
Abstract
Background and aims:
For people trying to stop using alcohol or other drugs (AOD), the process is often characterised by periods of abstinence followed by relapse into their previous drug-related way of life and subsequent re-entry into the treatment system. There is a call for greater attention to the how of these transitions, with a special focus on the phase of leaving treatment. The aim of this article was to get a better understanding of the transformation of practice when moving from a drug-using to a non-using lifestyle by exploring the experience of (1) the involvement in treatment settings, (2) the process of leaving treatment, and finally, (3) the early phase of changing everyday practice into a drug-free way of living.
Method:
The article takes on a social practice approach, in particular Bourdieu’s concepts of habitus, “doxa” and field to analyse 17 in-depth interviews with Norwegian men and women seeking treatment for problems resulting from the use of drugs and/or alcohol.
Results:
The study shows that the support of professionals operates as transitional relations that can bridge the transformation from a drug-using to a drug-free life, by providing a social web of relations, positions, settings and activities. However, leaving treatment and establishing AOD-free practice involves moving into something unknown in the sense that there is no embodied, taken-for-granted knowledge about how to relate to a world where drug use is not the focal point of existence.
Conclusions:
The process of change, then, involves being exposed to an existential feeling of maladjustment. To get beyond the feeling of maladjustment, and get into the doxic mode takes time, and involves reconfiguration of habitus through reorientation of social settings, relations and networks. The treatment system could potentially develop a continuum of support during these transformations.
Patterns of alcohol or other drug (AOD) use are extremely heterogeneous, and despite of what might be a common impression, a large percentage of people struggling with problems related to AOD use eventually overcome their problems (Hser & Anglin, 2011; McIntosh & McKeganey, 2001). A relatively smaller percentage (between 20% and 30%) of this heterogeneous population of individuals facing problematic AOD use actually seeks out professional treatment for help with their related difficulties (see, e.g., Heyman, 2013; Willenbring, 2010). It was this group of individuals that was the focus of our study. For many of these individuals alcohol or other drug use has become the focal point of their existence, permeating their way of life with a range of adverse outcomes, which can be a strong motivator to start life-changing processes to overcome their problems (Årstad, Nesvåg, Njå, & Biong, 2018; Neale, Nettleton, & Pickering, 2013). Because of the accumulated negative consequences of their AOD use, moving from a drug-using to a non-using lifestyle often involves a dramatic and demanding transition, implying a process of detoxification followed by changes in everyday living regarding daily routines, relationships and social network, activities, housing, education and/or employment and more. Despite the motivation and desire to make substantial and sustainable lifestyle changes, the process of succeeding is often characterised by periods of abstinence followed by relapse into the previous drug-related way of life and subsequent re-entry into the treatment system (McKay, 2017; McKay, Franklin, Patapis, & Lynch, 2006; Neale et al., 2013). The extended nature of these processes indicates their difficulty for the people involved, including friends and family, as well as the considerable problem and an ongoing challenge they cause at the level of society, for the treatment system and for policy makers (Hser & Anglin, 2011; McKay, 2017).
A lot of effort has been made to develop effective treatment interventions, programmes and models to help people overcome their AOD-related problems. Even though improvements are evident, one could still hope for better success (McKay, 2017; White & Kelly, 2011). Addressing this challenge, addiction treatment is asked to reconnect to the larger and more enduring process of personal and family recovery (White & Kelly, 2011). In general, consistent findings in treatment evaluation research are that the length of stay in treatment is positively associated with favourable treatment outcomes (Hser & Anglin, 2011, pp. 20–21). Additionally, a substantial volume of evidence suggests consistent benefits of abstinence-oriented social networks and involvement in self-help groups in facilitating treatments for substance-use disorder (Hser & Anglin, 2011; Kelly, 2003; Kelly, Stout, Magill, & Tonigan, 2011; Moos, 2007). The literature on recovery has recognised that the struggle of making pervasive lifestyle changes is as complex and unique as the individuals involved, including multiple dimensions and factors interwoven with the broader social context of individuals’ everyday lives (Cloud & Granfield, 2008; Hser & Anglin, 2011; Laudet, 2007; Leamy, Bird, Boutillier, & Slade, 2011; Ness, Borg, & Davidson, 2014; White, 2008). Other studies (see, e.g., Best, McKitterick, Beswick, & Savic, 2015; Cloud & Granfield, 2008), bring forward the concept of social capital to understand the individual journey of change-making processes, highlighting “social capital as a critical determinant of building personal strengths and resources and for tapping into community supports and resources” (Best et al., 2015, p. 272). Thus, there is strong evidence for acknowledging that moving from a drug-using to a non-using lifestyle is a long-term process occurring in communities predicated on relationships and meaningful activities (Best, Beswick, Hodgkins, & Idle, 2016; Best et al., 2015; McKay, 2017).
The body of knowledge referred to above has broadly been organised around variable-based explanations, highlighting significant components, factors and social resources involved in the process of change (Neale et al., 2015; Orford et al., 2006; von Greiff & Skogens, 2013). However, the subjective experience of early attempts to make lifestyle changes, and the complex dynamics of these changing practices as a profound social reality have received less attention. There is a need for a better understanding of these long-term processes of recovery, and their underlying mechanisms that sustain or lead to change of drug-use behaviour (Hser & Anglin, 2011; White & Kelly, 2011). Through a social practice approach, with the performative character of social life in the foreground (Halkier & Jensen, 2011; Hughes, 2007; May, 2001; Nettleton & Green, 2014; Orford, 2008), we hope to provide useful ways of thinking about the possibility of change in everyday practice in the case of people with problems related to AOD use. We propose to address this by focusing on the interplay between context, circumstances and practice. Further, by standing within the discipline of sociology, we contribute to a multidisciplinary perspective within the field of addiction and recovery.
