
Abstract
Objective:
The aim of the present study was twofold. The first aim was to explore how frequently physicians evaluate driving fitness when a patient has a serious alcohol problem, which is accomplished by examining differences in physicians’ compliance with their intervention/notification obligation among different alcohol-related ICD-10 diagnoses. The second aim was to explore how many heavy alcohol users have a valid driving license.
Methods:
Data from all patients with an alcohol-related ICD-10 diagnosis code as a cause of a hospital visit were collected during a three-month period from Kuopio University Hospital and North Karelia Central Hospital.
Results:
Eighty-one percent (81%) of patients with alcohol-related ICD-10 diagnoses were heavy alcohol users and had alcohol withdrawal syndrome, alcohol-related organ disease or multidrug abuse combined with alcohol abuse. The driving fitness of these patients was significantly reduced, and the health requirements of the driving license were not met. Physicians evaluated driving fitness for only 20% of alcohol-related hospital visits/hospitalisations. Moreover, fitness to drive was evaluated in only 24% of cases of a patient with a major alcohol problem and a valid driving license. Driving fitness was most frequently evaluated in cases with alcohol-related convulsions (74%). In total, 80% of patients with a major alcohol problem had a valid driving license even though the requirements of driving fitness were not met.
Conclusions:
The obligation to evaluate the driving fitness of heavy alcohol users is often neglected, except in cases of alcohol-abuse-related convulsions. Physicians should play a greater role in monitoring road safety, or sanctions should be set for failures to obey the obligations. The driving fitness of a patient hospitalised due to alcohol use should be assessed more regularly. Cognition problems related to alcohol-related liver disease/alcohol-related dementia are probably often overlooked. Alcohol-abuse-related conditions are poorly recognised and remain unreported to the authorities.
Driving under the influence of alcohol (DUI) is a major traffic problem. Alcohol plays a role in one-quarter of all fatal motor vehicle accidents in Finland (Holopainen, 2015). Alcohol dependency not only is a risk factor for DUI but also causes alcohol-related organ complications and alcohol-related withdrawal symptoms. These conditions and hangovers increase the risk of motor vehicle accidents (MVAs) (Smith & Dischinger, 2011). From 2012–2016, a total of 213 fatal MVAs were caused by drunk drivers in Finland (26 to 54 per year). In many cases, a fatal motor vehicle accident is the final end-point of long-standing alcohol abuse. Alcohol abusers are also heavy users of healthcare services and drugs affecting the central nervous system. Alcohol withdrawal syndromes, alcohol-related trauma, alcohol intoxication, alcohol-related organ disease (liver diseases) and alcohol-related dementia are common reasons for hospital visits (Koch-Weser, Sellers, & Kalant, 1976). Alcohol abuse, alcohol addiction and a variety of alcohol-related health problems constitute an extensive challenge for practitioners working in hospitals and in general practices. Although alcohol-related road accidents represent only a small portion of all instances of alcohol-related harm, driving under the influence of alcohol causes approximately 25% of all road fatalities in the European Union (Mayhew & Ireland, 2015).
Our hypothesis is that healthcare professionals neglect their legal obligations by not evaluating driving fitness and/or notifying the police even when patients have serious and long-standing alcohol problems. The driving ability of these patients may be impaired, for example, when the driver is suffering from alcohol withdrawal syndrome (convulsions, falling asleep accidents, or observational failures/distraction) or through alcohol-related mental/behavioural disorders (Sutherland, Sheedy, & Kril, 2014). Chronic liver failure may lead to hepatocerebral degeneration and cognitive problems (Renjen, Khanna, Rastogi, & Khan, 2013). Patients with any alcohol-related hospital contact are at a higher risk for cirrhosis development (Askgaard et al., 2017). Based on the third European Commission Directive on the Driving License (Annex III), “Driving licenses shall not to be issued to, or renewed for, applicants or drivers who are dependent on alcohol or unable to refrain from drinking and driving” (EUR-Lex, 2006: L 403/50). However, little information is available concerning compliance with this directive in different EU countries.
