
Abstract
Polydrug use is presented as a particular drug-use phenomenon when the combination of substances is and always has been the practice. The origin of the term is found in the early years of the war on drugs under the Nixon administration in the US, when it was used to justify the intensification of repressive measures against drug users and to counter the growing accommodation and normalisation of cannabis. Only by presenting cannabis as the first step towards the use of harder drugs could the repression of this largely innocuous and widely used substance be justified. Drug users were presented as “polydrug users”, which offered an explanation of problematic use as rooted in the drug user, the addict, who would switch substances in accordance with availability and price. Having become established for political reasons, the term has become entrenched because it resonates and vividly describes social practice. Yet it does not add to understanding of social reality but occludes and confuses because it presents “polydrug” as a particular and peculiar pattern of consumption and not as the norm.
Alcohol and cocaine when used concurrently are metabolised by the liver into a unique compound called cocaethylene that has stimulant, euphoric and anaesthetic effects, and significantly increases the risk of cardiac-related illnesses. Heroin injectors who combine or replace their heroin with the synthetic opioid fentanyl must be aware of its far greater potency. Combining various mind and mood-altering substances is the quintessential meaning of “polydrug use”, and may involve acute health risks that consumers and medical professionals need to be aware of. It would be erroneous, however, to presume that it was these concerns that motivated adoption of the term in the drug policy discourse. Far from enhancing the understanding of synergistic effects, the objective behind formulating and establishing the term was to point to a new form of problematic behaviour. While it does denote an established social practice and therefore differs from such fabrications as thirdhand smoke (Bell, 2014) or passive drinking (Burgess, 2009), it has created confusion in the analysis of drug-using behaviour.
Inadvertently, the very coining of the term to describe an ostensibly new and different form of behaviour, suggested the deviation from a stipulated though never enunciated norm, of mono drug use. This construction effectively has turned social practice on its head since most incidents of drug consumption encompass multiple substances, be these used concurrently or over a longer cycle.
It is this underlying reality that lends stability to the term and credibility to the rising number of studies and publications on drug combinations (Karjalainen, 2017). Yet, its rise, popularity, and implicit suggestion of particularity are suggestive of a process of social construction driven by vested interests and connected networks. Since the term presents as unusual a phenomenon that is regular social practice, its function is not to deepen insight or generate new knowledge. It is the contention of this article that the pseudo-scientific pretentions of the “polydrug” label mask an ideological function that is entirely extra-theoretical (Hacking, 1999).
Hypothesis, methods and orientation
My starting hypothesis is that over the past century the international control system has selected and adopted different theoretical models from the drugs field, to justify and extend itself. Since the foundational assumption of the system, the “world drug problem”, 1 is a chimera, and the overall objective of a “drug-free world” is illusory, concepts are continually being adapted to better manage expectations of critical constituencies such as voters, taxpayers, and professional groups. Concepts therefore have a rhetorical function of justifying the appropriation of resources in pursuit of a greater good (the drug-free world), while providing a rational explanation for the failure of previous efforts.
With “polydrug” the drug problem is reconfigured and restated through a series of associations with established and recognised threats. Its primary function is therefore rhetorical, and the objective is to legitimate a series of political measures. In support of this proposal, I cite utterances of drug policy makers and policy documents, and track the occurrence of a few critical terms through the Google Ngram viewer. This is an online search engine for counting the appearance of words or word clusters found across sources printed between 1500 and 2008 in Google’s text corpora, making allowances for the increase in publications over time.
From its emergence to the current use, the term “polydrug use”, and its implicit misrepresentation of social reality, throws an interesting sidelight on the drug control system, the mis-information produced by scientific expertise and the role of the drug-treatment sector. As with many social phenomena, social trends, political reactions and scientific observations follow broad patterns across Western countries. But in the field of drug control the role of the US is pivotal to the definition of the issue and the shaping of governmental responses, hence I draw on US as well as European sources.
The construction of “drugs of addiction” as a justification of the control system
It has been noted that the semantic value of “drug” has changed significantly in the course of the 20th century, losing all association with medicine and simply denoting a menace. Establishing the negative connotation of “drug” was part of the control project, initiated with the international prohibition of the opium trade, and built on the evolving notion of addiction.
As drug users are suspected of switching between substances depending on price and availability, the precautionary principle was evoked early on to justify the prohibition of novel substances, or those with little use or popularity in a particular country (Musto, 1972). Cannabis for instance was banned in the UK in 1925 when consumption was miniscule. In recent years many European countries have banned the herbal stimulant khat even though there was no recorded consumption.
