the correlation coefficient shows, younger people achieved higher scores in the PGSI screening test. The chance of the occurrence of problem gambling decreased every 10 years by 36.3% (OR = 0.637) (see Table 3).
Multivariate model of logistic regression: Relations between gender, age and education level and occurrence of problem gambling.
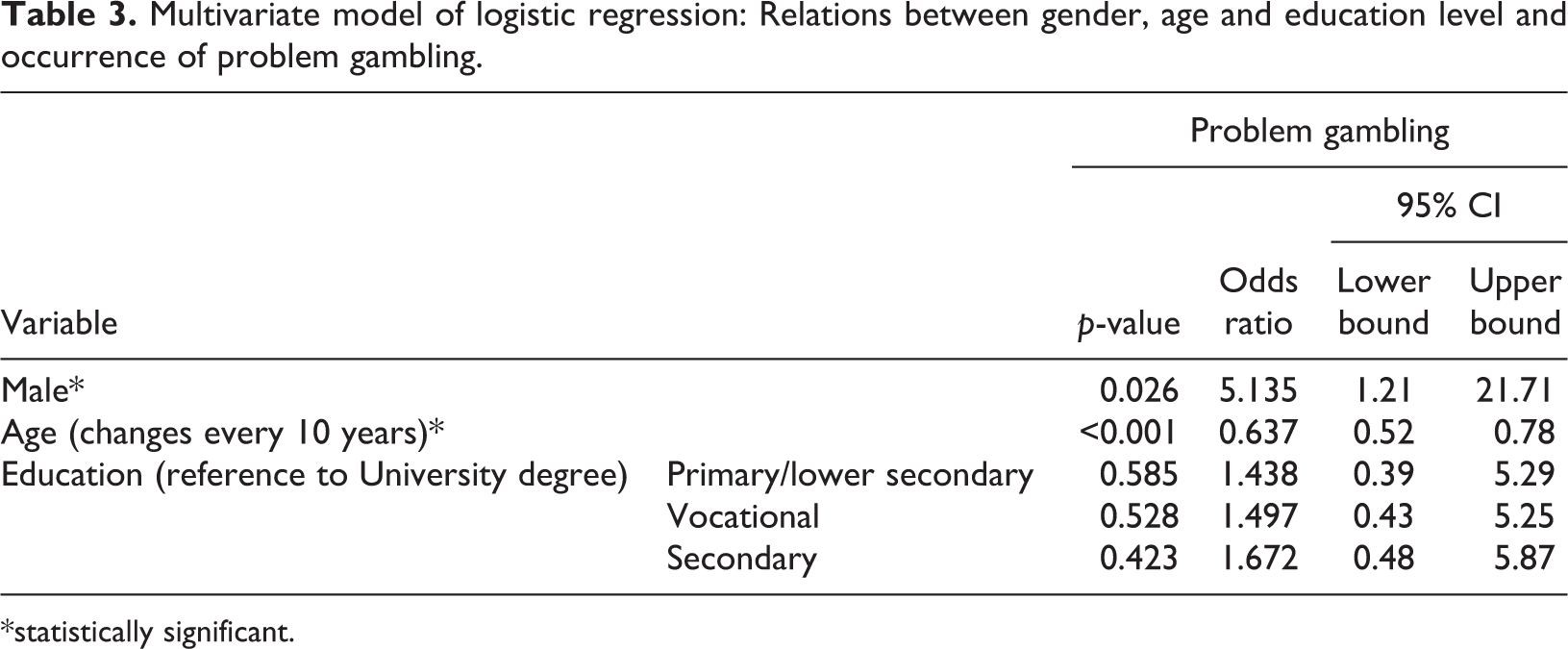
*statistically significant.
