
Abstract
Aim:
To investigate social inclusion/exclusion in terms of criminality, substance abuse and participation in the labour market in clients treated for substance abuse in Sweden in the 1980s during a follow-up period of 27 years.
Method:
SWEDATE data are used for background information on the clients. The data were collected through interviews with clients registered for treatment in 31 in-patient treatment units in 1982 and 1983. Data on labour market status, education and medication related to drugs were collected from public registers. The study population consisted of 1132 individuals, who were followed from the year after exiting from treatment (Year 1) until the end of the follow-up (December 2013).
Results:
Among those who survived, the women seem to have succeeded better in terms of social inclusion both at an aggregated level and when the individual pathways were followed during the follow-up period. When comparing pathways between adverse and non-adverse groups during the follow-up period the results show movements from being adverse to non-adverse but also the opposite. In the last follow-up in 2013, the majority of the clients defined as non-adverse for the last nine years were in some way established in the labour market (including studies). In total, about two fifths of the group were in some way established in the labour market.
Conclusions:
The fairly high proportion of clients moving between being adverse and non-adverse during the follow-up might support the perspective suggesting that dependence should not be considered as chronic.
Keywords
During the early 1980s, a comprehensive research project studying Swedish in-patient care for drug abuse was carried out; the so-called SWEDATE (Swedish Drug Addict Treatment Evaluation) project (Bergmark, et al., 1994). Background data were collected through interviews with clients registered for treatment in 31 in-patient treatment units in 1982 and 1983. A total of 1656 clients were registered and, of these, 1163 were interviewed. At the time, in-patient treatment units in Sweden were not specialised according to substance abuse, but instead admitted and mixed all types of clients. The data collected in the project are substantial and complex and include background data on a majority 1 of the clients in Sweden who were treated for problems with drug abuse in 1982 and 1983.
A follow-up of samples of the SWEDATE group was carried out after one and subsequently five years. A sample of clients (n = 436) were interviewed after one year showing that, by and large, the sample continued to have alcohol or drug problems (Bergmark et al., 1994). After five years, two groups were created from the one-year sample constituting the clients with the “best” (n = 43) versus the “worst” (n = 40) outcomes in terms of drug abuse, criminality, social integration, psychological status and welfare support. 2 These two groups were followed up using public registers with the aim of investigating how stable the results from the one-year follow-up were. The results indicated that two thirds of the persons in the best group still had positive outcomes in the variables measured. Only one person in the worst group had changed to a positive outcome after five years (Byqvist, 1993).
Now, more than thirty years later, a follow-up project on all the SWEDATE clients (n = 1163) is being carried out to investigate how the lives of the SWEDATE clients have turned out using data from relevant public registers. So far, the mortality rates and causes of death in the group have been investigated and mortality rates according to dominant substance misuse have been compared (von Greiff, Skogens, Berlin, & Bergmark, 2018). In addition, individual characteristics as well as gender-specific similarities and differences regarding predictors of mortality have been analysed (Skogens, von Greiff, Berlin, & Bergmark, 2019). Results show differences in standardised mortality rates (SMR) and causes of death in different groups based on type of misuse. Gender differences have emerged and the greatest differences were found in the groups whose self-reported dominant substance misuse was cannabis or opiates. The SMR was higher among men in all the groups studied except for those mainly misusing alcohol. Drug and alcohol related demise was the most common cause of death in the group as a whole. There was also a large increase in the proportion of deaths related to drug and alcohol misuse when contributing causes were considered, compared with when only the underlying (primary) cause of death was accounted for (von Greiff et al., 2018).
In terms of individual characteristics as well as gender-specific similarities and differences regarding predictors of mortality, the results showed that imprisonment and being a parent without custody of the child seemed to constitute risk factors for mortality among women, but not among men. A social network of friends seemed to be more important for men and treatment dropout was a significant risk factor for premature death among men, but not among women. Both men and women who self-reported alcohol as their most dominant form of substance abuse experienced a higher mortality risk compared with those whose dominant substance abuse consisted of stimulants (Skogens et al., 2019).
The aim of the present article was to investigate social inclusion/exclusion in the group during the follow-up period in terms of criminality and substance abuse as well as the group’s participation in the labour market. It is well known that there are gender differences in pathways in and out of addiction as well as treatment careers (cf. Grella & Joshi, 1999; Pelissier & Jones, 2005). However, long-term follow-up of gender-specific analyses on social inclusion and how persons may take different turns over a long period of time are rare. The SWEDATE data allow for such follow-up with a majority of a cohort of persons treated for drug abuse. The specific research questions were: How have (male and female) clients developed in terms of criminality and substance abuse? How does establishment on the labour market differ between women and men with adverse versus non-adverse outcomes in terms of criminality and substance abuse?
Long-term follow-ups on social inclusion in clients treated for substance abuse
One of the problems with long-term follow-ups of psychosocial treatment of substance abuse is that their design often does not allow for conclusions that are statistically stable, and at the same time interesting, from a treatment perspective. Differences in terms of definitions of abstinence, type of abuse and follow-up time make comparisons between studies complicated. However, Oscarsson (2006) points out that follow-up studies over a long period of time can provide valuable contributions to knowledge on the interplay between psychosocial treatment, individual characteristics and social factors.
