
Abstract
This study examined the prevalence of secondary traumatic stress (STS) among substance-abuse therapists in relation to burnout, work-related stressors, as well as peer and leader support.
Methods:
A quantitative cross-sectional design examining 383 Norwegian substance-abuse therapists. Electronic surveys were distributed to practitioners in Norway via email and social media.
Results:
A total 22% of the respondents reported experience of secondary trauma, with the most frequently reported symptoms being flashbacks (13%) and intrusive thoughts (13%). More than 72% of therapists had also been exposed to patient direct threats. Female therapists estimated the level of trauma among their patients as higher than did male therapists. Male therapists (32%) were more likely to report secondary trauma than females (19%).
Conclusions:
The findings indicate a high prevalence of trauma symptoms in substance-abuse therapists, and suggest increased focus on the role of patient direct threats when treating patients with substance-abuse disorder. The study also highlights the need for research that examines variables that interact with gender in predicting STS in therapists treating substance abuse, as well as trauma.
In memory of Dr. Ayna Johansen, our esteemed colleague, researcher and clinician, who passionately contributed to the fields of addiction and therapy. Permission has been obtained from the estate to include Dr. Johansen’s name, the primary researcher of this study.
Patients entering treatment for substance-use disorders (SUDs) have high exposure rates to traumatic events, and one in five SUD therapists experiences STS as a result of working with these patients (Bride et al., 2009; Farley, Golding, Young, Mulligan, & Minkoff, 2004; Gielen, Havermans, Tekelenburg, & Jansen, 2012; Reynolds et al., 2005). This is concerning given the potential personal and professional impact of STS (Bride & Kintzle, 2011; Bride, Radey, & Figley, 2007; Choi, 2011; Yassen, 1995). The indirect trauma exposure of working with patients with PTSD (posttraumatic stress disorder) may produce lower job satisfaction and occupational commitment (Bride & Kintzle, 2011), as well as high levels of staff turnover (Duraisingam, Pidd, & Roche, 2009). If not properly addressed, such exposure can also lead to secondary traumatic stress disorder (Yassen, 1995), which is distinguished from PTSD in that the trauma exposure itself is indirect. As one of four possible exposure criteria for diagnosis for PTSD in the most recent DSM 5 (American Psychiatric Association, 2013), secondary exposure to traumatic events is recognised as a legitimate trauma event, in line with direct exposure. As the effects of trauma are emotional and relational, traumas may impact the quality of care provided (Bride et al., 2007; Choi, 2011). Specifically, it is likely that a trauma-exposed therapist will try to restrict their affective experience and receptivity, when working therapeutically with trauma-exposed patients. Thus, addressing STS among SUD therapists may improve worker retention and well-being, as well as treatment and outcomes.
Therapists find it difficult to ask their patients about trauma, independent of their own direct trauma exposure (Gielen, Krumeich, Havermans, Smeets, & Jansen, 2014). They worry it could reactivate their patients, and exacerbate emotional dysregulation and/or substance abuse. This is a problem, as SUD therapists treat many more patients who have PTSD than they realise. International studies have shown that approximately one of every three SUD patient meets PTSD diagnostic criteria (Bonin, Norton, Asmundson, Dicurizio, & Pidlubney, 2000), and a majority of these (71%) do not talk about their traumas unsolicited (Jacobsen, 1989). They may forget, and not sufficiently process therapists’ interventions due to the stress of starting treatment (Johansen, Tavakoli, Bjelland, & Lumley, 2015). At the same time, they generally want to be asked about their traumas (Gielen et al., 2014; Glover-Graf & Janikowiski, 2001; Jacobsen, 1989). This mutual avoidance of trauma-related themes is a considerable challenge to SUD treatment as they likely need to be addressed in an integrated and careful manner through the treatment course (Glover-Graf & Janikowiski, 2001; Johansen et al., 2015).