Materials and methods
Ethics and study outline
The study plan was reviewed and approved by the Research Ethics Committee of the Northern Savonia Hospital District and Trafi (Finnish Transport Safety Agency). All hospital visits and hospitalisation periods related to alcohol abuse from January–March 2016 were investigated. The data were collected from the University Hospital of Kuopio and the North Karelia Central Hospital. These hospitals are situated in eastern Finland. For all patients, a search was carried out for ICD-10 diagnosis code F10. This search covered all alcohol-related visits provided that the use of alcohol was diagnosed. The diagnosis may have been the primary or secondary diagnosis of the hospital visit. If a patient had more than one alcohol-related hospital visit, the ICD-10 code was registered from the first hospital visit (45 patients had more than one visit during the three-month period). Each patient was recorded only once in the final data. The patients’ medical records were searched and analysed (including the primary healthcare records in the case of the hospital visit) by the first author. Thereafter, we assessed the following questions from the patient records: (1) Were diagnostic signs of alcohol-use disorder (AUD) present? (2) Did any collateral drug dependence affect their driving ability? (3) Were any attempts made to evaluate driving fitness? (4) Were there any signs of an impaired driving fitness? (5) Did the patient have a valid driving license (from Trafi). In the study, we used the Stata 14.0 (StataCorp, TX, USA) software.
Criteria for alcohol dependence
Alcohol dependence is defined in the Finnish Current Care Guidelines (i.e., the Finnish guidelines for healthcare professionals that are intended as a basis for treatment decisions; Alho et al., 2015). At least three of the following criteria must be established for at least one month or repeatedly over the past year for a period shorter than one month: A strong desire or compulsive need to use alcohol A reduced ability to control the use of alcohol and the alcohol dose Withdrawal syndrome from the use of alcohol Enhanced tolerance of alcohol Focus on the use of alcohol so that other sources of pleasure and interests are replaced by drinking and recovering therefrom Continued alcohol abuse despite drawbacks
In addition, the Current Care Guidelines recognise that alcohol dependence is likely if the alcohol concentration in the patient’s blood or breath is more than 1 per mille at a doctor’s appointment, more than 3 per mille in any situation or more than 1.5 per mille without signs of intoxication. These criteria were taken into account when estimating the level of alcohol abuse.
Driving fitness and notification obligation in Finland
In Finland, health requirements for a driving license are based on the EU directive 2006/126/EY, which has been implemented on the national level through the Driving License Act (2011/386) and Trafi’s Instructions to Physicians on Assessment of Driving Fitness. Moreover, the Driving License Act includes certain other relevant provisions, including 21 §, which obligates the physician, regardless of Finnish law confidentiality obligations, to notify the police when he or she concludes a holder of driving license is not able to fulfil the applicable health requirements due to a non-temporary impaired state of health or continuous abuse of intoxicants. Under Finnish legislation, a DUI offender may apply for the alcohol interlock programme “health-based interlock”, which enables a conditional driving license. Admission to the programme requires an appointment with a doctor or another healthcare professional regarding the alcohol abuse of the applicant. The programme is voluntary for DUI offenders, of whom 500 participate in the programme each year. Based on the 2018 statistics of the Police of Finland, more than 13,000 DUI alcohol and 1600 alcohol+drug cases were recorded in 2017.
Based on Finnish Transport Safety Agency regulations, if alcohol dependence is at least likely (as defined above), the driving fitness criteria are not met. These drivers are not allowed to drive, and physicians must deny driving privileges and start alcohol intervention. Alcohol dependence is a contraindication for driving based on the EU directive. In cases with alcohol dependence/alcohol-related withdrawal syndrome, physicians are obliged to order at least one to three months of driving cessation and to initiate treatment and follow-up procedures for treatment of the addiction. If the response is inadequate and the driving ban continues for more than six months, physicians are obligated to provide this information to the traffic authorities. No patients who are addicted to, or are misusers of drugs or central nervous medicines are allowed to drive under any circumstances.