Types of gambling
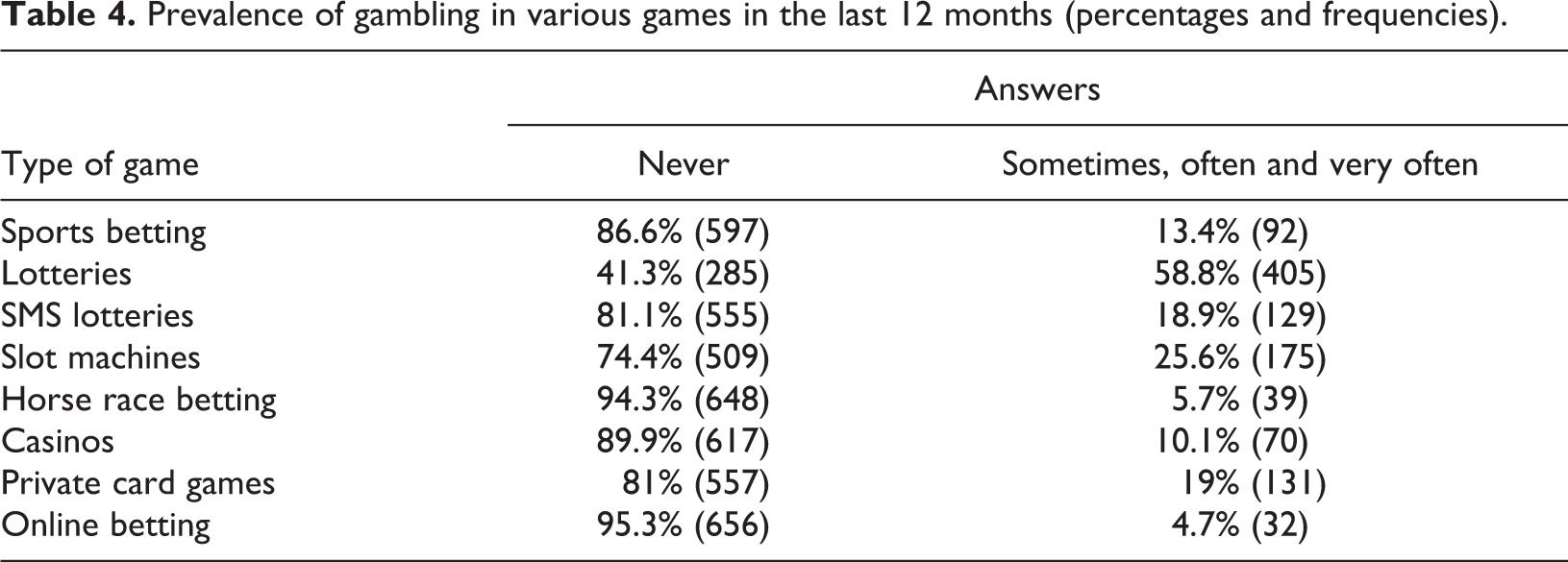
The most popular type of game in the homeless population was lotteries (numbers game, scratch cards, and lotto). Almost 60% of the respondents had gambled on lotteries during the 12 months before the study; 25.6% of respondents gambled on slot machines, and 18.9% on SMS lotteries and private card games (offline, outside casino). The least popular form of gambling were online bets (4.7%) and horse race betting (5.7%), (see Table 4). More than 40% (n = 278) of the homeless population gambled on more than one type of game during the 12 months preceding the study.
Prevalence of gambling in various games in the last 12 months (percentages and frequencies).
Chi-square analysis showed that, regardless of gender, the most popular types of gambling were lotteries (p = 0.002). Furthermore, women gambled on SMS lotteries and slot machines (p = 0.046), while men opted for slot machines (p = 0.046) and private card games (p = 0.003). The least popular game in the homeless population, regardless of gender, was online betting, but even in this category, men gambled online about three times more often than women. Correlations (R-Pearson) between gender and playing particular gambling games are weak and vary from 0.076 on SMS lotteries to 0.118 on sport betting and lotteries.
Gambling on slot machines and online betting were most prevalent among younger respondents (18–34-year-olds). Among senior respondents (55 and older), the most popular forms of gambling were lotteries, horse racing bets, and private card games. The correlation between age and playing particular gambling games was weak, varying from 0.012 on lotteries to –0.293 on slot machines.