Research shows that female therapists have a greater risk of developing symptoms of STS (Baum, 2015; Michalopoulos & Aparicio, 2012), and are more susceptible to the effects of patients with histories of sexual violence (Kassam-Adams, 1995). Single status also associates with greater STS vulnerability, especially for men. Men’s vulnerability relates to achievement motivation and self-esteem (Maslach, Schaufeli, & Leiter, 2001; Roness & Matthisen, 2002). Most studies indicate that age and experience have a linear and inverse relationship with STS (Ghahramanlou & Brodbeck, 2000). A U-curved relationship (Steed & Bicknell, 2001) is also possible between age/experience and symptoms such that younger and less experienced as well as older and more experienced therapists have a higher risk of developing symptoms (Perkins & Sprang, 2013). While inexperience may impact the novel therapist, the most experienced are likely to be affected because they tend to take on more challenging cases (Lund, 2006). To understand STS in substance-abuse therapists requires a greater understanding of the prevalence of trauma symptoms in relation to risk factors for stress.
Methods
A web-based cross-sectional survey method was used to assess the prevalence of STS, and describe symptoms. This design is appropriate for describing patterns in previously unexplored phenomena, and is a rapid and cost-effective method of gathering quantitative data from a large set of respondents (Ringdal, 2013). Ethical approval was granted by the Regional Ethics Committee East of Norway.
Procedure
Participants were recruited online, or via email sent to several substance abuse inpatient and outpatient treatment units. Online we recruited participants through six closed, professional groups on Facebook. The online strategy was chosen to attract relevant, whilst excluding unintentional, respondents (Nosek, Banjai, & Greenwald, 2002). Prior to filling out the survey and in accordance with standard web-based research (Ringdal, 2013), participants provided informed consent by checking off on an abbreviated consent form that they understood the purpose of the study. Through email we sought individuals working with mental health, and/or SUD treatment. The email was distributed to employees within the department of substance use and addiction at Akershus University Hospital, which includes four outpatient treatment centres and six inpatient units. Furthermore, we recruited members of the main mental health practitioner professional bodies (e.g., the Norwegian Association of Social Workers). Respondents were invited to participate in an anonymous web-based questionnaire examining the issue of working with traumatised patients, excluding professionals without SUD treatment experience at the analytic level.
Participants
Participants included 383 practitioners, comprising 290 (76%) women and 93 (24%) men. Of these, 103 (27%) participants were social workers, 88 (23%) psychologists, 77 (20%) nurses, 80 (21%) social pedagogues, and 31 (8%) child protective service workers. Based on available descriptions of Norwegian SUD practitioners (Norwegian Health Directorate, 2015; Statistics Norway, 2016), this gives the sample a level of precision of 4.65 at the .95 confidence level. Therapists had worked with substance use and/or behavioural addictions for an average of 8.13 years (SD = 6.86), with a range of < 1 year to 33 years of experience and 67% (257) said they received regular supervision. We excluded 43 practitioners due to not fitting within the included professional groups, 36 for having no experience of SUD treatment, and seven for working in the SUD field as administrators. A total of 301 (77%) respondents were recruited online, while 82 (21%) were recruited via email. There was no significant difference between participants recruited via the two sources either on mean years worked in SUD (p = .63), burnout (p = .29) or STS (p = .13).
Measures
The web-based survey took approximately 15 minutes to complete, and was published digitally through “Nettskjema”. This is a tool for designing and managing data collection using online forms and surveys, made available on the web pages of the University of Oslo.
STS
Secondary traumatic stress was assessed using the Compassion Fatigue Short Scale (Adams, Figley, & Boscarino, 2008), which includes 13 items for STS such as flashbacks from work situations and burnout, such as feeling tired or weak due to work. The scale has a high discriminant validity (Boscarino, Figley, & Adams, 2004) and with sensitivity and specificity of 79% and 76%, respectively (Boscarino et al., 2004). Items are rated on a Likert scale, ranging from 1 to 10, with scores of 7 or higher indicating STS. Adams, Boscarino, and Figley (2006) reported the internal consistency estimates for the Burnout subscale as .90 and for the Secondary Trauma subscale as .80, with the combined scale having an internal consistency of .90.