In Finland, a doctor shall (verbally) deny driving privileges for at least three months after an alcohol-related seizure if the patient has a Group 1 driving license (motor passenger cars and motor cycles). For patients with a Group 2 driving license (large lorries and professional drivers), the traffic authorities should be notified after one convulsion.
Results
Sample data
The data were collected from 431 patients (Table 1). The ages of the patients ranged from 11 to 88 years (standard deviation: 15.9, mean age: 48.4, median age: 51). The gender distribution was 327 (76%) males and 104 (24%) females. Among all patients with alcohol-related ICD-10 diagnoses, driving fitness was evaluated in only 20% (88/431) of the cases (either during the hospital visit or in the recent past). Driving fitness was evaluated in 24% (83/347) of cases in which a patient had a major alcohol problem. The proportion of males was higher in the group of alcohol abusers (78%) than in the group of non-alcohol abusers (65%) (based on the Chi-square statistic; the result is significant, p < 0.05).
Age and gender distributions of the sample.
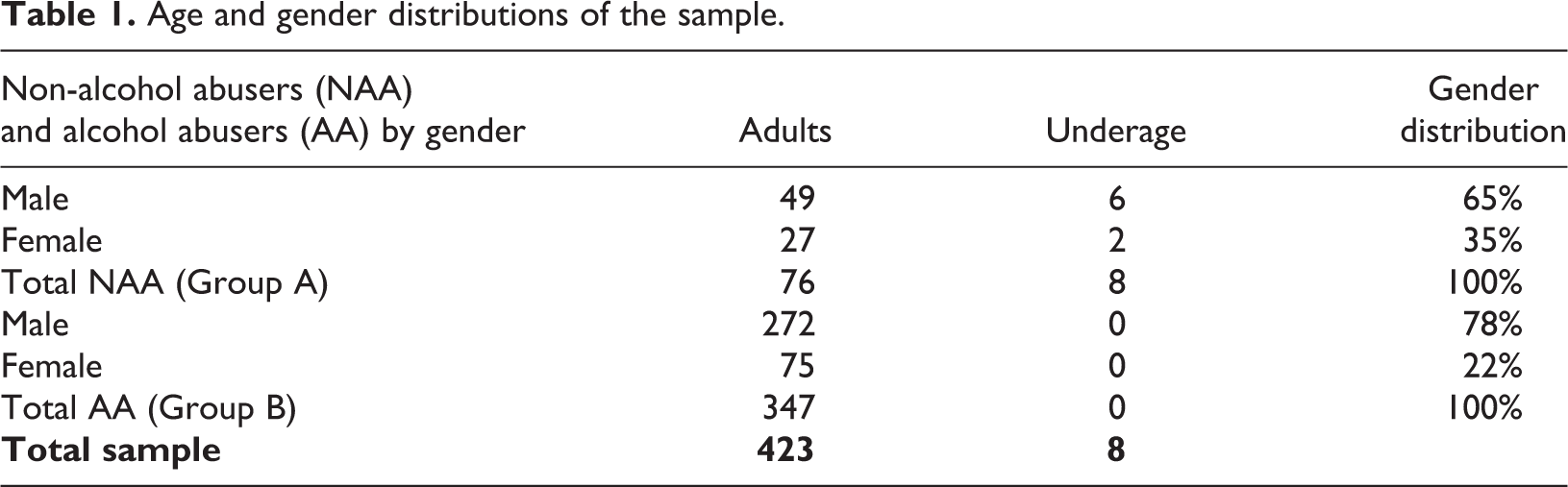
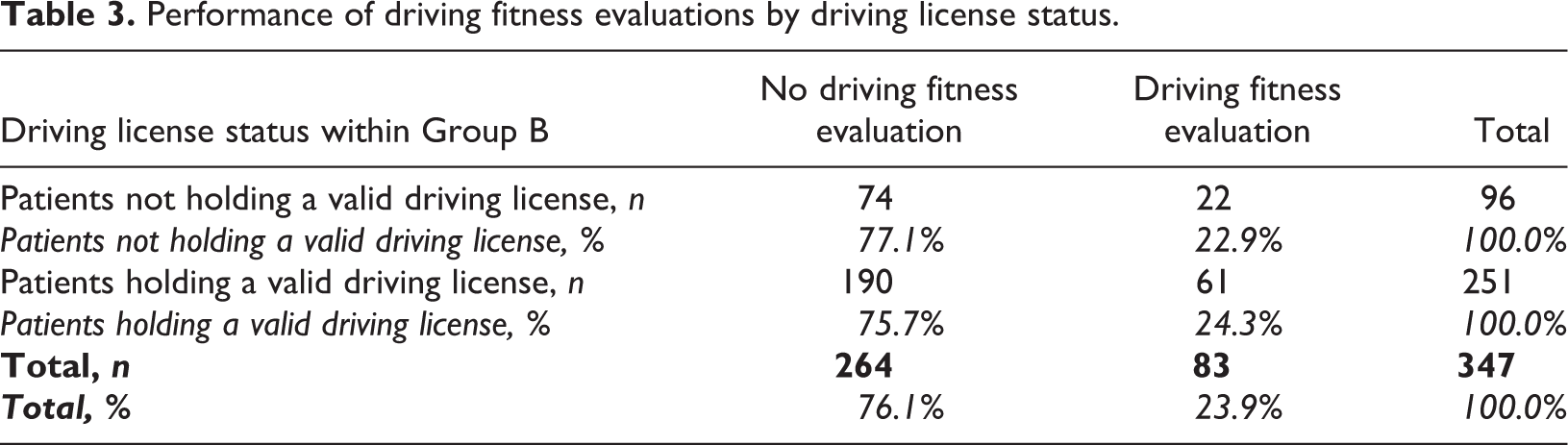