Based on the above, the aim of this article was to gain a better understanding of the transformation of practices when moving from a drug-using to a non-using lifestyle by exploring the subjective experience of (1) the involvement in treatment settings, (2) the process of leaving treatment, and finally, (3) the early phase of changing everyday practice into a drug-free way of living. Through listening to the stories told by people who had made efforts to make major lifestyle changes, this study sought to elucidate the reorientation of practices in the early phase of theses changing processes.
Background and theoretical perspective
“You have to turn everything around…EVERYTHING needs to change!” This is an account from a participant of this study, which captures some of the essence of their experience of what needed to be done when giving up long-term heavy drug use. The process of reforming and rebuilding lives involves profound changes in everyday practices, relationships and social settings (Hughes, 2007; Maruna, 2001). Along with Weinberg (2000, 2002), Nettleton, Neale, and Pickering (2011), Nettleton and Green (2014), and Hughes (2007) bring forward the sociological literature on social practice and on the body when linking the internal environment of the body and the external environment of social context, which gives rise to actions, experience and identity. They argue that the transformation of moving from a drug-using to a non-using life is rooted in the materiality of the body, in habitual action as well as social practices, which are, in turn, bound up with identities. Moreover, they define habitual action as bodily action – the social is inscribed onto bodies.
This line of thinking is related to the social practice approach (Nettleton & Green, 2014; Weinberg, 2002) and social practice theory (SPT) (Keller, Halkier, & Wilska, 2016; Reckwitz, 2002) which draw on Bourdieu’s theory of practice and cover diverse disciplines and fields of research. A social practice approach calls attention to understanding social life and what the conditions of possibility for transforming and reconfiguring social practices might be (Halkier, Katz-Gerro, & Martens, 2011; Keller et al., 2016; Nettleton & Green, 2014), and has proven to be useful in providing insight into health practices and health behaviour, consumption practices, as well as practices of addiction and recovery. At the core of this perspective we find the ambition to synthesise both social and mental structures (Nettleton & Green, 2014), by focusing on the relational processes at play (a) between individuals, (b) between individuals and social context (field), (c) between individuals, context and resources, and (d) in the context of structural forces and embodied manifestations. This allows us to understand the complex experience of transforming living practice as a relational, embodied and social process. Nettleton and Green (2014) illustrate that Bourdieu’s theory of practice and, in particular, the concepts of habitus, field and doxa can be useful to identify the conditions of transformation of practices. We believe this approach is relevant when examining the transformation of practice people undertake when leaving long-term heavy AOD use.
Bourgois and Schonberg (2009) use the concept of habitus in their ethnographic studies to capture the complexity of why people act and feel the way they do, why public interventions do not work as expected and why it is so difficult to stop using drugs. Without substantial institutional resources, it is difficult for long-term chronic users to figure out how to pass the time of day. They have to construct a new personal sense of meaning and dignity. Instead, they often fall back on their more familiar and persuasive righteous dopefiend ways of being in the world, and they seek out old drug-using friends and acquaintances. (Bourgois & Schonberg, 2009, p. 281)
As shown by these authors, a long period of extensive AOD use influences the user’s embodied, taken-for-granted understanding of the social world and one’s place in it. It influences the user’s perception of the possibilities and boundaries that exist for them in the social world. Thus, the process of transformation, the recovering bodies (Nettleton et al., 2011) or the migrating identities (Hughes, 2007), must acquire a new range of skills to manage multifaceted demands in the landscape of different social arenas and social networks, meaning that involvement in new non-using practises includes being exposed to unfamiliar situations and realties in which the embodied, habitual action not yet is establish (Hughes, 2007; Nettleton et al., 2011). This is a demanding and challenging process and makes people vulnerable to relapses. The deep entanglements of previous drug-using practice create an inevitable pull which one must disengage from (Hughes, 2007; Martin, 2011). Nettleton’s study participants describe the challenge of everyday practices as a “nightmare”, involving all kinds of emotional troubles and “dys-appearances” – things that do not make any sense – which require attention (Nettleton et al., 2011, pp. 348–349). In these processes the engagement and involvement of formal services and service networks is described by research participants to be of great importance, potentially allowing them to pursue new trajectories in living and identity practices (Hughes, 2007; Neale et al., 2013; Nettleton et al., 2011).
Draus, Roddy, and Asabigi (2015) take the concept of habitus in their analysis of women’s accounts of their transition from active substance use to a recovery-oriented existence. In their study they take the social context of residential substance abuse treatment as a point of departure for studying the process of adjustment from active street sex work to life in structured substance abuse treatment. Here, the authors argue that the treatment process represents a deliberate modification or reconstruction of habitus. In order to understand the process of undoing the deeply embedded (embodied) adaptations that result from long-term drug use, Draus et al. (2015) argue that the restrictive environment and rules of conduct that characterise the social setting of treatment can provide expanded opportunities and establish new habitual actions and identities. However, considering the phase of adjustment from the social setting of treatment to drug-free living, the inevitable pull towards previous lifestyles might play itself out. In the study by Draus et al. (2015) the authors expected, and found, that desired behavioural and identity transformed in the participants as the external environment changed in terms of social networks, geographic settings, economic resources and opportunities. Hence, changing the exterior environment and social network once again when leaving treatment, another readjustment is needed, exposing newly establish behavioural and identity transformation to risk.