Analysis of multivariate logistic regression shows that the intensity of gambling on SMS lotteries, slot machines, and casino games decreases with age, by 36% every 10 years. The most significant decrease of frequency of gambling was noted among internet betting gamblers (OR = 0.39). In general, the younger the gambler, the greater the chance of gambling on a particular game very often. There was no statistically significant influence of gender and education on frequency of gambling (see Table 5).
Multivariate model of logistic regression: Relations between age and frequency of gambling in various types of gambling games (very often).
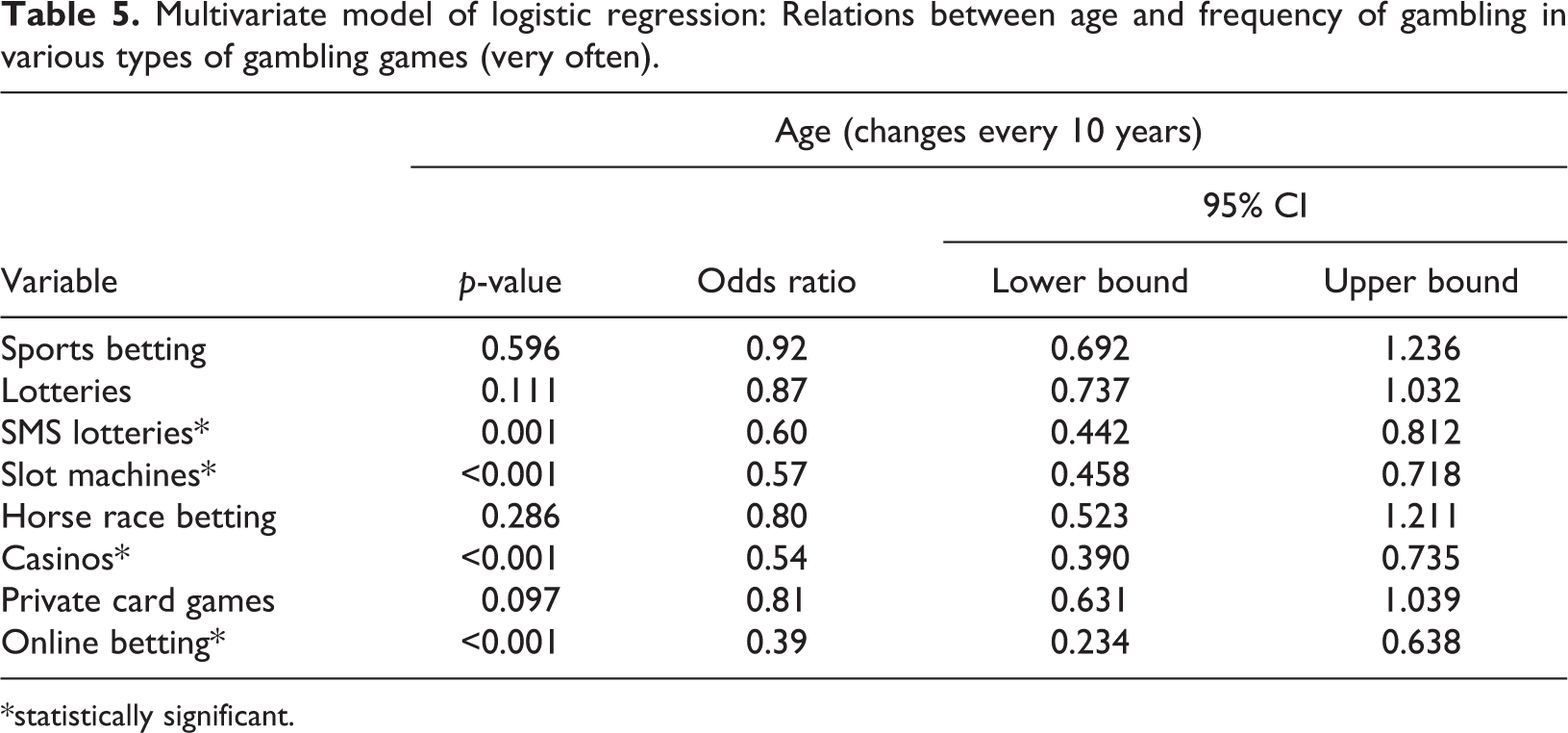
*statistically significant.