A central theme in follow-up studies of patients after treatment is mortality and causes of death. Positive outcomes are often measured in terms of abstinence or reduction of abuse, health status, criminality and employment. A 33-year follow-up of 581 male heroin addicts admitted to compulsory drug treatment showed that among those alive a majority reported drug use or tested positive for heroin. One fifth were daily alcohol drinkers (Hser, Hoffman, Grella, & Anglin, 2001). In general, the group was characterised as marginalised in terms of unemployment, criminality, health problems etc. Hser (2007) discusses the findings in terms of long-term stable recovery from heroin addiction, suggesting that breaking the vicious circle (of drug use) later in life appears to be rather difficult. In previous follow-ups of the same material, the focus has, among other things, been on timing and the duration of methadone maintenance in relation to common patterns of episodes of treatment, abstinence and relapses and the conclusion has been that the cessation of narcotics is unlikely to occur and that, when it does, it is a slow process (Hser, Anglin, & Powers, 1993; Hser, Yamauchi, Chen, & Anglin, 1995).
Mental health status has been studied in follow-ups over a long period of time. In a study of heroin patients at methadone maintenance clinics in California in the 1970s, where the focus was on gender differences in physical and mental health, women reported significantly more chronic health problems and psychological distress compared to men and compared to population norms (Grella & Lovinger, 2012). Women with past-year substance use also had poorer mental health than other women. The importance of problem severity at treatment entry for long-term effects of treatment was analysed in a five-year follow-up of 708 cocaine-dependent patients showing that patients with severe drug and psychosocial problems had poorer long-term outcomes (Simpson, Joe, & Broome, 2002).
Having a form of employment is an important component of social wellbeing as it contributes to the creation of identity, strengthens social capital and improves physical and mental health (Leufstadius, Eklund, & Erlandsson, 2009; Luyckx, Schwartz, Goossens, & Pollock, 2008; Mossakowski, 2008). Previous research on effects of drug abuse on employment indicates that hard drug use in particular has a negative impact on employment, participation in the labour market and income (Huang, Evans, Hara, Weiss, & Hser, 2011). Gender is also a contributing factor. Even if there have been changes, there is still a gap between women’s and men’s working hours; in 2013, 30% of Swedish women worked part time compared to 11% of men (SCB, 2014). A significant reason for this is that women still tend to be the primary caregivers of their children which also affects participation in the labour market for women with drug abuse (SCB, 2014).
Alm (2015) explored the abuse from a longitudinal perspective following a cohort of Swedes born in 1953 described as “first generation addicts” (p. 110) and their flow of social exclusion and integration over time. The results showed that according to the social inclusion/exclusion measurements used in the study (related to the labour market), almost one in five (18%) of the research cohort with a known abuse problem during adolescence was socially included in society at the age of 56, compared to 72% of those in the cohort for whom there was no documented abuse. The rest were either socially excluded or deceased. Furthermore, the results showed that the situation was much more unstable in the addiction group and that those in the addiction group just did not go from being excluded to being included. No gender differences were found regarding the consequences of addiction.
A 37-year follow-up of Swedish conscripts with self-reported drug use showed weaker links to the labour market among those treated in hospital for an abuse diagnosis (Davstad, Leifman, Allebeck, & Romesjö, 2013). This is in line with another Swedish study showing that only 3% of those with serious drug-abuse problems had a strong attachment to the labour market, while 73% of men and 77% of women had a weak or non-existent labour market attachment (Olsson, Adamsson Wahren, & Byqvist, 2001). However, research from the US on the importance of supported employment for the reduction of drug use and crime has shown no reductions of cocaine and heroin use (Uggen & Shannon, 2014).
A seven-year follow-up of 126 heroin addicts showed that barely half (48%) used opiates (Stimson, Oppenheimer, & Thorley, 1978) and the time in unemployment was extensive (Oppenheimer & Simpson, 1982). This tendency was also found in more recent follow-ups: a study of patients five years after detoxification showed higher participation in the labour market in those who were abstinent (76.9% compared to 59.3%) (Ribiero, Dunn, Lima, & Laranjeira, 2007) and a 12-year follow-up of 321 cocaine-dependent male patients showed that those who achieved stable recovery (five years of abstinence from cocaine) reported fewer psychiatric symptoms, less criminal involvement and unemployment during the year prior to the interview (Hser et al., 2006).
There are studies contradicting the pessimistic results reported above. In a five-year follow-up using interviews with a representative sample of clients treated for Alcohol and other drugs (AOD) problems in the county of Stockholm, Stenius, Ullman, Storbjörk, and Nyberg (2011) found that the majority reported no mental health problems in the last 30 days and had an improved social situation (with their own housing and employment). The crime levels in the group had decreased remarkably.
A central issue in research on substance abuse is how these problems are to be understood. In a medically oriented view, addiction (or drug dependence) is emphasised as being a chronic disorder (Institute of Medicine, 2006; McLellan, Lewis, O’Brien, & Kleber, 2000), stressing that the observed abstinence in a given individual is to be understood with a long-term view in mind. From this perspective, abstinence is merely a deviation from the dependence that will most likely appear in the longitudinal process, dominated by substance abuse. This approach has led to a growing interest in studies with a longitudinal dynamic approach (Hser, 2007) aiming to investigate and identify patterns of drug use, related incidents and behaviours over time.
Considerable interest has also been shown for a perspective suggesting that drug dependence is transient and that many individuals with addictive behaviour overcome their problems without professional treatment or self-help groups (Klingemann & Sobell, 2007). The approach is often based on studies of individuals in untreated remission (Rumpf, Bishof, & John, 2007).
The present long-term follow-up with a relatively substantial number of individuals with treatment experience, followed over a vast time-span may help shed light on whether these perspectives on substance abuse are contradictory or whether a combination of both might be possible. However, some draw-backs with the long time-span should be taken into account. First, the obvious fact that mortality increases along with age. Second, since criminality is used as one of the measures of social exclusion, the strong relation found between age and crime, the so called “age–crime curve”, in which criminal behaviour increases during adolescence, peaks in late adolescence and rapidly declines in adulthood, has to be considered (e.g., Piquero, Farrington, & Blumstein, 2003; Sweeten, Piquero, & Steinberg, 2013).