With relevance to this and to provide a potential understanding of why the risk of relapse after discharge from treatment is high (which is in the margin of, but also evident in the study of Draus et al., 2015), Weinberg (2000) argued that drug abuse treatment discourse can be differentiated into two contrasting ecologies: (1) being “in” the programme, meaning being within the social world of a programme in which people can take control over their addictions; or (2) being “out there”, referring to the world of drug use in which people are chronically vulnerable to temptations and relapses. Beyond making a statement about the contradicting contemporary definition and understanding of addiction, Weinberg’s data evidently show that the risk of falling back into previous practices of AOD use as soon as the safe and structured boundaries of residential treatment are no longer present is high. The newly establish drug-free life within the social world of a programme has no, or very little, bearing outside the programme, where old associations, places and networks are available configurations for previous drug-use-related practice.
Considering the contrasting environments of, or space between the social world of a treatment programme and the conditions of possibilities in the world outside, it is of importance to gain a better understanding of the demanding process of disentanglement from previous drug-using practice. Bourdieu’s concepts doxa and illusio might illuminate part of the relational social dynamic at play during these transformations. Doxa refers to the “relationship of immediate adherence that is established in practice between a habitus and the field in which it is attuned” (Bourdieu & Nice, 1990, p. 68; Veenstra & Burnett, 2014, pp. 188, 193). The concept of illusio captures the relationship between a person and a certain field, and represents the interest that the individual has in that field (Bourdieu, 2000; Bourdieu & Wacquant, 1992). Every field is characterised by the pursuit of a specific goal (or goals), and illusio describes practices related to pursuing this goal; the investment that the participants make in the field and their involvement in it (e.g., in a treatment programme) are perceived as interesting and important (engagement), and therefore worthwhile. Deeply felt commitment and participation within the field are expressed via “doxic” attitudes, whereby a positive investment and the presence of high-value rules together establish illusio. When the social world appears natural and self-evident, the individual experiences the doxic mode (Bourdieu, 1977; Veenstra & Burnett, 2014). Conversely, when individuals move into unfamiliar situations and social settings, they will experience lack of doxic modes, consequently, the experience of a strong feeling of maladjustment might occur. Hence, the experience of the embodied “pull” towards previous drug-using practices, networks and relationships, might be manifested as part of this relational social dynamic.
The attempt to make major changes in living practices by entering and re-entering diverse social settings, networks and relationships, including the social world of treatment, exposes the individual involved to challenging and vulnerable situations. There is a call for greater attention to the how of these transitions, with a special focus on the phase of leaving treatment, in order to contribute to the knowledgebase from which treatment support and development might benefit.
Method and sample
This study was based on in-depth interviews carried out during autumn 2013 with 17 men and women living within the catchment area of Stavanger University Hospital. All of the participants had experienced years of severe AOD use, for which they sought professional help, they had been, or still were, socially marginalised, and they were recruited from both outpatient and residential treatment facilities. In relation to the participants’ preferred use of drugs, two reported use of only alcohol, one reported use of only cannabis, and the rest reported use of multiple drugs. Further, they had all been given patient status based on their problems related to AOD use, and they were all aged 18 years or older. Since we were interested in the subjective experience of recovery, the selection of participants was based on them being abstinent or having made a significant reduction in drug use, and their self-reported experience of making positive lifestyle changes.
The study received ethical approval in advance from the Regional Committee for Medical and Health Research Ethics (approval no. 2013/559/REK) in spring 2013. Participant recruitment, interviews and data analysis were performed as part of a larger prospective longitudinal cohort study, called the Stayer Study. Details about the methods used for sampling and recruitment are available elsewhere (Hagen, 2018). Participants for the individual interviews in the present study were recruited in parallel with the recruitment of the participants to the Stayer Study at a six-month follow-up test point. At the six-month follow-up, associates of the Stayer Study responsible for recruitment provided participants who had made a substantial reduction in AOD use or who were abstinent, with information about the recovery project, and asked them if they considered themselves to be moving towards a better life, a life that they wished for. Those who confirmed that this was the case were then asked by the associates for their additional consent to allow the first author to contact them. The recruitment phase lasted until the selected research participants reflected the variety of the characteristics exhibited by the entire Stayer Study cohort (see Table 1). Thus, the participants of our study represent a specific group of individuals.