Yet, these assertions are based on inferences and judgments. The very concept of “drugs”, it has been argued, is not a “scientific” assessment, but a moral evaluation that presupposes a network of intertwining discourses. If, as Fraser and Moore have proposed, drugs are a “political category” (Fraser & Moore, 2011, p. 10), and action oriented, we can then reverse the “realist” view that the control system was constructed to control the dangers posed by drugs, and suggest instead that drugs were socially constructed to justify the creation and expansion of the control system. This system is based on the acquisition and distribution of powers and resources, along a value-based hierarchy where “drugs” become a defining principle in the allocation of rights. Authority is therefore invested in specialised agencies, while the targets of policy interventions, such as drug consumers and traders are divested of their rights to liberty, property and even life. Contempt and even hatred for addicts, dealers, smackheads, junkies, is a defining feature of repressive countermeasures. The latest authoritarian leader to unleash a state-sponsored, extra-judicial blood letting, Rodrigo Duterte, president of the Philippines appealed to the people: “If you know of any addicts, go ahead and kill them yourself as getting their parents to do it would be too painful” ( Guardian, 2016). Even UN agencies at the apex of the international system have been accused of being slow in ensuring “that the domestic drug laws mandated by the treaties are drafted and implemented in a manner that safeguards human rights” (Lines, Hannah, Schleifer, Avafia, & Barrett, 2017, p. 234).
In trying to explain that urge to punish the drug offender, Thomas Szasz has compared 20th-century drug users to witches and heretics, who played the function of the ritual victim or pharmakon (Szasz, 1970). The proposal that medicine presents a form of social control parallels the notion of bio-power and connects with the anthropological reflections of René Girard (1972) who posits that the scapegoat mechanism fulfils the function of sacrifice and lies at the origin of human culture. The war on drugs may therefore meet a subterranean but all the same urgent social psychological need, which has nothing to do with public health or morality.
However important the scapegoat mechanism may be in orchestrating the archetypes of the collective subconscious, rational criticism and political processes demand detailed explanations as to why particular victims are chosen.
The political instrumentalisation of the war on drugs
According to some commentators the drug control system was built for political ends from the outset and has become embedded in the partisan divide that characterises the public discourse on social issues in the US that is often referred to as the “culture wars”. Rising drug consumption and liberal attitudes towards drugs, and particularly marijuana, in some quarters found political expression in state level policies, but were countered by, and possibly even triggered, a repressive and intolerant reaction. This came to a head in the early 1970s when president Nixon declared the war on drugs, ostensibly because of spreading marijuana use and the prospect of thousands of Vietnam veterans coming home with entrenched heroin habits. Many commentators now think that the main motive was his “animus toward the counterculture” (Martin, 2016). Behind the smokescreen of publicly funded methadone programmes, the criminal justice system was mobilised to crack down on the opposition. The presentation of drugs as an existential threat to the nation …was also a symbolic means of stigmatizing youth protest, anti-war sentiment, Black Power and anyone with a non-regulation haircut—underscoring once again that pot prohibition had little to do with the actual effects of the herb and everything to do with who was using it. (Lee, 2013) The Nixon campaign in 1968, and the Nixon White House after that, had two enemies: the antiwar left and black people. You understand what I’m saying? We knew we couldn’t make it illegal to be either against the war or black, but by getting the public to associate the hippies with marijuana and blacks with heroin, and then criminalizing both heavily, we could disrupt those communities. We could arrest their leaders, raid their homes, break up their meetings, and vilify them night after night on the evening news. Did we know we were lying about the drugs? Of course we did. (Baum, 2016)
Since then, successive US presidents have elaborated an extensive system of repression, exclusion and patronage by substantially investing in law enforcement. The subsequent exponential increase in the US prison population, and the disproportionate targeting of African Americans has led many US scholars to attribute concrete motives to drug prohibition advocates. It is now widely argued that drug control has been devised as a tool for the systematic persecution of ethnic minorities. Since felons are stripped of many civic rights after their release, the targeted use of drug laws has created a large underclass of American men (mainly) from minority ethnic groups, who are “denied the right to vote, automatically excluded from juries, and legally discriminated against in employment, housing, access to education, and public benefits, much as their grandparents and great-grandparents were during the Jim Crow era” (Alexander, 2010, p. 15).
Poly at the gateway to the drug war: Arresting the normalisation of cannabis in the 1970s
The primary target of anti-trafficking campaigns in the Reagan and elder Bush era was cocaine, which, with the ingenuity of backstreet chemists, was being turned into crack for new consumer groups (Golub & Johnson, 1996). The confluence of controversial consumption patterns with politics of race, class, criminal justice and welfare reform opened new possibilities for repressive policies targeted predominantly at ethnic minorities and the poor (Bourgois, 1995; Reinarman & Levine, 2004). But the ground had been prepared by a systematic campaign of problematising “drugs” at a time when large sections of the population were learning to live with by far the most popular illicit drug, marijuana.