Material and method
All 31 in-patient units that participated were focused on substance abuse, including polydrug abuse, often combined with alcohol abuse. The study was restricted to those who were between age 15 and 35 years at intake to treatment (92% of all 1163 interviewed) and who had complete information in the national registers (31 individuals lacked complete information, i.e., they had not died according to the Swedish death register (DORS) but were missing in the Swedish population registers in 2013). The age restriction was included in order to decrease the impact of old age in the results. After these restrictions, the study population consisted of 1034 individuals. They were followed from the year after exit from treatment (Year 1) until the end of the follow-up (December 2013), and data were collected on labour market status, educational attainment, crimes, and care related to drugs. The exit from treatment occurred in a narrow time-span (1982–1986) where the latest exit (1986) allowed us to follow the entire study population for a minimum of 27 years. The SWEDATE data were linked to Swedish registers where the following variables were collected:
From the Swedish national council for crime prevention
In prison: In cases where the sentence is imprisonment, time in prison is counted as 2/3 of the penalty period starting from the decision date. 3 “In prison” refers to imprisonment where none of the other options occurred during years covered by time in prison.
Active in crime: Crimes that resulted in penalties corresponding to imprisonment (all penalties except day fines and pecuniary fines) or when any of the sentences is a drug offence (BRB 19680064 and 19680070) regardless of the sanction. Judgements that did not lead to imprisonment but involved multiple crimes that occurred on different dates are also included. The years from the first crime to the final crime are counted as time active in crime.
From the National Board of Health and Welfare
Healthcare: Years with care for alcohol related diagnoses, 4 drug-related diagnoses 5 or poisoning 6 according to Patientregistret (PAR) (in-patient care and from 2001, also specialised out-patient care).
Care of Substance Abusers (Special Provisions) Act (LVM): 7 Appears for compulsory care in the registry (even if notifications did not lead to LVM care).
From Statistics Sweden
Highest level of education: Highest level of education achieved in 2013.
Labour market status: Link to the labour market according to The National Board of Health and Welfare (2010, pp. 64–65; ses also Bäckman, Jakobsen, Lorentzen, Österbacka, & Dahl 2011). In the original definition, three-year intervals were used but since our data are from three specific years (1993, 2003, 2013), we have created a simplified version (see below). The groups are exclusively divided by rank so if a person belongs to several groups, the highest rank is chosen. Core labour: Employment income of at least 3.5 Price Base Amounts.
8
No early retirement, no unemployment and no substantial sick leave (i.e., not 25% or more in sickness benefit). Unstable labour/substantial unemployment: Summary of several subcategories (for details see The National Board of Health and Welfare, 2010, pp. 64–65). Labour income between 0.5 and 3.5 basic amounts, including sick leave (i.e., < 25% sickness benefit) and/or comprehensive unemployment benefit (i.e., < 25% unemployment benefit). Includes also persons on unemployment benefit of at least 25% of the equivalent disposable income and persons with an early retirement pension of one basic amount or more. Student: Student income (e.g., student loan or student grant) of at least 0.87 basic amounts and working income of a maximum of 1.75 basic amounts or employment income less than 0.5 basic amounts and any student income. Substantial sick leave/early retirement/sickness benefit: Any sickness benefit. In the case of employment income, the sickness benefit is at least 25% of the income earned. If there is no employment income, the sickness benefit corresponds to at least 25% of the equivalent disposable income. Includes also persons with an early retirement pension accounted for at least one basic amount. Not more than 0.5 basic amounts in earned income. Economically inactive: Employment income below 0.5 basic amounts and does not belong to the above categories. A heterogeneous group, having in common the fact that they have had very little connection with the labour market and the general systems for compensation in case of loss of income.
In order to follow inclusion/exclusion in the study population, data for the variables In prison, Active in crime, Care of Substance Abusers (Special Provisions) Act and Health care (alcohol or drug related diagnoses and poisoning) have been collected through the whole follow-up period. Pathways in three steps were created, i.e., the follow-up time was divided into three, nine-year long periods 9 and data were sorted into the groups as shown in Figure 2.
Non-adverse: Individuals who were not sentenced to prison during the nine-year period, were not active in crime or who did not receive any care for alcohol, drug and/or poisoning according to both PAR and the Care of Substance Abusers (Special Provisions) Act.
Adverse: Individuals who were sentenced to prison during the nine-year period, were active in crime or who received care for alcohol, drug and/or poisoning according to both PAR and the Care of Substance Abusers (Special Provisions) Act.
Dead: Individuals who had died during the nine-year period.
Results
At baseline, all the clients in the study were registered for in-patient treatment for substance abuse. Thus, they were all judged to have experienced major substance abuse (for example, 70% had experienced hospital and/or institutional care for drug and alcohol misuse, almost half had suffered a non-fatal overdose when they were registered). The group was at the time characterised as being in a vulnerable and marginalised situation. For example, the majority did not have their own housing, 52% of the women and 40% of the men had attempted suicide and/or had received psychiatric care for diagnoses other than substance misuse (for more details, see Skogens et al., 2019). Mean age at intake to treatment was 25.5 years for men and 23.4 years for women, and at exit from treatment 26.7 years for men and 24.6 years for women.