Comparison of the demographic characteristics of the interviewees in the present study and the Stayer cohort
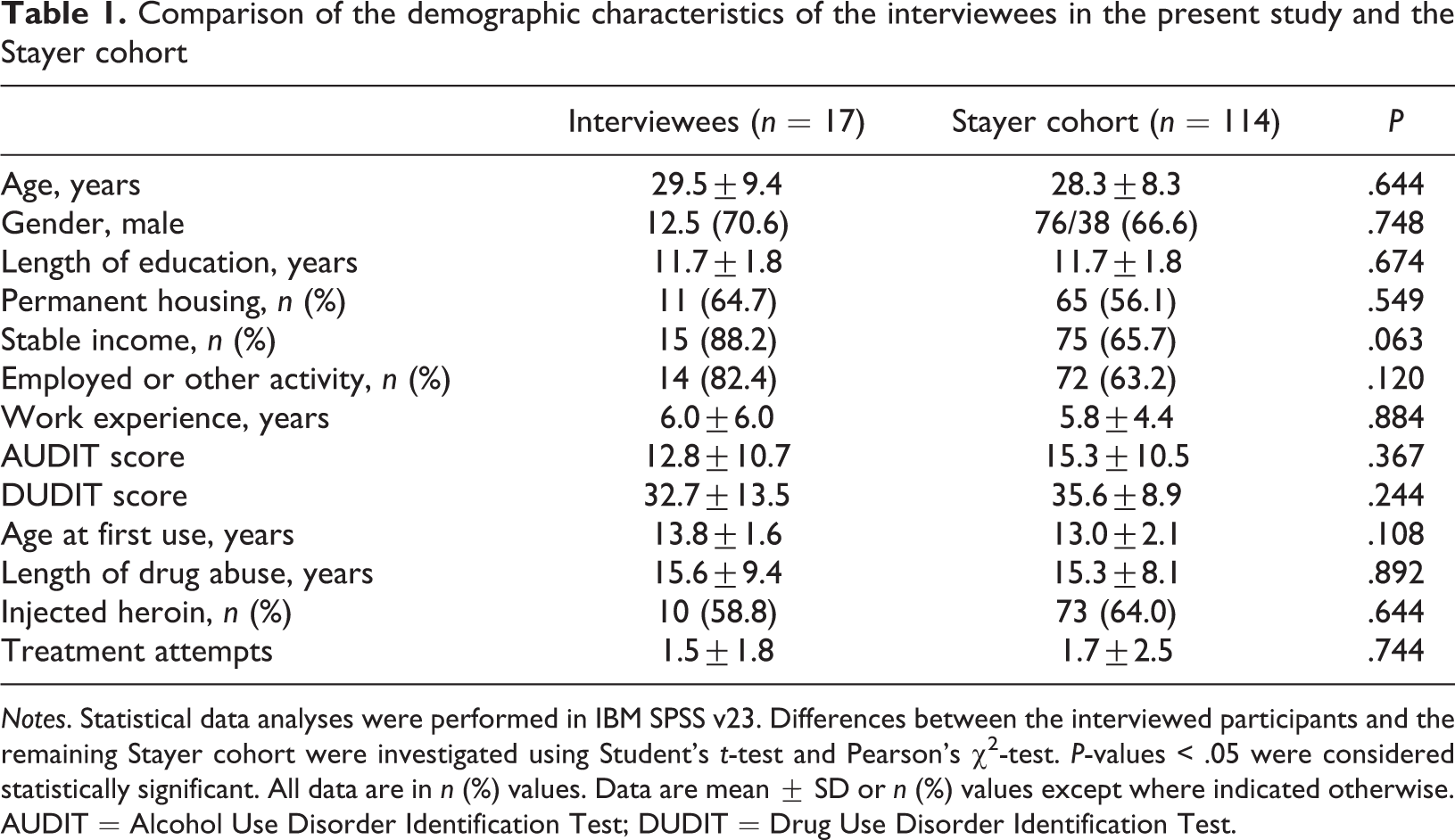
Notes. Statistical data analyses were performed in IBM SPSS v23. Differences between the interviewed participants and the remaining Stayer cohort were investigated using Student’s t-test and Pearson’s χ2-test. P-values < .05 were considered statistically significant. All data are in n (%) values. Data are mean ± SD or n (%) values except where indicated otherwise.
AUDIT = Alcohol Use Disorder Identification Test; DUDIT = Drug Use Disorder Identification Test.
The interviews were conducted at a location shared with the Stayer Study, which is a medical centre in downtown Stavanger. All of the interviews were conducted by the first author. Deliberate attempts were made in the interviews to ensure that the conversations were open and exploring, in order to facilitate the participants relating what was important to them (Järvinen & Mik-Meyer, 2005). The participants were encouraged to describe the various stages of their drug-using experience. Certain specific themes were covered in all of the interviews, including the onset of drug use, escalation of consumption, life situation, attempts to stop, social networks and friendships, relapses, and involvement in treatments. Guided by grounded theory as it is presented by Charmaz (1990), the researcher asked questions such as “Why do you think that is?”, “How do you feel about that?”, “What’s your experience with […]?” and “What made you do that?”. This exemplifies a version of ethnographic interviewing using descriptive, structural and contrast questions, which are intended to produce narratives about socially embedded experiences (Halkier & Jensen, 2011, p. 110).
Confidentiality was ensured by (1) keeping contact information separate and in a secured locker, in accordance with Health Research Ethics guidelines, (2) giving each individual a pseudonym and identity number (as was done for all of the participants in the Stayer Study), and (3) not including the names of the facilities where the individuals had received treatment.