In total, 84 patients (19.5%, Group A) were categorised as non-alcohol abusers (typically one isolated alcohol-related hospital visit without a history of alcohol problems), whereas 347 (80.5%) patients had a serious alcohol problem, alcohol-use disorder (AUD), polysubstance abuse problem or serious alcohol withdrawal syndrome (Group B). Evaluations were performed by the authors based on the medical records and Trafi’s regulations. Among Group B (patients with an AUD etc.), driving fitness was evaluated (or the patient was found not to have a valid driving license) in 83/347 (23.9%) cases. Drivers in Group B did not fulfil the driving fitness criteria because of serious alcohol/drug abuse based on Trafi’s regulations.
Proportion of diagnoses and assessment of driving fitness
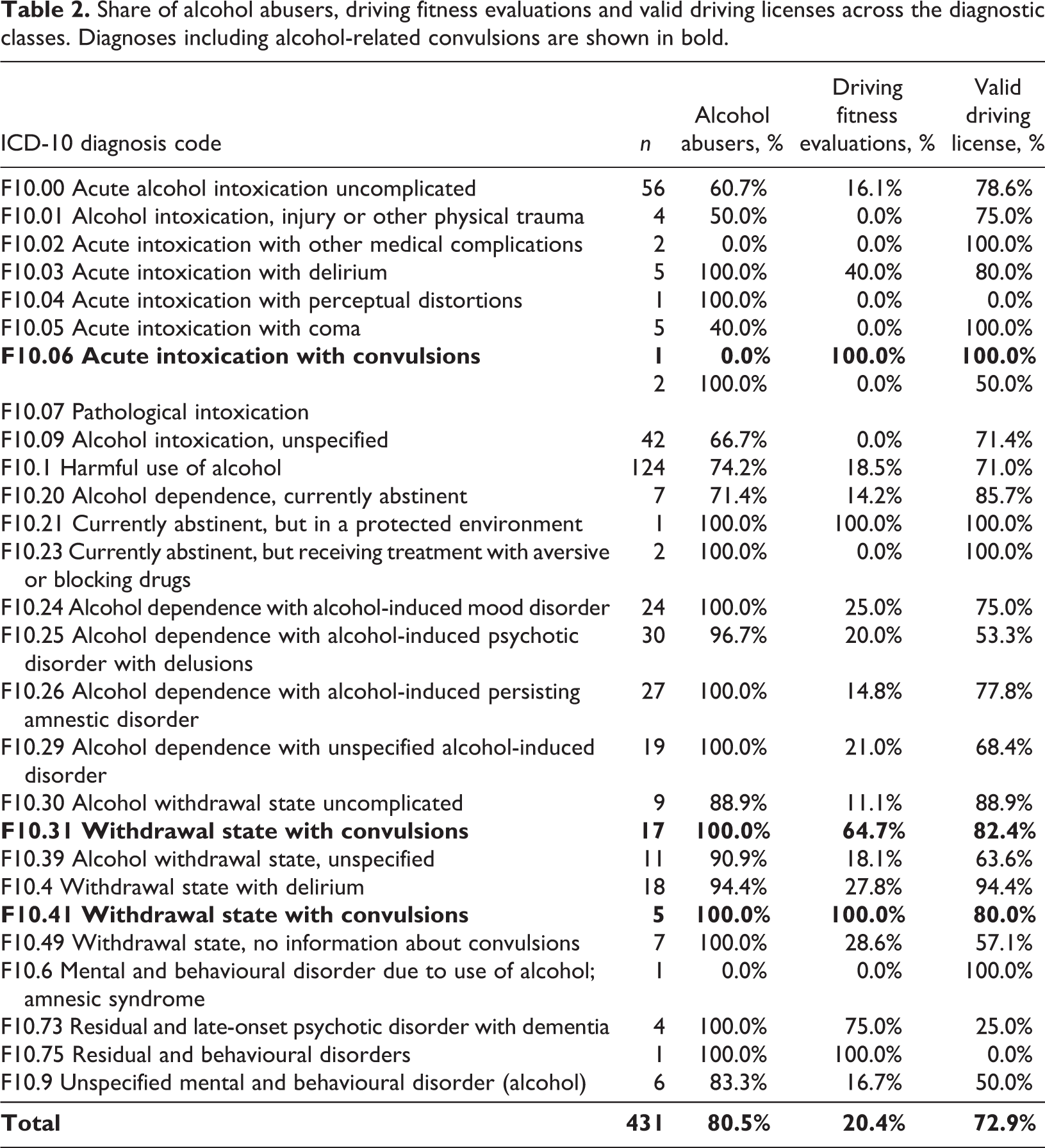
The most frequently diagnosed group was F10.1 (Harmful use of alcohol); among this group, 74% (92/124) of the patients had an AUD or were heavy alcohol users (multiple alcohol-related hospital visits/alcohol-related organ disease) (Table 2). Patients with a diagnosis of F10.24–F10.29 (these diagnoses contain a definition of alcohol addiction) had a major alcohol problem, and only one patient (1/99) with an F10.25 diagnosis could not be verified as alcohol-dependent. Nevertheless, 68% (68/99) of the patients in this group had a valid driving license, but the physicians conducted a driving fitness assessment in only 20% (20/99) of cases (see Table 1).
Share of alcohol abusers, driving fitness evaluations and valid driving licenses across the diagnostic classes. Diagnoses including alcohol-related convulsions are shown in bold.
Performance of driving fitness evaluations by driving license status.
In total, 23 patients had an alcohol-related convulsion diagnosis (ICD-10 diagnosis codes F10.31, F10.41, and F10.06) during the three-month period; driving fitness was evaluated in 73.9% (17/23) of these cases. Physicians evaluated driving fitness significantly more actively if a patient had alcohol/withdrawal-provoked epileptic convulsions than when other manifestations of alcohol abuse were present (Chi-square test: χ2, (2) = 34.51; p < 0.005). Among this group, if convulsions were excluded, the driving fitness assessment was performed in only 20.4% (66/324) of cases. However, the driving ban was often temporary even for convulsion-related visits when the patient suffered from chronic alcohol abuse.