Aggregated yearly rate
At an aggregate level, the proportion of non-adverse individuals was relatively stable during the follow-up period for both men and women (Figure 1). However, the proportion of non-adverse individuals was higher among women. As expected, the proportion of deceased individuals increased during the follow-up period and was almost twice as high for men compared to women at the end of the follow-up period (27 years after discharge): 42% versus 22% deceased respectively. The proportion in healthcare or LVM care (without indication of crime activity) was relatively stable for both women and men at roughly 10%. When crime activity occurs at the same year as healthcare or LVM care the proportion was declining during follow-up, from approximately 25% the first year after discharge to approximately 15% at the end for both men and women. Crime was consistently more common among men, but decreased continuously during the follow-up period among both men (from 50% to 11%) and women (from 28% to 10%). Among men, a small but fairly stable proportion was in prison (the percentage dropped slightly over the years). The corresponding proportions for women were very low.
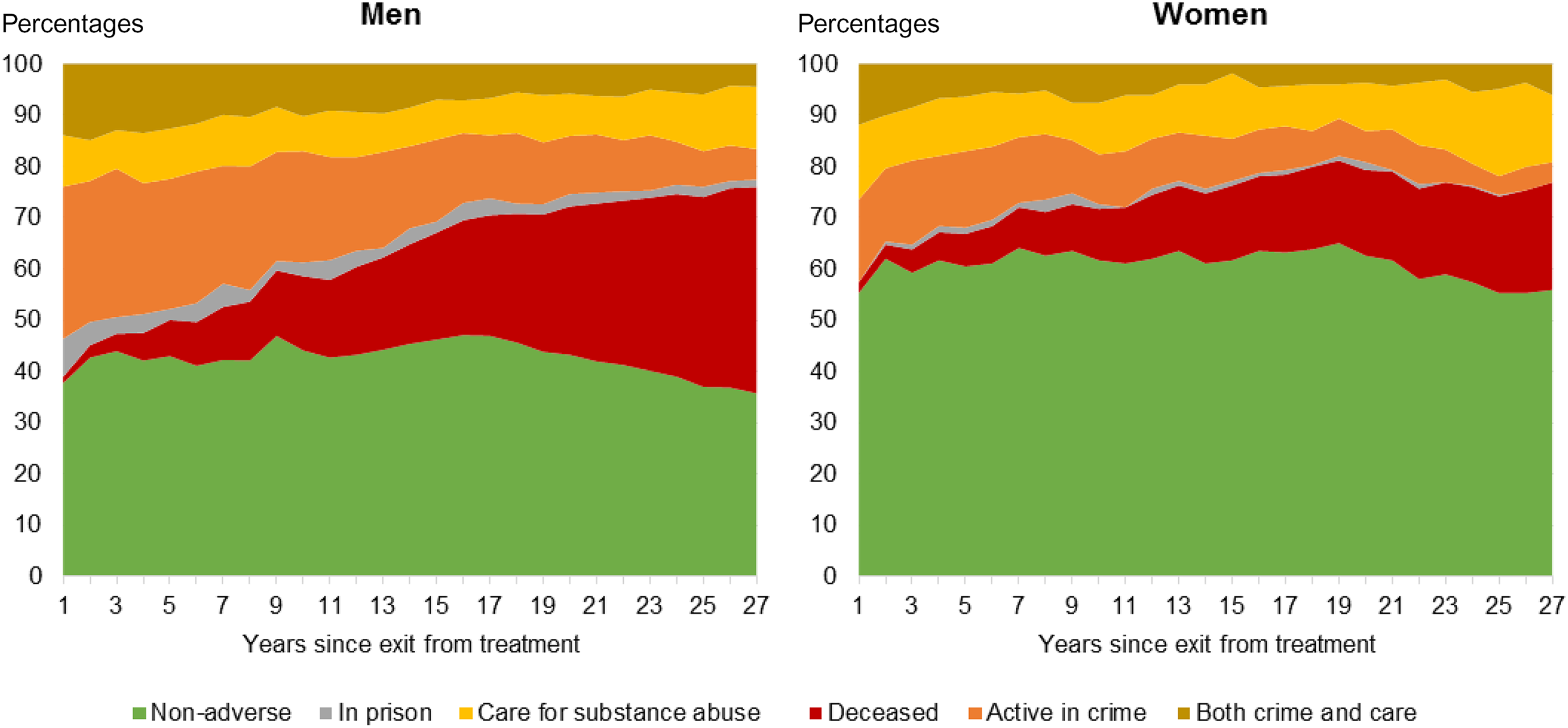
Aggregate yearly rate. The whole study population aged 15–35 years at intake to treatment (n = 1034) distributed according to years since discharge, where 0 refers to year of discharge. Men (n = 705) and women (n = 329) respectively (percentages).
Pathways in three stages
Figure 2 describes the proportion of men and women defined as non-adverse (green boxes in the figure), adverse (orange boxes), and deceased (red boxes) during the three studied time-periods (p1–p3). Each time-period sums up to 100%, covering the proportion that followed a specific path (through the three different stages: non-adverse, adverse, and deceased) up to that time-period.