The interviews were audiotaped and then transcribed and entered into a qualitative software package (NVivo 10) for systematic coding. As mentioned above, a grounded theory approach (Charmaz, 1990) guided the commencement of the analysis. According to Charmaz (1990), a grounded theory approach can be used as a starting point in both framing of questions and readings of interviews, fostering a sensitive reading to look for themes and issues. Based on repeated readings of the data and related literature, theoretical approaches can be applied to expand the perspective on how to interpret the themes and issues raised by the participants, and in particular to grasp the complexity of their experiences and practices. In our case Bourdieu’s practice theory was introduced and applied to themes and issues emanating from the participants’ stories. In addition to this, a narrative approach helps us to understand the language and verbal interactions (narratives and narrating) used as bearing traces of the broader social structure, social settings and their circulating discourses and power relations (Maruna, 2001; Riessman, 2008). Further down the analytical road we “discovered” that the methodological strategies derived from analytical translation of social practice theory (Halkier & Jensen, 2011), fitted well within our chosen methodological approach. It is worthwhile mentioning that Charmaz argues for a social constructivist version of grounded theory, and that Halkier and Jensen argue for a social constructivist version of practice theory. In combination these methodological tools allowed us to analyse the material to identify associations between people, places, living practices and self-conceptions. Our “groundedness” was applied by starting with data from lived experiences, sensitised by theoretical concepts such as “identity/self”, “recognition”, “meaning”, “emotions”, “change”, “action”.
Based on the above presented methodological “toolbox”, the analysis of the collected data began with a simple thematic coding that involved identifying practices and self-conception associated with both using and not using drugs. It was important to identify and record accounts related to diverse social settings, daily lives, actions and social relationships. On the basis of the emerging insights, a more intensive analysis was used to search for core aspects and conditions for the transforming recovery process and changing practices. Accounts similar to “I’m new to this life”, “I have to learned how to live again” or “I don’t know how to do anything” were expressed by the participants, thus creating the aspiration to apply theory of practice with the use of Bourdieu’s concepts habitus, field and doxa to gain a better understanding of the social dynamic and transformation of practice underlying these accounts.
Results
At the time of the interviews, all but two of the participants had not been using AOD for at least six months or longer. All but three of the participants had received inpatient treatment. Three participants were still living in a residential facility, while the others lived in their own accommodation or were accommodated in housing programmes. Moreover, eight of the participants attended self-help or peer-support groups such as Alcoholics or Narcotics Anonymous (AA/NA) either as an adjunct to or after professional treatment, as well as receiving welfare support (to provide a stable income) and/or being enrolled in a welfare programme. Their employment statuses varied from long-term or temporary unemployment to being in a training programme preparing for employment, to normal employment but with reduced working hours. The mean age of the participants was 29.5 years, with ten aged 22–30 years, five aged 31–40 years and two older than 41 years. Most of the participants preferred using opiates, but AOD were also used.
The 17 participants in our study had experienced years of drug use, starting from a young age and escalating to extensive AOD use. The use of AOD had resulted in the participants dropping out of school and/or losing employment, as well as in broken friendships, partner and/or family relationships, hence, it can be argued that our participants were, at the time when they were recruited to the Stayer Study, social marginalised. All but one at the time of the interviews had experienced previous phases of abstinence and recurrent relapses, as well as repeated treatment attempts. Prior to the last admission, those who reported being abstinent at the time of the interview had had the experience of “hitting rock bottom”, or coming to the point where “enough is enough” (Årstad et al., 2018). At the time of the interviews, the participants were attempting to achieve a drug-free life. The obtained storylines indicated that the participants saw themselves as changing from drug addicts to recovering addicts (Anderson & Bondi, 1998), echoing the traditional narratives of Alcoholics Anonymous (AA) and Narcotic Anonymous (NA) (Strobbe & Kurtz, 2012; Weegmann & Piwowoz-Hjort, 2009).
With the aim of identifying the social dynamic underlying these personal and existentialistic experiences and transformations, the present analysis focused on three key themes based on the participants’ experiences as recounted during the interviews: (1) their involvement in the residential treatment setting, (2) the process of leaving treatment, and (3) the process of changing everyday practices into a drug-free way of living.
Getting involved
With relevance to Weinberg (2000), the stories told by the participants in the present study indicated that when in treatment they managed not to use any AOD. In several of the interviews it was expressed that not using drugs was “easy” when participating in a programme, as opposed to the problems and challenges occurring when they were outside the safe boundaries of the treatment setting, dealing with old associates, as well as attempting to establish new practices and new social networks. Most of the participants acknowledged that involvement in a treatment programme was crucial for the process of recovery, but only on the condition of deep-felt commitment. Bourdieu’s concept of illusio is relevant here, by describing the experience of positive investment and the worthwhile nature of “working the programme”.
The stories told by the participants in this study who had received inpatient treatment bear traces of drug-abuse treatment discourses as presented by Weinberg (2000). They spoke of involvement in the treatment programme as being crucial for their process of recovery, but the involvement in the programme needed to be honest and with a deep-felt commitment. This was based on their previous experience of relapse and re-entering treatment. As presented in the background section, illusio in Bourdieu’s thinking (Bourdieu, 2000; Bourdieu & Wacquant, 1992) captures the deep-felt commitment to invest in the programme and acknowledge the worthiness of the rules. The implication of taking part in the illusio, pursuing the specific goal of recovery, holds a probability of fulfilment of different prospects for the future (Bourdieu, 2000), in the case of these participants a better life, a life without drug use, an independent “normal” life. With reference to Nettleton, Neale, and Pickering (2013), it is worth mentioning here that the “goals of recovery” or the “normal”, must be understood not only as a personal goal, but also as a product of a society that encourages and privileges normalities.