Patient presenting problems
This was assessed by asking participants to estimate the percentages of the patients on their current caseload who had experienced different types of trauma exposure, had PTSD, relationship problems, depression, or used more than one substance. Additionally, we asked participants to indicate whether or not (YES/NO) patients had ever threatened them.
Professional support
Profession al support was assessed by asking whether participants received supervision (YES/NO). It was also assessed as perceived leader and peer support, using single items. The items asked participants to assess the degree to which they felt supported by (a) their peers and (b) their superiors according to a Likert scale ranging from 1 (never) to 5 (almost daily).
Data cleaning and preparation
In cases of single, missed items, a sample average score was used to replace the missing value. No cases were missing non-random data. The STS variable was positively skewed, and a log10 transformation was used to improve the normality of the distribution. Analyses were conducted with and without the logtransformed variable, without changing the results, and we thus report the non-transformed STS variable. The Statistical Package for the Social Sciences (SPSS) was used to perform the analyses, and significance was set at p = .05.
Analytic procedure
Percentages are provided for non-continuous variables, and between-group differences examined using Chi-square (χ2). Pearson correlations were used to assess relationships between continuous variables. To examine differences between groups based on gender we used Analysis of Variance (ANOVA), and independent samples t-tests were used to further examine significant differences.
Results
Descriptive of patient presenting problems
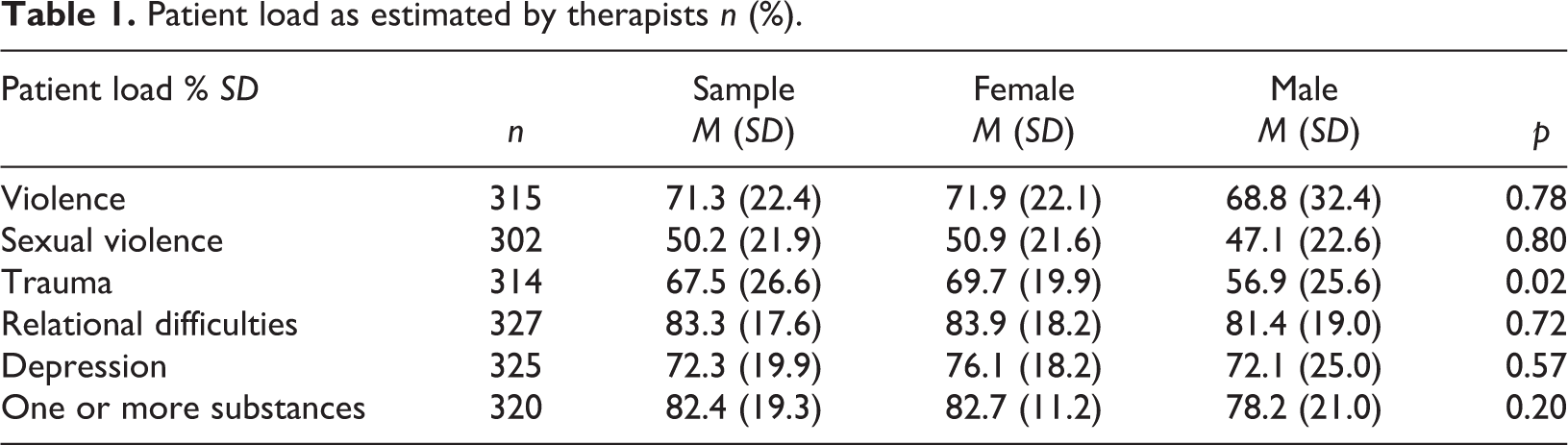
Table 1 shows how participants estimated load in the patient group for all participants, including the total sample, gender, and profession. It shows that all groups reported that the majority of their patients have been subjected to violence, sexual abuse, trauma, relationship problems and/or depression, and that they abuse more than one substance. A total of 72.4% reported having been threatened by one or more patients, with no differences between men’s and women’s accounts. In contrast, women estimated their patients’ total level of trauma exposure higher than men (F = 5.44(1), p = .02).
Patient load as estimated by therapists n (%).