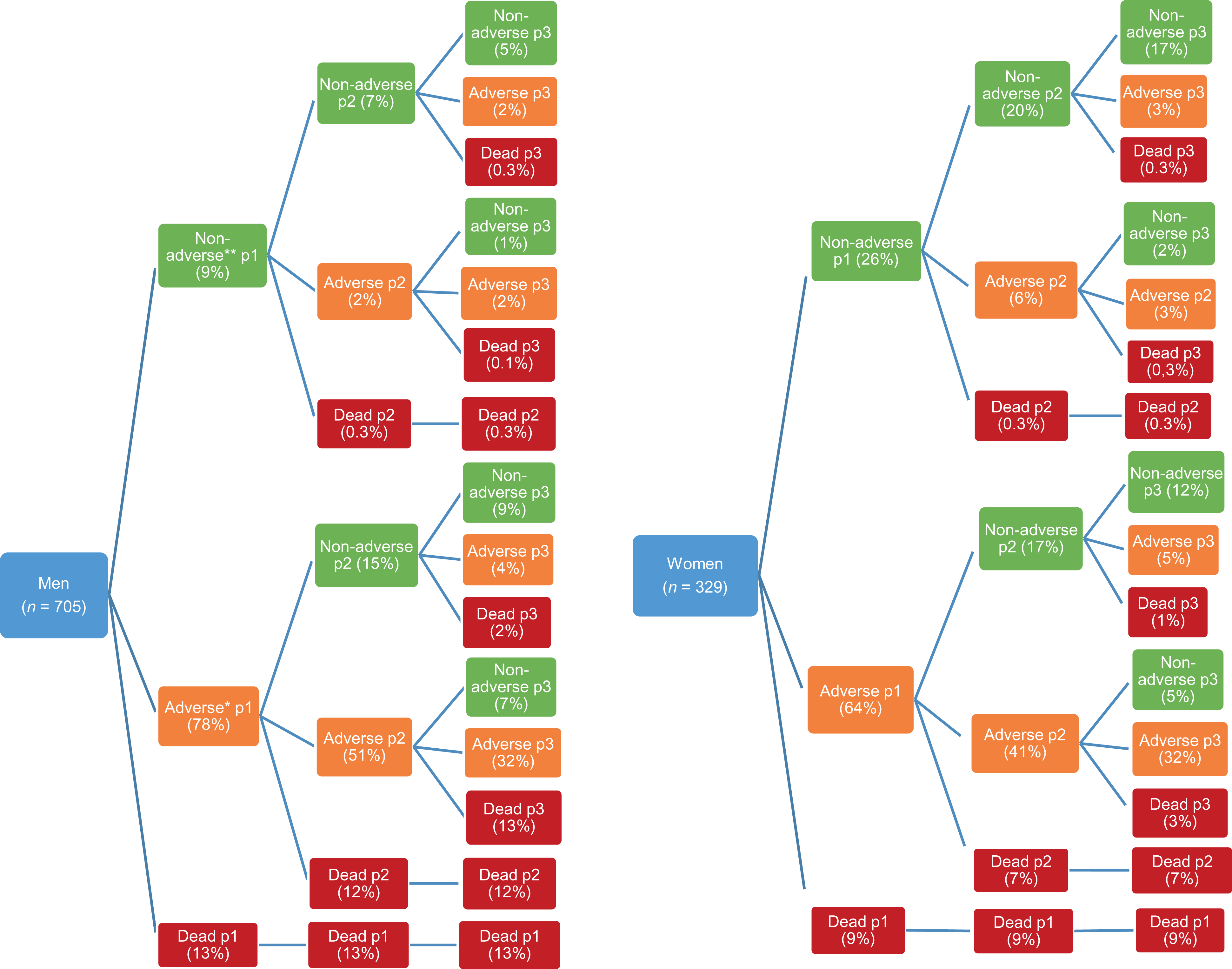
Pathways based on the entire study population aged 15–35 years at intake (n = 1034), divided into adverse and non-adverse groups during three time-periods (p1–p3). Men and women respectively (percentages).
In the last time-period, p3, 22% of the men (5+1+9+7%) were non-adverse, 40% (2+2+4+32%) adverse, and 43% were deceased (the totals may differ slightly from 100% due to rounding errors, since the proportions in each period are given in integers). Of the 22% defined as non-adverse at p3, just over one fourth (5 out of 22%) had stayed in that category throughout the entire follow-up period (p1–p3). This implies that the non-adverse group largely changed over the years studied. Among the 9% who were defined as non-adverse in p1, almost a third became adverse or died during p2. On the other hand, 15% of those defined as adverse at p1 were defined as non-adverse at p2. In other words, the adverse group also changed during the follow-up period, but the main reason for the decrease was due to the fact that the number of deceased had increased by 12–13% for each follow-up period.
The non-adverse group constituted a higher proportion among the women in p3 compared to the men: 36% (17+2+12+5%) versus 22%. Among the women, almost half (17 out of 36%) had been defined as non-adverse during the complete follow-up period (p1–p3). On the other hand, among those 43% of women (3+3+5+32%) who were defined as adverse at the last time-period (p3) three out of four (32 out of 43%) had stayed in that category at each time-period. The higher mortality rate in the men compared to the women was also visualised in the pathways, especially among the majority who ended up in the adverse category from the beginning. The fact that the men had a higher mortality rate than the women did not change the relation between non-adverse and adverse outcomes. The proportion of men defined as adverse (in relation to non-adverse) was still higher than in the women when the deceased were excluded (not shown in Figure).
The probability of escaping the adverse pathway might be described in an alternative way using transition probability from a certain stage at a given time-period, i.e., each stage sums up to 100% at a given time-period. Among the men who were defined as adverse in the first time-period (78% in p1), 11% managed to move into and then stay in the non-adverse path in both p2 and p3. The corresponding proportion in the women who managed to move from the adverse stage in p1 (64% adverse in p1) and then stay in the non-adverse path both p2 and p3 was 18%. Conversely, among the men and the women who were defined as non-adverse in the first time-period (9% vs 26% in p1) approximately half (48%) of the men and two thirds of the women (65%) remained in the non-adverse path in both p2 and p3, while 44% versus 26% of the men and the women ended up adverse or deceased in p3. The remaining 8% versus 9% were adverse in p2 but ended up non-adverse in p3.