Becoming involved and “working the programme” with a deep felt intensity (illusio) were themes identified in many of the narratives, although with individual variations. Fredrik (28 years old) had been heavily involved in drug use (including heroin injection) for years. He started using drugs at the age of 12, had made numerous attempts to stop and had had numerous treatment admissions, but reportedly without really wanting to stop using drugs. At the time of his last admission his self-reported condition was as bad as it could be, described in the classical NA phrasing of “hitting rock bottom” (Strobbe & Kurtz, 2012; Weegmann & Piwowoz-Hjort, 2009): Fredrik: So, it was a little bit like I began thinking to myself, this is my last chance to do things differently compared to what I’ve done before. […] But then I started doing things wrong. I started drinking in my first two home visits. But I could really feel that this was wrong, so I stopped. Then I started doing other things, I started looking at what I had in front of me in life. And I started training a bit, and I started getting involved in the programme [at the institution]. It was a pretty nailed programme, it’s tough, but I started somehow to engage more, go a little more into it, and care.
Like Fredrik, the story of Cecilie (23 years old) also exemplified the classical “hitting rock bottom” experience. Cecilie started using drugs when she was 12 years old. From that age forward her drug use escalated and her habitus was adapted to a life revolving around drug use, drug-using friends and networks. At the time she was admitted, she was living on the streets, was very weak and in deep despair. In the interview she described the following: Cecilie: […] you know, there were many […] especially two who worked at the facility, former heavy users […] they had obtained an education and worked there. So they understood very well my situation, they could give me support […]. And then, eventually, I took part in the treatment. Not the first weeks, when I was left alone because I was so sick, but pretty early on it was required that I took part in the programme, participate in discussion groups, join in groups and stuff like that, and that’s the reason for me being off drugs today, those two, together with the staff […] there was no means of escape.
Immersion in the social world of treatment programmes includes the establishment of practices associated with disciplining behaviour through a mixture of daily routines and obligations, social relationships and networks, group meetings, and technologies such as urine testing. Bill (31 years old) elaborated this as follows: Bill: My stay in the residential treatment institution lasted for about 10 months. There were clear boundaries, structure and routines. You had to learn to eat, get up in the morning, exercise, work […] go to bed, get back up the next morning; that routine is important to learn. In the institution you are surrounded by people all the time, 24/7, you work with people constantly, there is always something going on, I mean, there are about 15–20 people working there.
Consistent with the findings of Draus et al. (2015), the somewhat mechanical and trivial steps described above take on a deeper significance during the transition phase. Cecilie referred to these basic daily routines as “getting her life back on track”. Normal daily routines seem to be deeply rooted in a conception of life itself, the essence of existence: Cecilie: […] you know, the first year being off drug use is all about getting your body well, getting rid of the abstinences, getting your sleeping pattern back, I mean, I hardly slept for about half a year. Just get your body back in order, exercise, build some muscles, put some weight on, just get your life back on track, get some routines, manage to eat, and manage to get up […] stuff like that.
In summary, the present subjects considered involvement in a treatment programme to be crucial to establishing a way of being that was unrelated to previous drug-using practices, but the involvement needed to be deep-felt and considered worthwhile. However, the process of leaving treatment was experienced as both challenging and fragile. The social world of treatment programmes and the outside world were considered to be “contrasting ecologies” (Weinberg, 2000). Leaving the structured institutional existence that constrained their drug-use practices and empowering them to take control of their lives also meant that they were moving into social settings, networks and environments that they portrayed as being full of temptations and frustrations, which made them vulnerable to their drug-using practice once again.
In here, out there: From treatment to independent living
The contrasting ecologies of addiction (Weinberg, 2000) are similar to a classic AA/NA phrasing of being “out there”, which reflects an ambivalence towards the outside society (Rafalovich, 1999). In the participants’ stories the aspiration of a drug-free life was related to the idea of a life within mainstream society. This was conceptualised in phrases such as “living in the real world”, “returning to or living within normality” or “returning back to the society”. The participants who were chasing the goal of recovery associated drug-free practice with a “normal life”, an “ordinary” life or a life within mainstream society, similar to findings in the study by Nettleton et al. (2013). To express this, one can argue, participants tap into available popular mainstream discourse to express their dreams or aspirations for a “new and drug-free life”.
However, taking a social practice approach, these accounts, we argue, go beyond being a discursive repertoire, and reflect an experience of a contrasting and substantial difference between drug-using and drug-free practices, as well as the contrast between the boundaries of treatment facilities and the world outside, which seems to run through the stories told by the participants. In their stories they revealed a perceived experience of, for instance, a demanding challenge of keeping up newly established drug-free practices within the social setting of the treatment facilities in contrast to keeping it up within the looming outside world.
One common theme articulated in the interviews related to the contrasting environment between “working the programme” and the “outside world”, was the challenge of keeping up with daily routines that had been established within the institution after being discharged. Bill now lived in his own apartment and held a 60% work position, and he talked about the difficulties of maintaining disciplined sleeping patterns and activities which he adapted when he was “working the programme”: Bill: I’m off work from Thursday to Monday. If I haven’t made any plans and activities for these days, and, you know, just being lazy, staying up all night and sleeping all day, that really does something to me. It’s like old wounds and patterns pop up to the surface. Then I really have to straighten myself up, I mean, it’s nobody else doing it, I have to be responsible for myself. It’s not like in the institution, where someone else takes that responsibility. You know, I’ve had to learn to recognise old patterns and habits, and correct myself and change things. Usually it takes a couple of days before I actually realise that I’m doing it, and can stop myself and reverse it.