Symptoms of STS and burnout
Analysis of STS and burnout symptoms show that the most frequently reported symptom of STS is flashbacks from work situations (13%) and intrusive thoughts (13%), followed by sleep problems due to patients’ difficulties (7%), including dreaming about one’s work (6%). The prevalence of clinically significant STS (score > 7) was 22% for the whole sample. Men had a significantly greater risk of meeting cut-off for diagnosis of secondary trauma (SD = 5.96, p = .02). Men’s STS was mediated by perceived work stress (F = 5.82, p = .02), while women’s was not. The entire sample reported high levels of overall burnout (33% felt trapped by work, 19% felt weak, 17% had difficulty separating their work and private lives, and 13% felt powerless).
Discussion
The aim of the current study was to assess the prevalence of STS and its symptoms among a sample of Norwegian SUD therapists and work-related risk factors. A total of 353 participants responded to our web-based cross-sectional survey which was distributed via email and social media. Statistical analysis of the data showed that SUD therapists’ caseloads were mostly representative of patients with trauma histories.
Patient presenting problem
Therapists estimated that 68% of their patients had been victims of traumatic events. This estimate is somewhat higher than those reported by a study that examined SUD therapists in the US, which found half of their patients had experienced these traumas (Bride et al., 2009). Estimates are also somewhat higher than prevalence rates of co-occurring PTSD in the SUD treatment population (Bonin et al., 2000; Fetzner, McMillan, Sareen, Asmundson, & Gordon, 2011; Kjøsnes, 2014; Mills, Lynskey, Teesson, Ross, & Drake, 2005), which is surprising given that SUD therapists have been shown to generally underestimate the rate at which their patients are affected by trauma (Gielen et al., 2012). Additionally, female therapists reported a significantly higher estimate of patient trauma, than male therapists. One possible explanation for this could be that socially constructed gender roles make up a general expectation that women are more caring, and have greater sensitivity to others than men. It is therefore possible that patients feel that it is easier to open up to female therapists, thus allowing women to gain more accurate perceptions of the presenting problem. This view is in accordance with one study from Finland, showing that both male and female patients preferred a female SUD therapist (Kuusisto & Artkoski, 2013).
Along with these results, nearly three out of every four therapists reported having been threatened or felt threatened by a patient at some point in their practice, suggesting most of the therapists also have been directly subjected to potentially traumatic experiences in the workplace. The finding is in line with one study on the prevalence of patient threats towards SUD therapists in the USA, which reported that 84% of the participants had experienced directly some form of physical or psychological violence. The study also connected exposure to threats with work performance (Bride, Choi, Olin, & Roman, 2015), but did not report on the extent to which these experiences had occurred inside or outside clinical practice. Taken together, however, these numbers come across as high, and suggest SUD therapists may deal with threats as part of their everyday work lives.
Symptoms of STS and burnout
Results indicated 22% of the therapists in the current sample met criteria for STS. This is in accordance with research from the US and Australia where 19% and 19.9% of SUD therapists reported STS, respectively (Bride et al., 2009; Ewer et al., 2015). Contrary to other research (Baum, 2015; Cornille & Meyers, 1999; Michalopoulus & Aparicio, 2012; Perkins & Sprang, 2013), we found that men (32%) scored higher on STS than women (19%). Source of recruitment (online vs. in/outpatient units) did not explain the gender difference as there were no differences between the male and female samples depending on source. This makes the current study a first to indicate STS gender effects in SUD therapists that suggest further exploration of gender dynamics in relation to development meeting criteria for cut-off of secondary traumatic stress disorder (Yassen, 1995).
The most frequently occurring STS symptoms were flashbacks and intrusive thoughts, which were reported by 13% of our sample. Sleep problems were less frequent and experienced by 7%. These findings are consistent with another study on STS in SUD therapists indicating that the flashback symptoms are the most frequently occurring symptom (43%), and that sleep problems occurred less frequently (26%) (Bride et al., 2009). About 19% of our sample indicated feeling emotionally weak, compared to Bride et al. (2009) where 25% felt emotionally weak. The discrepancies in reported symptomatology from the past studies of Ewer et al. (2015) and Bride et al. (2009) that used the Secondary tTraumatic Stress Scale (STSS; Bride, Robinson, Yegidis, & Figley, 2004) may be due to scaling discrepancies between these scales. The STSS was developed consistent with Figley’s definition of STS with identified symptoms that parallel those of PTSD. The respondents are asked to indicate how frequently each item has been true for them in the past seven days using a five-point, Likert-type scale. Scores of 3 and above on each item place the respondent in moderate to high STS. The current study used the Compassion Fatigue Short Scale, which includes a stricter definition of a positive occurrence, demanding an item score of 7 out of 10 as the cut-off mark for a moderate to high STS (Boscarino et al., 2004).