The shift in public attitudes is reflected in the number of people believing that marijuana should be legalised, rising from 12% in 1969 to 30% in 1978 (Pew Research Center, 2013). At that point the possession of small amounts of marijuana was decriminalised in a number of US states, including Alaska, California, Colorado, Maine, Mississippi, New York, Nebraska, North Carolina, Ohio and Oregon. In popular culture characters like Cheech and Chong presented the pot head not as a fearsome menace but as lovably “dazed and confused”.
A change of policy was called for and signalled by the conclusions of the National Commission on Marihuana and Drug Abuse, appointed and tasked by President Richard Nixon. Reporting under the enigmatic title “Marihuana: A signal of misunderstanding; first report”, it found that cannabis was not dangerous, compared its use to that of alcohol, and recommended decriminalisation and social measures rather than the criminal justice system to discourage use. Pointing to the “emotionalism” surrounding the topic of drugs, it found that governments had been pressured into action and had created growing bureaucracies “at the federal, state and community levels, of a vested interest in the perpetuation of the problem among those dispensing and receiving funds” (Sterling, 2013).
The vested interests around the president’s office reacted immediately. John D. Ehrlichman is on record calling it “a lousy report” while Nixon worried that the message would be misunderstood as an argument for legalisation. 2 The recommendations were not followed and the findings were suppressed as the White House continued investing in the very drug control machinery the report had warned about.
The behavioural epidemiology pioneered by the Marijuana Commission was continued in school surveys, and recorded the rapid spread of illicit drug use, predominantly marijuana. Datasets from hospital emergency rooms, meanwhile, found 5755 different two-drug combinations (Gropper & Burke, 1974), and pointed to a clear medical requirement for understanding the synergistic effects. These findings allowed clinicians to propose that “drug abusers have historically tended to abuse more than one drug” (Kaufman, 1976, p. 279).
It was against this background that the term polydrug emerged. The origin, then, was not a drive for better information needed by clinicians. It was, according to the then Director of the National Institute on Drug Abuse (NIDA): …a Federal, political term, rather than a scientific term…the word became big in the field about 2 and a half years ago when there was a growing recognition that there were drug problems that were distinct from either the alcohol problem or the heroin problem. (DuPont, 1976, p. 311)
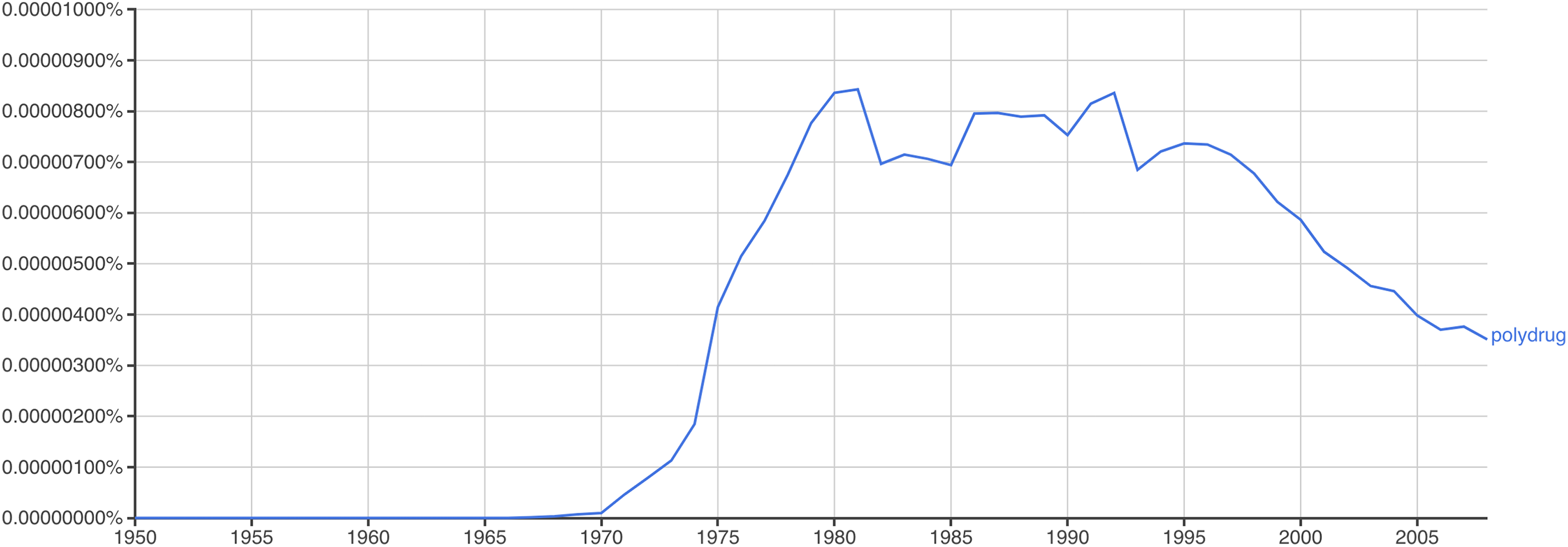
Incidence of the term “polydrug” in English-language literature.