Fredrik also talked about how the safe and comforting boundaries of the institution contrasted with drug-free life outside the treatment facially. Experiencing loneliness was prominent in his story. Even though he transferred from residential treatment to a housing programme with some staff, he found being on his own both liberating and frightening: Fredrik: Yes I was in treatment, and moved out in November 2012, and transferred into a housing programme, which is governmental housing for addicts who have completed long-term residential treatment. Doing that was liberating, and really great, but it scared me too, at first. It’s like, you come straight out from the institution and have to adjust to the life on the outside. Then you realise it’s actual rather lonely. You know, in the institution there are people all around you all the time, there is always someone asking how you’re doing. You know, you’re really well looked after. […] when you’re out of there, then the evenings come, and you’re lonely, but that’s okay, then some more evenings come, and it’s not so okay anymore […] it feels real lonely.
As stated by Hughes (2007, p. 689), “transforming identity involves pursuing a new trajectory, new kinds of participation in changing configurations”. The significance of this social mechanism is found in Bill’s story. The transition from the safe boundaries of residential treatment to independent living is about losing oneself, and subsequently (by changing practices) slowly becoming oneself. Bill expressed this process very clearly as follows: Bill: I feel that my identity slowly comes back; the longer I’ve been in the job I have, the longer I hang out with my new friends, the more I feel that I start to become myself again, become a person that I can like. This is something you do not learn in treatment, this is something you learn after treatment, really, this is how I feel. In residential treatment you get a kind of identity too, but it disappears when you leave, because then you don’t hang out with those people any longer, you don’t do those things anymore, you have another life, thus you find this new identity. It’s fairly smooth for me now, but during the first months I didn’t understand a thing.
Into the unknown
The embodied experience when encountering diverse social arenas and networks with a “drug-free agenda” was experienced by the participants of this study as alienating and often as accompanied with the feeling of maladjustment. The findings highlight that moving from a drug-using to a drug-free life involves changes in everyday practices. The process of moving into social settings and networks with a drug-free agenda was to a large extent unknown or forgotten by the study participants. As all the participants had had years of extended drug use, their everyday practice had been drug-use related over a long period of time, resulting in a disconnected relation to conventional social settings and practices not related to AOD-using practice. Further, for two thirds of the participants their early onset of drug use had created a deeply social entanglement related to AOD use. How they had learned to know and experience themselves was related to AOD use, which over time created a embodied know-how of the world that was AOD-use related, similar to what Gelpi-Acosta (2015) calls “junkie” habitus. Bill described this as follows: Bill: You know, in all settings possible, you have been using, in all kinds of situations you can think of. Using and scoring is related to all my experiences, and to all my emotions too. I mean, to all the emotions I ever felt I’ve been scoring. Everything arouses, or reminds me of using and scoring. Nothing is free from the memory of using. Even just going to the store is a reminder of use. Peter: Yes. It is not done in a jiffy this. Far from it. You must learn to live again. On my journey to residential treatment, I didn’t know myself as an adult person. I’ve used drugs virtually every single day since I was 16, 17 years old […] there are so many things that need to fall into place. Cecilie: You know, I’ve been using for 10 years […] so for 10 years that was my only object […] So, before [she is now a non-user] everything was related to drug use. I mean, I was using all the time, so that was all there was. My whole life revolved around using. Get the gear, use, avoid getting sick, score. Everything else was completely gone. Except for my dope friends I had nobody. No contact with family. Nothing […] I didn’t know how to do anything.
When AOD-related practice has been the focal point of existence over a long period of time, even from a very young age, this becomes a deeply embedded part of a person’s habitus. Thus, when the mental structure of habitus was not attuned to the structure and logic of the social settings and networks, which Kathrine (24 years old) called the “real world”, any pre-reflexive repertoire of embodied practice is considered “out of place”, leaving the person feeling maladjusted and often stupid. Bourdieu used the common expression “fish out of water” to describe the experience of the habitus encountering social fields for which it has not acquired and stored an understanding of its regularities and rhythms; in other words, the doxic mode to conventional social fields, which is not drug-use related, is missing. This is an embodied complex experience leaving one with emotions such as shame and guilt. The following excerpt reflects this mechanism. Kathrine: It’s a bit, like, very uncomfortable to meet the real world. I mean, you don’t have anything to contribute with, you know. It’s like you haven’t moved anywhere and it’s like you still are 15 in your head. I mean, you haven’t developed in any ways. Fredrik: You must not think that to stop using dope is the big thing, then the world opens up, you know, it’s not like that. It hurts to start living again when you’ve never done it before, you know […] I mean, imagine sitting in an enclosed room for 20 years, and then suddenly you’re supposed to go out and live like everybody else […] do what everybody else is doing. […] the abilities, potentialities and possibilities for a person to act are linked to the properties and rhythms of a field, the capital operating in the field, the constitution of habitus and the degree to which the person shares similar opinions and beliefs of the field (doxa). (Veenstra & Burnett, 2014, p. 193)
Practices need to be located in a certain time and space, and thus there is a need to access social arenas where these practices can be “acted out” in relation to somebody who both recognises and “acts upon” them. The resources, social dispositions, beliefs and understandings acquired and stored over time as drug users move through their lives are generally at odds with the ability to take advantage of opportunities available in social settings that are considered mainstream and do not involve drug-related practices. This in turn is rooted in the materiality of the body, in habitual action as well as social practices, which in turn is bound up with identities. “What I am is inextricably bound up with what I do” (Hughes, 2007, p. 677). With individual variation depending on previous experiences, some more than others expressed in the interviews that the most basic way of acting in, or relating to social settings and networks as a non-drug-using person, such as the way you talk to people and even behaviour as apparently trivial as how you walk, felt unknown and unfamiliar to them. When such mundane embodied actions appear unfamiliar and strange, it mirrors the challenge of becoming embedded in conventional non-drug-using life, as well as how the social is inscribed onto bodies.