A total of 12 patients were diagnosed with alcohol-related dementia/mental disorder (F10.6, F10.73, F10.75, and F10.9). Driving assessments in the medical records were found for five of these patients (5/12). Five (5/12) of the patients had valid driving licenses.
Driving licenses
Seventy-seven percent (332/431) of all patients had valid Group 1 driving licenses and 30% (99/431) also had Group 2 driving licenses. Seventy-three percent (252/347) of the patients with AUD/heavy alcohol use had at least a Group 1 driving license and 25% (87/347) also had a Group 2 driving license. Among the patients with alcohol-related convulsions, 83% (19/23) had a valid Group 1 driving license and 22% (5/23) also had a Group 2 driving license. Seventy-two percent (n = 251) of the patients with an alcohol problem had valid driving licenses.
In total, eight patients were non-adults (younger than 18 years old). None of the minors had a serious alcohol problem. Driving assessments were not performed for any of these youngsters. The age limit for driving a moped in Finland is 15 years. Among these patients, child protection authorities were informed as a rule. Especially in cases of minors, early intervention is vital because early drinking is linked to a higher lifetime AUD risk (DeWit, 2000).
Discussion
Patients with serious alcohol addiction often have a history of repeated hospital visits due to alcohol withdrawal syndrome or alcohol-related organ complications. Based on our study, more than 80% of all alcohol-related hospital visits were made by alcohol abusers or heavy alcohol users. Most patients had a valid driving license. However, physicians rarely executed any actions even when alcohol dependence was diagnosed. Patients with alcohol-related convulsions were an exception. Health requirements were evaluated better if the patient had convulsions, probably because the guidelines for the driving requirements are better known for epilepsy. The physicians probably evaluated driving fitness due to the convulsion per se instead of due to the underlying alcohol problem. In a few cases, the physician asked the patient whether he/she had a valid driving license and the patient denied having one; however, the driving license register revealed that these drivers indeed had a valid driving license. Doctors should be able to determine whether the patient has a valid driving license.
Doctors’ obligations to notify were studied in southwest Finland in 2015 (Löytty, 2015). According to the study, physicians made 9% of all driving license decisions based on a self-imposed notification. Approximately 10 clinicians were responsible for more than 70% of all notifications. Another study suggested that 10% of fatal MVAs could be avoided if physicians would comply with their notification obligation (Tervo, Koisaari, & Tervo, 2016). Alcohol-related health problems are underrepresented in all notifications, although alcohol is the major traffic obstacle and a public health problem.
Doctors need education in traffic medicine
The results highlight the importance of education in traffic medicine. Doctors are dedicated to dealing with medical issues, and legal obligations may be forgotten, or time may be lacking. Driving fitness should receive attention in hospitals and during doctors’ appointments. Driving fitness should always be evaluated for patients with repeated alcohol-related visits, because these patients have a history of alcohol abuse. In many cases, starting with a temporary driving ban and initiating treatment and follow-up procedures for the treatment of addiction are easy steps.