Labour market status
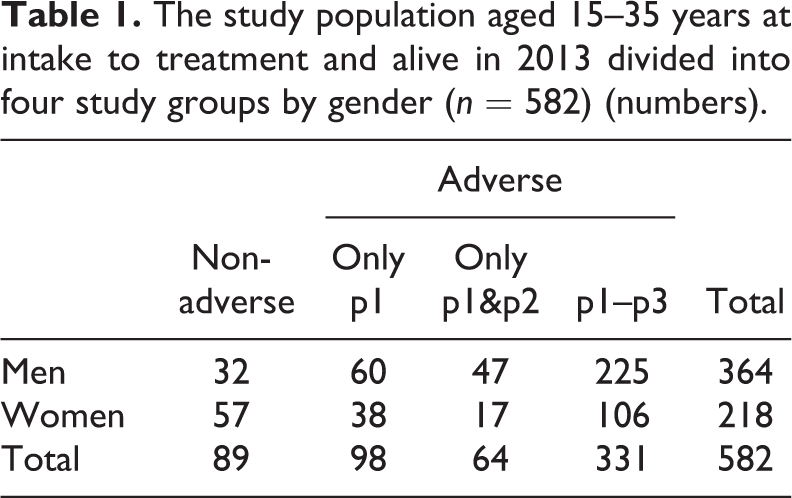
The following analysis focuses on social inclusion in terms of labour market status. The analysis is restricted to the four largest pathway groups: those who were defined as non-adverse in all three stages (“Non-adverse” in Table 1); those who were adverse in the first stage but non-adverse in the last two stages (“Only p1” in Table 1); those who were adverse in the first two stages but non-adverse in the last stage (“Only p1&p2” in Table 1); those who were adverse in all three stages (“p1–p3” in Table 1). With this restriction, the study population consisted of 582 individuals, which corresponded to just over half (56%) of the entire study population aged 15 to 35 years at intake to treatment (n = 1034) of whom 34% were excluded since they were deceased by the end of the follow-up (year 2013) and 10% were excluded since they belonged to one of the four pathway groups which were excluded due to their small numbers. The outcomes of the variables above have been compared between adverse and non-adverse groups in terms of criminality/crime and/or substance abuse during the follow-up period (Table 1).
The study population aged 15–35 years at intake to treatment and alive in 2013 divided into four study groups by gender (n = 582) (numbers).
A contributing prerequisite for being established in the labour market is the level of education. Therefore, the highest completed level of education in the study groups is described. As shown in Table 2, the level of education was generally low. However, there are some variations between the groups. The proportion with the highest level of education equivalent to post-secondary education was greatest in the non-adverse group for men. Among women, the proportion with post-secondary education was almost as high in the group that was adverse during the first period as in the non-adverse group. There did not seem to be a clear difference between adverse and non-adverse groups who had at least started the upper secondary level. Nevertheless, the group that had been adverse during the whole follow-up period (p1–p3) included a higher proportion who had only completed primary school (33% in men compared to 12–26%, and 47% in women compared to 19–35%) as well as a higher proportion with missing information on educational attainment compared to the other groups.
The highest completed level of education among men and women in the four study groups (n = 582), for the year 2013 (percentages).
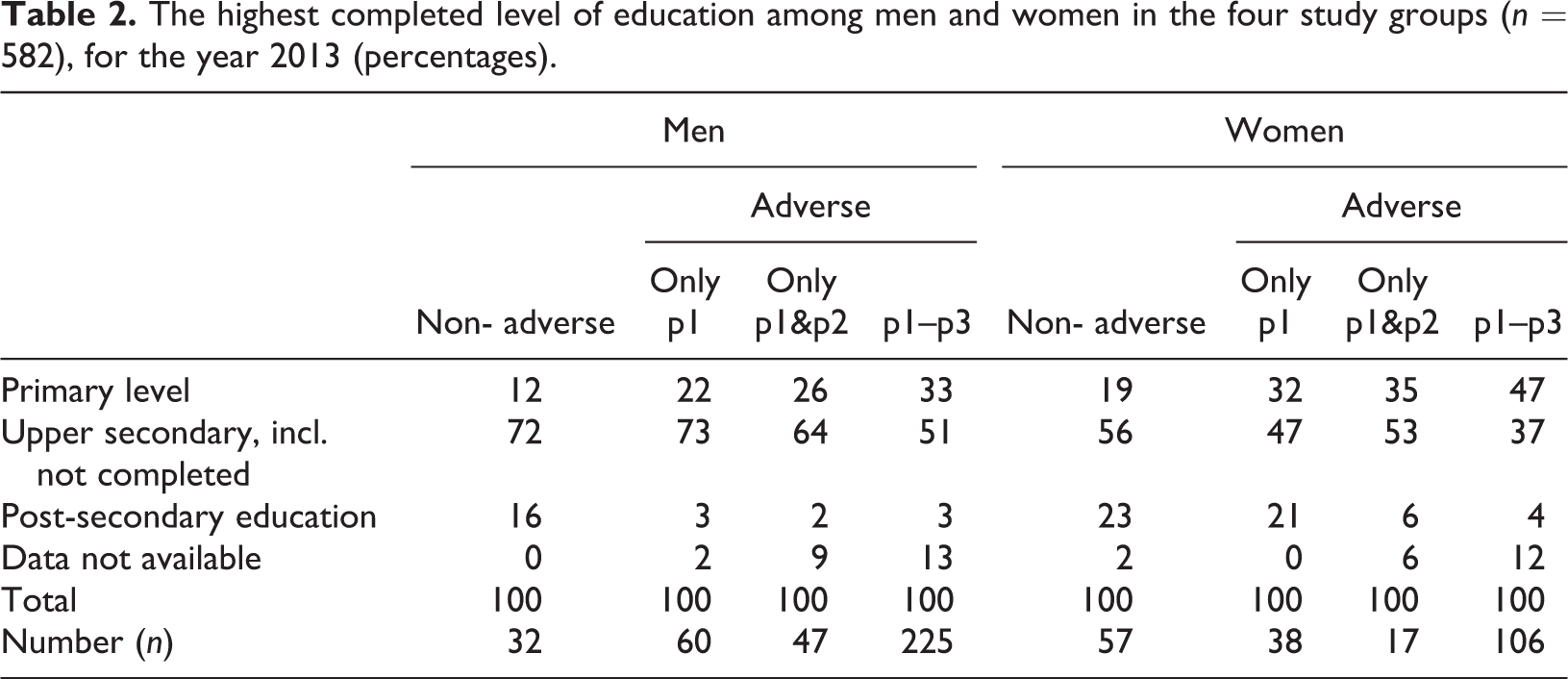
Table 3 shows the clients’ labour market status in three specific years at ten-year intervals during the follow-up period. In 2013, 42% of the women and 38% of the men were working (including unstable workforce) or studying (figures not in table). The corresponding proportions in 1993 were 54% for women and 48% for men, and in 2003 47% for women and 38% for men. When comparing the four study groups some differences emerged. While between 78% and 97% of the non-adverse men and between 65% and 84% of the non-adverse women were categorised as “in workforce/studying”, the percentages were lower in the adverse p1–p3 group: 19% to 35% for men and 19% to 31% for women. This indicates that the non-adverse groups were more socially integrated in terms of labour market presence. Further, at an aggregated level, labour market presence decreased in relation to the length of time the group continued to be active in crime and/or substance abuse during the whole/entire follow-up period. This difference between the groups was more apparent among the men. Among the women, it was even the case that in 2013, those who were adverse only during the first period (p1) had a slightly higher labour market presence than those who were non-adverse during the whole follow-up period (68% vs. 65%).