Lotteries and slot machines were the most popular forms of gambling among the respondents, regardless of their educational level. The least popular game was online betting, with the exception of the respondents with secondary education, for whom horse racing was the least likely selected game. Only the correlation between lotteries gambling and education was statistically significant (p < 0.001).
Different from the general homeless population, the most popular forms of gambling among problem gamblers were slot machines (82.1%), lotteries (76.9%), and private card games (57.1%). The least popular types of gambling were horse race betting (22.4%), online bets (23.1%), and SMS lotteries (30.3%). The analysis showed a statistical significance between frequency of gambling in various forms and prevalence of problem gambling. The lowest correlation was noted for gambling on SMS lotteries and lotteries, while the highest was for gambling in casinos, but with a strength of correlation close to 0.5 (see Table 6).
Prevalence of gambling in various gambling games in the last 12 months among non-problem and problem gamblers (percentages and frequencies).
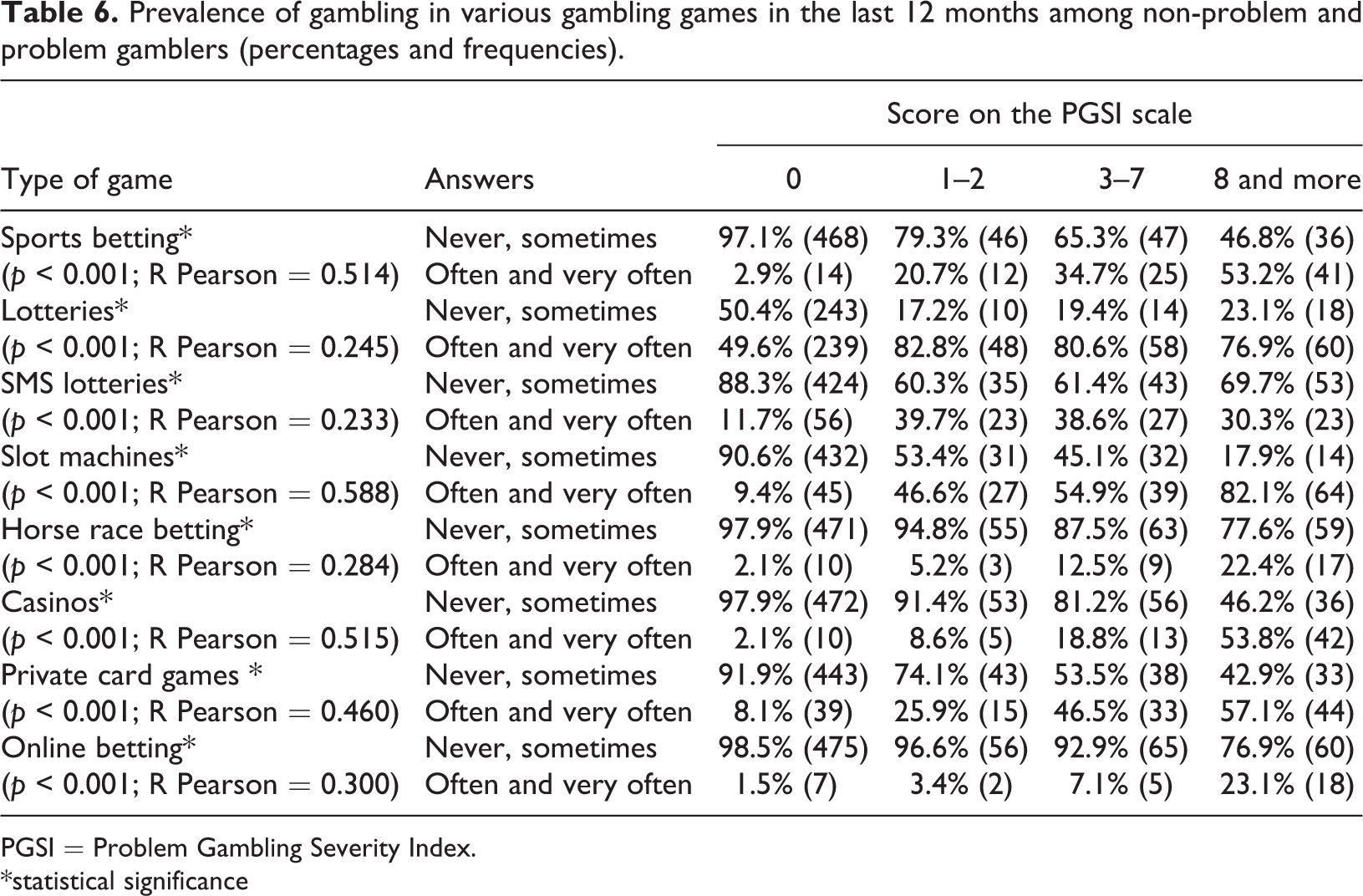
PGSI = Problem Gambling Severity Index.