Implications
The study confirms that STS is prevalent among SUD therapists (Bride et al., 2009; Ewer et al., 2015). Patients with SUD tend to report higher rates of trauma exposure, which may explain the high prevalence of STS among SUD therapist. The results also show that although female therapists reported significantly higher estimates of patient caseload, male therapists had a higher prevalence of STS. The results highlight the importance of studying SUD therapists and the potential relationship between STS and gender. In this study, STS was prevalent among the therapists, who also reported high exposure to patients with SUD or PTSD, and most reported having been threatened by patients at least once. Future research should examine demographic factors, along with contextual work factors, including supervision experience and work satisfaction, and their roles in affecting male and female therapists’ STS. Furthermore, future studies of gender differences within a social context could bring together seemingly discrepant findings of both gender similarity and gender differences. Gender-sensitive social contextual research will potentially provide a deeper level of understanding of female and male therapists in relation to their life experiences.
Neither of the most commonly available STS instruments, such as the Compassion Fatigue Self-Test (CFST), STSS or the ProQol (Professional Quality of Life Self: Stamm, 2005) measure patient direct threats (Adams et al., 2008; Bride et al., 2004; Stamm, 2005). The inclusion of such items would easily facilitate improved comparisons of caseload differences between different populations of therapists, as well as giving a more comprehensive assessment of the nature of trauma symptoms in therapists.
The findings of the present study also have important implications for clinical practice. The identification of therapists with high exposure to SUD and PTSD patients can be useful for targeting specific preventative interventions to reduce the likelihood of them developing STS. The results highlight the importance of adequate training and supervision for SUD therapists with regard to treating trauma, but also specific to managing the stress of patients’ direct threats. Therapists and supervisors may benefit from simply learning about the presence of STS in SUD treatment practice, as it validates an overlooked area. Clinic administrators and counselling supervisors may use these insights to increase preventive efforts, including use of psychoeducation, self-care, and debriefing as techniques to improve staff resilience. Clinical training and supervision of therapists must develop self-care tools that are gender-sensitive and respond to the needs of both male and female therapists.
Limitations
The study includes a sample partially acquired online, which introduces a potential selection bias. An online survey may have been attractive to male therapists as a means to more anonymously address a problem. This may cause the current results not to generalise to the broader population. Second, although the study showed most of the participants had experienced threats as part of their professional work, this study did not examine the dynamics of patient threats upon therapist STS either continuously, or qualitatively, but, rather, recorded the prevalence of such experiences. This is a problem as it means the item does not discriminate between severity and degree of repetitiveness of this problem. As such, it is impossible based on current data to either rule out or exclude the effects of patient direct threats on the therapists’ symptoms of trauma. Finally, the use of the CFST in the current study limits the direct comparison to past studies of STS in substance-use therapists (e.g., Bride et al., 2009; Ewer et al., 2015), which have used the STSS as a measure.
Conclusions
There is limited research on factors that contribute to STS in SUD therapist populations (Bride et al., 2009; Ewer et al., 2015) and the current study adds important findings to the literature. The study is a first to connect STS with other types of workforce issues such as burnout, patient violence, and perceived work support. Contrary to past studies, we did not find women to have higher rates of STS than men, but, rather, showed a statistically significant difference with men reporting the highest levels of STS. Finally, the study showed that the majority of therapists also had experienced direct patient threats. The study shows there is a large degree of potential PTSD exposure among Norwegian SUD therapists and gives preliminary support of therapist gender effects in SUD treatment that warrant further examination.
Footnotes
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.