Links to the labour market among men and women in the four study groups (n = 582) for the years 1993, 2003, and 2013 (percentages).
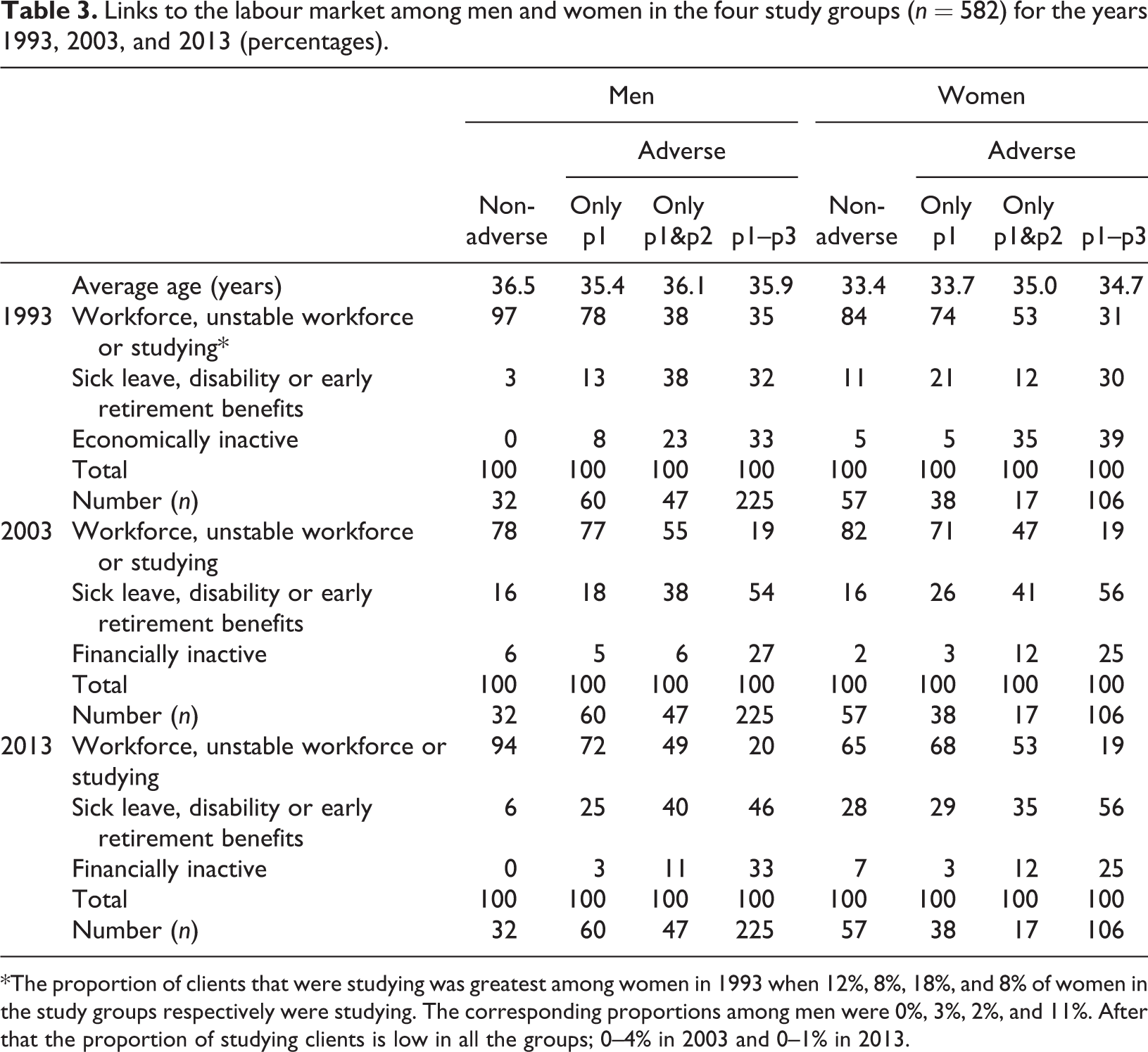
*The proportion of clients that were studying was greatest among women in 1993 when 12%, 8%, 18%, and 8% of women in the study groups respectively were studying. The corresponding proportions among men were 0%, 3%, 2%, and 11%. After that the proportion of studying clients is low in all the groups; 0–4% in 2003 and 0–1% in 2013.