*statistical significance
Discussion
This is the first study conducted in Central and Eastern Europe to provide information on the prevalence of problem gambling and frequency and type of gambling among the homeless population utilising rehabilitation shelters and night shelters in an urban setting. The results show that the prevalence of problem gambling in the homeless population amounts to 11.3%, and is 16 times higher than in the general population. The high prevalence of gambling disorders underlines the necessity to step up efforts to identify and address gambling problems among the homeless.
The significantly higher prevalence rate of problem gambling may have multiple causes. Previous research shows that problem gambling is more common among men and persons with a lower educational level (CBOS Report, 2012, 2015). Moreover, playing gambling games over a long period of time may cause debt, which leads to housing instability and homelessness (Rogers, Button, & Hume, 2005). At the same time, gambling can, by the gamblers themselves, be perceived as a way to end poverty and homelessness. Sadler (2000) suggests that, faced with poverty, individuals may undertake risky behaviours in an effort to manage poverty and improve their financial situation. A qualitative study by Marsden (2012) seems to confirm this thesis, as he identified that homeless youth saw gambling as a means to obtain money.
When comparing with results from international studies, we have to keep in mind that the validity of cross-national comparisons of results is limited by cultural and methodological differences, which hinges consequently upon the different definitions of “gambling” and “homelessness” and the acknowledgement of the high heterogeneity of these phenomena (Griffiths, 2015; Raylu & Oei, 2002). The high prevalence of problem gambling among the homeless population identified in our study confirms findings from similar studies conducted in the United States, Canada, and the United Kingdom (Matheson et al., 2014; Nower et al., 2015; Sharman et al., 2015, 2016). More specifically, in the United Kingdom the rate of problem gambling on the PGSI screening test was similar to that in our study: 11.6% (Sharman et al., 2015). A US study showed that 12% of African-American homeless individuals had gambling disorders (Nower et al., 2015). In a study conducted in Toronto, Canada, the prevalence of lifetime problem gambling (10%) and pathological gambling (25%) was even higher (Matheson et al., 2014). As Matheson and colleagues state, “the discrepancy between the prevalence of lifetime gambling problems in the general population versus that in clients of community-based services means that surveys that exclude vulnerable populations underestimate gambling problems” (Matheson et al., 2014, p. 542).
In this study, men were more likely than women to be classified as problem gamblers. Problem gamblers were the youngest group in the whole sample and most often had a lower education level. This sociodemographic characteristic of the Polish sample is consistent with characteristics of respondents from other studies on homelessness (Nower et al., 2015), but also with the profile of problem gamblers in the general population in Poland (CBOS Report, 2015). In other studies (Matheson et al., 2014; Sharman et al., 2015, 2016) the sociodemographic characteristics were not described in detail. In the studies mentioned above, only the proportion of males and females was consistent with our study. Multivariate logistic regression showed that in Poland men were at much greater risk than women of being involved in problem gambling. The younger gamblers also had a greater chance of experiencing a gambling disorder; this chance decreases every 10 years by about a third.