Concluding remarks
Studies of people making attempts to leave long-term heavy AOD use have shown the process to be accompanied by strong feelings of maladjustment (Martin, 2011; Maruna, 2001; Nettleton et al., 2011), creating a high risk of recovering users returning to their familiar drug-related way of living (Bourgois & Schonberg, 2009; McKay et al., 2006; White & Kelly, 2011). Drawing on a social practice approach and some Bourdieusian concepts, we have demonstrated that the participants in the present study were to varying degrees – and often to limited extents – attuned to the many diverse and overlapping social fields that constitute the non-drug-using social world. According to Bourdieu, the ability to act and behave in a reasonable way in relation to the regularity of a particular field depends upon a habitus attuned to the constitution of that field (Bourdieu, 1977, 2000; Bourdieu & Wacquant, 1992). In line with what Nettleton et al. (2011) observed in a previous study, the stories of the participants in this study reflect the recovering body finding itself exposed to unfamiliar situations and social settings in which habitual actions are not yet established. Our analysis of the social dynamic underlying this experience revealed that receiving treatment might facilitate access to social settings and relations that represent norms, regularities and rhythms of conventional society. The treatment system (including its employees) offers a specific social setting for acting out drug-free practice. However, in our material, the commitment to “work the programme”, the deep-felt involvement in the rules, routines and activities of the institution was highlighted as crucial in the process of change. Despite deep-felt commitment in working the programme, leaving treatment exposed the participants to difficulties and challenges related to loneliness and maladjustment, the ability to keep up mundane routines and habits, and to establish drug-free social networks and work relations. Understood through the concepts of habitus, field and doxa, the experience of maladjustment in relation to non-drug-related practices can be interpreted as a habitus not sufficiently attuned to the field in question to create the doxic mode.
In contrast to Gelpi-Acosta (2015), who applied the concept of habitus to explain why people continue to use drugs, our data exemplify the process of restructuring habitus through change in everyday living practices. Although Gelpi-Acosta considered that restructuring “junkie” habitus was extremely difficult, our findings demonstrate that reinsertion into practices not related to AOD use is possible via a slow process of entering social settings, building new relations within these settings and learning ways to contribute something worthwhile to them, which in turn legitimates your place in them, consequently replacing the feeling of maladjustment with the feeling of belonging and restored identity. However, the transformation of thinking, acting and relating is not a finished project, but an ongoing accomplishment, exactly through embodied participation in specific social fields. The ongoing practical investment and accomplishment is hard work, because the former drug-using embodiment is still the dominant non-reflective stance.
Taken together this article has highlighted that the process of moving from a drug-using to a non-using lifestyle involves learning a new set of social practices that, to a large extent, felt unknown to the participants. Inherent know-how about the world, and embodied taken-for-granted knowledge about how to participate in everyday life are adversely affected by drug use. The associated changes involve rebuilding new practices through engagement in social settings and networks. The analyses performed in this study have revealed how the social setting of treatment institutions forms a structure and social network that can provided the study participants with the opportunity to transform their way of thinking, relating and acting. However, the distinction between the social settings of treatment institutions and the diversities of social settings related to non-drug use practices constitutes a major challenge in maintaining the fragile newly embodied social practices of a drug-free life. We suggest that the adherence established in practice between habitus and the field of treatment does not necessary transfer over to any other social fields, because the field of treatment represents a socially structured space with its own regulative principles. As soon as habitus moves into other fields, with different regulative principles, the experience of possibilities, limits and boundaries within these fields, the immediate know-how of how to act and behave, in short the doxic mode, depends on the level of the habitus attuned to the field. The doxic mode can only be acquired through time spent “playing the game” by encountering different people and fields and reasoning our way through complex situations (Veenstra & Burnett, 2014).
It is our belief that attempts to stop using AOD and rebuild one’s life are relationally bound. Working with the social practical approach, the attempt to break the cycle of abstinence and relapse can be understood as a process of change in embodied social practices, relationships and social settings, which is bound up with transformations of self and identity. Through highlighting different dimensions of these transformations, this approach shared the common objective to illuminate the social complexity of addiction and recovery, and to provide an adequate sociological approach.
Finally, while the findings from this study are not widely generalisable, they might provide a better understanding of the social dynamic underlying the difficulties of making major lifestyle changes. This knowledge may contribute to improving and tailoring care, especially when a drug-user or ex-user moves between diverse social settings or enters new social arenas as a necessary part of changing practices.
Footnotes
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.