Being categorised as economically inactive usually implies being in a marginalised situation, largely excluded from society, compared to, for example, those in the middle category (sick leave, disability or early retirement benefits) who could be said to be part of society. A tendency in the results was that longer time-periods as adverse (in terms of crime and substance abuse) also had a negative effect in this sense, i.e., the longer the time being adverse, the greater the proportion of financially inactive individuals.
Discussion
The main aim of the present study was to follow up on social inclusion/exclusion in clients registered for treatment in 31 in-patient treatment units in Sweden in 1982 and 1983. Gender-specific analysis was performed regarding the group’s development in terms of criminality, substance abuse and labour market status.
As the first step, social inclusion was operationalised in a somewhat crude form: the persons were not allowed to have been active in crime or in heavy drug use. To be defined as “non-adverse”, no criminal activity nor any treatment for substance abuse during a nine-year period were allowed. Thus, the crude measurement was balanced due to the relatively long time the persons were to stay away from criminal activity or treatment. In a second step, the outcome in terms of labour market status in 1993, 2003 and 2013 was investigated.
When mortality was followed up in the SWEDATE group, standardised mortality rates (SMR) were in general higher for men, except for the group reporting alcohol as their main form of abuse (von Greiff et al., 2018). Thus, the women in the group had survived longer in general. The present study indicates that among those who survived, the women also seemed to have been more successful in terms of social inclusion both at an aggregated level (Figure 1) and when the individuals are followed in pathways during the follow-up period (Figure 2). One possible explanation for this result is that crime is included in defining inclusion/exclusion and that crime is more common among men than among women.
At baseline, the group was characterised as being in a vulnerable and marginalised situation. Thus, this type of client is generally considered as a group with a poor long-term outcome (cf. Simpson et al., 2002) and a group that finds it difficult to go from being socially excluded to being socially included (Alm, 2015; Hser, 2007). However, 17% of the women seemed to have managed to stay away from substance abuse and crime, at least in the sense of not being in any treatment or sentenced for any crimes during the entire follow-up period of 27 years. The corresponding percentage was much lower for the men at 5%. On the other hand, 9% of the men managed to go from being criminal and/or treated for substance abuse during the first nine years to staying away from crime and treatment during the last 18 years of the follow-up. Again, this proportion was higher for the women, but only slightly (12%). Previous research on gender differences among substance users indicates that criminality is higher among men (Gjersing & Bretteville-Jensen, 2014; Ravndal, Lauritzen, & Gossop, 2015). The present study might indicate that gender differences change over time. However, this needs to be further investigated in order to confirm this suggestion and understand the processes involved.
In line with previous research (cf. Davstad et al., 2013; Olsson et al., 2001; Ribiero et al., 2007), the labour market status was low among clients who had experienced substance abuse or crime (according to the definitions used in the present study) during all three follow-up periods. However, in the last follow-up in 2013, the majority of the clients defined as non-adverse for the last nine years were in some way established in the labour market (including studies). The women were better educated, although the gender difference is smaller than in the general population (SCB, 2018). In total, about two fifths of the group were in some way established in the labour market. This is twice as high as in a previous Swedish long-term follow-up on a cohort of “first-generation addicts” also using employment as a measure of social inclusion on an age-comparable study population (56 years old compared to 42–62 years old in the present study), showing that one fifth of the cohort was socially included (Alm, 2015). One reason for this difference is that Alm uses a stronger definition of labour market establishment when defining social inclusion. However, data from Alm’s study show that if “unstable workforce” were included, establishment in the labour market would still be higher in the present study.
Since being non-adverse requires that the person is not active in crime, the results may to some extent be related to the “age–crime curve” establishing that criminal activity increases and peaks during adolescence and declines as individuals enter adulthood (e.g., Piquero et al., 2003; Sweeten et al., 2013). Thus, this might have an impact on those who survive and become non-adverse between the first nine-year period and the second nine-year period but not between the second and third period. Being defined as non-adverse over a nine-year period could be compared with the period of five years of abstinence that is often used as a definition for “stable recovery” (cf. McLellan, 2010; The Betty Ford Institute Consensus Panel, 2007). Thus, the fairly high proportion of clients moving between being adverse and non-adverse during the follow-up might support the perspective suggesting that dependence is not to be considered as chronic (Klingemann & Sobell, 2007).
Limitations and strengths
The dominating reason for not being interviewed was dropout from treatment before the interview, which might indicate a more progressed abuse and could imply higher adverse outcome in this group. Thus, an adverse outcome in this study might be somewhat underestimated since it is limited to those who were interviewed. Another limitation concerns the fact that the women in the study seemed more socially included than the men. This could probably partly be explained by the fact that crime is used to define inclusion/exclusion since crime is more common among men than women.
The strength of the study lies foremost in that it includes the majority of the clients who were treated for problems with drug abuse in Sweden in 1982 and 1983 and the length of the follow-up. However, the results are presented as descriptive statistics, rather than inferential statistics, since our study population is neither a random sample nor a total population, and thus the results should be interpreted with caution.
Footnotes
Ethics
This research project was scrutinised and approved by the Ethical Review Board in Stockholm, Sweden (2015/329-31/5, 2015/1205-32, 2016/542-32/5).
Notes
Acknowledgement
We are grateful to Professor Anders Bergmark, Department of Social Work, Stockholm University, who was a member of the research team leading the SWEDATE project and who has supported the present follow-up project.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was funded by the Swedish Research Council for Health, Working Life and Welfare (Grant # 2015-000980).