Driving health and alcohol abuse: Obstacles and challenges
Education of physicians in traffic medicine in cases of alcohol abuse is useless if there are insufficient resources and tools to evaluate the degree of alcohol abuse and if no treatment possibilities are available. Different methods of implementing brief interventions should be assessed in general practice. A lack of time is a challenge in clinics when assessing alcohol abuse (Graham, Maio, Blow, & Hill, 2000; Kaner, Lock, McAvoy, Heather, & Gilvarry, 1999; Seppa, 2011) both in general practice and emergency medicine. Emergency departments (EDs) are appropriate places to implement brief interventions based on doctors and patients (Schermer, Bloomfield, Lu, & Demarest, 2003), but clinical inertia has been identified as a barrier in the ED (Huntley, Patton, & Touquet, 2004). Alcohol abuse is one of the most difficult areas during a doctor’s medical assessment of drivers in Norway (Brækhus, Wyller, & Engedal, 2010). In Sweden, a study showed that only one out of 1000 patients diagnosed with alcohol dependence was reported to the relevant authorities under the Swedish Driver’s License Act (Bjerre, Heed, & Kers, 2004). The ignition interlock programme seems to also reduce alcohol consumption among interlock users (Bjerre, 2003), and alcohol interlocks should be used more broadly for drunk-driving offenders; half of Australian high-risk drinkers stated that they would use interlocks personally (Bishop, Liu, Stephens, & Fitzharris, 2017). In Finland, 13 health-based alcohol interlock driving licenses were granted in 2014 (Löytty, 2015).The correlation between total alcohol consumption in Finland and alcohol-related fatal crashes is an important relationship; political decisions regarding alcohol prices are associated with alcohol-related harm (Herttua, Mäkelä, & Martikainen, 2011), which also manifests in traffic safety (Kalsi, Selander, & Tervo, 2018).
Doctors should treat alcohol addiction with the same seriousness as any other disease. In cases of alcohol-related hospitalisation, driving fitness should be evaluated in a manner similar to epilepsy or eye diseases. If an alcohol abuser undertakes to follow the treatment and complies with regular medical examinations, driving medical requirements can be re-evaluated by addiction medicine specialists or physicians familiar with substance-abuse assessments if the patient does not endanger traffic safety (Finnish Transport Safety Agency instructions; Trafi, 2015).
Motivation to stay sober can be improved if one’s goal is to reclaim the driving license. All drunk drivers cannot be screened from traffic through road safety raids by the police alone. Physicians often play a key role in the recognition of an alcohol problem in its early stages. An opportunity to provide addiction treatment must be provided for patients suffering from AUD.
Strengths and limits of the study
The present study was a two-centre study with a sufficient sample size. Electronic health records permitted a comprehensive investigation of each patient’s health records. Therefore, the severity of the alcohol problem could be reliably assessed in most cases. Unfortunately, DUI convictions were not available from the road safety agency. Comparing how many of the drivers had a history of DUI convictions or a controlled driving license with alcohol interlock would have been interesting. There may have been cases where driving fitness was evaluated but not registered in the medical records. This study included only two hospitals, and the situation might be different elsewhere in the country.
Conclusions
Alcohol remains a major traffic problem, and the requirements of EU directive 91/439/EES of 29 July 1991 are not implemented in practice; physicians fail to evaluate driving fitness in most cases even when a patient has a substantive alcohol-use disorder. Is issuing a directive worth the time if it is not known and respected in the EU? The notification obligation is not practiced in Finland even in cases where there is a severe alcohol problem. Paradoxically, doctors obey the law if the driver has a neurological disease affecting fitness to drive. Why do doctors not follow their obligation to notify authorities of impaired fitness to drive in the case of alcohol abusers? Perhaps clinicians use simple and proper tools to estimate when the alcohol problem is serious enough to impact driving safety. Patients may claim that they only drive when they are not under the influence of alcohol. Our study suggests that alcohol remains a taboo when assessing fitness to drive. Seizures induced by chronic alcohol abuse (“alcohol-induced epilepsy”) were the most common cause of temporary driving bans ordered by physicians. In most of these cases, the patients suffered from an advanced AUD, and their fitness to drive was permanently impaired. These drivers constitute a risk in traffic even when they are not under the influence of alcohol. Advanced-stage AUD should be an absolute contraindication for a driving licence with or without an ignition interlock. Doctors overlook an AUD in regard to driving fitness. Doctors should change their way of thinking when they are evaluating driving fitness; they must consider road safety if a driver has a substance-use problem or mental illnesses (or aviation safety, such as the case of the Germanwings suicidal crash). If doctors do not respect their obligations, the rights of road users are violated. In the end, the solution to the problem is not to increase driving bans but instead to identify alcohol abusers and guide these patients to treatment more actively.
Footnotes
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.