In addition, and as a contribution to the existing literature (Matheson et al., 2014; Nower et al., 2015; Sharman et al., 2015, 2016), our study provides detailed information about the types and frequency of gambling in homeless populations. More than 40% of the homeless population gambled more than one type of game. Similar to the general population in Poland, the most popular gambling games in the homeless population were lotteries. However, homeless people gambled on lotteries almost three times more often: 58.7% versus 20.5% noted in the general population study (CBOS Report, 2015). This may result from the high economic availability (low price of the ticket) and physical availability (large number of points of purchase) of the lotteries. Another reason for the higher prevalence of lottery gambling by homeless people may be related to the idea that winning money will help change their difficult situation and help them to leave homelessness.
The lotteries lose their popularity status when problems occur, as the nature of the gambling triggers a shift into more addictive variants. Homeless problem gamblers gambled most often on slot machines, lotteries, and private card games. The least popular were horse race betting, online bets, and SMS lotteries. These findings differ from the results of the British study where the most popular gambling games were electronic roulette machines, horse racing, slot machines, and football betting (Sharman et al., 2015). The analysis of multivariate logistic regression showed that in Poland the intensity of gambling SMS lotteries, slot machines, and casino games decreases with age by about one third every 10 years. The most significant decrease was noted among gamblers betting on the internet. In general, the younger the gambler, the greater the chance of gambling on a particular game very often, and thus the greater the chance of becoming a problem gambler.
Limitations
First, the local scope of the study limits the generalisation of our results to the whole Polish population of homeless individuals. However, homelessness is an urban phenomenon, and Warsaw offers the most extensive and most differentiated institutional support for homeless people in Poland, so much so that practitioners claim that homeless people from around the country come to Warsaw during wintertime.
Second, the study was conducted in rehabilitation shelters and night shelters, and those not under institutional care were excluded from the sample. We tried to limit this sample bias by collecting data during wintertime and by including the emergency shelters (number of beds in night shelters constituted about 35% of the total number of beds in the shelters included in the study). However, we have also pragmatically assumed that support or treatment offered to homeless people experiencing gambling problems will in the future mostly be provided by institutions.
Third, as we did not monitor refusals to participate in the study, we were unable to calculate the response rate. However, the sociodemographic profile of the study sample matches the characteristics and the profile of the homeless population in Poland (gender, education, age, time in homelessness). In another Polish study, Sochocki showed similarly that the majority of the homeless were male, 40–60 years old, and had experienced homelessness for a period of three to five years (Sochocki, 2010).
Fourth, our study does not allow for conclusions regarding whether problem gambling is the cause or the consequence of homelessness. This should be the subject of future research preferably using in-depth qualitative methods.
Finally, problem gambling is often associated with a variety of mental disorders. The study had a limited scope, and additional information on health problems and the social situation was not collected. The nature of the relationship between homelessness and gambling raises many questions, so future research is needed to explore that relationship.
Conclusions
The findings of the study suggest that problem gambling among the homeless can be viewed as a significant social and public health concern. Higher prevalence rates of gambling disorder among the homeless compared to the general population show that the homeless are a particularly vulnerable group. Staying in homelessness and young age are risk factors that increase gambling activity and may trigger development of gambling disorder. Among the homeless population lotteries are the most popular games, but along with the development of gambling disorder, homeless people choose gambling games with greater addictive potential. High rates of prevalence of problem gambling in the homeless population show the need to identify and monitor this problem and to provide access to gambling treatment or prevention programmes.
Footnotes
Ethical approval
All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki Declaration and its later amendments or comparable ethical standards. Ethical approval to conduct the study was obtained from the Bioethical Commission of the Institute of Psychiatry and Neurology from Warsaw, Poland.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The study was co-financed by the Fund of Solving of Gambling Problems being in disposal of the Ministry of Health (grant agreement no. 92/HM/2015; 17/HMK/2016).