Policy makers and agency staff had been preparing the ground. According to Henry Giordano, director of the Bureau of Narcotics and Dangerous Drugs (BNDD), “the use of marihuana develops a taste for drug intoxication which, in turn, leads many people to the use of more potent drugs—even heroin” (Lee, 2013). Applying elements of “tolerance” to a model of cross-substance dependence, the Attorney General John Mitchell claimed that after experimenting with marijuana the user “gets less of a charge from it, and this psychological dependency causes him to move on to the harder stuff.…We have got to get proof that it does create this dependency” [my emphasis] (Barcott, 2015, p. 53). And the next head of the BNDD, John Ingersoll, was quoted as saying: …it is a matter of record that the explosion in marijuana use has been accompanied by a sharp upturn in heroin use…We know that the overwhelming majority of those who use heroin or LSD…have had prior experience with either marijuana or hashish. (US News and World Report, May 25, 1970) (Goode, 1972, p. 13)
Interestingly, US policy makers have resurrected the model in recent years. The former US Attorney Geoff Sessions, an outspoken opponent of marijuana regulation and former New Jersey governor Chris Christie have used the “gateway theory” to draw a parallel between cannabis reform and the US “opioid crises” (Quenga, 2017). Mounting evidence of the number of opioid prescriptions falling significantly in those US states where medical and/or recreational marijuana is available (Wen & Hockenberry, 2018) has not deterred drug war advocates from employing the “gateway” as an argument for reintroducing tough penalties against cannabis users and sellers.
Poly lives on as a peculiarity
The term has lived on anyhow, corresponding neatly, albeit tautologically, to the reality of lived experience. Moreover, it has entered the bureaucratic discourse and become integrated in the monitoring and surveillance systems. With little sense of irony “polydrug users” continue to be presented as a particular type, and as a novel phenomenon, or in the words of the UK Drug Strategy, an “evolving challenge” (HM Government, 2017).
Yet it is increasingly clear that the majority of people interviewed on substance-use patterns report “having used two or more substances” (EMCDDA, 2009, p. 9). This would confirm the observation made in the previous UK drug strategy that “polysubstance abuse is increasingly the norm amongst drug misusers” (Home Office, 2010, p. 27).
Drugs have always been used in combinations, for reasons that extend from economy, to taste, to the management of effects. But crucially, drug use is mainly a social and recreational activity. The main objective is pursuit of pleasure, for many synonymous with consumption. Illicit substances have therefore been woven into culturally established recreational patterns surrounding music, dance, the ever-present promise or threat of sexuality and of course the consumption of licit substances. These often provide the model, hence in Europe cannabis continues to be often mixed with tobacco into what becomes known as a cannabis cigarette or “joint”. This most widely used “delivery vehicle” is already a polydrug cocktail combining the world’s two favourite weeds. Smoked at weekends, at parties, in neutral spaces on the way to recreational centres, cannabis/tobacco use is often followed by alcohol consumption. Far from presenting either a novel or a problematic phenomenon, poly has always been the norm.
Though this has long been known, it has had little impact on classificatory schemes because researchers have simply been working with categories that were defined by policy makers. Meanwhile, the drug treatment sector, expanded in most European countries during the 1990s, has largely been geared to working with opiate users, particularly injectors. Opiate users were highly visible “at risk populations”, whose habit was easily diagnosed, and who could be managed with the quasi-medical practices of supervised withdrawal in residential facilities and methadone substitution. Encouraged by the political concern about HIV/AIDS and a political imperative to reduce overdose deaths, treatment services rose to the occasion by heroically rolling out opiate substitution only to then find it challenging to respond to other needs.
Conclusion
“Polydrug” still has a lot of mileage for causing confusion among observers, laymen and policy makers alike. Academics working in the social sciences, or treatment professionals, will continue to make use of a term that implicitly suggests that mono drug use is some form of countercultural norm. Not only is that a deeply flawed assumption, but the lived reality of drug combinations is most of all a positive sign, suggesting that users are not enslaved to any one drug but remain in charge of the effect and experience. That kind of knowledge is the result of experience, prior knowledge and research, attitudes that are not encouraged by current policy nor accommodated by the hold-all term “misuse”. To learn more about the potential effect of two or more substances, users therefore have to turn to websites like EROWID for personal accounts. They may also peruse customer feedback on the quality of product they procure from dark web sites. Once again scene and market are pulling ahead, while the research and treatment sectors are limping behind, trapped by the assumptions that they are themselves responsible for establishing.
Footnotes
Declaration of conflicting interests
The author declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author received no financial support for the research, authorship, and/or publication of this article.